")
Back to Journals » Drug Design, Development and Therapy » Volume 12
Inhibitory effect of celecoxib on agomelatine metabolism in vitro and in vivo
Authors He JY, Fang P, Zheng X, Wang CC , Liu TH, Zhang BW, Wen J, Xu RA
Received 19 December 2017
Accepted for publication 31 January 2018
Published 9 March 2018 Volume 2018:12 Pages 513—519
DOI https://doi.org/10.2147/DDDT.S160316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Jiayang He,1 Ping Fang,2 Xiang Zheng,2 Chenchen Wang,2 Tenghui Liu,2 Bowen Zhang,2 Jian Wen,2 Ren-ai Xu3
1Department of Pharmacy, The First Hospital of Jiaxing, Jiaxing, Zhejiang, China; 2Department of Pharmacology, School of Pharmacy of Wenzhou Medical University, Wenzhou, Zhejiang, China; 3Department of Pharmacy, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, China
Aim: The aim of this study was to study the effect of celecoxib on agomelatine metabolism in vitro and in vivo.
Methods: Ten healthy male Sprague–Dawley rats were randomly divided into 2 groups: Group A (control group) and Group B (30 mg/kg celecoxib). Then a single dose of 20 mg/kg agomelatine was administered orally 30 min after administration of celecoxib. In an in vitro study, celecoxib with a series of concentrations was added to an incubation mixture containing recombinant human CYP2C9, human or rat liver microsomes to determine the half-maximal inhibitory concentration on the metabolism of agomelatine. Moreover, a mechanism study was performed to determine the inhibitory effect of celecoxib on CYP2C9.
Results: The results showed that a single dose of 30 mg/kg celecoxib significantly increased the area under the concentration-time curve and maximum concentration of agomelatine. In addition, celecoxib inhibited the metabolism of agomelatine in the in vitro studies, which was determined to be by a competitive mechanism on CYP2C9. Those results indicated that celecoxib has an inhibitory effect on the metabolism of agomelatine both in vivo and in vitro.
Conclusion: Thus, more attention should be paid when celecoxib is administered combined with agomelatine.
Keywords: agomelatine, liver microsomes, pharmacokinetics, celecoxib, CYP2C9
A Letter to the Editor has been received and published for this article.
Introduction
Depression is a prevalent, recurrent, and disabling mental disorder with high rates of morbidity and mortality, which plagues millions of people over lifetime worldwide.1,2 According to the estimation of the World Health Organization, depression will be the second leading cause of global disease burden and the first cause of disability-adjusted years all over the world in the near future.3,4 Agomelatine is a novel antidepressant with a dual mechanism of action: melatonin MT1 and MT2 agonist and 5-hydroxytryptamine 2C receptors antagonist.5–7 In 2009, agomelatine was approved by the European Union for the treatment of major depressive episodes in adults.8 And owing to the double interaction of 2 mechanisms, agomelatine has broad efficacy in different psychopathological conditions with reduced side effects and superior tolerability profile, such as low sexual dysfunction, lack of withdrawal syndrome, and less sleep problems.9–12 Agomelatine is mainly metabolized by hepatic CYP1A2 and CYP2C9 to its main metabolites, 3-hydroxy-agomelatine and 7-desmethyl-agomelatine.13
Celecoxib, as the first selective cyclooxygenase-2 inhibitor, is a nonsteroidal anti-inflammatory drug used for the treatment of rheumatoid arthritis, osteoarthritis, and familial adenomatous polyposis.14,15 Some in vitro studies had indicated that celecoxib is mainly metabolized by CYP2C9 and CYP3A4.16,17 It has been reported that celecoxib has therapeutic effects on varying degrees of depression. More and more studies are now showing that depression and inflammation have bidirectional effects, in which depression facilitates inflammatory response and inflammatory response promotes depression.3,14,18,19 So, celecoxib and agomelatine may be used in combination. Moreover, they are both metabolized by CYP2C9. Therefore, there is potential for drug–drug interactions (DDIs) between celecoxib and agomelatine. These interactions might lead to serious adverse events. Although Werner et al reported that celecoxib can inhibit the metabolism of CYP2D6 substrates, no published studies have evaluated the effect of celecoxib on agomelatine metabolism.20
In this study, in order to ensure the safety and effectiveness after the concurrent use of celecoxib and agomelatine, we investigated the effect of celecoxib on the pharmacokinetics of agomelatine in rats. Moreover, the effect of celecoxib on agomelatine in recombinant human CYP2C9*1, human and rat liver microsomes was also identified.
Materials and methods
Enzymes and chemicals
Recombinant human CYP2C9 and cytochrome b5 were kind gifts from Beijing Hospital (Beijing, China). Pooled human liver microsomes (HLMs) from donors were purchased from Gentest (Woburn, MA, USA). Agomelatine and its metabolite 7-desmethyl-agomelatine were purchased from Tokyo Chemical Industry Co., Ltd (Tokyo, Japan), and celecoxib was obtained from Shanghai Canspec Scientific Instruments Co., Ltd (Perfemiker, Shanghai, China). Carbamazepine used as the internal standard (IS) was purchased from Sigma-Aldrich Company (St Louis, MO, USA). The reduced nicotinamide adenine dinucleotide phosphate (NADPH) was from Roche Pharmaceutical Ltd (Basel, Switzerland). Formic acid (FA, 98% purity) of liquid chromatography (LC) grade was from J&K Scientific Ltd. (Shanghai, China). LC grade acetonitrile, methanol, and isopropanol were purchased from Merck (Darmstadt, Germany). Ultrapure water was freshly purified by a Milli-Q A10 System (Millipore, Billerica, MA, USA). All the other chemicals and solvents used were of the analytical grade commercially available.
Instrumentation and operation conditions
The concentrations of agomelatine were quantified using a Waters ACQUITY UPLC system (Waters Corp., Milford, MA, USA) coupled to a XEVO TQD triple quadrupole tandem mass spectrometer (Waters Corp.) with an electrospray ionization (ESI+) interface. Chromatographic separations were performed on an ACQUITY BEH C18 column (2.1×50 mm, 1.7 μm) with a C18 inline 0.2 mm stainless steel frit filter (Waters Corp.). The mobile phases consisted of water containing 0.1% FA and acetonitrile with isocratic elution in the ratio of 45:55. The flow rate was 0.3 mL/min with the injection volume of 2 μL. Mass spectrometric detection for quantitation by multiple reaction monitoring was performed on a XEVO TQD triple quadrupole mass spectrometer in the positive mode. The transitions were m/z 244.1 → 185.2, m/z 230.1 → 171.0, and m/z 237.1 → 194.2 for agomelatine, 7-desmethyl-agomelatine, and carbamazepine, respectively.
Rat liver microsomes
Liver obtained from 5 untreated rats were weighed and homogenized with cold 0.01 mM PBS containing 0.25 mM sucrose; the homogenates were centrifuged at 11,000 rpm for 15 min. The supernatants were then transferred to a new tube and centrifuged at 11,000 rpm for 15 min again. The supernatants were then ultra-centrifuged at 100,000 × g for 1 h. The microsomal pellets were resuspended with cold 0.01 mM PBS and stored at −80°C.21 Protein concentrations were determined by Bradford Protein Assay Kit (Thermo Scientific, Waltham, MA, USA).
Effects of celecoxib on the metabolism of agomelatine in human and rat microsomes
The incubation mixture contained HLMs or rat liver microsomes, 1 M potassium phosphate buffer (pH 7.4), agomelatine (100 μΜ; approximately the Km of human and rat liver microsomes), celecoxib (0, 0.01, 0.1, 1, 10, 50, and 100 μM) and 1 mM NADPH. Incubations were initiated following a 5 min preincubation in a shaking water bath at 37°C and then NADPH was added to start the reaction in a final volume of 200 μL. The mixture was incubated at 37°C for 50 min and terminated by cooling to −80°C immediately. Then 400 μL acetonitrile and 20 μL carbamazepine (IS, 400 ng/mL) were added. After vortex mixing for 2 min, the tubes were centrifuged at 13,000 rpm for 10 min. The supernatant was diluted 1:1 with water and 2 μL mixture was injected for analysis.
Effects of celecoxib on the metabolism of agomelatine in CYP2C9*1
Recombinant microsomes expressing CYP2C9 variants generated in Spodoptera frugioerda 21 insect cells were obtained according to the previously reported methods.22 The incubation mixture consisted of 5 pmol recombinant insect microsomes CYP2C9*1, 5 pmol purified cytochrome b5, 100 mmol Tris-HCl buffer (pH 7.4), agomelatine (50 μM for CYP2C9*1), inhibitor (celecoxib, 0–100 μM), and 1 mM NADPH. Different concentrations of celecoxib were added to a 200 μL reaction mixture to determine the half-maximal inhibitory concentration (IC50). In addition, in order to study the mechanism of inhibitory effect of celecoxib on agomelatine metabolism, final concentration of agomelatine ranged from 2.0 to 100 μM (2.0, 5.0, 10, 20, 50, and 100) and different concentrations of celecoxib (0, 5.0, and 10 μM) were added to a reaction mixture containing 5 pmol CYP2C9*1.
In vivo pharmacokinetic studies
Male Sprague–Dawley rats (250–280 g) obtained from Laboratory Animal Center of Wenzhou Medical University (Wenzhou, China) were used to study the pharmacokinetic interaction of agomelatine and celecoxib. All experimental procedures and protocols were reviewed and approved by the Animal Care and Use Committee of Wenzhou Medical University and were in accordance with the Guide for the Care and Use of Laboratory Animals.
Ten SD rats were divided randomly into 2 groups: the control group (Group A, n=5) and the study group (Group B, n=5). Food was prohibited for 12 h before administration but the rats had free access to water. Agomelatine and celecoxib were dissolved in 0.5% sodium carboxy methyl cellulose (CMC-Na) solution. The Group B was treated with 30 mg/kg celecoxib, while the Group A with equivalent amount of 0.5% CMC-Na. Then 20 mg/kg agomelatine was administered half an hour later. Blood samples were collected via tail vein to 1.5 mL centrifuge tube at the time points of 0.083, 0.25, 0.5, 0.75, 1, 2, 4, 6, 8, 12, and 24 h after oral administration of agomelatine. After centrifuging at 12,000 rpm for 10 min, plasma samples were immediately separated from whole blood and frozen at −80°C until analysis.
Statistical analysis
Data were expressed at the mean ± SD. The noncompartmental analysis was used to calculate the pharmacokinetic parameters by DAS version 3.0 (Bontz Inc., Beijing, China). The average plasma concentration time curve was plotted with Origin 8.0 (Originlab Company, Northampton, MA, USA). The IC50 was calculated with GraphPad (Version 5; Graphpad Software Inc., San Diego, CA, USA). Statistical comparisons of main pharmacokinetic parameters within each group were carried out with the Statistical Package for the Social Sciences (version 17.0; SPSS Inc., Chicago, IL, USA) by one-way analysis of variance for repeated measures coupled with the Dunnett’s test. In all cases, P-values <0.05 was considered to be of statistical significance.
Results
Effects of celecoxib on the metabolism of agomelatine in human and rat liver microsomes
As shown in Figure 1, when maximum concentration of celecoxib (100 μM) was used, celecoxib inhibited metabolism rate in CYP2C9*1, HLM, and rat liver microsome by 3.17%, 36.60%, and 23.43%, respectively. Moreover, the IC50 for inhibition activity in CYP2C9*1 was 20.10 μM, while it was 71.41 and 130.1 μM in human and rat liver microsomes (Figure 2).
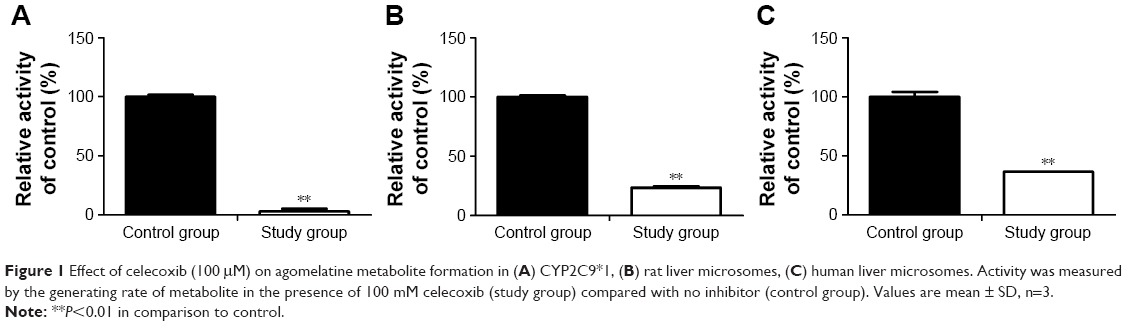 | Figure 1 Effect of celecoxib (100 μM) on agomelatine metabolite formation in (A) CYP2C9*1, (B) rat liver microsomes, (C) human liver microsomes. Activity was measured by the generating rate of metabolite in the presence of 100 mM celecoxib (study group) compared with no inhibitor (control group). Values are mean ± SD, n=3. |
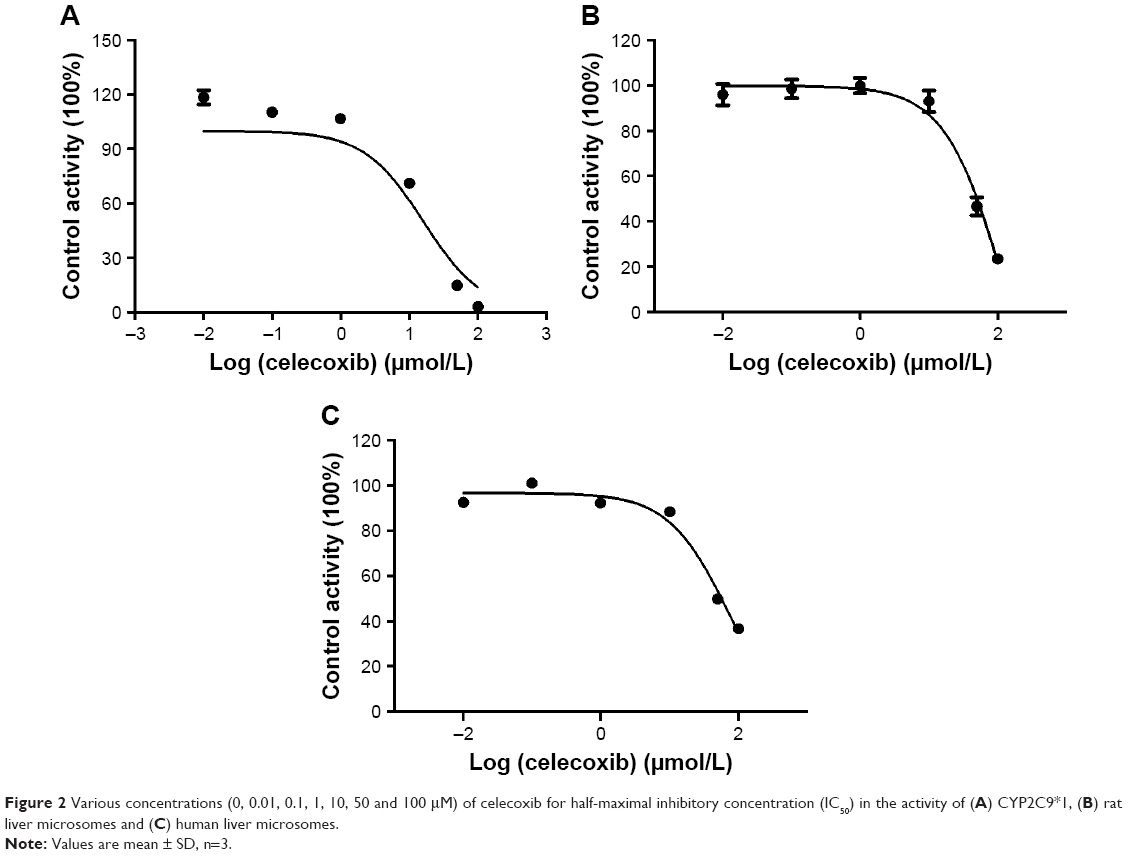 | Figure 2 Various concentrations (0, 0.01, 0.1, 1, 10, 50 and 100 μM) of celecoxib for half-maximal inhibitory concentration (IC50) in the activity of (A) CYP2C9*1, (B) rat liver microsomes and (C) human liver microsomes. |
Effects of celecoxib on the pharmacokinetics of agomelatine in rats
The mean pharmacokinetic parameters of agomelatine administered alone (Group A) and in combination with celecoxib (Group B) were calculated by DAS 3.0, and the statistical analysis results are presented in Table 1. Mean plasma concentration-time curves of agomelatine in 2 groups are presented in Figure 3.
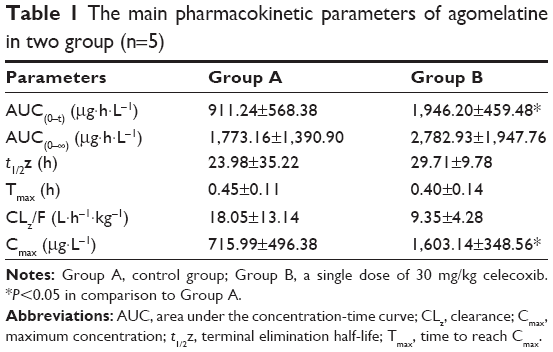 | Table 1 The main pharmacokinetic parameters of agomelatine in two group (n=5) |
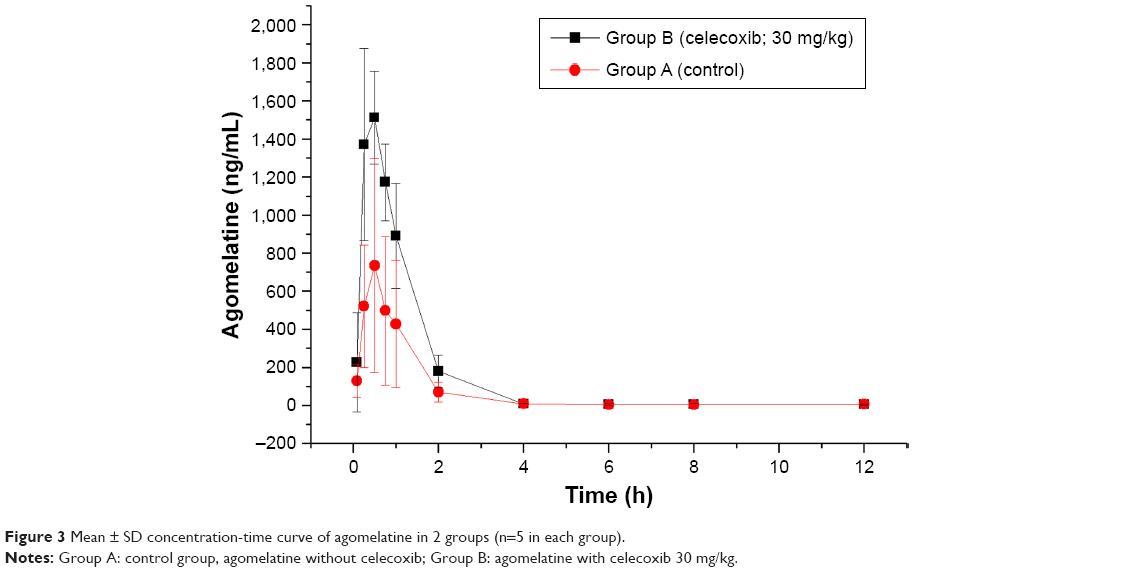 | Figure 3 Mean ± SD concentration-time curve of agomelatine in 2 groups (n=5 in each group). |
The mean plasma concentration-time curve showed that it had the highest concentration of agomelatine in Group B, which was given celecoxib 30 mg/kg. When coadministered with celecoxib, the maximum concentration and area under the concentration-time curve (Cmax and AUC(0–t)) of agomelatine were significantly increased compared with those of the control group.
Mechanism explaining the effect of celecoxib on CYP2C9 enzyme activity
The mechanism of celecoxib for the inhibitory effect on CYP2C9*1 activity was investigated by enzyme kinetic analysis. Lineweaver–Burk plots analysis indicated that celecoxib acts as a competitive inhibitor of CYP2C9 (Figure 4), the Km was 60.53 μM and Ki was 5.385 μM.
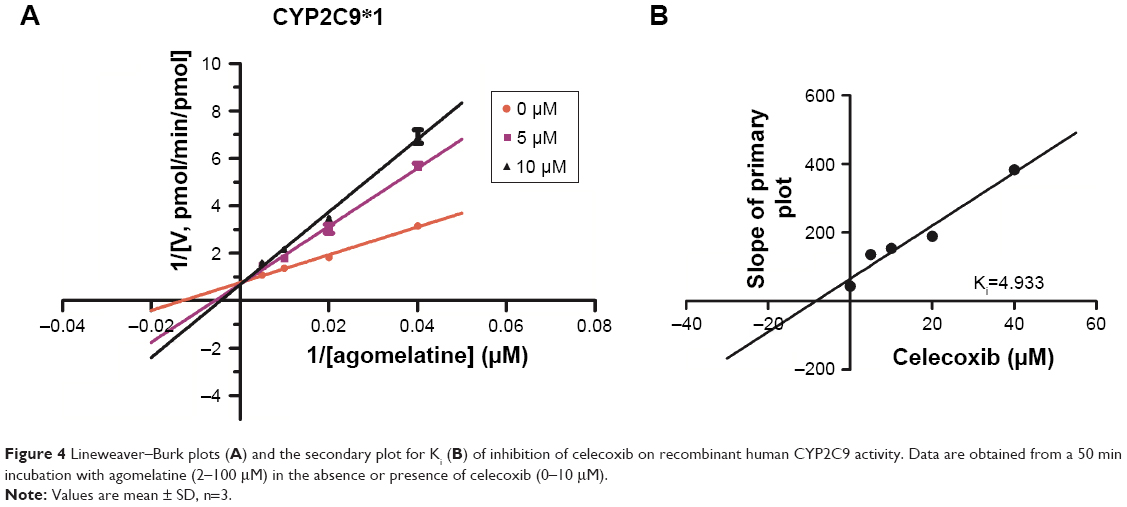 | Figure 4 Lineweaver–Burk plots (A) and the secondary plot for Ki (B) of inhibition of celecoxib on recombinant human CYP2C9 activity. Data are obtained from a 50 min incubation with agomelatine (2–100 μM) in the absence or presence of celecoxib (0–10 μM). |
Discussion
Agomelatine is mainly metabolized by CYP1A2 and CYP2C9.23 Drugs that inhibit or induce CYP1A2 and/or CYP2C9 activity could alter the pharmacokinetics of agomelatine. Especially, the inhibition of these metabolic enzymes may lead to an increased exposure of agomelatine. For example, fluvoxamine, a potent CYP1A2 and moderate CYP2C9 inhibitor, has the ability to inhibit the metabolism of agomelatine, resulting in an increase in agomelatine exposure.24 Given the possibility of coadministration of celecoxib with agomelatine and there being no studies that investigated the DDIs between these 2 drugs, it is important to evaluate the effect of celecoxib on the agomelatine metabolism. Our in vivo pharmacokinetic study showed that celecoxib (30 mg/kg) significantly increased the Cmax and AUC(0–t) of agomelatine compared with those of the control group. The results indicated that a single dose of celecoxib could inhibit the metabolism rate of agomelatine in vivo.
Moreover, several in vitro studies were also investigated to examine the inhibitory effect on the CYP2C9, human and rat liver microsomes. As shown in Figure 1, celecoxib at 100 μM significantly inhibited the metabolism of agomelatine in CYP2C9*1, human and rat liver microsomes. And in Figure 2, it showed that celecoxib inhibited agomelatine metabolism with IC50 of 20.10 μM for CYP2C9*1, 71.41 μM for HLM, and 130.1 μM for rat liver microsome. These results in vitro indicated that celecoxib exhibited an inhibitory effect on the metabolism of agomelatine in human CYP2C9, and human and rat liver microsome. These in vitro results support the pharmacokinetics study in vivo.
In addition, according to the previous report, we can know that agomelatine is mainly metabolized by CYP1A2 and CYP2C9, and celecoxib can inhibit the activity of CYP2D6,20 but the effect of celecoxib on other CYP enzymes, such as CYP2C9, is unknown. Thus, in order to explain the mechanism of the inhibition effect of celecoxib on agomelatine metabolism, we investigated the inhibitory effect on CYP2C9 activity in our vitro study. Enzyme kinetic analysis and Lineweaver–Burk plots analysis indicated that celecoxib competitively inhibited human CYP2C9 against substrate. Therefore, we infer that the increase in agomelatine exposure (Cmax and AUC(0–t)) may be caused by the inhibitory effect on CYP2C9 to a certain degree. However, given that CYP1A2 plays an important role in agomelatine metabolism, our further study should focus on whether celecoxib also has the inhibitory effect on CYP1A2 activity.
Conclusion
In summary, these findings demonstrate that coadministration of celecoxib could inhibit the metabolism of agomelatine in vivo and in vitro and alter some of its pharmacokinetic parameters (Cmax and AUC(0–t)). It is also indicated that celecoxib is a potential inhibitor of CYP2C9 and has competitive inhibitory mechanism. As the first study about the effect of celecoxib on agomelatine metabolism, it is significant in guiding clinical treatment when celecoxib and agomelatine are administered simultaneously.
Acknowledgments
This study was supported by the foundation of the First Hospital of Jiaxing. The authors are grateful to the members of the Beijing Institute of Geriatrics of the Ministry of Health and Laboratory of Clinical Pharmacology of Wenzhou Medical University for their advice and assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
Cameron C, Habert J, Anand L, Furtado M. Optimizing the management of depression: primary care experience. Psychiatry Res. 2014;220(Suppl 1):S45–S57. | ||
Wittenborn AK, Rahmandad H, Rick J, Hosseinichimeh N. Depression as a systemic syndrome: mapping the feedback loops of major depressive disorder. Psychol Med. 2016;46(3):551–562. | ||
Muller N, Schwarz MJ, Dehning S, et al. The cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in major depression: results of a double-blind, randomized, placebo controlled, add-on pilot study to reboxetine. Mol Psychiatry. 2006;11(7):680–684. | ||
Mathers CD, Stein C, Ma Fat D, et al. Global Burden of Disease 2000: Version 2 Methods and Results. Geneva: World Health Organization; 2002. | ||
Eser D, Baghai TC, Moller HJ. Agomelatine: the evidence for its place in the treatment of depression. Core Evid. 2010;4:171–179. | ||
Guardiola-Lemaitre B, De Bodinat C, Delagrange P, Millan MJ, Munoz C, Mocaer E. Agomelatine: mechanism of action and pharmacological profile in relation to antidepressant properties. Br J Pharmacol. 2014;171(15):3604–3619. | ||
Millan MJ, Gobert A, Lejeune F, et al. The novel melatonin agonist agomelatine (S20098) is an antagonist at 5-hydroxytryptamine2C receptors, blockade of which enhances the activity of frontocortical dopaminergic and adrenergic pathways. J Pharmacol Exp Ther. 2003;306(3):954–964. | ||
Green B. Focus on agomelatine. Curr Med Res Opin. 2011;27(4):745–749. | ||
Gargoloff PD, Corral R, Herbst L, Marquez M, Martinotti G, Gargoloff PR. Effectiveness of agomelatine on anhedonia in depressed patients: an outpatient, open-label, real-world study. Hum Psychopharmacol. 2016;31(6):412–418. | ||
Stein DJ, Ahokas A, Jarema M, et al. Efficacy and safety of agomelatine (10 or 25 mg/day) in non-depressed out-patients with generalized anxiety disorder: a 12-week, double-blind, placebo-controlled study. Eur Neuropsychopharmacol. 2017;27(5):526–537. | ||
Altinyazar V, Kiylioglu N. Insomnia and dementia: is agomelatine treatment helpful? Case report and review of the literature. Ther Adv Psychopharmacol. 2016;6(4):263–268. | ||
De Berardis D, Conti CM, Marini S, et al. Is there a role for agomelatine in the treatment of anxiety disorders?A review of published data. Int J Immunopathol Pharmacol. 2013;26(2):299–304. | ||
Liu X, Lu YF, Guan X, Zhao M, Wang J, Li F. Characterizing novel metabolic pathways of melatonin receptor agonist agomelatine using metabolomic approaches. Biochem Pharmacol. 2016;109:70–82. | ||
Alamdarsaravi M, Ghajar A, Noorbala AA, et al. Efficacy and safety of celecoxib monotherapy for mild to moderate depression in patients with colorectal cancer: a randomized double-blind, placebo controlled trial. Psychiatry Res. 2017;255:59–65. | ||
Kim SH, Kim DH, Byeon JY, et al. Effects of CYP2C9 genetic polymorphisms on the pharmacokinetics of celecoxib and its carboxylic acid metabolite. Arch Pharm Res. 2017;40(3):382–390. | ||
Tang C, Shou M, Mei Q, Rushmore TH, Rodrigues AD. Major role of human liver microsomal cytochrome P450 2C9 (CYP2C9) in the oxidative metabolism of celecoxib, a novel cyclooxygenase-II inhibitor. J Pharmacol Exp Ther. 2000;293(2):453–459. | ||
Tang C, Shou M, Rushmore TH, et al. In-vitro metabolism of celecoxib, a cyclooxygenase-2 inhibitor, by allelic variant forms of human liver microsomal cytochrome P450 2C9: correlation with CYP2C9 genotype and in-vivo pharmacokinetics. Pharmacogenetics. 2001;11(3):223–235. | ||
Kiecolt-Glaser JK, Derry HM, Fagundes CP. Inflammation: depression fans the flames and feasts on the heat. Am J Psychiatry. 2015;172(11):1075–1091. | ||
Shelton RC, Miller AH. Eating ourselves to death (and despair): the contribution of adiposity and inflammation to depression. Prog Neurobiol. 2010;91(4):275–299. | ||
Werner U, Werner D, Rau T, Fromm MF, Hinz B, Brune K. Celecoxib inhibits metabolism of cytochrome P450 2D6 substrate metoprolol in humans. Clin Pharmacol Ther. 2003;74(2):130–137. | ||
Wang Z, Sun W, Huang CK, et al. Inhibitory effects of curcumin on activity of cytochrome P450 2C9 enzyme in human and 2C11 in rat liver microsomes. Drug Dev Ind Pharm. 2015;41(4):613–616. | ||
Dai DP, Wang YH, Wang SH, et al. In vitro functional characterization of 37 CYP2C9 allelic isoforms found in Chinese Han population. Acta Pharmacol Sin. 2013;34(11):1449–1456. | ||
Sansone RA, Sansone LA. Agomelatine: a novel antidepressant. Innov Clin Neurosci. 2011;8(11):10–14. | ||
Madsen H, Enggaard TP, Hansen LL, Klitgaard NA, Brosen K. Fluvoxamine inhibits the CYP2C9 catalyzed biotransformation of tolbutamide. Clin Pharmacol Ther. 2001;69(1):41–47. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.