")
Back to Journals » Clinical Interventions in Aging » Volume 10
It is not their war: the impact of military operations on Philippine migrant care workers for elderly people in Israel
Authors Ron P
Received 21 November 2014
Accepted for publication 24 March 2015
Published 26 June 2015 Volume 2015:10 Pages 1053—1061
DOI https://doi.org/10.2147/CIA.S77886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Pnina Ron
School of Social Work, Faculty of Welfare and Health Sciences, University of Haifa, Haifa, Israel
Objective: A majority of work immigrants from the Philippines came to Israel to fill positions involving personal and nursing care. Most of them were in Israel during the Second Lebanon War, the Cast Lead operation, and the Protective Edge Operation. These migrant care workers experienced these events no differently than did the Israeli population. The goal of this study was to examine the connections between the Philippine migrant care workers’ exposure to the military operations and the levels of post-traumatic stress disorder (PTSD), death anxiety, and burnout among them.
Methods: A random sample of 147 Philippine migrant care workers was recruited through four agencies that employ migrant care workers. Participants completed a self-report questionnaire.
Results: Philippine migrant care workers reported high levels of PTSD, high levels of death anxiety, and low levels of burnout. Levels of exposure were positively associated with levels of PTSD, death anxiety, and negatively with burnout. A significant inverse relationship was found between interpersonal variables (self-esteem and sense of mastery) and the PTSD, death anxiety, and burnout levels reported by the participants.
Keywords: elderly care, death anxiety, work immigrants, burnout, military operations
Introduction
According to the values of Philippine culture, taking care of elderly people is considered a respectable job, and the sense of privilege at being able to “repay a debt of gratitude to those who helped me” (utang no loob). Hence, from a cultural perspective, according to the worldview of the Philippine women and men who come to Israel to increase their earnings and support their family members back in the Philippines, caring for elderly people is seen as a type of mission.1,2 Philippine migrant care workers engage with the elderly people and occasionally with their families within a few days after they arrive at the elderly person’s home in Israel; they live together and share the same household and destiny regarding the national and personal safety.
Wars and military operations have been a part of the Israeli population’s daily experience over the years. Recent examples include the Second Lebanon War (2006), the Cast Lead Operation (2008), and the Protective Edge Operation (2014). Due to the frequency of national terror attacks and military operations, most medical service providers and professional staff are already organized to function in cases of mass emergencies and have developed operational procedures for use in critical situations; however, for the immigrant workers, these situations are completely new, unfamiliar, and frightening. Moreover, over the last few decades, there has been greater attention to the impact that crisis conditions have on critical support professionals such as – but not limited to – rescue forces, nurses, and social workers.3,4 Yet very little attention has been paid to the impact on migrant care workers.
The impact of ongoing terror attacks, wars, and military operations
By definition, the conditions associated with ongoing missile attacks, military operations, and wars entail certain effects on the targeted population: loss of life, injuries, and increased anxiety and fear.5 Studies conducted with the immediate victims of such events, ie, the general population, survivors, and witnesses, have confirmed that populations living under such conditions are at a high risk for developing distress or acute stress disorder (ASD).6 The symptoms of distress include generalized fear and anxiety, repeated thoughts regarding the event, psychological symptoms, depression, and difficulty in daily functioning.7,8 In severe cases, a reaction of distress can result in post-traumatic stress disorder (PTSD) of varying severity.9,10 It was found that professional staff treating the civilian population in times of war reported levels of PTSD and acute stress lower than those experienced by the general population.3,4
Death anxiety is described as a term encompassing a cluster of death attitudes, characterized by fear, threat, discomfort, and other negative emotional reactions. The term “fear of dying” refers to the fear of undergoing a violent or painful death. One factor studied in relation to death anxiety is the sex variable. Studies that examined the sex variable indicated that women displayed higher levels of death anxiety than did men.11 Burnout is described as “a state of fatigue or frustration brought about by devotion to a cause, way of life, or relationship that fails to produce the expected rewards”.12 Burnout has also been equated with alienation, depression, anxiety, loss of idealism, and hopelessness in response to stress. Nursing is considered a helping profession that entails a very high risk of burnout, since it is very much a client-oriented profession, and nurses are involved in complex life-and-death situations.13 Among paraprofessionals, such as nursing assistants and workers caring for the elderly, the burnout occurs even sooner and its effects are stronger than that among nurses. In fact, the role of providing around-the-clock care for elderly individuals is considered to be the job with the highest burnout rate in Israel.14 It should be noted, however, that the study citing the highest burnout rates was conducted among paraprofessionals (nursing assistants) employed in nursing homes, where they work 8-hour shifts daily. After the shift, they go home, to be with their families and to attend to their own private affairs. It may be assumed that migrant care workers living day in and day out with an elderly person might experience even higher levels of burnout than those experienced by paraprofessionals who work shifts.
Based on the literature review, the current study investigated the following research questions: 1) what is the effect of variables related to the type of exposure to the stressful event (personal or professional/direct or indirect) on the levels of PTSD, death anxiety, and burnout, among the Philippine migrant care workers? 2) what is the effect of each of the interpersonal and intrapersonal variables (self-esteem, sense of mastery, and social support) on the levels of PTSD, death anxiety and burnout, among the Philippine migrant care workers?
Methods
Population and sample
The sample included 147 Philippine migrant care workers employed as caregivers for elderly people living in the northern and southern regions of Israel in private residences in the community. The reason for choosing only Philippine migrant care workers as study participants was that at the time of the Second Lebanon War (2006), most of the 20,000 migrant care workers in Israel were from the Philippines. As the study evolved, when seeking participants after the two other military operations, it was only obvious to choose Philippine participants again, to try to keep the characteristics of this group as similar as possible to those of the first group. From the two designated geographic areas, Northern and Southern Israel, we randomly chose four agencies that employed both local Israelis and Philippine migrant care workers for the elderly. The reason for choosing these two particular geographic areas was that both were under major bombing attacks, which endangered the lives of the civilians living there. During the Protective Edge Operation, civilians living in Israel’s central region were also at risk due to the bombings. Yet, for the purposes of the study, it was decided to limit the recruitment of participants to these two geographic areas. We contacted the directors of the sampled employment agencies directly, explained the goal of the study, and asked for their cooperation in distributing the questionnaires to their employment agents, so that they would contact the relevant employees, ie, the Philippine migrant care workers who had been in Israel during all of the three military events mentioned herein. At this stage, the sampling method became a snowball sample, because the employment agents asked the Philippine migrant care workers they knew to ask their friends if they were also in Israel during those three military operations. The questionnaires were sent by mail to each of the agencies and were mailed back to us. Of a total of more than 600 questionnaires that were sent out to the group of workers, 147 (approximately 24%) questionnaires were returned. Twenty-seven of these questionnaires were not included in the final sample, due to missing data. The demographic characteristics of the study participants are tabulated in Table 1.
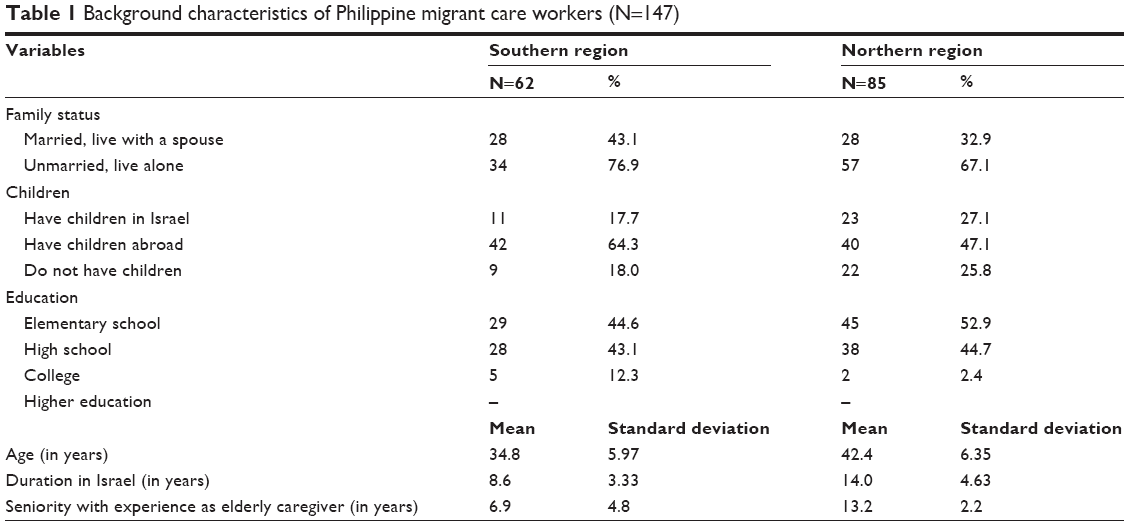 | Table 1 Background characteristics of Philippine migrant care workers (N=147) |
Instruments
Independent variables
Exposure to military operations: Personal and professional exposure to military operations was determined based on the participant’s direct or indirect exposure to a military event. The variable was measured using five questions. For example: “Were you in the area that was affected by the war/military operation?” Answer categories were dichotomous. Participants who did not experience this event or could not relate to such events answered “no”, which was given a score of 0, and those who had experienced this event or had been exposed to similar events answered “yes”, which was given a score of 1. This instrument had been used previously in studies with a similar focus.3,4 The demographic variable was measured using a self-report questionnaire.
Professional experience was measured by the number of years of experience in the profession of caregiving for the elderly.
Social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS).15 The scale consists of 12 items that are rated on a 7-point Likert scale (1= strongly disagree and 7= strongly agree). A high average score indicates a high level of social support reported by the research participants. The original tool’s reliability was 0.88 Cronbach’s alpha, and in the present study Cronbach’s alpha was 0.91.
Sense of mastery was measured using the scale of Pearlin and Schooler.16 The scale includes seven items that are rated on a 5-point Likert scale (1= strongly disagree and 5= strongly agree). A high average score indicates a strong sense of mastery reported by the research participants. The reliability of the original scale was 0.79 Cronbach’s alpha, and in the current study it was 0.81.
Self-esteem was measured using the ten items of the Rosenberg Scale of self-esteem.17 The items are ranked on a 5-point Likert-like scale ranging from 1= disagree completely to 5= strongly agree. A high average score indicates a high level of self-esteem among the research participants. The questionnaire’s reliability rate was between 0.81 and 0.90 Cronbach’s alpha.
Dependent variables
PTSD was measured using the DSM-IV-TR. Participants’ reports related to experiences over the last month that coincided with symptoms, as described to them, eg, “(you) felt as though something really bad that had happened to you in the past was happening all over again”. Responses were provided on a 4-point scale, ranging from 0= “not at all” to 3= “almost all the time”. A high average score indicated a high level of PTSD among the research participants. Internal reliability of this instrument was 0.90 Cronbach’s alpha.
Death anxiety was measured using the Carmel and Mutran questionnaire,18 which includes six fear-of-death items, eg, “I am very scared of death”, rated on a 5-point Likert scale, from 1= “strongly disagree” to 5= “strongly agree”. A high average score indicated a high level of death anxiety among the participants. The original questionnaire’s internal reliability was 0.76 Cronbach’s alpha and in the current study, it was 0.80 Cronbach’s alpha.
The internal reliability for the translated inventory, as estimated by Cronbach’s alpha coefficient, was 0.80 for the entire scale. In the current study, the internal reliability was 0.83 Cronbach’s alpha. Due to the high reliability rate of the entire scale, we used the mean and standard deviation (SD) of the entire scale in the statistical analysis.
Burnout was measured using the Maslach Burnout Inventory (MBI).19 The inventory includes 25 items, rated on a 7-point Likert scale from 0= “not at all” to 6= “all the time”. The Burnout Inventory is divided into three subscales: emotional exhaustion, depersonalization, and personal accomplishment. The higher the participant’s average score, the higher is his/her self-reported level of burnout. The internal reliability for the inventory as estimated by Cronbach’s alpha coefficient was 0.80 for the entire scale. In the current study, the internal reliability was estimated at 0.83 Cronbach’s alpha.
Data were collected at three points in time: approximately 2 months after the Second Lebanon War (as a part of data for another study concerning work immigrants that was conducted at that time), approximately 2 months after the Cast Lead Operation, and between 1 month and 2 months after the Protective Edge Operation. The questionnaire was administered in English and most of the participants were able to complete it on their own. Those who encountered difficulties while completing it received help from their friends (approximately 3% of participants).
Data was statistically analyzed using SPSS. The first statistical procedure conducted was to measure means, SDs, and Pearson correlations between the research variables. In the second stage of the analysis, we conducted three models of Linear Regression for each one of the dependent variables (burnout, intrusive memories, and level of stress).
The study was conducted according to the rules of the University of Haifa Ethics Committee.
Results
The means and the SDs for each of the research variables are presented in Table 2. The findings in Table 2 indicate high levels of social support among the participants as well as high levels of sense of mastery and self-esteem. The data pertaining to the study’s dependent variables revealed high levels of PTSD, high levels of death anxiety, and surprisingly low levels of burnout. To learn more about the association between the variable of exposure to military events and other independent variables and dependent variables, Pearson correlation tests were conducted. The findings are tabulated in Table 3.
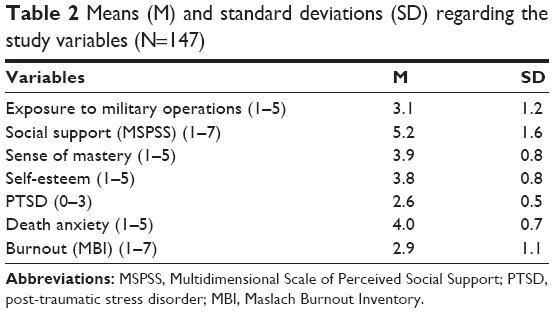 | Table 2 Means (M) and standard deviations (SD) regarding the study variables (N=147) |
 | Table 3 Pearson matrix correlations between the research variables |
As the data in Table 3 shows, associations were found between all the research variables. At this stage, three models of linear regression were conducted, for each of the dependent variables (PTSD, death anxiety, and burnout). Findings are listed in Table 4.
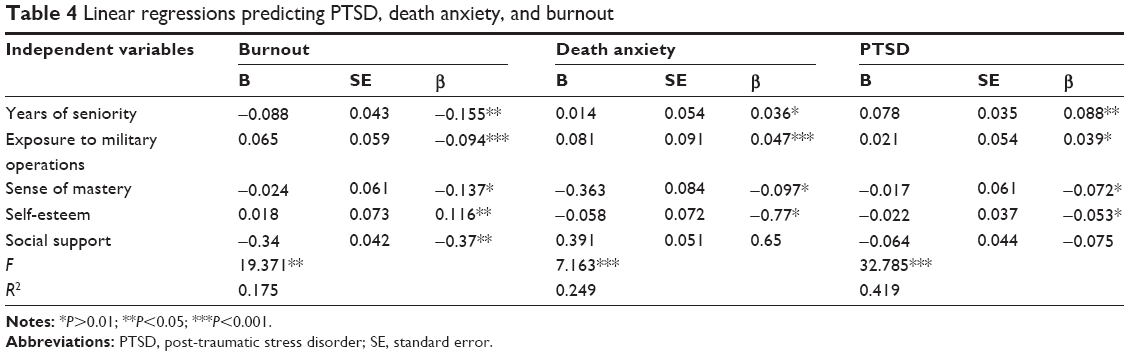 | Table 4 Linear regressions predicting PTSD, death anxiety, and burnout |
All three models rendered statistically significant results. The independent variables explained 41.9% of the variance of the PTSD levels, nearly 25% of the variance of death anxiety levels, and 17.5% of the variance of burnout levels. The exposure to military operations was significant in explaining both PTSD (β =0.039; P<0.01) and death anxiety (β =0.047; P<0.001).
To learn about the contribution of the research background and the study’s predictor variables on the levels of PTSD, death anxiety, and burnout among the participants, we utilized three models of two-step hierarchical regressions. In step 1, all of the independent variables were entered into the regression equation in all the three models. Step 2 was different for each of the models: in the first model, death anxiety and burnout were entered into the regression equation; in the second model, PTSD and burnout were entered into the regression equation; and in the third model, PTSD and death anxiety were entered into the regression equation. The findings are presented in Table 5.
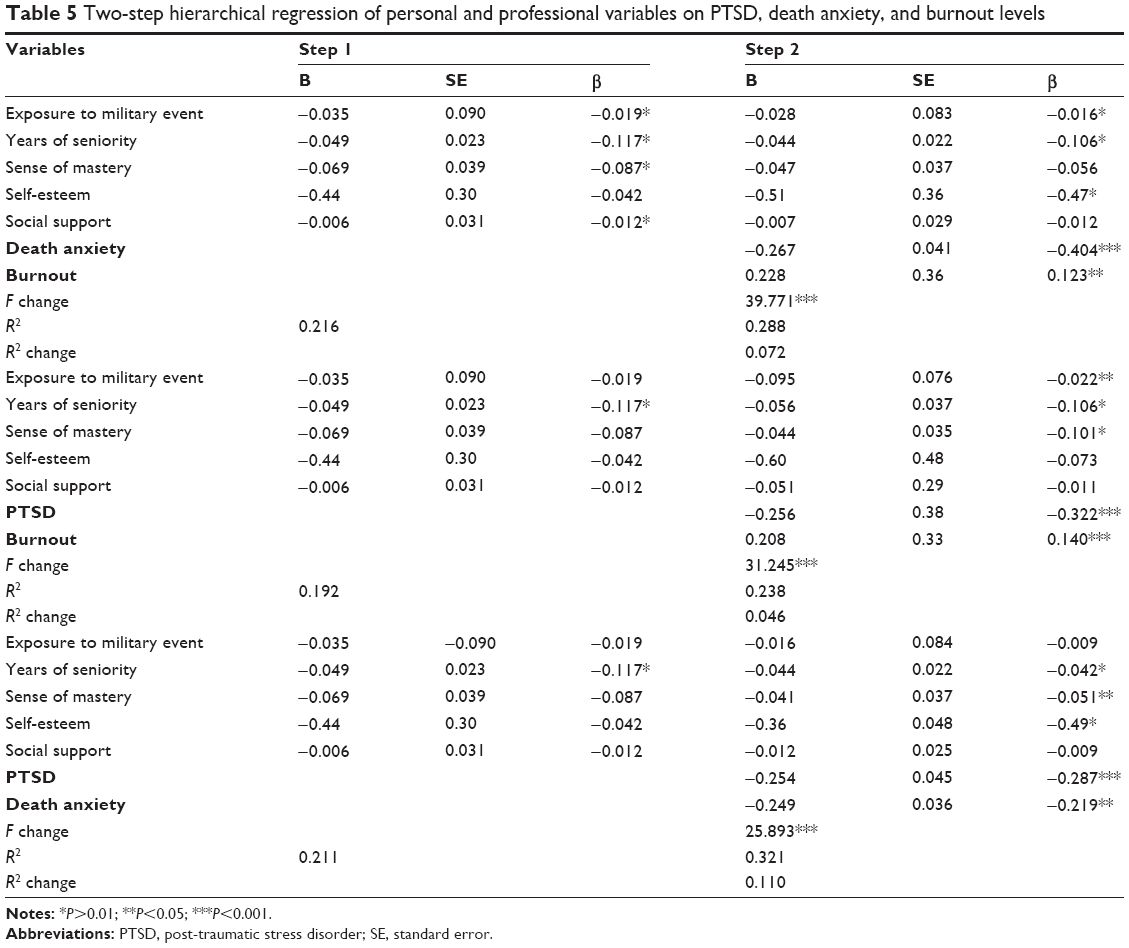 | Table 5 Two-step hierarchical regression of personal and professional variables on PTSD, death anxiety, and burnout levels |
As shown in Table 5, all three models rendered statistically significant findings. Death anxiety added 40.4% to the explained variance of the PTSD levels, the PTSD added 32.2% to the explained variance of the death anxiety levels, and 17.9% to the explained variance of the burnout levels.
Discussion
Philippine migrant care workers who came to Israel to find employment as personal and nursing aides to elderly people have become part of the general population in the country, sharing the difficulties inflicted by wars and military operations. The study findings show high levels of PTSD and of death anxiety among the participants. These levels can be explained in several ways. The first explanation relates to the fact that most Philippine migrant care workers had never experienced military events such as wars or military operations. They did not know what to expect, what they should fear, or how they should behave. The issue of alarms and sirens that are heard routinely in wartimes, the sounds of falling missiles, and the need to refrain from gathering in public places such as markets and public institutions all constituted new, strange, and terrifying experiences. When this type of event is experienced for the first time, it may certainly increase the individual’s level of anxiety, as is likely the case regarding the Philippine migrant care workers. Moreover, the fact that their job demanded that they continue functioning in a routine fashion increased the sense of stress, both during the event and afterward. Once they experienced such an event, they understood that military events are liable to occur again and again. They described post-traumatic symptoms, mostly those related to disrupted sleep and intrusive memories.
In addition, the high levels of death anxiety reported by the interviewees are related to their experiences during the military events. It is likely that people who find themselves in areas in which there are life-threatening events will begin to fear for their lives. It is also likely that the fear experienced by these people will intensify if they are responsible for the lives and welfare of their children, as was the case for several of the Philippine migrant care workers who participated in this study.20 An additional explanation for the high levels of PTSD is related to the socio-geographic structure in Israel. In general, civilians’ exposure to military operations is very high in Israel, as it is a very small country, and the population has the characteristics of a close-knit community. Hence, news of such events travels fast and affects everyone, either directly or indirectly. The immediacy and intensity of exposure creates an atmosphere of angst that engulfs the entire population, and almost no one remains detached.
The current research results are somewhat similar to those of other studies, which have claimed that working in a trauma zone and with traumatized clients and simultaneously experiencing the exposure to the traumatizing event often increases the level of personal stress. In these studies, stress was manifested by various symptoms, including PTSD, found among social workers,21,22 and among hospital nurses.23,24 Fullerton et al8 found that rescue workers exposed to a disaster reported significantly higher levels of ASD and PTSD than did a control group of workers who were not exposed to the event. Moreover, these studies found that rescue workers with previous disaster exposure were 6.77 times more likely to develop PTSD.
Contrary to the current study, some studies have claimed that working with traumatized clients and the exposure to traumatic events often decreases personal stress levels, as manifested in PTSD symptoms.3,4,25
It may be assumed that the degree of exposure to traumatic events, in terms of their number and intensity, is an important factor in the current study as well. Philippine migrant care workers undergo a process of adapting to a new culture that is entirely different from the one they come from. Often, female Philippine migrant care workers opt to leave their family members behind, even when it comes to young children who are still in need of their mother. In addition, the arrangement of living and sharing a household with the elderly person under one’s care is another type of stressor. All in all, it seems that Philippine migrant care workers continuously experience life events that are far from simple for them. In addition, it may be assumed that sharing a routine with elderly people who are prone to experience higher levels of PTSD also affects the level of PTSD symptoms of the aides who care for them.20 Another explanation for the high levels of PTSD demonstrated by Philippine migrant care workers can be based on sex. Several studies have indicated differences between men and women in terms of the level of post-traumatic symptoms, whereby women reported higher levels of the symptoms than did men.7,26 The study of Ron (accepted in Journal of Traumatology) about PTSD symptoms among members of three generations of Arabs and Jews in Israel following the very same wars and military operations that affected the participants of the current study found that women, both Jewish and Arab, in all three generations, experienced higher levels of PTSD than did the male participants.27 Although women are less frequently exposed to the frontline events of wars or military operations than men, they experience higher levels of post-traumatic symptoms and develop PTSD more frequently than do men.7,26,28 It is important to note that the current study, like many others before it, did not enable the researcher to determine whether the higher levels of post-traumatic symptoms among women were related to women’s tendency to reveal their emotions or whether women are in fact more sensitive to traumatic events such as war.
Death anxiety should be explored in terms of its content and to detect whether men and women in fact imbue this concept with different content, suggesting that essentially, the difference in men’s and women’s responses is not related to levels of death anxiety, but rather to its content. The current study did not include male migrant care workers; hence, a comparison related to the sex variable was not possible. Consequently, future studies should further examine the issue of death anxiety among female and male migrant care workers.
Findings also demonstrated that the more exposure participants had to events such as military operations or wars, the lower were their levels of burnout, as indicated by an inverse correlation. Given the absence of research regarding the effects of war and military events on semiprofessional immigrant populations, we approached this issue by examining its effect on professionals in the field of nursing. In general, burnout has been equated with alienation, anxiety, loss of idealism, and loss of hope in response to stress.29,30 Nursing is considered a helping profession that entails a very high risk of burnout, since it is very much a client-oriented profession, and nurses are involved in complex life-and-death situations. Ron and Shamai4 found high levels of burnout among hospital nurses working under the same circumstances of war and military operations. Moreover, Hare et al,31 in one of the first studies on the work stressors of nursing assistants in nursing homes, compared the levels of burnout among nurses and certified nursing assistants and found higher burnout and depersonalization rates among the latter. The study also found that nursing assistants had more negative attitudes and less empathy toward the elderly patients than did the nurses.32 Other studies found that levels of stress,33 fatigue, and disrupted sleeping patterns were higher among nursing assistants than among other health care workers. This was most evident among those treating elderly individuals with cognitive deficiencies or impairments.
In contrast to the findings of the mentioned studies,29,31,33 participants of the current study reported low levels of burnout, despite having to perform similarly demanding tasks under the difficult conditions of exposure to potentially traumatic events. These divergent results cannot be easily explained, for the following reasons: 1) as far as we know, no previous research has studied the phenomenon of burnout among migrant care workers caring for elderly individuals in times of war; 2) in all of the above-mentioned studies29–33 regarding burnout, participants worked in nursing homes and their positions involved working in shifts. By contrast, in the present study, the focus is on personal or nursing aides living in elderly people’s private homes and providing around-the-clock care, thus filling a function similar to that of a family member; 3) in an Israeli study about nursing assistants’ work stressors and the connection to the workers’ well-being, findings indicated low levels of well-being among nursing-home workers.14 One of the conclusions was that most of the nursing assistants in Israel are well-educated and over-qualified women immigrants from the former Soviet Union, who worked as physicians in their former homeland; their inability to find work suitable to their professional training and personal skills was a factor that increased their feelings of frustration. Philippine migrant care worker women, on the other hand, are not well-educated and their only reason for coming to Israel is the need to earn money.
Given that in the current study the social support variable was found to be significant and inversely related to the levels of burnout, it appears that one of the explanations for the low levels of burnout may be the migrant workers’ support networks. These networks include several spheres, such as the social sphere, which includes all migrant workers from the Philippines. These women have established for themselves social frameworks in which they meet on a regular basis, often in apartments that have been converted to churches. On Sundays, their free day, they meet with their friends, attend services related to their faith – which also fortifies them, and share and exchange information about their current situation and their families back home.34 Another support sphere is the dyadic cycle that is created between the caregiver and the elderly person who is the care recipient. Occasionally this is a triad. It should be noted that the caregiver and the care recipient live together day in and day out in an apartment; they run the household together and share with each other the good days and the bad days. Philippine migrant care workers understand the codependency between them and the elderly person under their care, so that this relationship quickly becomes reciprocal and includes an emotional aspect and active cooperation.2 The third sphere of support is the extended family of the elderly care recipient and the extended family of the caregiver. If the relationship develops in a positive manner, reciprocal interactions help the Philippine migrant care workers avoid burnout, as there is no aspect of depersonalization, no role conflict, and no sense of helplessness, all of which might have contributed to burnout. This finding should be further examined in future studies.
As regards internal personal variables, the findings of the study suggest the existence of an inverse relationship between PTSD, death anxiety, and burnout on one hand, and the variables of self-esteem and sense of mastery on the other hand. These findings support those demonstrated in the literature, which claim that self-esteem and sense of mastery are related to an individual’s ability to cope with stress and, thus, these factors impact the development of post-traumatic reactions and general distress.35,36 In addition, an analysis of the findings of the current study suggests that the sense of the mastery variable is the strongest predictor of levels of post-traumatic stress symptoms. This finding suggests that this internal personal characteristic serves as a protective factor following exposure to a stressful event, as suggested in the literature,37 and can help individuals withstand traumatic events.
Regarding death anxiety, the findings of the current study show differences between the levels of self-esteem and sense of mastery and the experience of death anxiety. These findings are in line with those presented in professional literature.38–40 Security conditions in Israel entail many dangers, due to the fact that neighboring countries threaten Israel’s existence, as evidenced by the relatively frequent terror attacks and the intermittent wars. Consequently, it is possible that some individuals who do not feel a complete sense of mastery or control over their lives perceive themselves as weak when encountering the source of stress, and believe that in regard to national security, all control is in the hands of fate. Typically, in wartime, when there is a pervasive awareness of the immediacy of death, and civilians have almost no ability to influence the events that unfold, their level of general anxiety increases, as does their level of death anxiety. However, these same feelings of an imminent fate beyond one’s control can also have a releasing effect, even if only to a limited extent, freeing the individual from the fear of death and resulting in lower levels of death anxiety.
The unique circumstances of the current study can supply an additional explanation for the negative relationship between death anxiety and self-esteem and sense of mastery. The fact that this relationship was examined in wartime, which in itself is characterized by extreme lack of control, rather than in routine times, also had an effect on the findings. Indeed, during the Second Lebanon War, the Cast Lead Operation, and Protective Edge Operation, the home front was under daily attack, which persisted during most hours of the day, and it was impossible to predict where and when the next missile would fall and who would be the next one to be injured – perhaps mortally so. It may be assumed that for individuals with high self-esteem and high sense of mastery, this situation created a cognitive dissonance between their high self-esteem and sense of mastery and the chaotic situation in which they found themselves. This gap between the individual’s inner feelings and the external reality can lead to high levels of anxiety, in general, and death anxiety, in particular.
It is important to note that in the majority of studies that deal with death anxiety, this variable is examined in times of routine rather than in times of crisis, emergency, or war. It is possible that the difference between the current study’s findings and those of previous studies in the field is related to the fact that in the current study, death anxiety was assessed a short while after the military events and the context of the questionnaires were related to the effect of these events. This explanation should be further examined, in order to understand the ways in which a traumatic event affects the relationship between the variables of self-esteem and sense of mastery and the individual’s level of death anxiety.
Research limitations
The study has several limitations. The study was conducted at three different points in time and investigated the reactions of female migrant care workers from the Philippines who lived in Israel and experienced the effects of the three military operations described herein. It may be assumed that their reactions after each of the military events were different, yet the direction of change is unknown. They may have developed a certain degree of resilience to stress and situations of post-trauma or, conversely, their levels of stress and trauma might have increased from one event to the next. It is recommended that future studies investigate the nature of the change in reactions over time.
An additional limitation has to do with the size of the study, as a group of 147 participants cannot be considered a representative number for this population. However, it should be noted that the subject of the study itself could have raised the participants’ levels of stress, especially after the Second Lebanon War (the earliest of the three military events they experienced). It is important to acknowledge the positive contribution of those migrant care workers who agreed to participate and to conduct additional studies with larger groups in the future.
Disclosure
The author reports no conflicts of interest in this work.
References
Agbayani-Siewert P. Assumptions of Asian of Asian American similarity: the case of Filipino and Chinese American students. Soc Work. 2014;49:213–234. | ||
Ron P. From “employer–employee” to “family of choice”: the development of the relationship between Philippine worker immigrants and elderly care recipients. Adv Aging Res. 2015;2:47–57. [accepted]. | ||
Ron P, Shamai M. Challenging secondary traumatization and burnout: the impact of ongoing national terror on social workers. Soc Work Res. 2011;35(1):36–45. | ||
Ron P, Shamai M. The impact of ongoing national terror on nurses in Israel. Comm Ment Heal. 2013;50(3):354–361. | ||
Stern J. The Ultimate Terrorists. Cambridge, MA: Harvard University Press; 1999. | ||
Nuttman-Shwarts O, Dekel R. Challenges for students working in a shared traumatic reality. Br J Soc Work. 2007;39(3):522–538. | ||
Cohen M. Acute stress disorder in older, middle-aged and younger adults in reaction to the Second Lebanon war. Int J Geriatr Psychiatry. 2008;23:34–40. | ||
Fullerton CS, Ursano RJ, Wang L. Acute stress disorder, posttraumatic stress disorder and depression in disaster or rescue workers. Am J Psychiatry. 2004;161(8):1370–1376. | ||
Gidron Y. Post-traumatic stress disorder after terrorist attacks: a review. J Nerv Mental Dis. 2002;190:118–121. | ||
Tuval-Mashiach R, Shalev AY. Epidemiology of psychological reactions to terror among adults in Israel. In: Zomer E, Bleich A, editors. Mental Health in Terror’s Shadow: The Israeli Experience. Israe: Pardes Publication; 2005:29–54. [Hebrew]. | ||
Dipolar SJ, Griffin M, Young JR, Neimeyer RA. Death anxiety and attitudes toward the elderly among older adults: the role of gender and ethnicity. Death Stud. 2003;27:335–354. | ||
Freudenberger HJ, Richelson G. Burnout: The High Cost of Achievement. Garden City, NY: Anchor Press; 1980. | ||
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JF. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987–1993. | ||
Ron P. The relations between work stressors and well-being among nursing assistants in nursing homes. Aging Clin Exp Res. 2008;20(4):359–367. | ||
Zimmet GD, Dahlin NW, Zimmet SG, Farley KG. The multidimensional scale of perceived social support. J Pers Assess. 1988;52:3. | ||
Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978;19:2–21. | ||
Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press; 1965. | ||
Carmel S, Mutran E. Preferences for different life-sustaining treatments among elderly person in Israel. J Gerontol. 1997;52B:S97–S102. | ||
Maslach C, Jackson SE. Maslach Burnout Inventory. Palo Alto, CA: Consulting Psychologist Press; 1981. | ||
Kelly TA. The role of religion, spirituality, and faith-based community in coping with acts of terrorism. In: Bongar BM, Brown LM, Beutler LE, Zimbardo PG, editors. Psychology of Terrorism. Oxford, UK: Oxford University Press; 2007:137–152. | ||
Adams RE, Figley CR, Boscarino JA. The compassion fatigue scale: its use with social workers following urban disaster. Res Soc Work Pract. 2008;18:238–250. | ||
Ben-Ezra M, Palgi Y, Essar N. Impact of war stress on posttraumatic stress symptoms in hospital personnel. Gen Hosp Psychiatry. 2007;29:264–266. | ||
Dekel R, Hantman S, Ginzburg K, Solomon Z. The cost of caring? Social workers in hospitals confront ongoing terrorism. Br J Soc Work. 2007;37:1247–1261. | ||
Essar N, Palgi Y, Saar R, Ben-Ezra M. Association between posttraumatic symptoms and dissociative symptoms in rescue personnel 96 hours after the Hilton hotel bombing in Sinai, Egypt. J Psych Trauma. 2007;6:49–56. | ||
Arvay MJ. Secondary traumatic stress among trauma counselors: what does the research say? Int J Adv Couns. 2001;23:283–293. | ||
Bleich A, Gelkopf M, Melamed Y, Solomon Z. Mental health and resiliency following 44 months of terrorism: a survey of an Israeli national representative sample. BMC Med. 2006;4(21):1–11. | ||
Ron P. Post-traumatic stress disorder among three generations families in times of war: a comparison between Israeli Jews and Arabs after the Second Lebanon War (2006) and cast lead operation (2009). Traumatology. 2006;20(4):269–276. | ||
Abdel-Khalek AM, Al-Kandari Y. Death anxiety in Kuwaiti middle-aged personal. Omega. 2007;55(4):297–310. | ||
Maslach C. Burnout – The Cost of Caring. Englewood Cliffs, NJ: Prentice-Hall; 1982. | ||
Soderfeldt M, Soderfeldt B, Warg LE. Burnout in social work. Soc Work. 1995;40:638–646. | ||
Hare J, Pratt CC, Andrews D. Predictors of burnout in professional and paraprofessional nurses working in hospitals and nursing homes. Int J Nurs Stud. 1995;25(2):105–115. | ||
Astrom S, Nillson M, Norberg A, Sandman PO, Winblad B. Staff burnout in dementia care – relations to empathy and attitudes. Int J Nurs Stud. 1999;28(1):65–75. | ||
Estryn-Behar M, Kaminski M, Peigne E, et al. Stress at work and mental health status among female hospital workers. Br J Ind Med. 1990;47:20–28. | ||
Plante TG, Canchola EL. The association between strength of religious faith and coping with American terrorism regarding the events of September 11, 2001. Pastoral Psychol. 2004;52(3):269–278. | ||
Ben-Zur H. Personal resources of mastery-optimism, and communal support beliefs, as predictors of posttraumatic stress in uprooted Israelis. Anxiety Stress Coping. 2008;21(3):295–307. | ||
Benight CC, Harper ML. Coping, self-efficacy perceptions as a mediator between acute stress response and long term distress following natural disasters. J Trauma Stress. 2002;15(3):177–186. | ||
Bonnano GA, Rennick C, Dekel S. Self-enhancement among high-exposure survivors of the September 11th terrorist attack: resilience or social maladjustment? J Pers Soc Psychol. 2005;88(6):984–998. | ||
Buzzanga VL, Miller HR, Perne SE, Sander JA, Davis SF. The relationships between death anxiety and level of self-esteem: a reassessment. Bull Psychon Soc. 1989;27(6):570–572. | ||
Cicirelli VG. Fear of death in older adults predictions from terror management theory. J Gerontol B Psychol Sci Soc Sci. 2002;57(4):358–366. | ||
Davis SF, Bremer SR, Anderson BJ, Tramill JL. The interrelationships of ego strength, self-esteem, death anxiety, and gender in undergraduate college students. J Gen Psychol. 1983;108(1):55–59. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.