")
Back to Journals » Clinical Interventions in Aging » Volume 15
Hormonal Function Responses to Moderate Aerobic Exercise in Older Adults with Depression
Authors Alghadir AH, Gabr SA
Received 22 April 2020
Accepted for publication 14 July 2020
Published 3 August 2020 Volume 2020:15 Pages 1271—1283
DOI https://doi.org/10.2147/CIA.S259422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Ahmad H Alghadir ,1 Sami A Gabr 1
Rehabilitation Research Chair (RRC), College of Applied Medical Sciences (CAMS), King Saud University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Sami A Gabr
Rehabilitation Research Chair (RRC), College of Applied Medical Sciences (CAMS), King Saud University, P.O. Box 10219, Riyadh 11433, Kingdom of Saudi Arabia
Tel +966 562060018
Fax +966 14698541
Email [email protected]
Background: Poor daily life physical activities among older people were related to depressive mood especially memory loss. In addition to that, the change in physical ability is significantly associated with the score of depression among older age.
Objective: The present study aimed to evaluate the effects of a supervised aerobic training program with moderate intensity for 12 weeks on mood profiles and hormonal levels of the hypothalamus-pituitary-adrenal axis (HPA axis) of older adults.
Methods: A total of 80 individuals of both gender (90 males, 110 females) of ages ranged between 65 and 95 years were recruited for this study. Based upon the profile of mood states (POMS) analysis, the participants were classified into two groups: control group (n=30) and depressive group (n=50). Leisure-time physical activity (LTPA), adrenal hormones such as ACTH, corticosterone (CORT), cortisol, DHEA/S, and cortisol:DHEA/S ratio were measured at baseline and post-intervention of moderate aerobic exercise for 12 weeks.
Results: Older adults with higher depressive scores showed a remarkable change in the level of adrenal hormones compared to control. There was a significant increase in the level of ACTH, CORT, cortisol, and cortisol:DHEA/S ratio, and decrease in DHEA/S. Compared to females, males showed an improvement in depressive mood score along with an increase in LPTA, DHEA/S and decrease in ACTH, CORT, cortisol, cortisol:DHEA/S ratio following 12 weeks of supervised aerobic training, respectively.
Conclusion: The findings of this study showed that 12 weeks of supervised exercise interventions are promising non-drug therapeutic strategies in improving depression among older adults. The potential performance in a psychological state occurs physiologically via optimizing the levels of the hormones of the HPA axis.
Keywords: adrenal function, depression, LPTA, aerobic exercise, POMS
Introduction
Depression refers to many feelings that are enough to change social daily life and produce negative effects on the human mood.1 Most studies revealed that human depression mainly related to disorder in concentration, memory loss, and other thinking abilities.2–4 The incidence of depression is doubly increased in both genders,5 whereas higher ratios of depression (15–30%) were reported among older adults.6,7 These ratios expose adults’ people of both genders to more serious physical health problems, which in turn may lead to mortality.8,9
Recent research works reported an association between the lower physical activities during daily life and depressive mood among older people especially memory loss,10,11 and that the change in physical ability significantly associated with the score of depression among older ages.12 In addition to that, a remarkable relation was reported between age, mood behavior, and physical activity, which collectively affect an older adult’s lifestyle.13,14
Thus, for good health, it is more convenient to verify the mechanistic relations between physical activity and mood behaviors among older adults. Previously, it was reported that the improper adrenal function plays a significant link between human physical activity and depressive mood states.15,16
Previous studies showed that the ability to respond to stress with aging was significantly reduced which might be related to abnormalities in the hypothalamus-pituitary-adrenal axis (HPA axis) function and subsequent release of large amounts of cortisol and other components of the HPA axis, such as the corticotrophin-releasing hormone.17,18 Because of stress, the produced abnormalities over-activate the HPA axis through neuroendocrine and autonomic pathways, and can badly affect the cellular immune response, glucose pathways, and lead to severe diabetic conditions.19,20
In human bodies, stress showed to be controlled via the activity of the HPA which controls the release of cellular physiological adrenal hormones.21,22 It was reported that the adrenocorticotrophic hormones (ACTH) and corticosterone hormones expressed from the HPA axis into the plasma are considered as important stress indicator.21,22 In addition, the secretion of cortisol and rises its level was the most pronounced among older adults exposed to daily life stressors.15–22
In most studies, cortisol levels appear to have varying functions according to age whereas, younger ages exhibiting a smaller the cortisol awakening response (CAR) compared to adults.23,24 These ultimately promote the HPA axis to utilize a complex interplay of neural and hormonal systems to release sufficient cortisol to respond to the demands of the environments. The interference within this complex system originate to a deficient in stress coping which might lead to stress-related psychopathology.24,25
In addition, dehydroepiandrosterone (DHEA) and its sulfate form (DHEA-S) are the most abundant hormones regulated by the HPA axis along with cortisol. DHEA as anti-glucocorticoid showed to play potential significant roles in many body disorders such as immunity, obesity, and in stress processing.26–29 DHEA-S showed to have a long half-life and slower clearance rate thus; it serves as a reservoir for DHEA.30 In stress, DHEA is primarily released from the adrenal in parallel with cortisol in response to HPA axis activation by ACTH.27,29 A strong regulatory influence of DHEA was reported on the HPA upon release. A direct down regulatory impact on corticoid receptors,26,27 emotion regulation neurocircuitry,31 and enhanced behavioral activation associated with stress coping significantly appeared following the release of DHEA.32
In humans, the negative impact of high cortisol on episodic memory in older and young adult males were significantly attenuated by the release of DHEA,33,34 and improved decision-making competence was shown to be associated with greater stress reactive DHEA levels.35 DHEAS was suggested to play a role as a marker of proper stress management against psychosocial stress including job-related stress.36 During aging, the increase in the cortisol/DHEAS ratio refers significantly to an increase in the neurotoxicity and probably contributes to the occurrence of age-related neurodegenerative illnesses.37,38 Thus, higher secretions of DHEA/DHEAS considered of great importance in improving health outcomes,39–42 including psychological status, and reduced risk of death from cardiovascular disease.39–42 Similarly, corticosterone (CORT) levels were generally raised following stressful events and impairs in cognition/memory and stress coping which in turn lead to a reduction in the structural and functional plasticity of the brain.43,44 In healthy and diseased subjects, corticosterone is the major biosynthetic route of mineralocorticoid that it converted to aldosterone.45,46
The physical exercise showed to produce a new situation of homeostasis in human bodies. It maintains the augmentation of the energetic demand via many countless physiological alterations,21–23 whereas, the promotion of the HPA axis with exercise produce increment in the level of ACTH from pituitary corticotrophin cells which in turn helps in the increase of cortisol,47–49 and most related adrenal hormones like androgens which may participate with human health.50
Although drug therapy was the main choice for the treatment of patients with abnormal mood profiles particularly depression, Exercise interventions as alternative treatments have been used in research as well as in clinical practice, mainly due to response failure to drug treatment.51–53
A significant reduction in depressive symptoms was observed in older patients with depression following physical exercise training,54–56 and signifies physical exercise as an effective non-pharmacological treatment for depression in older adults.56,57 The positive effect of physical exercise based on the physiological changes in the function of HPA, whereas physical exercise can modulate cortisol via the upregulation of the glucocorticoid receptors.55–61
The effect of physical exercise of different intensities on depression and other related mood disorders was evaluated in many studies.62–68 Many of which showed that aerobic training significantly affects positively on depression.62,63
In a systematic review and meta-analysis study, the physical exercise showed to promote the levels of cortisol among subjects with mild depression disorders (MDD), whoever these findings significantly controlled by the type of exercise, frequency, and the type of cortisol measurement.69
Several studies performed on middle-aged/older adult individuals suggest beneficial positive effects on mood, well-being, and cognition.70–72 In a recent pilot study, the feasibility of aerobic exercise as an antidepressant treatment strategy was evaluated in young adults with MDD. In that study, a decrease in depression scores with a significant increase in VO2max as a measure of good physical performance was predicted following exercise interventions for 12 weeks.73
Although aerobic exercise may reflect neurobiological changes and produces antidepressant effects via physiological changes in VO2max among younger ages,73 little work has assessed the potential effects of moderate aerobic training on adrenal hormones and its required efficiency for alleviating symptoms in depressed older adults.74–79
Considering, the potential role of physical activity in enhancing physiological adrenal function, and its effects on mood profiles among older adults as previously reviewed in the literature. Thus, the present study tried to evaluate the effects of supervised aerobic training interventions with moderate intensity for 12 weeks on adrenal hormonal levels such as DHEA, cortisol, ACTH, corticosterone among older adults with depression. In addition, the association between physical activity scores, adrenal hormones, and scores of mood profiles were evaluated following 12 weeks of supervised aerobic training.
Materials and Methods
Subjects
A total of 200 healthy subjects with an age range of 65–95 years old and mean age of (69.7 ± 5.91) were recruited for this study, between 15 January 2013 and 15 September 2013 via electoral roll randomized selection. Out of them, only 80 subjects who matched the inclusion criteria participated in this study. Based on the POMS analysis, the subjects were classified into two groups: the control group (n= 30) and the depressive group (n= 50). The design of the experimental protocol containing two groups: the control group (n= 30) and the depressive group (n= 50) was evaluated as shown in the flow chart Figure 1. Subjects with endocrine, immune, psychiatric illness, eating disorders, and taking glucocorticoid medication were excluded from this study. Standardized measures such as weight, height, and body mass index were calculated pre and post-exercise tests. The demographics and baseline characteristics of participants are shown in (Table 1). All study participants gave informed consent before participation. Regarding the ethical guidelines of the 1975 Declaration of Helsinki, the study protocol was reviewed and approved by the ethical committee of Rehabilitation Research Chair (RRC), King Saud University, Kingdom of Saudi Arabia, under file number (ID: RRC-2014-007).
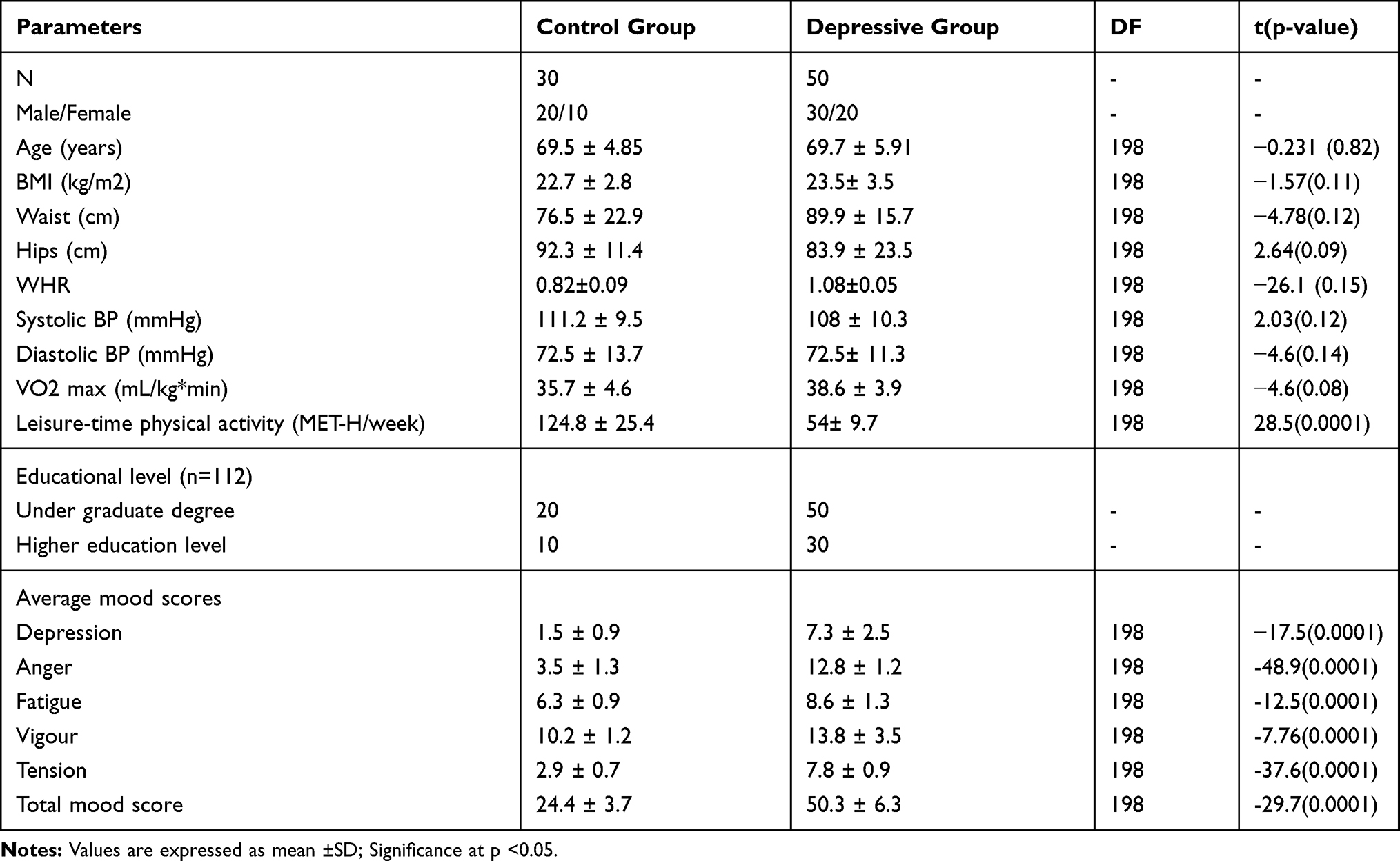 |
Table 1 The Demographics and Baseline Characteristics of Participants |
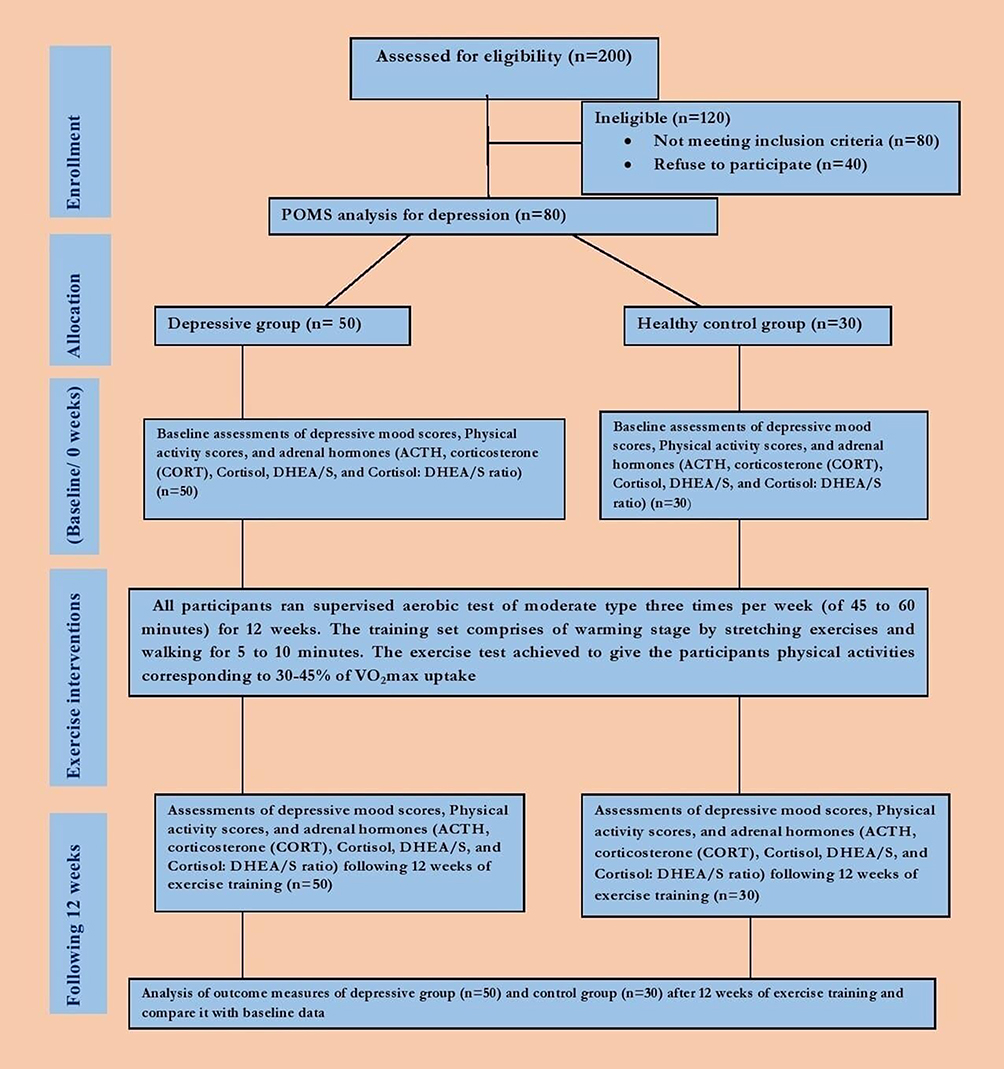 |
Figure 1 Flow diagram of the participants through the study. Participants classified according to POMS analysis and participated in supervised aerobic test of moderate type three times per week (of 45 to 60 minutes) for 12 weeks. |
Outcome Measures
Profile of Mood States (POMS)
Depressive mood score among studied subjects was performed using a validated short version of the POMS as previously reported.79–83 The POMS is a self-report 32 items questionnaire designed to evaluate mood states. It is designed to measure mood in five different domains: fatigue (6 items), irritation (7 items), vigor (5 items), tension (6 items), and depression (8 items). The answers are scored on a 5-point Likert scale,83 ranging from “not at all” (0) to “extremely” (4). The reliability and validity of this scale are good (α =.76–α =.95).79–83 In the current study, internal consistency for the different domains ranged from α =.85 to α =.94 respectively. Based on the POMS analysis, the subjects were classified into two groups control group (n= 30), and the depressive group (n= 50).
Leisure-Time Physical Activity (LTPA)
Physical activity scores in the form of a leisure-time physical activity (LTPA) were estimated for all participants by using a pre-validated global physical activity questionnaire as previously reported.84 For each participant, the activity donated as energy expenditure rate was calculated weekly as metabolic equivalents per hour/week (T-LPTA-MET/H/W) as previously reported.84,85
Training Procedure
Participants of both control and depressive groups performed the exercise test according to Karvonen’s formula,85 three times per week for 12 weeks. The program of this study was designed in the form of a treadmill-walking mode. The training intensity of each participant was calculated according to Karvonen’s formula,85 as training heart rate (THR), which mainly based on both the predicted maximum heart rate and resting heart rate corresponding to respective age. The participants performed the exercise test for 45 to 60 minutes to gain physical activities corresponding to 30–45% of VO2max uptake as previously reported,85 and gradually increased until they reach 65% to 75% of VO2max for moderate intensity, which used in this study.
Design of the Exercise Program
The exercise test performed three times per week each exercise session consisted of three phases warm-up, active, and cool-down phases;
Warm-Up Phase
The subject performed a simple stretching exercise for all large muscle groups and walked for 5 to 10 minutes at a training fraction (TF) equal to 30%–40%.
Active Phase
The subject was allowed to reach his pre-calculated training heart rate (THR) in bouts with a total time of from 30 to 45 minutes.
Cool-Down Phase
In this phase, the workload decreased gradually within 10 to 15 minutes until the participant’s HR and blood pressure returned nearly to the resting level. Throughout the entire training session, the heart rate of the participant was monitored using a portable heart rate monitor to maintain exercise intensity within the pre-calculated training heart rate (65% to 75%).
Assessment of Adrenal Hormones
Fasting blood samples were collected from all participants at 8.30 in the morning to avoid a probable diurnal influence at both pre-exercise and 5–10 minutes’ post-exercise-training program. The proposed time for blood collection was selected for the control of the circadian hormonal range as previously reported in the procedures of other studies.86 After centrifugation, serum samples of all tests were stored at-80 ºC until reused. Several adrenal hormones were considered in order to detect major adrenal pathways. Both cortisol and ACTH were measured in serum samples using immunoassay technique according to instructions of RIA-ELISA kit (DPC Inc., CA, USA), and SIA-ELISA kit (MD Biosciences Inc, MN, USA) respectively. Serum levels of DHEAS were measured by an immunoassay (Diagnostic Products Corporation, Immulite 1000) with an intra-assay CV of <5.2%. Serum levels of corticosterone (CORT) were measured by a quantitative competitive enzyme immunoassay technique that measures corticosterone (Assaypro LLC, St. Charles, Missouri, MO 63,304, USA).
Statistical Analysis
Power calculations of the selected sample size of 80 subjects showed to give an estimated power of 95% and a significance level of 0.05 with an expected frequency of 6.5%. An SPSS statistical program (SPSS, IBM Statistics V.17) was used to analyze all data produced in this study. The data of continuous variables are expressed as mean±SD, while those of categorical variables are described as counts and percentages. A non-parametric test (Mann–Whitney-Wilcoxon test) and the χ2 test were used to analyze frequency differences between the groups. In all groups’ pre- and post-exercise training, two independent sample t-tests were used for comparison between the studied variables such as depressive mood score (dependent variable), physical activity, and adrenal hormones (independent variables). In addition, multiple stepwise regressions and Pearson’s correlations analysis were used to estimate the associations between physical activity scores (LPTA-MET-H/W) and those of Adrenal hormones; cortisol, DHEA, cortisol:DHEA ratio, ACTH, and Corticosterone serum concentrations in older subjects with depression and in controls. All tests were two-tailed; because of multiple assessments, results were only considered statistically significant at a value of p <0.01.
Results
A total of 80 subjects were involved in this study, most of them are males (n= 50; 62.5%). They are classified according to mood profile score into normal (n= 30) and depressive (n=50). Compared to controls, subjects with depression showed no significance in all demographic parameters; BMI (p=0.11), WHR (p=0.15), waist (p=0.012), hips (p=0.09), Age (p=0.82), and VO2 max (P=0.08) as shown in Table 1.
In the baseline state, participants of the depressive group showed a significant difference in all average mood scores (p=0.0001) compared to the control group. In addition, a significant decrease (P=0.0001) in leisure-time physical activity scores was reported among subjects with depression compared to those of the control group (Table 1).
In this experiment, a significant improvement in depressive mood profile was achieved in the subjects of both control and depressive groups following 12 weeks of moderate aerobic training as shown in Table 2. Compared to pre-test results, all parameters of mood profiles; anger, fatigue, vigor, tension, and total mood score were significantly improved in the subjects of control and depressive groups following exercise training for 12 weeks respectively as shown in Table 2.
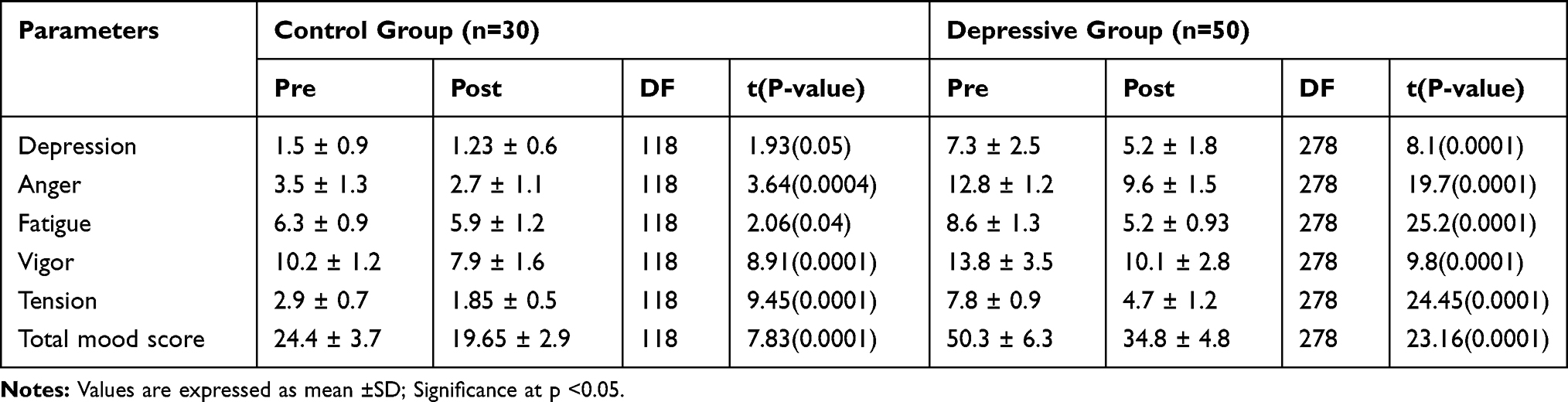 |
Table 2 Mood Scores in Studied Subjects Following 12 Weeks Supervised Aerobic Training Program (Means ± SD) |
The change in the expression levels of the adrenal hormones; cortisol, DHEA, cortisol:DHEA ratio, ACTH, and Corticosterone serum concentrations were estimated in this study. There was a significant increase in DHEA and a decrease in the serum levels of cortisol, cortisol:DHEA ratio, ACTH, and Corticosterone of depressive participants compared to the control group following 12 weeks of moderate aerobic training (Table 3). There was a significantly higher change in LPTA in normal and depressive older adults following 12 weeks of aerobic training (P=0.0001) (Table 3).
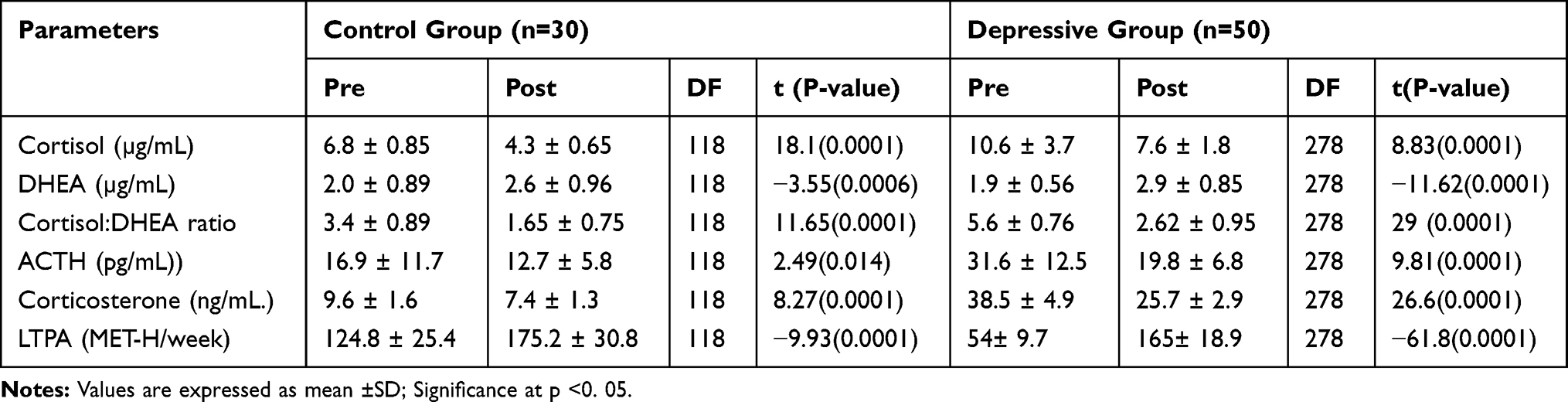 |
Table 3 Change in the Level of Adrenal Hormones and Leisure-Time Physical Activity (LTPA) Score of Participants Following 12 Weeks Supervised Aerobic Training Program (Means ± SD) |
According to physical activity status, the depressive participants are classified into two groups low LPTA group (n=20) and high LPTA (n=120). The data obtained showed that the improvement in serum levels of adrenal hormones significantly correlated with the status of physical activity (LPTA-MET-H/W) in all depressive participants as reported in a Table 4.
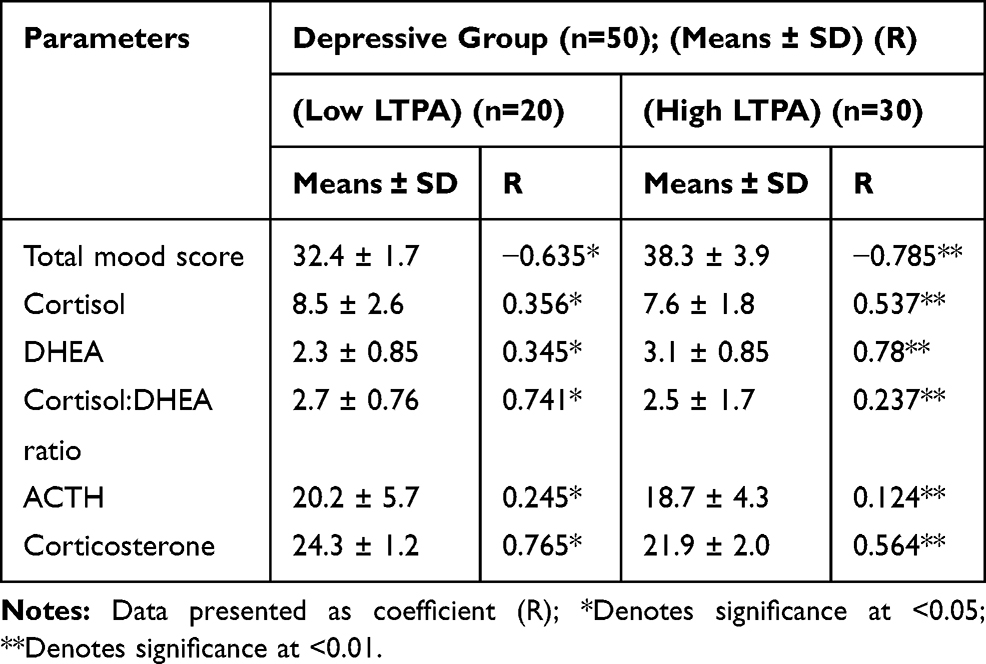 |
Table 4 Post Training Correlation Analysis of Adrenal Hormones and Depressive-Related Variables According to the Level of Leisure-Time Physical Activity (LPTA-MET-H/Week) After 12 Weeks of Exercise |
Regarding gender, a significant difference in physical activity profile (LPTA-MET-H/W), adrenal blood hormones, and total mood profile was reported in female and male participants. There was a higher mood profile associated with a higher change in adrenal hormones and lower LPTA status in female compared to male participants pre- and post-exercise program (Figures 2 and 3).
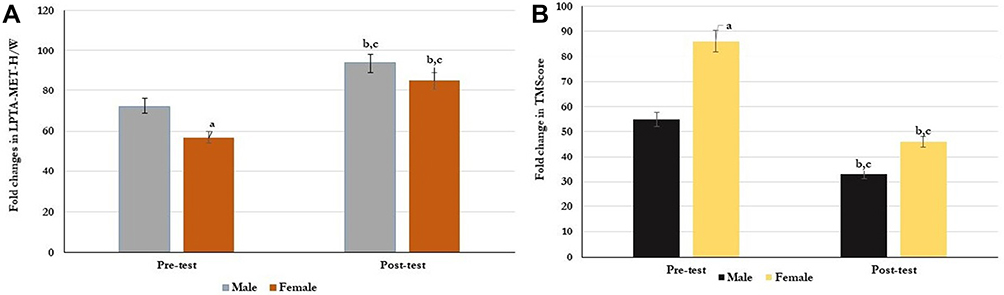 |
Figure 2 Association between gender, Physical activity (LPTA) (A), depression (total mood score; Score) (B) in older adults at Pre- and Post-exercise training. Significant improve in physical activity (A) and depression (B) was reported in males compared to females following 12 week of exercise training. ap= 0.05 (male vs female at baseline), bp=0.01 (male vs female after 12 week of exercise training), cp =0.001 (pre-test vs post-test for male/female). |
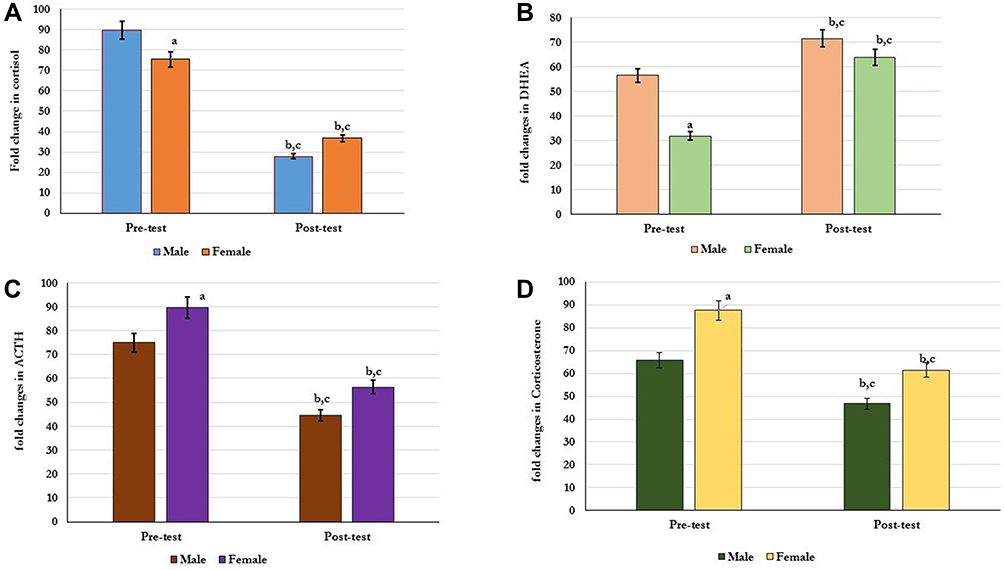 |
Figure 3 Association between gender and the profile of adrenal hormones in older adults at Pre- and Post-exercise training. Following 12 week of exercise training, males showed significant improve in the levels of cortisol (A), DHEA (B), ACTH (C), and corticosterone (D) compared to females. ap= 0.05 (male vs female at baseline), bp=0.01 (male vs female after 12 week of exercise training), cp =0.001 (pre-test vs post-test for male/female). |
Physical activity (p=0.05) showed to be higher in males compared to females at baseline (Figure 2A), whoever both genders showed a significant increase (p=0.001) in the scores of physical activity after exercise test as shown in Figure 2A. Also, total depressive scores (TMscores) were significantly higher (p=0.05) in females compared to males (Figure 2B). In both genders, TM-scores were significantly (p=0.001) reduced following exercise test for 12 weeks, however, more improvement in the scores of TMS was reported in males than females (p=0.01) (Figure 2B).
Adrenal hormones significantly improved (p=0.001) in all participants following exercise graining (Figure 3). A significant decrease in the levels of cortisol, ACTH, and Corticosterone with a significant increase in the levels of DHEA was reported in both genders after exercise test as shown in Figure 3A–D. However, males showed more improvements than females (p=0.01).
Discussions
In older populations, the occurrence of psychological and depressive disorders significantly attributed to physical inability.12 The drastic effects of physical problems increase the incidence of depression criteria among older people.13 It was reported that exercise plays a significant role as a means of physical rehabilitation to conserve the fitness and health of the human body. Previously, most studies showed that physically active bodies showed a remarkable decrease in depression states via a change in all parameters of their lifestyle,87,88 however, the exact mechanism of action is unknown.89
Therefore, in this current research work, we examined the mechanistic role performed by the supervised aerobic exercise of moderate intensity in reducing depressive mood side effects in older ages. We proposed that the improvement of physical fitness could change the depressive mood of older adults via the buffering of adrenal hormones.
The results from our analyses showed an increase in depressive mood scores and significant change in the level of adrenal hormones among older adults with physical inactivity. The data obtained are in line with those who reported a link of mood disorders such as anxiety and depression with disability and loss of health among older adults of both genders.90 However, more emotional benefits and low depression were clearly reported in subjects with physically active and could confront physical health challenges.12,81
In this current study, the data showed a significant difference between male and female participants in depressive mood score, physical activity, and change in the level of adrenal hormones. This matched with other studies, which confirmed a higher incidence of depression among females with longer age rather than males.91 This may be related to higher neural disorders among the female gender, especially in older ages.92 In addition, the previous study concluded that women have a higher response to HPA disorders under daily life stress than males, which facilitate the development of depression via the elevation of cortisol levels.93
Regarding the change in adrenal hormones, our data showed a significant increase in serum cortisol, corticosterone (CORT), ACTH, cortisol:DHEA/S ratio, and decrease in DHEA in older adults with depression. The data are in agreement with other studies that reported that patients with higher depressive and stress incidence scores showed an abnormality in adrenal hormones such as an increase in serum levels of cortisol, corticosterone (CORT), ACTH, cortisol:DHEA ratio, and decrease in DHEA/S.94–98 In addition, the results support the potential roles of cortisol and corticosterone (CORT) in the expression of aldosterone that aids in the prognosis of psychological stress and cardiovascular outcomes.95,99
Favorable positive effects on physiological, psychological, and immunological functions were reported following regular exercise interventions,100 therefore it necessary to study the relationship between physical activity status, depressive mood, and subsequent alteration in the secretion of adrenal hormones in older adults.
In the present study, a significant improvement in mood profile, the levels of adrenal hormones, and a significant increase in physical activity (LPTA=MET-H/W) were observed among all participants of control and depressive groups. However, in relation to gender, significant improvement in depression mood profile with optimizing response in the levels of adrenal hormones and an increase in LPTA status was reported in males more than females’ participants following 12 weeks of supervised moderate aerobic exercise. These observations were in accordance with previous results which showed greater improvements in depression, anxiety and stress following 12-week aerobic training program,101,102 or at 6 month’s follow-up,102 or after 10-weeks of walking intervention on participants with depression, anxiety, and obsessive-compulsive disorders.104
The results of the current study are in harmony with previous studies, which focused upon the effect of physical activity on depression via controlling adrenal hormones secretion.104–107 It was shown that physical exercise interventions were proposed to protect against changes in the adrenal system with aging.105
The current study demonstrated that the level of DHEA hormone was elevated significantly after exercise in both control and depressive groups of our adult participants as compared to the pre-exercise level respectively. After exercise interventions for 12 weeks, the results showed that there was a highly significant correlation (P= 0.01, r= 0.78) between the level of DHEA/S hormone and physical activity level (LPTA). This result matched with previous studies, which had shown that DHEA/S levels increase in response to exercise.108 Exercise increased the production of DHEAS from the adrenal cortex through the hypothalamus-pituitary-adrenal axis.109 In addition, most studies reported that the change in the level of DHEA depends mainly upon the type and intensity of exercise test,110–112 however, our study showed contrary results with those who not able to define any increase in the level of DHEA/S in older adults.112
In this study, a reduction in the level of the adrenal hormones was reported in both healthy control and adults with depressive mood following supervised exercise interventions for 12 weeks. The data showed a significant decrease in the levels of cortisol, ACTH, and corticosterone in control and depressive groups of our adult participants as compared to the pre-exercise level respectively. In relation to the decrease in cortisol, cortisol:DHEA/S ratio of the studied older subjects significantly decreased immediately post-exercise.
The data of the present study were in line with Heaney et al,97 who showed a significant decrease in serum cortisol, cortisol:DHEA/S ratio and increase in DHEA/S levels in older adults who regularly participated in aerobic exercise compared to adrenal hormones of sedentary individuals with higher stress incidence scores. In addition, the change in ACTH and corticosterone levels was in accordance with those who reported decreased plasma ACTH and corticosterone levels following physical exercise.113,114 The obtained data signify the role of supervised aerobic exercise interventions in modulating the effects of the HPA axis, which mediate the reactivity of the human body against depression disorders.115–117
Conclusions
The findings of this study showed that 12 weeks of supervised exercise interventions are promising non-drug therapeutic strategies in improving depression among older adults. The potential performance in a psychological state occurs physiologically via optimizing the levels of the hormones of the HPA axis.
Acknowledgments
The authors are grateful to the Deanship of Scientific Research, King Saud University for funding through Vice Deanship of Scientific Research Chairs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR.
2. Austin MP, Mitchell P, Wilhelm K, et al. Cognitive function in depression: a distinct pattern of frontal impairment in melancholia? Psychol Med. 1999;29:73–85. doi:10.1017/S0033291798007788
3. Beats BC, Sahakian BJ, Levy R. Cognitive performance in tests sensitive to frontal lobe dysfunction in the elderly depressed. Psychol Med. 1996;26:591–603. doi:10.1017/S0033291700035662
4. Nebes RD, Butters MA;, Mulsant BH, et al. Decreased working memory and processing speed mediate cognitive impairment in geriatric depression. Psychol Med. 2000;30:679–691. doi:10.1017/S0033291799001968
5. Blazer DG. Mood disorders: epidemiology. In: Sadock BJ, Sadock VA, editors. Comprehensive Textbook of Psychiatry New York: Lippincott Williams & Wilkins. 2000:1298–1308.
6. Kindermann SS, Brown GG. Depression and memory in the elderly: a meta-analysis. J Clin Exp Neuropsychol. 1997;19:625–642. doi:10.1080/01688639708403749
7. Lockwood KA, Alexopoulos GS, Kakuma T, Van Gorp WG. Subtypes of cognitive impairment in depressed older adults. Am J Geriatr Psychiatr. 2000;8:201–208. doi:10.1097/00019442-200008000-00004
8. Boone K, Lesser B, Miller B, et al. Cognitive functioning in a mildly to moderately depressed geriatric sample: relationship to chronological age. J Neuropsychiatr Clin Neurosci. 1994;6:267–272.
9. Butters MA, Becker JT, Nebes RD, et al. Changes in cognitive functioning following treatment of late-life depression. Am J Psychiatry. 2000;157:1949–1954. doi:10.1176/appi.ajp.157.12.1949
10. Koenig HG, Blazer DG. Mood disorders. In: Blazer DJ, Steffens DC, Busse EW, editors. Textbook of Geriatric Psychiatry.. Arlington, VA: American Psychiatric Publishing; 2004.
11. Rapp MA, Dahlman K, Sano M, Grossman HT, Haroutunian V, Gorman JM. Neuropsychological differences between late-onset and recurrent geriatric major depression. Am J Psychiatr. 2005;162:691–698. doi:10.1176/appi.ajp.162.4.691
12. Lenze EJ, Rogers JC, Martire LM, et al. The association of late-life depression and anxiety with physical disability: A review of the literature and prospectus for future research. Am J Geriatr Psychiatr. 2001;9:113–135. doi:10.1097/00019442-200105000-00004
13. Oeppen J, Vaupel JW. Broken limits to life expectancy. Science. 2002;296:1029–1031. doi:10.1126/science.1069675
14. Schulz R, Martire LM, Beach SR, Scheier MF. Depression and mortality in the elderly. Curr Dir Psychol Sci. 2000;9:204–208. doi:10.1111/1467-8721.00095
15. Otte C, Hart S, Neylan TC, Marmar CR, Yaffe K, Mohr DC. A meta-analysis of cortisol response to challenge in human aging: importance of gender. Psychoneuroendocrinology. 2005;30:80–91. doi:10.1016/j.psyneuen.2004.06.002
16. McEwen BS. Mood disorders and allostatic load. Biol Psychiatry. 2003;54:200–207. doi:10.1016/S0006-3223(03)00177-X
17. Gotovac K, Sabioncello A, Rabatic S, Berki T, Dekaris D. Flow cytometric determination of glucocorticoid receptor (GCR) expression in lymphocyte subpopulations: lower quantity of GCR in patients with post-traumatic stress disorder (PTSD). Clin Exp Immunol. 2003;131:335–339. doi:10.1046/j.1365-2249.2003.02075.x
18. Checkley S. The neuroendocrinology of depression and chronic stress. BMJ. 1996;52:597–617.
19. Bauer M, Jeckel CMM, Luz C. The role of stress factors during aging of the immune system. Ann NY Acad Sci. 2009;1153:139–152. doi:10.1111/j.1749-6632.2008.03966.x
20. Pauli R, Souza L, Rogatto G, Gomes R, Luciano E. Glicocorticóides e síndrome metabólica: aspectos favoráveis do exercício físico nesta patofisiologia. Rev Port Cien Desp. 2006;6:217–228.
21. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159:2349–2356. doi:10.1001/archinte.159.19.2349
22. Urhausen A, Gabriel H, Kindermann W. Blood hormones as markers of training stress and overtraining. Sports Med. 1995;20(4):251–276. doi:10.2165/00007256-199520040-00004
23. Platje E, Vermeiren R, Branje SJ, et al. Long-term stability of the cortisol awakening response over adolescence. Psychoneuroendocrinology. 2013;38(2):271–280. doi:10.1016/j.psyneuen.2012.06.007
24. Klimes-Dougan B, Hastings PD, Granger DA, Usher BA, Zahn-Waxler C. Adrenocortical activity in at-risk and normally developing adolescents: individual differences in salivary cortisol basal levels, diurnal variation, and responses to social challenges. Dev Psychopathol. 2001;13(3):695–719. doi:10.1017/S0954579401003157
25. Rotenberg S, McGrath JJ, Roy-Gagnon M-H, Tu MT. Stability of the diurnal cortisol profile in children and adolescents. Psychoneuroendocrinology. 2012;37(12):1981–1989. doi:10.1016/j.psyneuen.2012.04.014
26. Kalimi M, Shafagoj Y, Loria R, Regelson W, Padgett D, Regelson W. Antiglucocorticoid effects of dehydroepiandrosterone (DHEA). Mol Cell Biochem. 1994;131:99–104. doi:10.1007/BF00925945
27. Maninger N, Wolkowitz OM, Reus VI, Epel ES, Mellon SH. Neurobiological and neuropsychiatric effects of dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEAS). Front Neuroendocrinol. 2009;30(1):65–91. doi:10.1016/j.yfrne.2008.11.002
28. Morgan CA, Southwick S, Hazlett G, et al. Relationships among plasma dehydroepiandrosterone sulfate and cortisol levels, symptoms of dissociation, and objective performance in humans exposed to acute stress. Arch Gen Psychiatry. 2004;61(8):819. doi:10.1001/archpsyc.61.8.819
29. Kroboth P, Salek F. DHEA and DHEA-S: a review. J Clin Psychopharmacol. 1999;39:327–348.
30. Jiang X, Zhong W, An H, et al. Attenuated DHEA and DHEA-S response to acute psychosocial stress in individuals with depressive disorders. J Affect Disord. 2017;215:118–124. doi:10.1016/j.jad.2017.03.013
31. Yen SS. Dehydroepiandrosterone sulfate and longevity: new clues for an old friend. Proc Natl Acad Sci U S A. 2001;98(15):8167–8169. doi:10.1073/pnas.161278698
32. Hartkamp A, Geenen R, Godaert GLR, et al. Effect of dehydroepiandrosterone administration on fatigue, well-being, and functioning in women with primary Sjogren syndrome: a randomised controlled trial. Ann Rheum Dis. 2008;67(1):91–97. doi:10.1136/ard.2007.071563
33. Alhaj HA, Massey AE, McAllister-Williams RH, McAllister-Williams R, McAllister-Williams H. Effects of DHEA administration on episodic memory, cortisol and mood in healthy young men: a double-blind, placebo-controlled study. Psychopharmacologia. 2006;188(4):541–551. doi:10.1007/s00213-005-0136-y
34. Van Niekerk JK, Huppert FA, Herbert J. Salivary cortisol and DHEA: association with measures of cognition and well-being in normal older men, and effects of three months of DHEA supplementation. Psychoneuroendocrinology. 2001;26:591–612. doi:10.1016/S0306-4530(01)00014-2
35. Shields GS, Sazma MA, Yonelinas AP. The effects of acute stress on core executive functions: a meta-analysis and comparison with cortisol. Neurosci Biobehav Rev. 2016;68:651–668. doi:10.1016/j.neubiorev.2016.06.038
36. Cho S, Park WJ, Kang W, et al. The association between serum dehydroepiandrosterone sulfate (DHEAS) levels and job-related stress among female nurses. Ann Occup Environ Med. 2019;31:e18. doi:10.35371/aoem.2019.31.e18
37. Ferrari E, Cravello L, Falvo F, et al. Neuroendocrine features in extreme longevity. Exp Gerontol. 2008;43:88–94. doi:10.1016/j.exger.2007.06.010
38. Ferrari E, Cravello L, Muzzoni B, et al. Age-related changes of the hypothalamic-pituitary-adrenal axis: pathophysiological correlates. Eur J Endocrinol. 2001;144:319–329. doi:10.1530/eje.0.1440319
39. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381:752–762. doi:10.1016/S0140-6736(12)62167-9
40. Allard JB, Duan C. Comparative endocrinology of aging and longevity regulation. Front Endocrinol. 2011;2:75. doi:10.3389/fendo.2011.00075
41. Ohlsson C, Vandenput L, Tivesten A. DHEA and mortality: what is the nature of the association? J Steroid Biochem Mol Biol. 2015;145:248–253. doi:10.1016/j.jsbmb.2014.03.006
42. Barrett-Connor E, Goodman-Gruen D. The epidemiology of DHEAS and cardiovascular disease. Ann N Y Acad Sci. 1995;774:259–270. doi:10.1111/j.1749-6632.1995.tb17386.x-i1
43. McEwen BS. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev. 2007;87(3):
44. Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. 2009;10(6):
45. Funder JW. Reconsidering the roles of the mineralocorticoid receptor. Hypertension. 2009;53(2):286–290. doi:10.1161/HYPERTENSIONAHA.108.119966
46. Natasa H, Paul D, Wes MO, et al. Subchronic treatment with aldosterone induces depression-like behaviours and gene expression changes relevant to major depressive disorder. Int J Neuro Psycho Pharmacol. 2012;15(2):247–265. doi:10.1017/S1461145711000368
47. Inder WJ, Hellemans J, Swanney MP, Prickett TC, Donald RA. Prolonged exercise increases peripheral plasma ACTH, CRH and AVP in male athletes. Med Sci Sports Exerc. 1998;85(3):835–841.
48. Smilios I, Pilianidis T, Karamouzis M, Tokmakidis SP. Hormonal responses after various resistance exercise protocols. Med Sci Sports Exerc. 2002;35(4):644–654. doi:10.1249/01.MSS.0000058366.04460.5F
49. Sephton SE, Sapolsky RM, Kraemer HC, Spiegel D. Diurnal cortisol rhythm as a predictor of breast cancer survival. J Natl Cancer Inst. 2000;92:994–1000. doi:10.1093/jnci/92.12.994
50. Andersen ML, Bignotto M, Machado RB, Tufik S. Different stress modalities result in distinct steroid hormone responses by male rats. Braz J Med Biol Res. 2004;37(6):791–797. doi:10.1590/S0100-879X2004000600003
51. Brosse AL, Sheets ES, Lett HS, Blumenthal JA. Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Med. 2002;32:741–760. doi:10.2165/00007256-200232120-00001
52. Blumenthal JA, Sherwood A, Rogers SD, et al. Understanding prognostic benefits of exercise and antidepressant therapy for persons with depression and heart disease: the UPBEAT study – rationale, design, and methodological issues. Clin Trials. 2007;4:548–559. doi:10.1177/1740774507083388
53. Kok RM, Reynolds CF. Nonpharmacologic treatments for depression in older adults-reply. JAMA. 2017;318:1284. doi:10.1001/jama.2017.12024
54. Moraes H, Deslandes A, Ferreira C, Pompeu FAMS, Ribeiro P, Laks J. O exercício físico no tratamento da depressão em idosos: revisão sistemática. Rev Psiquiatr Rio Gd Sul. 2007;29:70–79. doi:10.1590/S0101-81082007000100014
55. Deslandes AC, Moraes H, Alves H, et al. Effect of aerobic training on EEG alpha asymmetry and depressive symptoms in the elderly: a 1-year follow-up study. Braz J Med Bio Res. 2010;43(6):585–592. doi:10.1590/S0100-879X2010007500041
56. Silveira H, Deslandes AC, de Moraes H, et al. Effects of exercise on electroencephalographic mean frequency in depressed elderly subjects. Neuropsychobiology. 2010;61:141–147. doi:10.1159/000279304
57. Silveira H, Moraes H, Oliveira N, Coutinho ESF, Laks J, Deslandes A. Physical exercise and clinically depressed patients: a systematic review and meta-analysis. Neuropsychobiology. 2013;67:61–68. doi:10.1159/000345160
58. Deslandes A, Moraes H, Ferreira C, et al. Exercise and mental health: many reasons to move. Neuropsychobiology. 2009;59:191–198. doi:10.1159/000223730
59. Schuch FB, Deslandes AC, Stubbs B, Gosmann NP, Silva CTB, Fleck MPA. Neurobiological effects of exercise on major depressive disorder: A systematic review. Neurosci Biobehav Rev. 2016;61:1–11. doi:10.1016/j.neubiorev.2015.11.012
60. Moraes HS, Deslandes AC, Cevada T, Souza ACFM, Laks J. The effect of physical exercise on cortisol levels in older adults: a systematic review. Rev Bras Ativ Fis Saude. 2012;17:314–320.
61. Stranahan AM, Lee K, Mattson MP. Central mechanisms of HPA axis regulation by voluntary exercise. Neuromolecular Med. 2008;10:118–127. doi:10.1007/s12017-008-8027-0
62. Foley LS, Prapavessis H, Osuch EA, De Pace JA, Murphy BA, Podolinsky NJ. An examination of potential mechanisms for exercise as a treatment for depression: A pilot study. Ment Health Phys Act. 2008:69–73.
63. Nabkasorn C, Miyai N, Sootmongkol A, et al. Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. Eur J Public Health. 2006;16:179–184. doi:10.1093/eurpub/cki159
64. Vedamurthachar A, Janakiramaiah N, Hegde JM, et al. Antidepressant efficacy and hormonal effects of Sudarshana Kriya Yoga (SKY) in alcohol dependent individuals. J Affect Disord. 2006;94:249–253. doi:10.1016/j.jad.2006.04.025
65. Chan ES, Koh D, Teo YC, HjTamin R, Lim A, Fredericks S. Biochemical and psychometric evaluation of Self-Healing Qigong as a stress reduction tool among first year nursing and midwifery students. Complement Ther Clin Pract. 2013;19:179–183. doi:10.1016/j.ctcp.2013.08.001
66. Krogh J, Nordentoft M, Mohammad-Nezhad M, Westrin A. Growth hormone, prolactin and cortisol response to exercise in patients with depression. J Affect Disord. 2010;125:189–197. doi:10.1016/j.jad.2010.01.009
67. Carneiro LS, Mota MP, Vieira‑Coelho MA, Alves RC, Fonseca AM, Vasconcelos‑Raposo J. Monoamines and cortisol as potential mediators of the relationship between exercise and depressive symptoms. Eur Arch Psychiatry Clin Neurosci. 2017;267:117–121. doi:10.1007/s00406-016-0719-0
68. Moraes HS, Silveira HS, Oliveira NA, et al. Is Strength Training as Effective as Aerobic Training for Depression in Older Adults? A Randomized Controlled Trial. Neuropsychobiology. 2020;79(2):
69. Beserra AHN, Kameda P, Deslandes AC, Schuch FB, Laks J, Moraes HS. Can physical exercise modulate cortisol level in subjects with depression? A systematic review and meta-analysis. Trends Psychiatr Psychother. 2018;40(4):360–368. doi:10.1590/2237-6089-2017-0155
70. Greer TL, Furman JL, Trivedi MH. Evaluation of the benefits of exercise on cognition in major depressive disorder. Gen Hosp Psychiatry. 2017;49:19–25. doi:10.1016/j.genhosppsych.2017.06.002
71. Schuch FB, Dunn AL, Kanitz AC, Delevatti RS, Fleck MP. Moderators of response in exercise treatment for depression: A systematic review. J Affect Disord. 2016;195:40–49. doi:10.1016/j.jad.2016.01.014
72. Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J Psychiatr Res. 2016;77:42–51. doi:10.1016/j.jpsychires.2016.02.023
73. Jaworska N, Courtright AK, De Somma E, MacQueen GM, MacMaster FP. Aerobic exercise in depressed youth: A feasibility and clinical outcomes pilot. Early Interv Psychiatry. 2019;13(1):128–132. doi:10.1111/eip.12537
74. Pajonk FG, Wobrock T, Gruber O, et al. Hippocampal plasticity in response to exercise in schizophrenia. Arch Gen Psychiatry. 2010;67(2):133–143. doi:10.1001/archgenpsychiatry.2009.193
75. Carter T, Guo B, Turner D, et al. Preferred intensity exercise for adolescents receiving treatment for depression: A pragmatic randomised controlled trial. BMC Psychiatr. 2015;15:247. doi:10.1186/s12888-015-0638-z
76. Radovic S, Gordon MS, Melvin GA. Should we recommend exercise to adolescents with depressive symptoms? A meta-analysis. J Paediatr Child Health. 2017;53(3):214–220. doi:10.1111/jpc.13426
77. Smoak B, Deuster PA, Rabin D, Chrousos GP. Corticotropin-releasing hormone is not the sole factor mediating exercise-induced adrenocorticotropin release in humans. J Clin Endocrinol Metabol. 1991;73:302–306. doi:10.1210/jcem-73-2-302
78. Duclos M, Guinot M, Le Bouc Y. Cortisol and GH: odd and controversial ideas. App Physiol Nutr Metabol. 2007;32(5):895–903. doi:10.1139/H07-064
79. Tsuji I, Tamagawa A, Nagatomi R, et al. Randomized controlled trial of exercise training for older people (Sendai Silver Center Trial: SSCT): study design and primary outcome. J Epidemiol. 2000;10:55–64. doi:10.2188/jea.10.55
80. Wald FDM, Mellenbergh GJ. The short Dutch version of the Profile of Moods States (POMS) questionnaire. Ned Tijdschr Psychol. 1990;45:86–90.
81. Wicherts JM, Vorst HCM. Model adaptation of the short version of the profile of moods states and variance between males and females. Ned Tijdschr Psychol. 2004;59:2–21.
82. Likert R. A Technique for the Measurement of Attitudes. Arch Psychol. 1932;140:1–55.
83. Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–1581. doi:10.1249/MSS.0b013e31821ece12
84. Trinh OT, Nguyen ND, van der Ploeg HP;, Dibley MJ, Bauman A. Test-retest repeatability and relative validity of the global physical activity questionnaire in a developing country context. J Phys Act Health. 2009;6(Suppl 1):S46–53. doi:10.1123/jpah.6.s1.s46
85. Karvonen M, Kentala K, Mustala O. The effects of training heart rate: a longitudinal study. Ann Med Exp Biol Fenn. 1957;35:307–315.
86. Cadore E, Izquierdo M, Dos Santos M, et al. Hormonal responses to concurrent strength and endurance training with different exercise orders. J Strength Cond Res. 2012;26:3281–3288. doi:10.1519/JSC.0b013e318248ab26
87. Baker MK, Kennedy DJ, Bohle PL, et al. Efficacy and feasibility of a novel tri-modal robust exercise prescription in a retirement community: A randomized, controlled trial. J Am Geriatr Soc. 2007;55(1):1–10. doi:10.1111/j.1532-5415.2006.01031.x
88. Dishman RK, Berthoud H, Booth FW, et al. Neurobiology of exercise. Obesity. 2006;14(3):345–356. doi:10.1038/oby.2006.46
89. Craft LL, Perna FM. The benefits of exercise for the clinically depressed. Prim Care Companion J Clin Psychiatry. 2004;6(3):104–111. doi:10.4088/PCC.v06n0301
90. Mathers C, Fat G, Boema JT. The Global Burden of Disease: 2004 Update. Geneva, Switzerland: World Health Organization; 2008.
91. Kendler KS, Thornton LM, Prescott CA. Gender differences in the rates of exposure to stressful life events and sensitivity to their depressogenic effects. Am J Psychiatr. 2001;158:587–593. doi:10.1176/appi.ajp.158.4.587
92. Goodwina RD, Gotlib IH. Gender differences in depression: the role of personality factors. Psychiatry Res. 2004;126:135–142. doi:10.1016/j.psychres.2003.12.024
93. Weiss EL, Longhurst JG, Mazure CM. Childhood sexual abuse as a risk factor for depression in women: psychosocial and neurobiological correlates. Am J Psychiatr. 1999;156:816–828. doi:10.1176/ajp.156.6.816
94. Brown ES, Woolston JD, Fro A, et al. Hippocampal volume, spectroscopy, cognition, and mood in patients receiving corticosteroid therapy. Biol Psychiatry. 2004;55:538–545. doi:10.1016/j.biopsych.2003.09.010
95. Sonino N, Fallo F, et al. Psychological aspects of primary aldosteronism. Psychother Psychosom. 2006;75(5):327–330. doi:10.1159/000093956
96. Cizza G, Ronsaville DS, Kleitz H, et al. Clinical Subtypes of Depression Are Associated with Specific Metabolic Parameters and Circadian Endocrine Profiles in Women: the Power Study. PLoS One. 2012;7(1):e28912. doi:10.1371/journal.pone.0028912
97. Heaney JLJ, Carroll D, Phillips AC. Physical Activity, Life Events Stress, Cortisol, and DHEA in Older Adults: preliminary Findings that Physical Activity May Buffer Against the Negative Effects of Stress. J Aging Phys Act. 2014;22(4):465–473. doi:10.1123/JAPA.2012-0082
98. Wong SY, Leung JC, Kwok T, et al. Low DHEAS levels are associated with depressive symptoms in elderly Chinese men: results from a large study. Asian J Androl. 2011;13(6):898–902. doi:10.1038/aja.2011.116
99. Kubzansky LD, Adler GK. Aldosterone: a forgotten mediator of the relationship between psychological stress and heart disease. Neurosci Biobehav Rev. 2010;34(1):
100. Mackinnon LT. Chronic exercise training effects on immune function. Med Sci Sports Exerc. 2000;32:S369–S376. doi:10.1097/00005768-200007001-00001
101. Abrantes A, Strong D, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23:923–927. doi:10.1016/j.janxdis.2009.06.008
102. Brown R, Abrantes A, Strong D, et al. A pilot study of moderate-intensity aerobic exercise for obsessive compulsive disorder. J Nerv Ment Dis. 2007;195:514–520. doi:10.1097/01.nmd.0000253730.31610.6c
103. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders: A pilot group randomized trial. J Anxiety Disord. 2008;22:959–968. doi:10.1016/j.janxdis.2007.09.010
104. Otte C, Marmar CR, Pipkin SS, Moos R, Browner W, Whooley M. Depression and 24-hour urinary cortisol in medical outpatients with coronary heart disease: the heart and soul study. Biol Psychiatry. 2004;56:241–247. doi:10.1016/j.biopsych.2004.06.003
105. Tremblay M, Copeland J, Van Helder W. Effects of training status and exercise mode on endogenous steroid hormones in men. J Appl Physiol. 2004;96:531–539. doi:10.1152/japplphysiol.00656.2003
106. Phillips AC, Burns VE, Lord JM. Stress and exercise: getting the balance right for aging immunity. Exerc Sport Sci Rev. 2007;35(1):35–39. doi:10.1097/jes.0b013e31802d7008
107. Jassim HA, Ja’ffar JI, Hussein AG. Effect of Moderate Exercise on the level of DHEAS hormone and lymphocyte apoptosis in healthy subjects. Faculty Medicine Baghdad. 2010;52(2):223–227.
108. Dressendorfer R, Wade C. Effects of a 15-d race on plasma steroid levels and leg muscle fitness in runners. Med Sci Sports Exerc. 1991;23(8):954–958. doi:10.1249/00005768-199108000-00012
109. Mayer EA, Fanselow MS. Dissecting the components of the central response to stress. Nat Neurosci. 2003;6:1011–1012. doi:10.1038/nn1003-1011
110. Copeland JL, Consitt LA, Tremblay MS. Hormonal responses to endurance and resistance exercise in females aged 19–69 years. The Journals of Gerontology. Series A. Biol Sci Med Sci. 2002;57:B158–B165. doi:10.1093/gerona/57.4.B158
111. Giannopoulou I, Carhart R, Sauro LM, Kanaley JA. Adrenocortical responses to submaximal exercise in postmenopausal Black and White women. Metabolism. 2003;52:1643–1647. doi:10.1016/S0026-0495(03)00312-3
112. Aldred S, Rohalu M, Edwards K, Burns V. Altered DHEA and DHEAS response to exercise in healthy older adults. J Aging Phys Act. 2009;17:77–88. doi:10.1123/japa.17.1.77
113. Salmon P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: a unifying theory. Clin Psychol Rev. 2001;21:33–61. doi:10.1016/S0272-7358(99)00032-X
114. Droste SK, Gesing A, Ulbricht S, Müller MB, Linthorst AC, Reul JM. Effects of long-term voluntary exercise on the mouse hypothalamic- pituitary adrenocortical axis. Endocrinology. 2003;144:3012–3023. doi:10.1210/en.2003-0097
115. Dimeo F, Bauer M, Varahram I, Proest G, Halter U. Benefits from aerobic exercise in patients with major depression: a pilot study. Br J Sports Med. 2001;35(2):114–117. doi:10.1136/bjsm.35.2.114
116. Lai SM, Studenski S, Richards L, et al. Therapeutic exercise and depressive symptoms after stroke. Am Geriatr Soc. 2006;54(2):240–247. doi:10.1111/j.1532-5415.2006.00573.x
117. Lampinen P, Heikkinen RL, Ruoppila I. Changes in intensity of physical exercise as predictors of depressive symptoms among older adults: an eight-year follow-up. Prev Med. 2000;30(5):371–380. doi:10.1006/pmed.2000.0641
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.