")
Back to Journals » Clinical Interventions in Aging » Volume 14
Illness representations of dementia: a scoping review
Authors Shinan-Altman S, Werner P
Received 3 November 2018
Accepted for publication 15 December 2018
Published 18 January 2019 Volume 2019:14 Pages 179—193
DOI https://doi.org/10.2147/CIA.S193316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Richard Walker
Shiri Shinan-Altman,1 Perla Werner2
1The Louis and Gabi Weisfeld School of Social Work, Faculty of Social Sciences, Bar Ilan University, Ramat Gan, Israel; 2Department of Community Mental Health, University of Haifa, Haifa, Israel
Abstract: As the number of persons with dementia grows, an increasing number of families, professionals, and laypersons will come into contact with persons with cognitive deterioration. Assessing dementia illness representations (IRs) among these groups may have great importance for understanding their responses to dementia. The purpose of this study was to summarize and critically review the literature on dementia IRs. A total of 25 articles that satisfied the inclusion criteria were identified. The review revealed that conceptually, research attention on dementia IRs has increased over the past several years as a result of changes in the notion of IRs and in the dementia discourse. Regardless of the population examined, dementia was mostly described as a chronic condition, presenting more cognitive than behavioral symptoms, and as being caused mainly by age, heredity, and abnormal brain changes. Methodologically, the area of dementia IRs is characterized by design, sample, and data collection weaknesses. Findings suggest that although the literature in the area of dementia and IRs is increasing, several conceptual and methodological limitations still have to be resolved in order to advance knowledge in the area. The research and clinical implications of these findings stress the importance of IRs in the area of dementia.
Keywords: dementia, illness representations, scoping review
Introduction
The Self-Regulation Model (SRM)1 is an empirically validated model for understanding beliefs and coping processes related to illness. The model describes the ways in which individuals perceive illness (cognitive illness representations [IRs]) and react to it emotionally (emotional representations). Cognitive IRs consist of seven dimensions of subjective beliefs about the illness2: Identity – perceptions of symptoms; Causes – the perceived causes of the symptoms; Timeline – beliefs about the course of the illness; Consequences – the perceived impact of the illness; Control – the perceived ability to control the illness; Illness coherence – the extent to which patients perceive that they understand the illness and its implications; and Cyclical timeline – beliefs about the temporal changeability of the illness. Emotional representations refer to the production of emotional responses to the disease, such as worry and anxiety.2 Overall, it has been shown that intervention programs, mapping and challenging maladaptive IRs, while at the same time forming alternative representations, can change both IRs and functioning, leading to improved psychosocial outcomes.3 Indeed, IRs have received considerable attention in the literature over the past several years in relation to a variety of diseases, such as cancer and chronic pain.3,4 However, surprisingly, only few studies have examined the concept in the area of dementia.
Dementia is an umbrella term encompassing a variety of diseases characterized by cognitive deterioration, with Alzheimer disease (AD) being the most common type of dementia.5 Accordingly, AD and other dementias are characterized by decline from a previously attained level of cognitive functioning.5 Over time, these cognitive changes compromise the person’s ability to manage everyday activities, leading to increased levels of dependency on those around them.6 Overall, studies examining the prevalence of dementia consistently show a remarkable increase over time in the number of persons affected,7 as well as in the costs of health care provided to persons with dementia and their caregivers.8 Moreover, lately increased attention is being paid to the prevention of dementia through the involvement in health behaviors aimed at decreasing and managing risk factors associated with its development.9 Given these developments and in light of the accumulated knowledge regarding other diseases and the associations between IRs and health behavior,10,11 it is surprising that up until now the topic has not been widely examined in relation to dementia.
To address this gap, we performed a scoping review, a method widely used to understand and summarize knowledge about complex concepts.12 This type of review provides a preliminary assessment of the potential size and scope of available research literature. It aims to identify the nature and extent of research evidence.13 Using this method, we will attempt to understand the development of the concept of IRs in the area of dementia, paying specific attention to conceptual, methodological, and clinical aspects. We hope this review will provide the basis for directing future research on this important subject.
Method
Search strategy
A computer-based literature search was performed to identify publications on the topic of dementia (including neurocognitive disorders, dementia, AD, mild cognitive impairment (MCI), cognitive deterioration, and cognitive decline) and IRs from inception up until November 2018. PubMed, PsycINFO, and CINHAL databases were chosen for the search, as they contain publications that cater to a wide range of health conditions including dementia. In an attempt to locate “gray literature,” additional searches were conducted through Google Scholar.
The following search terms were used: (“illness representation*” OR “self regulation model” OR “illness cognition” OR “illness perception*”) AND (“neurocognitive disorder*” OR “Alzheimer*” OR “dementia” OR “mild cognitive impairment” OR “cognitive deterioration” OR “cognitive decline”).
The search was restricted to publications in the English language on human subjects and was supplemented by the manual searching of reference lists. Two researchers independently reviewed the titles and abstracts of the identified articles. Articles that appeared to meet the inclusion criteria were read in full.
Inclusion and exclusion criteria
Studies that identified the key terms in the title, abstract, or MeSH heading were retained. Inclusion criteria were studies that applied IRs to dementia, articles written in English, and articles published in peer-reviewed journals. Articles were excluded if they were not written in English or were published as book chapters, comments, or dissertations.
Data extraction and analysis
Search results for all databases were merged. Duplicates and nonrelated papers were excluded. Titles and abstracts of the remaining papers were assessed against the inclusion and exclusion criteria independently by both authors. The resulting papers were pooled, and disagreements were resolved through discussion based on the full text article. A standardized form was used to summarize the content of each article. The variables extracted were reference/country, aim of the study, study design, participants, and main finding/results.
Results
Figure 1 demonstrates the study flow chart according to PRISMA guidelines.14 The PRISMA diagram maps the flow of information through the various review stages. The diagram outlines the number of articles retrieved, number of articles kept for full review, number of articles excluded, reasons for exclusion, and number of articles kept for analysis. A total of 97 records were retrieved into an endnote library from the three data sets searched. Of these, 55 records remained after the removal of duplicates. Four additional records were obtained through Google Scholar search of already identified articles. Details concerning study flow and reasons for exclusion are shown in Figure 1. Table 1 summarizes the extracted information regarding: country, study aims, study design, year of publication, participants, and main findings. Several interesting findings emerge from the table in terms of the chronological and conceptual development of this area of research, as well as regarding its methodological aspects.
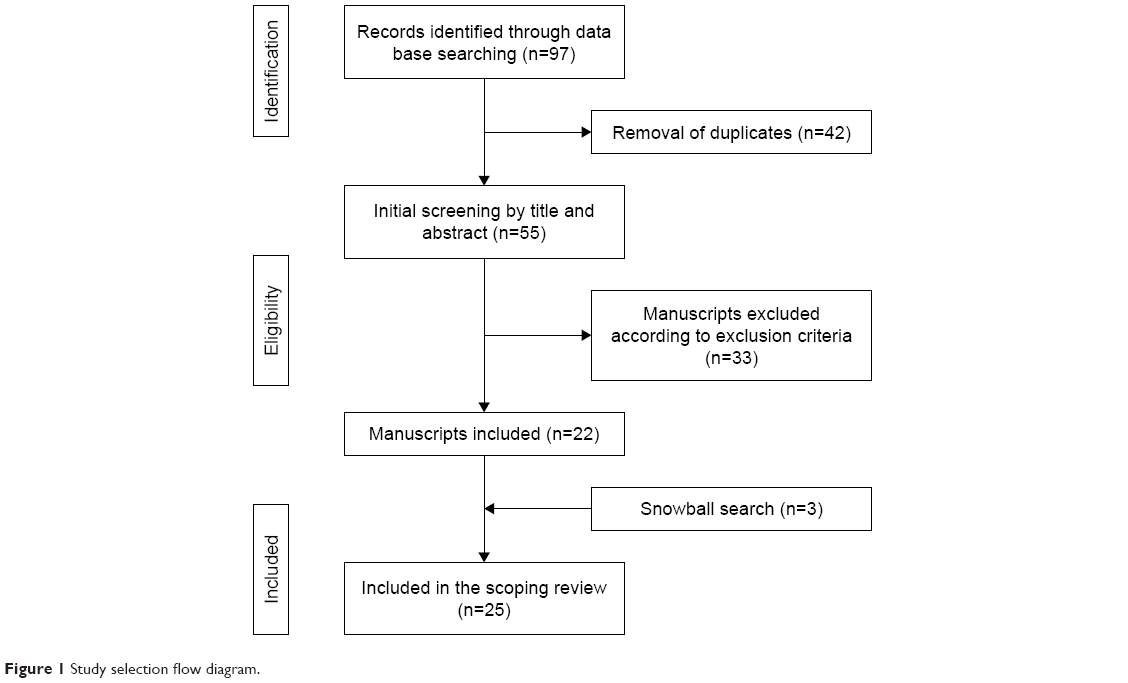 | Figure 1 Study selection flow diagram. |
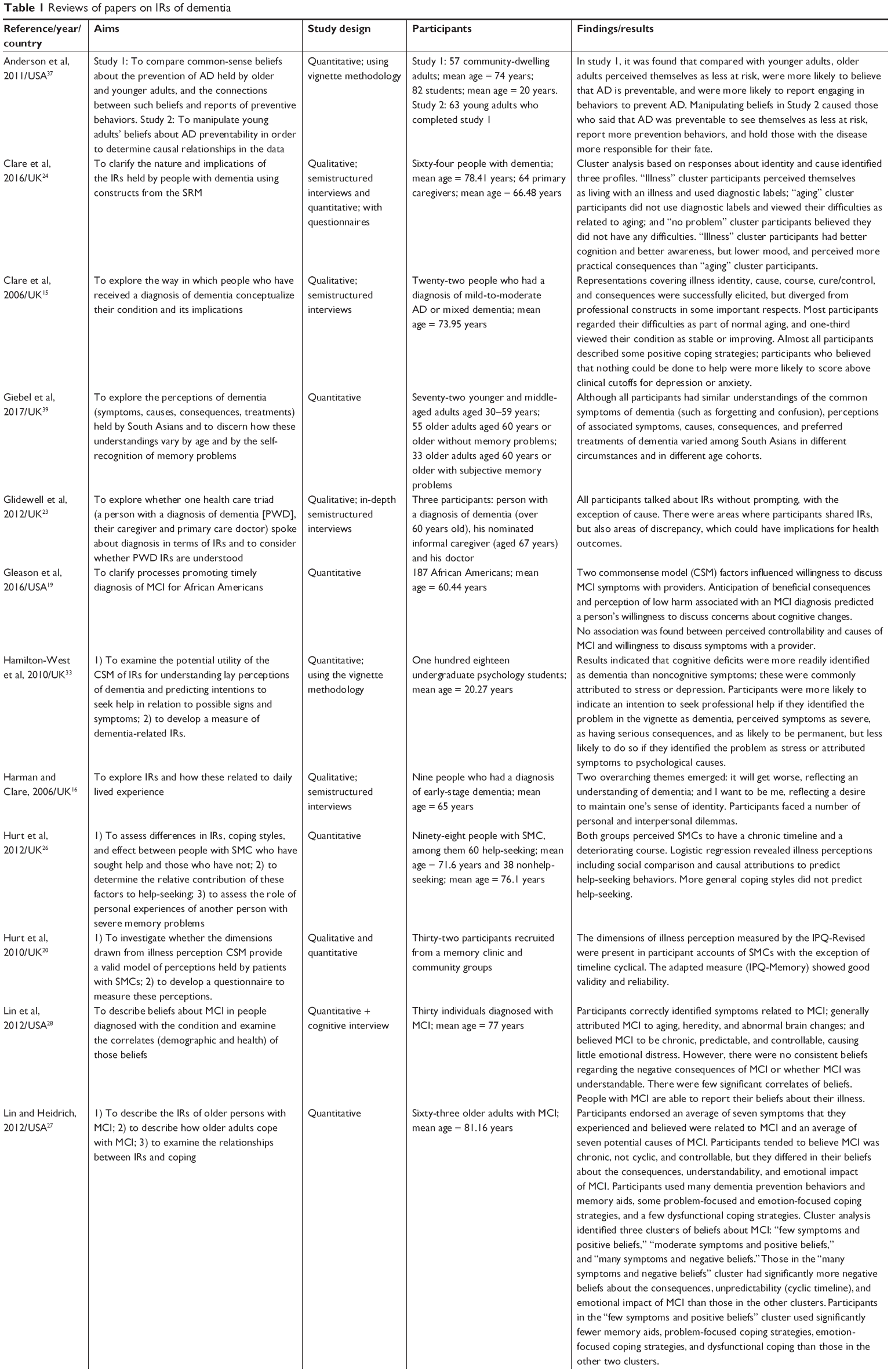  | Table 1 Reviews of papers on IRs of dementia |
Chronological development of research in the area of IRs and dementia
The bulk of research in the field of dementia IRs was gradually developed over the last two decades. The first two studies were published in 2000 and 2003 and were conducted among children and siblings of people with AD and among the lay public. The four subsequent studies, published in 2006, were all conducted among people with MCI or in the early stages of dementia.15–18
Conceptual aspects of IRs of dementia
Overall, the IR dimensions examined in most previous studies were identity, causes, cure/control, consequences, timeline (chronic/acute/cyclical), coherence, and emotional representations. Four studies19–22 assessed other dimensions such as preventability, responsibility, and social comparison.
Studies assessing people with dementia showed that they are more likely to use descriptive terms such as “memory decline” and “confusion” to refer to their condition than diagnostic terms such as “Alzheimer disease.” People with dementia may attribute the cause of their condition to one of a diverse range of factors (eg, aging, heredity, abnormal brain changes) and may identify multiple consequences of having the condition (such as familial and financial).15,16,23–25 In terms of timeline and control, people with dementia believed that dementia is a chronic condition,15,16,24–28 while some perceived dementia as uncontrollable condition.16,20,26
Studies concentrating on family caregivers found that they mentioned memory decline and confusion with time and place as symptoms of dementia. The causes of dementia, according to family caregivers, included biological hereditary, aging, and lifestyle factors.21,29,30 Some viewed dementia as having serious consequences,21 while the findings regarding the ability to control dementia were not uniform.22,29 Studies assessing formal caregivers showed that they also mentioned memory decline and confusion with time and place as symptoms of dementia. Formal caregivers perceived dementia as a chronic disease associated with severe consequences, while the main causes of dementia stem from risk factors followed by psychological factors.31,32 Finally, it was found that among the lay public, cognitive deficits were more readily identified as dementia than noncognitive symptoms.33,34 In addition, the lay public believed that the main causes of dementia stem from risk factors, followed by psychological factors. They perceived dementia as being chronic with serious consequences, and as a disease that is not controllable, but moderately dependent on treatment effectiveness.35
It should be noted that little work has been carried out to examine dementia IRs among different ethnic groups.19,36 The findings of these studies suggest that despite a potential shift in dementia IRs such as the believing that early recognition of MCI is beneficial, there are still misconceptions in regard to dementia among minority ethnic groups, such as believing that people living with dementia are unhygienic, aggressive, and have the same needs as children.36
Methodological aspects of studies assessing dementia IRs
In this section, we will describe the type of population examined, the methodology, and the assessment instruments that were used.
Research populations
The majority of studies were conducted among people with dementia (n=13) in the early-moderate stages of the disorder. Five studies assessing family caregivers included spouses/partners, children, siblings, and granddaughter/sister/niece.21,22,24,29,30 Three of the studies examining formal caregivers assessed physicians, social workers, and nurses.23,31,32 Finally, seven studies were conducted among students or the lay public.19,33–38
Research methodology
Thirteen studies used quantitative methods (using questionnaires) and seven used qualitative methods (including in-depth, semistructured interviews, vignette methodology, and discussion groups). Five studies used mixed methods, namely, both qualitative and quantitative methods.
Assessment instruments used to examine dementia IRs
As can be seen in Table 2, most quantitative studies used a revised or brief version of the Illness Perception Questionnaire (IPQ)2 with adaptations. The most common adaptations referred to the cause dimension, which was measured in some studies with an open item asking for “the three most important factors that you believe cause AD,”37 while in other studies the cause dimension was measured with a multiple item including different causes such as stress, worry, aging, heredity, and abnormal brain changes.19,22,27,28,31–33,35,38,39 In addition, six studies19–22,26,37 used dimensions that are not specifically included in the original IPQ and IPQ-Revised (eg, distress, perceived threat).
 | Table 2 Assessment instruments of dementia IRs |
The assessment instruments used varied in the number of items they included, from eight items30 up to 97 items.27,28 In addition, almost all measures adopted similar scoring systems using five-point Likert-type scales. Regarding the scales’ psychometric characteristics, almost all studies examined internal consistency (through Cronbach’s alpha), but only four examined validity (concurrent validity, discriminant validity, and face validity).26,33,38,39
Relationship between dementia IRs and outcome variables
It should be noted that given the relatively small number of articles and their heterogeneity, we cannot make concrete predictions about dementia IRs. Moreover, only six of the 25 publications included in this review examined factors associated with IRs. Among these publications, four outcome variables were examined: help-seeking, professional burnout, sense of coherence, and willingness to discuss concerns about cognitive changes. Findings showed that students and the lay public were more likely to indicate an intention to seek help if they perceived dementia as having severe symptoms and consequences, such as permanent damage, with higher perceived coherence.33,35 Among older adults with subjective memory complaints, it was found that IRs including social comparison and causal attributions predicted help-seeking behavior.26 Among formal caregivers, emotional representations were significantly associated with professional burnout, namely, the higher the negative emotional representations, the higher the professional burnout.32 Among carers of people with dementia, perceiving dementia as having severe symptoms and consequences with lower coherence and negative emotional representations were associated with a lower sense of coherence.30 Finally, significant correlations were found between anticipation of beneficial consequences and willingness to discuss concerns about cognitive changes among the lay public.19
Discussion
As the number of persons with dementia increases because of demographic changes,40 an increasing number of families, professionals, and laypersons will come into contact with persons with cognitive deterioration. Assessing IRs of these groups may have great importance for understanding their responses to dementia, as has been shown in other diseases.3,4 The present review intends to advance the current state of knowledge in this area by critically reviewing published literature on the topic. Several conceptual and methodological issues emerged.
Conceptual issues
Understanding IRs in the area of dementia
Overall, the study of dementia IRs is still in an early to moderate stage of development, in comparison with other diseases such as cancer, which has been extensively examined among persons with the disease and among other involved parties.3 However, research attention on the topic has increased over the past several years. This might be the result of two main reasons: one is related to the concept of IRs and the other to changes in the dementia discourse.
The concept of IRs
IRs were traditionally conceptualized to examine illness perceptions among persons with a disease.1 As such, their implementation with persons with dementia was limited, especially among those in the advanced stages, when cognitive deterioration affects the individual’s ability to accurately communicate his/her experiences of the disease. Lately, the contribution of IRs has expanded to include healthy populations.41–43 Thus, 12 of the 25 publications included in this review were conducted among nonaffected samples. This is an important development, as it enables a deeper understanding of the disease among lay persons. Moreover, this information might provide the necessary foundation and guidance for the development of educational programs to raise awareness and knowledge about dementia, to reduce misconceptions, and to increase timely help-seeking.
The dementia discourse
For many years, the popular understanding of dementia was based primarily on a medical model, which almost exclusively addressed the clinical aspects of cognitive deterioration.44 Lately, however, dementia discourse has been undergoing changes, and the implementation of a social model, which enables hearing the voices of the persons with the disease,45 is now encouraged. Thus, in recent years, literature has emerged, which acknowledges the individual’s experience, rights, and perspective. This literature expands our sense of dementia beyond neurobiology and neuropsychology and includes the person’s experience.46,47 This shift is reflected in the development of the literature reviewed here. Indeed, starting in 2006, we observed an increase in the number of studies examining IRs of persons with dementia in the early stages of the disease, using mostly qualitative methods, which voiced participants’ personal perceptions and experiences.
IRs’ dimensions in the area of dementia
Overall, similar to other diseases,48 previous studies in the area of dementia have concentrated on assessing the most traditional dimensions of IRs, with the most consistent findings emerging for identity, causes, timeline, consequences, and control. Regardless of the population examined, dementia is mostly described in the reviewed papers as a chronic condition, presenting more cognitive than behavioral symptoms, and as being caused mainly by age, heredity, abnormal brain changes, and stress or worry.
Examination of the studies in this review showed that, regardless of the type of participants included, memory decline and confusion with time and place were correctly identified as dementia symptoms. Similarly, beliefs of dementia as a chronic condition were consistent across studies. The most frequently endorsed causes of dementia were aging, heredity, abnormal brain changes, and stress or worry.
While overall, these perceptions are congruent with the clinical characteristics of dementia,49 it should be noted that perceiving dementia as a terminal illness may have a major impact on expectations, treatments, attitudes, and help-seeking. Furthermore, concentrating mostly on cognitive symptoms might suggest that there is not enough available knowledge,50 underscoring the importance of the latest efforts invested worldwide to increase knowledge and awareness about dementia.51
Assessing correlates of IRs
It should be noted that research in the area of dementia and IRs is mostly descriptive, and only few studies have examined correlates of IRs. Three studies found an association between IRs and help-seeking.26,33,35 This is a significant finding for two reasons. First, the association between IRs and help-seeking is at the core of the commonsense model52 and demonstrates the suitability of this model in the area of dementia. Second, it suggests that subjective perceptions of dementia, together with the objective nature of symptoms, are important factors in the help-seeking process.53
However, a closer examination of the findings about IRs and help-seeking showed that the worse the disease is perceived, the more people seek help. This finding is worrisome, since it indicates that people seek help only when cognitive deterioration is perceived as reaching the more advanced stages. Several possible explanations have been offered for this delay, such as that the symptoms of dementia can be difficult to recognize in their early stages,54 attribution of memory problems to normal aging,55 stigma, and embarrassment.56 Yet, it should be noted that therapeutic interventions are increasingly recognized as being most efficient in the early stages and that seeking help in the early stages of dementia allows optimal medical management to delay progression.57 Therefore, educational programs should take into consideration the connections between IRs and help-seeking, in order to advance help-seeking in an appropriate and timely manner.
Methodological issues
As stated, research about IRs and dementia is gradually conceptually evolving. However, our review of the literature shows that, methodologically, it is characterized by design, sample, and data collection weaknesses, which need to be addressed.
Sample issues
Regardless of the type of population examined, the majority of the studies in the review were based on nonrepresentative and small samples.15–17,19,20,24,25,28,31–35,37
To advance the existing knowledge and be able to generalize and draw conclusions, there is a need to start conducting large-scale studies based on representative samples, which will allow the examination of IRs among different populations, as has been done in regard to other diseases.58
Design issues
According to the current review, all studies examining dementia IRs until today were cross-sectional, therefore limiting the possibility of assessing changes in dementia IRs across time, as has been done with regard to other diseases.4,59 This is an important limitation, especially since, as noted by Leventhal et al,1 IRs do not remain static but are rather dynamic – formed and changed through active processing. In the case of dementia, a progressive disease involving cognitive deterioration6 examining changes across time might be especially important.
Data collection issues
Two main issues associated with data collection arise from examining the body of knowledge on dementia IRs accumulated until today: the first relates to the type of data collection used, and the second to the instruments used.
The current understanding of dementia IRs is based mainly on quantitative methodology. Indeed, only eight studies included in this review were qualitative, while another four used a mixed methods methodology. Two reasons might explain this tendency: first, as mentioned above, the use of qualitative methods to assess IRs of persons with dementia has increased lately, as a result of the change in the dementia discourse.45 Second, the availability of a valid structured instrument, such as the IPQ, facilitates the use of quantitative methodologies. And indeed, overall, most previous studies exploring dementia IRs were based on detailed descriptions of modifications of the IPQ and the IPQ-Revised. Thus, these modifications are consistent with the recommendations of Weinman et al60 and Moss-Morris et al,2 who argued that users can adapt the IPQ and IPQ-Revised to be illness specific. However, it should be noted that the IPQ is limited, given that people with moderate to severe dementia may be unable to complete it.
In addition, the qualitative components of the mixed methods studies offered an opportunity for a deeper examination of IRs. Information from the qualitative interviews was also utilized to adapt the IPQ-R specific population (eg, patients with subjective memory complain).20 Furthermore, the qualitative research findings revealed that participants nurtured additional perceptions and feelings regarding dementia that they could not express through the structured questionnaires. Therefore, one of the conclusions of the mixed methods studies was to expand the IPQ by adding some open questions in order to receive more information about IRs, which cannot be expressed by the closed questionnaire.24,32
Limitations of the review
The present review has two main limitations. First, despite making every attempt to include the relevant literature, we cannot disregard the possibility that some studies may not have been identified. This is an inherent limitation of a review paper which, in an effort to be specific, is prone to not including all studies of importance. Second, information was synthesized and reported in summary tables, but no statistical techniques were used to assess methodological issues, such as sample size. However, it should be noted that this review was not intended to be an exhaustive review of the literature in the area, but rather to focus readers’ attention on conceptual and methodological developments and their impact for future research and for clinical interventions.
Future research
Our examination of the current body of knowledge in the area of dementia IRs revealed several promising lines of inquiry for future investigations. Some relate to conceptual aspects and others to methodological aspects.
Conceptually, one of the areas in need of further attention is the examination of dementia IRs among different ethnic groups. This is especially important since, according to Leventhal and Ian,61 cultural factors influence individuals’ IRs. Furthermore, recent studies recognize ethno-racial differences in the prevalence and incidence of dementia,62 stressing the importance of developing this direction. In addition, it is suggested that future studies would examine IRs among young people with dementia and their surrounding (eg, family members, formal caregivers). This is especially important as alertness for dementia in young patients (before the age of 65 years) is increasing.63
Methodologically, additional research with more representative samples and more fully validated measures are necessary in order to further explore and detail racial and ethnic differences in dementia IRs. In addition, this review revealed that the majority of studies were cross-sectional, which may hinder the ability to understand the dynamic nature of dementia IRs. Therefore, as suggested in the area of IRs and mental health,48 longitudinal and intervention studies are required to show the influence of interventions aimed at challenging negative illness perceptions and exploring how this impacts upon clinical outcomes. These designs will also allow exploration of how illness perceptions may change over time. For example, a study following individuals throughout a lifetime would be an interesting one. Moreover, the development and validation of standardized measures to examining dementia IRs are imperative.
Clinical implications
Advancing these conceptual and methodological issues will promote the development of more effective clinical interventions. Indeed, the study of IRs in other areas has suggested that to improve health and psychosocial outcomes, it may be beneficial for interventions to target individuals’ maladaptive or unrealistic IRs, while at the same time forming alternative representations.3,48 The time has come to advance this knowledge in the area of dementia as well.
Special attention should be paid to perceptions of personal control, which might be useful to increase the use of adaptive coping strategies such as cognitive reappraisal and reduce maladaptive coping strategies such as avoidance or denial.3 In the same vein, a systematic review of the literature exploring IRs in mental health utilizing the SRM has found that perceptions of personal control over one’s illness and beliefs that treatment can help control symptoms were associated with greater engagement with services, treatment adherence, a reduction in symptoms, and less emotional distress.48
In addition, interventions that aim to decrease the perceived emotional impact of AD may reduce psychological distress and may improve one’s quality of life. However, it should be noted that in interventions targeting IRs, it is important to hold in mind that some IRs about poor illness outcomes may be realistic; for a family member of a relative with advanced AD, representations of a chronic timeline and severe consequences may be justified. In these cases, interventions could better target IRs such as emotional representations in order to allow ventilation of the emotional distress.
To sum up, this review indicates that despite important advances, gaps in the theoretical and methodological issues of dementia IRs remain. We have tried to identify these gaps and provide suggestions for further advancing this area of knowledge. Nevertheless, the 25 reviewed studies have provided valuable insight into the significant meaning of IRs in the area of dementia, offering valuable implications for clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
Leventhal H, Meyer D, Nerenz D. The common-sense representations of illness and danger. In: Rachman R, editor. Contributions to Medical Psychology. Oxford: Pergamon Press; 1980. | ||
Moss-Morris R, Weinman J, Petrie K, Horne R, Cameron L, Buick D. The revised illness perception questionnaire (IPQ-R). Psychol Health. 2002;17(1):1–16. | ||
Richardson EM, Schüz N, Sanderson K, Scott JL, Schüz B. Illness representations, coping, and illness outcomes in people with cancer: a systematic review and meta-analysis. Psychooncology. 2017;26(6):724–737. | ||
Karademas EC, Dimitraki G, Papastefanakis E, et al. Adaptation to inflammatory rheumatic disease: do illness representations predict patients’ physical functioning over time? A complex relationship. J Behav Med. 2018;41(2):232–242. | ||
Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014;10(11):634–642. | ||
Cheston R, Christopher G, Ismail S. Dementia as an existential threat: the importance of self-esteem, social connectedness and meaning in life. Sci Prog. 2015;98(Pt 4):416–419. | ||
Werner P, Savva GM, Maidment I. Dementia: introduction, epidemiology and economic impact. In: Chew-Graham CA, Ray M (editors). Mental Health and Older People. Basel: Springer International Publishing; 2016:197–209. | ||
Tejada-vera B. Mortality from Alzheimer’s Disease in the United States: data for 2000 and 2010. NCHS Data Brief. 2013;(116)1–8. | ||
Frankish H, Horton R. Prevention and management of dementia: a priority for public health. Lancet. 2017;390(10113):2614–2615. | ||
Mcgrady ME, Peugh JL, Hood KK. Illness representations predict adherence in adolescents and young adults with type 1 diabetes. Psychol Health. 2014;29(9):985–998. | ||
Sonney J, Insel KC, Segrin C, Gerald LB, Ki Moore IM. Association of asthma illness representations and reported controller medication adherence among school-aged children and their parents. J Pediatr Health Care. 2017;31(6):703–712. | ||
Davis K, Drey N, Gould D. What are scoping studies? A review of the nursing literature. Int J Nurs Stud. 2009;46(10):1386–1400. | ||
Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Infor Libra. 2009;26(2):91–108. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. | ||
Clare L, Goater T, Woods B. Illness representations in early-stage dementia: a preliminary investigation. Int J Geriatr Psychiatry. 2006;21(8):761–767. | ||
Harman G, Clare L. Illness representations and lived experience in early-stage dementia. Qual Health Res. 2006;16(4):484–502. | ||
Lingler JH, Nightingale MC, Erlen JA, et al. Making sense of mild cognitive impairment: a qualitative exploration of the patient’s experience. Gerontologist. 2006;46(6):791–800. | ||
Moniz-Cook E, Manthorpe J, Carr I. Facing the future: a qualitative study of older people referred to a memory clinic prior to assessment and diagnosis. Dementia. 2006;5(3):375–395. | ||
Gleason CE, Dowling NM, Benton SF, Kaseroff A, Gunn W, Edwards DF. Common sense model factors affecting African Americans’ willingness to consult a healthcare provider regarding symptoms of mild cognitive impairment. Am J Geriatr Psychiatry. 2016;24(7):537–546. | ||
Hurt CS, Burns A, Brown RG, Barrowclough C. Perceptions of subjective memory complaint in older adults: the illness perception Questionnaire-Memory (IPQ-M). Int Psychogeriatr. 2010;22(5):750–760. | ||
Lingler JH, Terhorst L, Schulz R, Gentry A, Lopez O. Dyadic analysis of illness perceptions among persons with mild cognitive impairment and their family members. Gerontologist. 2016;56(5):886–895. | ||
Roberts JS, Connell CM. Illness representations among first-degree relatives of people with Alzheimer disease. Alzheimer Dis Assoc Disord. 2000;14(3):129–136. | ||
Glidewell L, Johnston M, Thomas R. Shared understandings of dementia? An application of the common sense self-regulation model to a case study. Dementia. 2012;11(2):217–250. | ||
Clare L, Quinn C, Jones IR, Woods RT. “I don’t think of it as an illness”: illness representations in mild to moderate dementia. JAD. 2016;51(1):139–150. | ||
Matchwick C, Domone R, Leroi I, Simpson J. Perceptions of cause and control in people with Alzheimer’s disease. Gerontologist. 2014;54(2):268–276. | ||
Hurt CS, Burns A, Brown RG, Barrowclough C. Why don’t older adults with subjective memory complaints seek help? Int J Geriatr Psychiatry. 2012;27(4):394–400. | ||
Lin F, Heidrich SM. Role of older adult’s illness schemata in coping with mild cognitive impairment. J Psychosom Res. 2012;72(5):357–363. | ||
Lin F, Gleason CE, Heidrich SM. Illness representations in older adults with mild cognitive impairment. Res Gerontol Nurs. 2012;5(3):195–206. | ||
Quinn C, Jones IR, Clare L. Illness representations in caregivers of people with dementia. Aging Ment Health. 2017;21(5):553–561. | ||
Lo Sterzo E, Orgeta V. Illness representation and sense of coherence in dementia caregiving. J Health Psychol. 2017;22(6):722–732. | ||
Shinan-Altman S, Werner P, Cohen M. Social workers’ and nurses’ illness representations about Alzheimer disease. Alzheimer Dis Assoc Disord. 2014;28(1):73–78. | ||
Shinan-Altman S, Werner P, Cohen M. The connection between illness representations of Alzheimer’s disease and burnout among social workers and nurses in nursing homes and hospitals: a mixed-methods investigation. Aging Ment Health. 2016;20(4):352–361. | ||
Hamilton-West KE, Milne AJ, Chenery A, Tilbrook C. Help-seeking in relation to signs of dementia: a pilot study to evaluate the utility of the common-sense model of illness representations. Psychol Health Med. 2010;15(5):540–549. | ||
Roberts JS, Connell CM, Cisewski D, Hipps YG, Demissie S, Green RC. Differences between African Americans and whites in their perceptions of Alzheimer disease. Alzheimer Dis Assoc Disord. 2003;17(1):19–26. | ||
Shinan-Altman S, Werner P. Is there an association between help-seeking for early detection of Alzheimer’s disease and illness representations of this disease among the lay public? Int J Geriatr Psychiatry. 2017;32(12):e100–e106. | ||
Parveen S, Peltier C, Oyebode JR. Perceptions of dementia and use of services in minority ethnic communities: a scoping exercise. Health Soc Care Community. 2017;25(2):734–742. | ||
Anderson LN, Mccaul KD, Langley LK. Common-sense beliefs about the prevention of Alzheimer’s disease. Aging Ment Health. 2011;15(7):922–931. | ||
Quinn C, Morris RG, Clare L. Beliefs about dementia: development and validation of the representations and adjustment to dementia index (Radix). Am J Geriatr Psychiatry. 2018;26(6):680–689. | ||
Giebel CM, Worden A, Challis D, et al. Age, memory loss and perceptions of dementia in South Asian ethnic minorities. Aging Ment Health. 2017;27(5):1–10. | ||
Wimo A, Guerchet M, Ali GC, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2017;13(1):1–7. | ||
Shinan-Altman S. Medical social workers’ perceptions of obesity. J Soc Work. 2017;17(3):343–357. | ||
Gaston AM, Cottrell DJ, Fullen T. An examination of how adolescent-caregiver dyad illness representations relate to adolescents’ reported diabetes self-management. Child Care Health Dev. 2012;38(4):513–519. | ||
Rexhaj S, Python NV, Morin D, Bonsack C, Favrod J. Correlational study: illness representations and coping styles in caregivers for individuals with schizophrenia. Ann Gen Psychiatry. 2013;12(1):27. | ||
Camp CJ. Flexibility in persons with dementia. In: Sinnott JD, editor. Identity Flexibility During Adulthood. Cham: Springer; 2017:99–114. | ||
Dröes RM, Chattat R, Diaz A, et al. Social health and dementia: a European consensus on the operationalization of the concept and directions for research and practice. Aging Ment Health. 2017;21(1):4–17. | ||
Goldsmith M. Hearing the Voice of People with Dementia: Opportunities and Obstacles. London: Jessica Kingsley; 1996. | ||
Sabat SR. Voices of Alzheimer’s disease sufferers: a call for treatment based on personhood. J Clin Ethics. 1998;9(1):35–48. | ||
Baines T, Wittkowski A. A systematic review of the literature exploring illness perceptions in mental health utilising the self-regulation model. J Clin Psychol Med Settings. 2013;20(3):263–274. | ||
Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. BMJ. 2015;350. | ||
Cahill S, Pierce M, Werner P, Darley A, Bobersky A. A systematic review of the public’s knowledge and understanding of Alzheimer’s disease and dementia. Alzheimer Dis Assoc Disord. 2015;29(3):255–275. | ||
World Health Organization. Global action plan on the public health response to dementia 2017–2025. 2017. | ||
Bishop GD, Converse SA. Illness representations: a prototype approach. Health Psychol. 1986;5(2):95–114. | ||
Werner P, Goldstein D, Karpas DS, Chan L, Lai C. Help-seeking for dementia: a systematic review of the literature. Alzheimer Dis Assoc Disord. 2014;28(4):299–310. | ||
Eustace A, Bruce I, Coen R, et al. Behavioural disturbance triggers recognition of dementia by family informants. Int J Geriatr Psychiatry. 2007;22(6):574–579. | ||
Perry-Young L, Owen G, Kelly S, Owens C. How people come to recognise a problem and seek medical help for a person showing early signs of dementia: a systematic review and meta-ethnography. Dementia. 2018;17(1):34–60. | ||
Devoy S, Simpson EEA. Help-seeking intentions for early dementia diagnosis in a sample of Irish adults. Aging Ment Health. 2017;21(8):870–878. | ||
Panegyres P, Berry R, Burchell J. Early dementia screening. Diagnostics. 2016;6(1):6. | ||
Cabassa LJ, Lagomasino IT, Dwight-Johnson M, Hansen MC, Xie B. Measuring Latinos’ perceptions of depression: a confirmatory factor analysis of the illness perception questionnaire. Cultur Divers Ethnic Minor Psychol. 2008;14(4):377–384. | ||
Arcoleo K, Feldman J. Asthma illness representations: do they really change over time? Biol Psychol. 2017;129:377. | ||
Weinman J, Petrie KJ, Moss-Morris R, Horne R. The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychol Health. 1996;11(3):431–445. | ||
Leventhal H, Ian B. The common-sense model of self-regulation of health and illness. In: Cameron L, Leventhal H, editors. The Self-Regulation of Health and Illness Behavior. London: Routledge; 2012:56–79. | ||
Hillman A, Latimer J. Cultural representations of dementia. PLoS Med. 2017;14(3):e1002274. | ||
Perrone F, Cacace R, van Mossevelde S, et al. Genetic screening in early-onset dementia patients with unclear phenotype: relevance for clinical diagnosis. Neurobiol Aging. 2018;69:292.e7–292.e14. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.