")
Back to Journals » Clinical Interventions in Aging » Volume 15
Higher Normal Levels of Triglyceride and Low and High-Density Lipoprotein Cholesterol Might Have a Protective Effect Against Activities of Daily Living Disability Within Chinese Female Centenarians: A Cross-Sectional, Complete Sample Study
Authors Wang S , Liu M , Yang S , Wang J, Jia W, Cao W, Han K , He Y
Received 6 November 2019
Accepted for publication 26 January 2020
Published 14 February 2020 Volume 2020:15 Pages 225—237
DOI https://doi.org/10.2147/CIA.S237505
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Shengshu Wang,1 Miao Liu,1,2 Shanshan Yang,1 Jianhua Wang,1,2 Wangping Jia,1 Wenzhe Cao,1 Ke Han,1 Yao He1,2
1Institute of Geriatrics, The 2nd Medical Center, Beijing Key Laboratory of Aging and Geriatrics, National Clinical Research Center for Geriatrics Diseases, Chinese People’s Liberation Army General Hospital, Beijing 100853, People’s Republic of China; 2State Key Laboratory of Kidney Diseases, Chinese People’s Liberation Army General Hospital, Beijing 100853, People’s Republic of China
Correspondence: Yao He
Institute of Geriatrics, The 2nd Medical Center, Beijing Key Laboratory of Aging and Geriatrics, National Clinical Research Center for Geriatrics Diseases, State Key Laboratory of Kidney Diseases, Chinese People’s Liberation Army General Hospital, Beijing 100853, People’s Republic of China
Tel +86 10-66876415
Fax +86 10-68219351
Email [email protected]
Background and Objective: Activities of daily living (ADL) disability seriously affects the quality of life in the elderly. This study aims to examine the prevalence of ADL disability and its possible correlation with lipid profile indicators (LDL-C, TG and HDL-C) among female centenarians in Hainan, China.
Methods: A cross-section of complete sample study including 822 female centenarians was conducted from the China Hainan Centenarians Cohort Study (CHCCS) from June 2014 to December 2016. Barthel index was used to estimate ADL disability and multivariate logistic regression model was used to explore the relationship between lipid profile indicator and ADL disability.
Results: A total of 822 female centenarians were recruited in Hainan province, and the median age was 102 (IQR: 101– 104) years, and 244 (29.7%) centenarians had ADL disability. After adjustment, 1 mmol/L increment in LDL-C, TG and HDL-C were associated with 26.4% (aOR=0.736, 95% CI:0.592– 0.915), 29.8% (aOR=0.702, 95% CI:0.521– 0.948) and 60.5% (aOR=0.395, 95% CI:0.257– 0.610) decline in ADL disability of female centenarian, respectively. The prevalence of ADL disability showed downward trend with the increase of the quintile of LDL-C, TG and HDL-C (Ptrend< 0.05). Increment of HDL-C levels had the strongest protective effect against ADL disability.
Conclusion: We concluded that a new possible association of higher normal lipid profile indicators, especially HDL-C, might have a protective effect on ADL disability among female centenarians.
Keywords: centenarian, low-density lipoprotein cholesterol, LDL-C, triglyceride, TG, high-density lipoprotein cholesterol, HDL-C, activities of daily living, ADL
Introduction
The aggravating worldwide trend of aging population expands the average life span of human beings with the development of economy, society and medical treatment. Moreover, the number of disabled elderly people and the burden of diseases are also increasing rapidly.1 Activities of daily living (ADL) are an important indicator that reflects the decline or even loss of body function caused by aging, which affects the quality of life, health, and longevity of the elderly.2 In the context of global population aging, human beings need to face the heavy burden of diseases while paying attention to the continuous prolongation of survival time,3 in that the elderly with ADL disability usually need daily care and medical services.4 Centenarians, as a special group of aging population enjoying the longest life span, show delayed or no diseases or factors that cause early death. Therefore, centenarians are regarded as an ideal template for the study on the elderly.5–7 However, at present, the number of studies on ADL disability and related risk factors of centenarians as a template of health and longevity research are very scare.
Dyslipidemia is one of the important risk factors of many chronic noninfectious diseases.8–10 The cholesterol hypothesis suggests that the increment in cholesterol level begins in middle-aged people and becomes more obvious with age, as well as positively correlated with all-cause mortality and related quality of life.11 The prevalence of dyslipidemia is high in adults, but lipids profile in the elderly tends to decline with the increase of age.12 Different blood lipid indicators have different physiological functions, and some studies even believe that the “blood lipid paradox” among the elderly has caused extensive discussion. A normal scope of increase of blood lipid level among the elderly is closely related to good quality of life.13,14 However, the distribution characteristics of blood lipid indicators in centenarians are rarely studied, and their impacts on health are not clear.
Generally, the number of studies on the relationship between lipids profile and ADL disability in the elderly are scarce. Differences are found in the distribution of lipids profile and its effect on health between the elderly and adults. A reasonable range of blood lipid level rise may have a positive effect on reducing ADL disability. According to a Japanese cohort study on the elderly,15 low blood lipid level is related to their decreased level of activity. Moreover, some studies believe that the increase in blood lipid is related to the increase in the recovery rate of ADL disability among the hospitalized disabled elderly, especially the female.16 These findings suggest that higher blood lipid level may lead to better outcomes for ADL, which contradicts the traditional understanding on the effect of blood lipid on health. However, whether this relationship still applies to the longest-living groups of people and how they relate to each other are not clear. Therefore, in this study, the cross-sectional data set of the China Hainan Centenarian Cohort Study (CHCCS) from 2014 to 2016 was used to describe ADL disability and its correlations with LDL-C, TG, and HDL-C.
Materials and Methods
Study Population
This study was conducted from the cross-sectional survey of China Hainan Centenarians Cohort Study (CHCCS), which was based on the community population and was designed as a complete sample prospective cohort study of centenarian throughout the Hainan province in China, and the baseline survey was conducted from June 2014 to December 2016 in the form of household survey of face-to-face interview by the multidisciplinary research team. The design, implementation and methods of CHCCS have been reported previously.7 Briefly, all participants and their relatives were aware of the planned study and the criteria for inclusion and exclusion. The baseline survey included field questionnaire survey, physical/clinical examination and biological specimen collection, and finally included 1002 participants (18.0% male, 82.0% female). In this study, 822 female centenarians in CHCCS were recruited as the subjects. This study was approved by the Ethics Committee of the Chinese People’s Liberation Army General Hospital (Beijing, China). All participants signed the written constant agreement and the study was conducted in accordance with the Helsinki declaration.
Measures
Lipid profiles included LDL-C, TG and HDL-C. Fasting blood samples were collected using four vacutainer tubes (2 mL each) by local experienced nurses with more than 5 years working experience and blood specimens were shaken and placed in a bio-refrigeration box, and then transported to the Laboratory of Hainan Branch of the Chinese PLA General Hospital for testing within 6 hrs. Serum LDL-C, TG and HDL-C were determined by automatic biochemical analyzer. We defined untreated LDL-C ≥ 4.1mmol/L, TG ≥ 2.3 mmol/L and HDL-C < 1.0 mmol/L as dyslipidemia, respectively,17 The levels of LDL-C, TG and HDL-C were analyzed as continuous and quartile variables, respectively.
Other Measurement
Sociodemographic characteristics, including age, gender, ethnicity (Han, ethnic minority), marital status (married, widowed/divorced/unmarried), educational level (illiteracy, primary school and above) and residential type (living together with families, living alone), were assessed at baseline survey. There were three rounds for age validation process to avoid participants from exaggerating their age.7 Then clinical examinations, including the measurement of blood pressure, anthropometric indices, were conducted by the specialized group consisting of experienced geriatricians and trained nurses from the Hainan Branch of the Chinese PLA General Hospital. The blood pressure was measured by an electronic sphygmomanometer (1mmHg = 0.133 kPa) with an accuracy of 1 mmHg, which should be measured twice, and repeated measurement should be made at intervals of 1–2 mins. If the difference between the two results of SBP or DBP was more than 5 mmHg, it should be measured again, and the average of the three results should be recorded.18 Measures of Body Mass Index (BMI) included underweight (<18.5 kg/m2), normal body weight (18.5–24.0 kg/m2), and overweight (≥24.0 kg/m2).19 Fasting blood glucose was determined by automatic biochemical analyzer as long as the fasting blood samples were sent to the laboratory.
In the face-to-face survey, we collected the information on participants’ history of diseases and medication including previous hyperlipidemia or cardiovascular disease, and taking lipid-lowering or cardiovascular medicine. Health-related behaviors were measured by self-reported smoking status, alcohol use,20 and infrequent physical activity was defined as once weekly or less.21
Study Outcome
ADL disability was estimated as study outcomes, and we have conducted a face-to-face interview to assess the ability to perform ADLs and checked through relatives or caregivers, which have been found to be valid and reliable.22 Participants were asked if they have difficulty performing each of 10 ADLs from the Barthel ADL Index (decorating, bathing, dressing, transferring, toileting, eating, walking across a room, climbing the stairs, defecation control and urination control).23,24 The 10 items of Barthel ADL Index are summed to give a score from 0 to 100, and each item has a 0 point for inability to 10 or 15 points for complete dependence. A total Barthel ADL Index score of 0–20 suggests complete dependence, 21–60 severe dependence, 61–95 moderate dependence and 100 complete independence.25 We defined ADL disability as reporting Barthel index score ≤60 in this study.
Statistical Analysis
Statistical analysis was performed by using SPSS version 24.0 (IBM Inc., New York, USA) and the significance of all tests was set at a two-tailed α value of 0.05. Kolmogorov–Smirnov test was used to confirm whether continuous variables subject to normal distribution. In this study, all continuous variables do not subject to the normal distribution, so the Kruskal–Wallis test was used to estimate the difference, and the results were represented by median and interquartile range (IQR). Chi-square test was used to estimate the difference of categorical variable and the results were represented by number and percentage. Multivariable cumulative logistic regression models were used to detect the relationship after adjusting ages, nationality, marital status, educational level, residential type, BMI, Glucose and DBP, smoking, drinking, physical activity, and continuous and Quintile variables of LDL-C, TG and HDL-C were used as independent variables and ADL disability as dependent variables. In sensitivity analyses, we excluded participants with current and previous hyperlipidemia, cardiovascular disease, and taking lipid-lowering/cardiovascular medicine, to examine the association with indicators of lipid profiles and ADL disability in female centenarian without dyslipidemia and cardiovascular disease. Meanwhile, we also examine the correlation among the excluded participants.
GraphPad Prism version 8.0 (GraphPad Software Inc, USA) was used to draw the association graph of distribution characteristic and STATA version 15.0 (Stata Corp, USA) was used to draw the restricted cubic splines to display the correlation between LDL-C, TG, HDL-C and ADL disability.
Results
Among 822 female centenarians recruited from June 2014 to June 2016 in Hainan province, the median age was 102 (IQR: 101–104) years, 244 (29.7%) centenarians were ADL disability. Tables 1–3 show that, with the increase of the quintiles of LDL-C, TG and HDL-C, the proportion of ADL disability decreases gradually (Ptrend≤0.01), and the levels of BMI and DBP in centenarian show an upward trend, while distribution trend of FPG shows an inverted “U” shape.
 |
Table 1 General Characteristics of Low-Density Lipoprotein Cholesterol Among Hainan Female Centenarians |
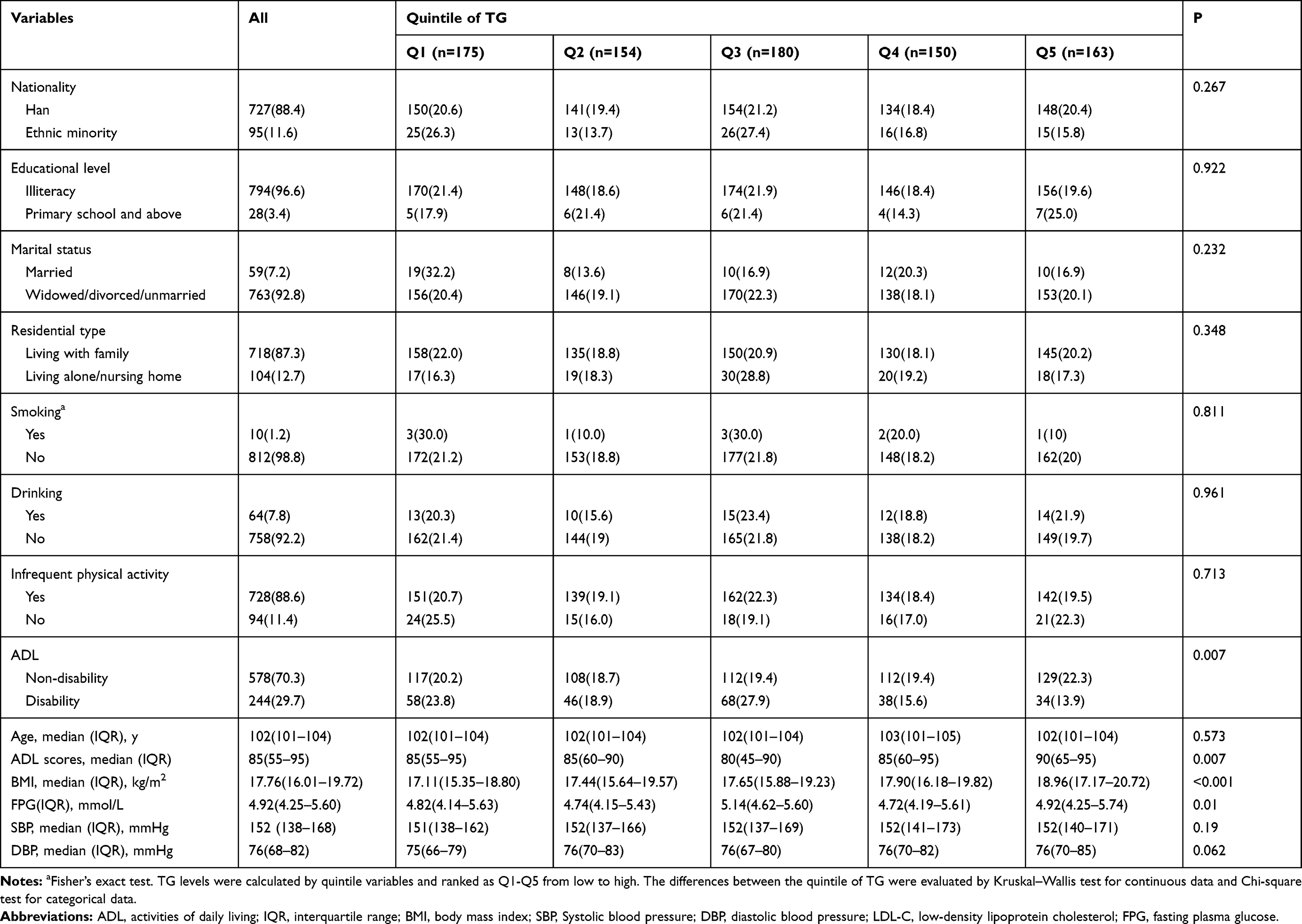 |
Table 2 General Characteristics of Triglyceride Among Hainan Female Centenarians |
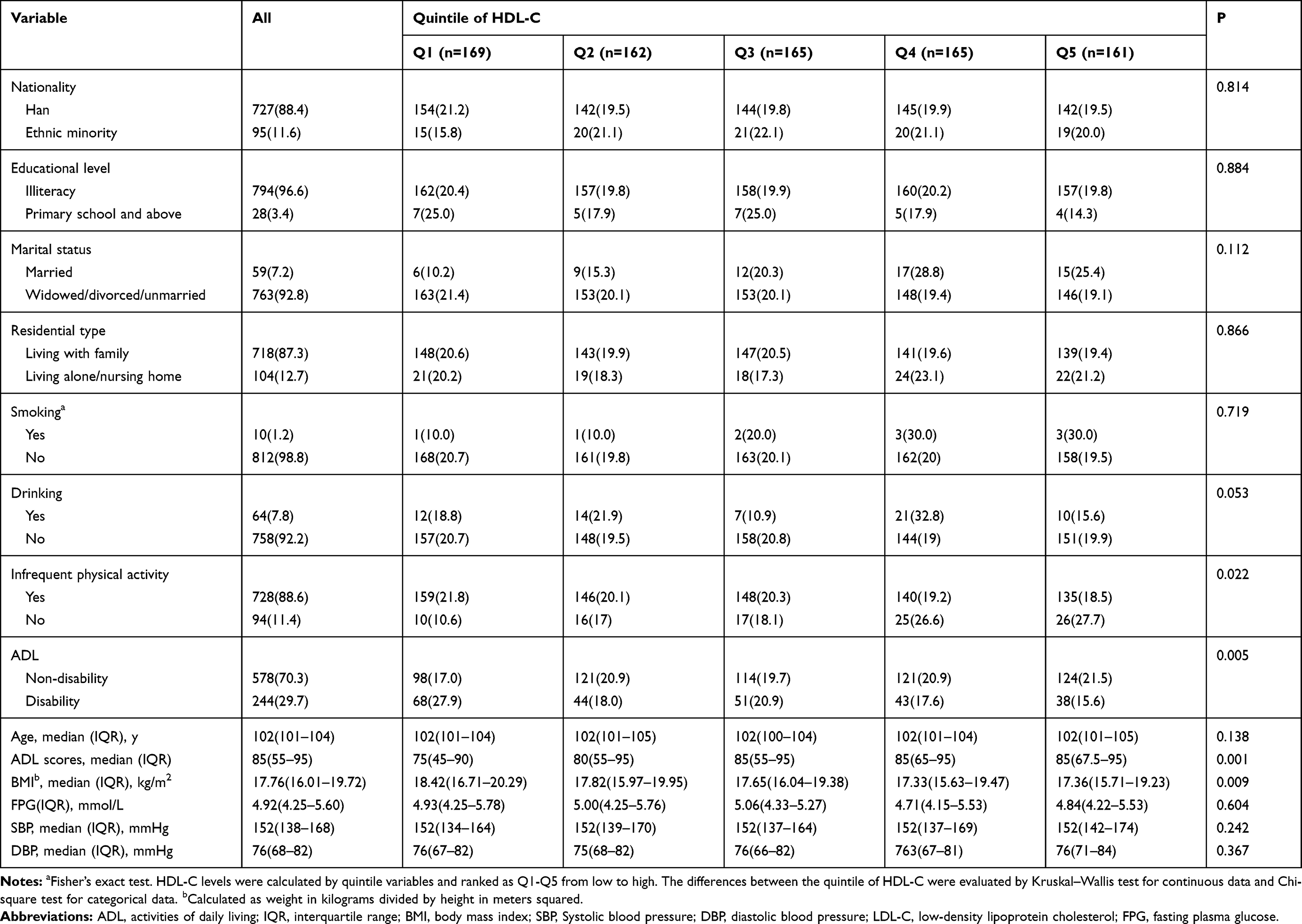 |
Table 3 General Characteristics of High-Density Lipoprotein Cholesterol Among Hainan Female Centenarians |
Figure 1 shows that, with the aggravation of ADL disability, the level of LDL-C, TG, HDL-C appears a significant downward trend in female centenarian. No statistical difference is observed between the distribution of the levels of LDL-C, TG, HDL-C and age in female centenarian.
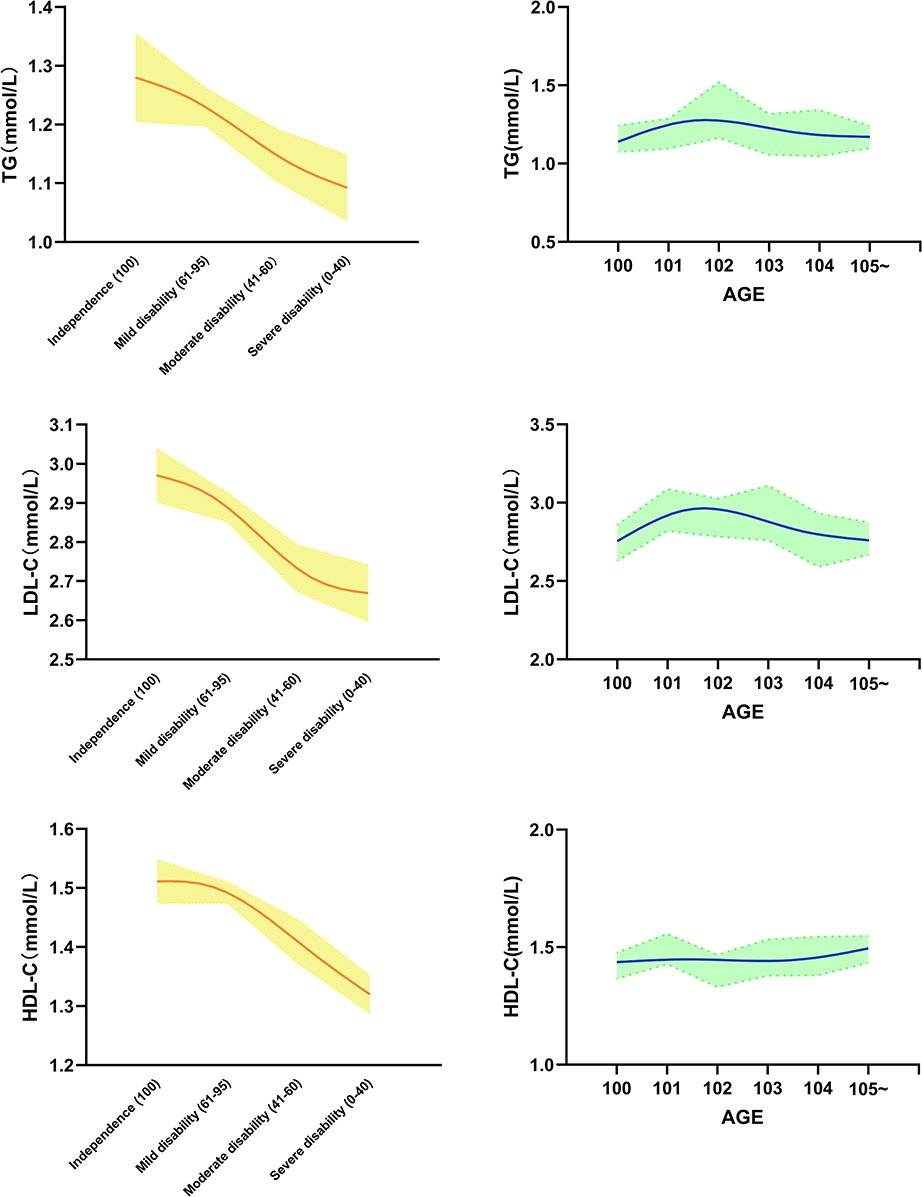 |
Figure 1 With the aggravation of ADL disability, the levels of LDL-C, TG, HDL-C appear to have a significant downward trend in female centenarians. |
The model 3 of Tables 4 and 5 show that, after adjustment, 1 mmol/L increment in LDL-C, TG and HDL-C was associated with 26.4% (aOR=0.736, 95% CI:0.592–0.915), 29.8% (aOR=0.702, 95% CI:0.521–0.948) and 60.5%(aOR=0.395, 95% CI:0.257–0.610) decline in ADL disability of female centenarian, respectively. Sensitivity analysis (Table 5, Table S1) shows that, excluding 112 participants with hyperlipidemia, previous hyperlipidemia, cardiovascular disease, and taking lipid-lowering drugs and cardiovascular disease drugs, 1 mmol/L increment in LDL-C, TG and HDL-C were associated with 31.9% (aOR=0.681, 95% CI: 0.521–0.891), 34.7% (aOR=653, 95% CI: 0.446–0.955) and 55.1% (aOR=0.449, 95% CI: 0.276–0.729) decline in ADL disability of female centenarian, respectively. Among the three lipid profile indicators, elevated HDL-C levels have the strongest protective effect against ADL disability.
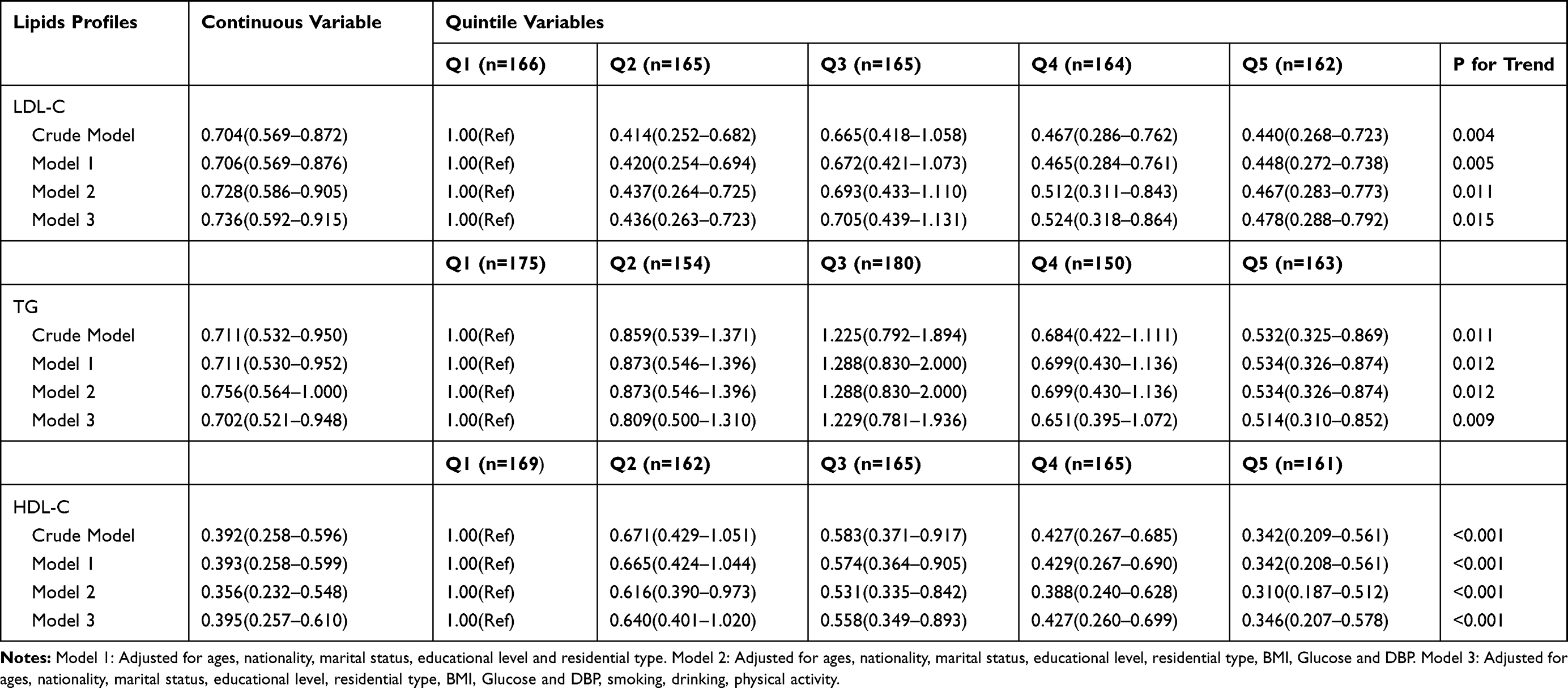 |
Table 4 The Odds Ratios (ORs) for ADL Disability in Different Lipids Profiles Indicators |
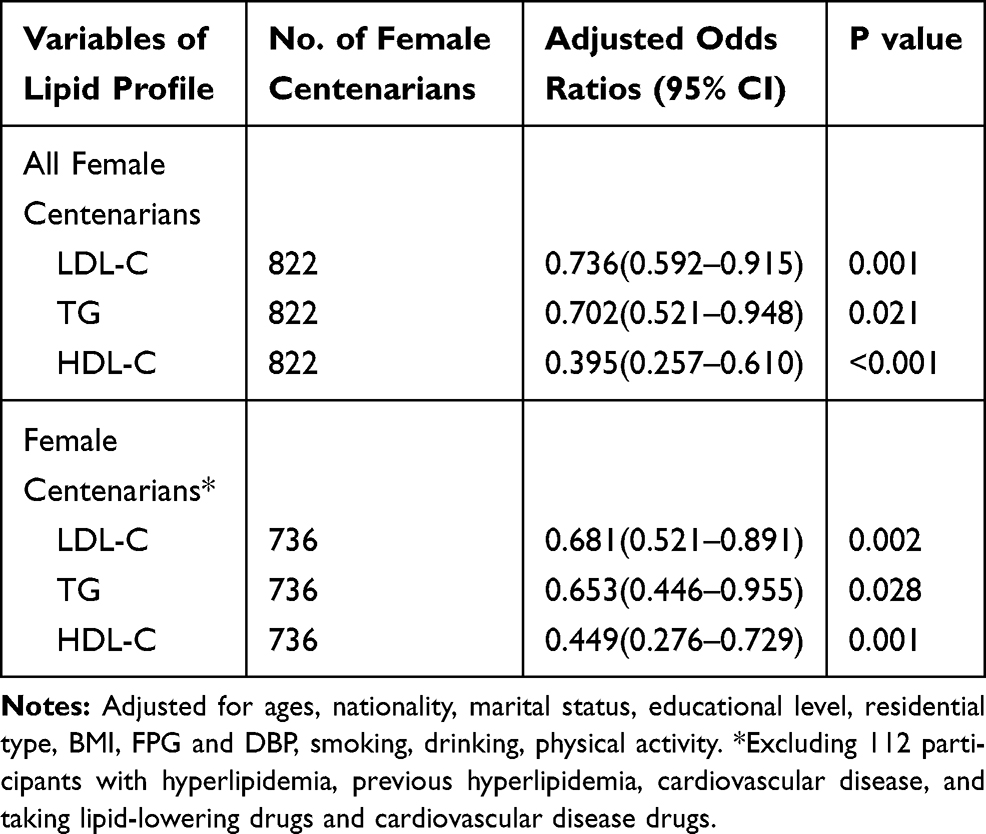 |
Table 5 Association Between LDL-C, TG and HDL-C and ADL Disability in Hainan Female Centenarians |
Table 6 shows the associations between ADL disability and quintile variables of LDL-C, TG and HDL-C in different models. Taking Q1 as a reference, after adjustment of three models, the prevalence of ADL disability is a downward trend with the increase of the quintile of LDL-C (Ptrend<0.005), TG (Ptrend<0.02) and HDL-C (Ptrend<0.001). In three models, the HDL-C of Q5 all have the strongest protective effect against ADL disability, followed by LDL-C and TG.
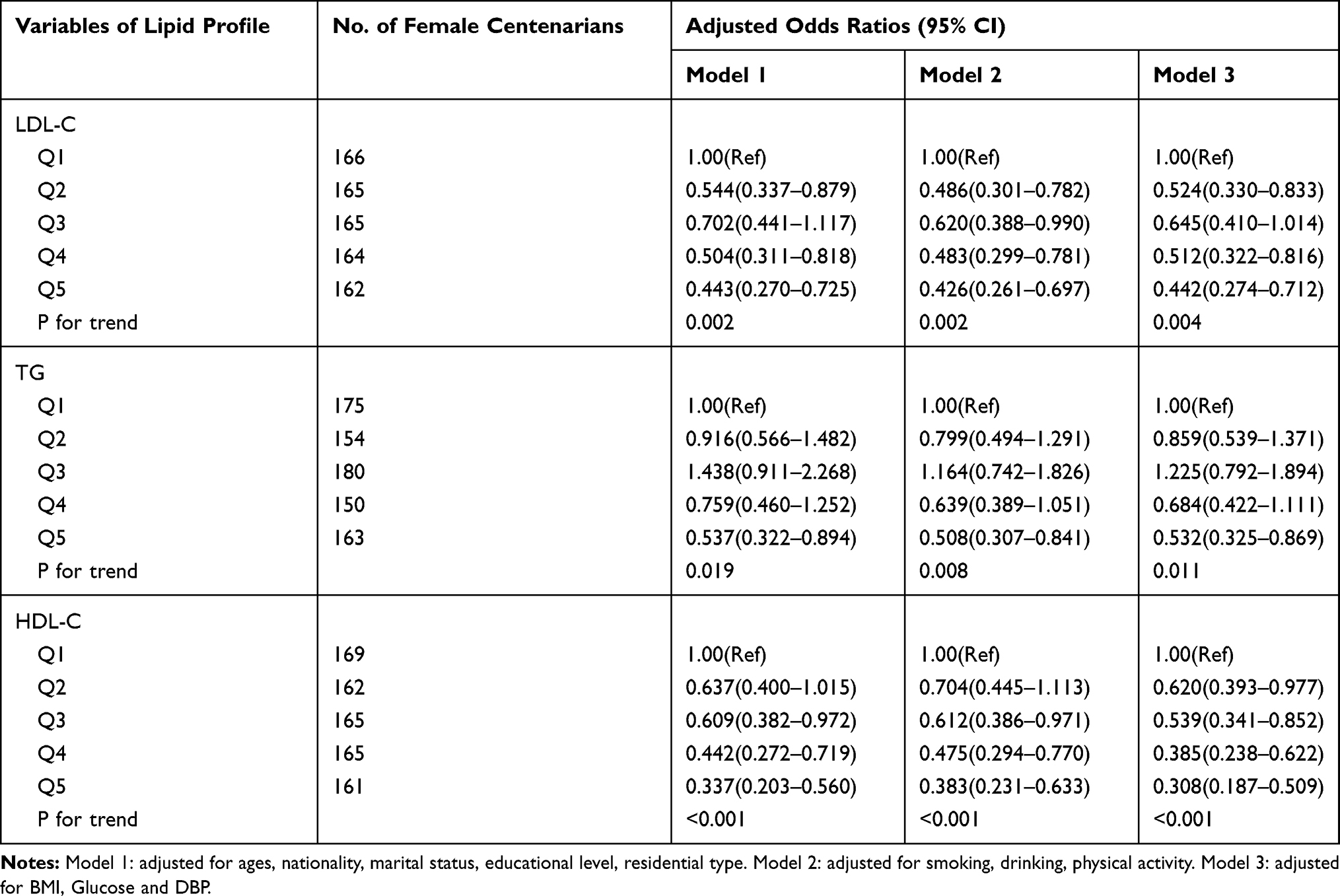 |
Table 6 Association Between LDL-C, TG and HDL-C and ADL Disability in Hainan Female Centenarians in Different Models |
Restrictive cubic splines are used to visualize and analyzed the correlation between ADL disability and LDL-C, TG and HDL-C (Figure 2). After adjustment, the level of LDL-C, TG and HDL-C is inversely associated with ADL Disability and the P of linear test between LDL-C and ADL disability was 0.001, for TG and HDL-C were <0.001. The results of sensitivity analysis (Figure S1), excluding 112 participants with hyperlipidemia, previous hyperlipidemia, cardiovascular disease, and taking lipid-lowering drugs and cardiovascular disease drugs, remain stable.
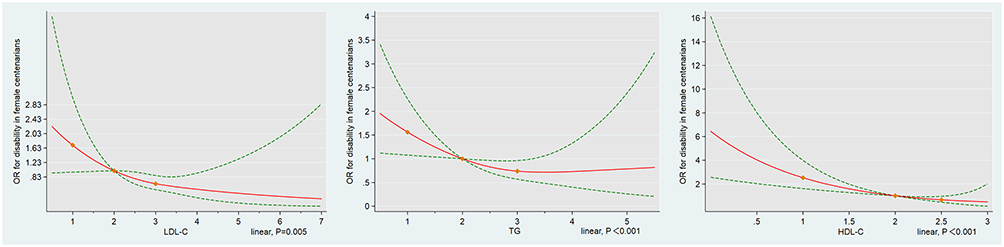 |
Figure 2 Restrictive cubic splines are used to visualize and analyze the correlation between ADL disability and LDL-C, TG and HDL-C levels. |
Discussion
This study, based on the baseline data of the CHCCS database, showed that the increase in LDL-C, TG, and HDL-C levels in Chinese female centenarians had a positive effect on the prevention of ADL disability. To our knowledge, this study firstly evaluated this problem using a full sample of centenarians from the region with the longest longevity. The main advantage of this study is that different statistical models and sensitivity analyses were used to comprehensively control and adjust various potential confounding factors, and similar results proved the robustness of the results. In addition, total cholesterol cannot fully reflect the effect and function of other specific blood lipid indicators. Therefore, the different potential effects of LDL-C, TG, and HDL-C on ADL disability in centenarians were investigated, respectively, in this study.
In the current study, only female centenarians were included as subjects. This is because 822 female and 180 male centenarians were included in the cross-sectional data of the CHCCS and the statistically significant associations between lipids profile indicators and ADL disability only existed in female centenarians. Difference in sample size between male and female centenarians could not explain the inconsistencies of the relationship between lipids profile and ADL disability. Thus, we decided to include only female centenarians subjects to avoid sample bias.
The centenarians in Hainan province were analyzed in our study because Hainan centenarians were regarded as a research template for longevity. The CHCCS was established to explore the health and longevity factors of centenarians. Hainan province, an independent sea island with a good climate, has the highest longevity index in China, and was known as “World Longevity Island”. Most of the centenarians have been indigenous and lived on the island throughout their entire lives, which was considered to have genetic stability.7
In the current study, elevated LDL-C, TG and HDL-C levels have the similar pattern to affect ADL disability, but they have a different pattern to define dyslipidemia, including high TG and LDL-C and low HDL-C. Among the three lipid profile indicators, elevated HDL-C levels have the strongest protective effect against ADL disability. At present, the exact explanation of the above inconsistent patterns is unclear. We think the possible main reason is that the subjects of this study are centenarians. Centenarians may have a delayed onset of lipids-related illness, whereas others may do not suffer from any lipid-related illness.
The prevalence of ADL disability in the CHCCS was 29.7%, which was lower than similar research results. The Chinese Longitudinal Healthy Longevity Survey showed that the prevalence of ADL disability in women over 100 years old was 58.8%.26 The incidence of ADL disability in a French population over 90 years old was 33%.27 A Californian cohort study on elderly aged 90 years and older showed that the average incidence of disability acquired during the annual follow-ups was 16% and the highest incidence was 65% in the baseline data.28 The overall prevalence of ADL disability in Chinese female centenarians is at a low level. One reason may be the use of different ADL assessment scales and differences in the representativeness of the subjects. Another reason may be that Hainan’s unique geographical and climatic environment and relatively stable genetic environment contribute to better physical function of female centenarians in Hainan.
Total cholesterol refers to the sum of cholesterol of various lipoproteins in the blood, which cannot fully represent the physiological functions of specific blood lipid indexes. The physiological functions and health effects of various blood lipid indexes are also inconsistent.8 LDL-C is also called as “bad cholesterol”, and shows higher accuracy than TC in risk assessment and prediction of atherosclerotic diseases. HDL-C can transport cholesterol from extrahepatic tissues to the liver for metabolism, and hence is called “good cholesterol”. TG, also known as fat, can supply energy to the body, regulate physiological functions and dissolve nutrients. Continuing with the topic in this study, the effects of LDL-C, TG and HDL-C on ADL disability were analyzed and compared.
There are few studies analyzing the relationship between blood lipid profile and ADL among the elderly population, but no such study on centenarians has been found. A Japanese cohort study on natural population has confirmed that having high blood lipid level within the normal range in the elderly have a protective effect on ADL disability, and the correlation is more significant in the elderly women.15 Among the hospitalized elderly patients with disability, the increase in blood lipid profile has a positive effect on the recovery rate of ADL disability.16 The results of our study on centenarians are similar to the above results in that the increase in LDL-C, TG, and HDL-C levels has a positive effect on the prevention of ADL disability. Due to the physiological function of HDL-C, HDL-C is regarded as a positive factor of health in the whole population. Relevant research demonstrates that the higher the level of HDL-C, the better the functional status,29 ADL,30 and cognitive function14 of the elderly. This study found that the increase of HDL-C in centenarians had the strongest protective effect on ADL disability, suggesting that the prevention of hypoHDL-C in the elderly and centenarians has important health significance.
The results in this study have partly challenged the traditional cognition of blood lipid, that is, among the centenarians, having a lower level of blood lipid profile does not actually make it more beneficial to health. The potential causes are as follows. Cholesterol has various physiological functions in the human body. When the function of important organs and the body of the elderly decreases, the nervous system may be more dependent on the level of blood lipid. Moreover, the physiological or health effects of blood lipid profile in centenarians may have different mechanisms in different genders, while the level of blood lipid profile in women centenarians is significantly higher than that in men at the same age.
There are several possible mechanisms that attempt to explain the effect of elevated lipid profile levels on the reduction of ADL disability, although the exact mechanism is unknown. 1) cholesterol is involved in the synthesis of vitamin D31 and steroid hormone,32. The physiological function of cholesterol may be more important for the ability of daily life of centenarian. 2) the decrease of lipid profile is related to inflammatory signs, which may affect the Barthel ADL score.33 3) lipid profile has effect on the physiological function of synapse, membrane and amyloid β in brain function.34
Limitations of this study should be noted. First, the baseline data of CHCCS is a cross-sectional survey, which has no causal inference effect. Second, although this study contains a complete sample of female centenarian who almost live in Hainan island environment throughout their lives, conclusion extrapolation to male centenarians or other regions needs to be cautious. Third, the scores of Barthel index in the study are collected in a face-to-face interview format, and there may be information bias among the participants with poor cognitive function.
Conclusions
To our knowledge, this study firstly explored the possible relationship between lipids profile indicators and ADL disability in female centenarian, and found that in female centenarian, higher normal levels of LDL-C, TG and HDL-C might be positive for prevention of ADL disability. The conclusion suggested that for the female oldest-old or centenarian, substantial lipid-lowering should be cautious or avoided.
Acknowledgments
All authors thank CHCCS staff who participated in the field survey and centenarians. This study was financed by Beijing Nova Program (Z181100006218085), Opening Foundation of State Key Laboratory of Kidney Diseases (KF-01-115), Opening Foundation of National Clinical Research Center of Geriatrics (NCRCG-PLAGH-2017017), National Natural Science Foundation of China (81773502, 81703285, 81703308), and Medical Big Data Fund of Chinese PLA General Hospital (2018MBD-029).
Disclosure
The authors declare that they have no competing interests.
References
1. Wu T, Lu L, Luo L, et al. Factors associated with activities of daily life disability among centenarians in rural Chongqing, China: a cross-sectional study. Int J Environ Res Public Health. 2017;14(11):1364. doi:10.3390/ijerph14111364
2. Katz S, Ford AB, Moskovitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. JAMA. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
3. Partridge L, Deelen J, Slagboom PE. Facing up to the global challenges of ageing. Nature. 2018;561(7721):45–56. doi:10.1038/s41586-018-0457-8
4. Herm A, Cheung S, Poulain M. Emergence of oldest old and centenarians: demographic analysis. Asian J Gerontol Geriatrics. 2012;7(1):19–25.
5. Ismail K, Nussbaum L, Sebastiani P, et al. Compression of morbidity is observed across cohorts with exceptional longevity. J Am Geriatr Soc. 2016;64(8):1583–1591. doi:10.1111/jgs.14222
6. Motta M, Bennati E, Ferlito L, Malaguarnera M, Motta L. Successful aging in centenarians: myths and reality. Arch Gerontol Geriat. 2005;40(3):241–251. doi:10.1016/j.archger.2004.09.002
7. He Y, Zhao Y, Yao Y, et al. Cohort profile: the China Hainan Centenarian Cohort Study (CHCCS). Int J Epidemiol. 2018;47:694–695h. doi:10.1093/ije/dyy017
8. Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25Pt B):2889–2934. doi:10.1016/j.jacc.2013.11.002
9. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/s0140-6736(04)17018-9
10. Libby P, Buring JE, Badimon L, et al. Atherosclerosis. Nat Rev Dis Primers. 2019;5(1):56. doi:10.1038/s41572-019-0106-z
11. Ravnskov U, Diamond DM, Hama R, et al. Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open. 2016;6(6):e010401. doi:10.1136/BMJOPEN-2015-010401
12. Lin H, Li Q, Hu Y, et al. The prevalence of multiple non-communicable diseases among middle-aged and elderly people: the Shanghai Changfeng Study. Eur J Epidemiol. 2017;32(2):159–163. doi:10.1007/s10654-016-0219-6
13. Yin ZX, Shi XM, Kraus VB, et al. High normal plasma triglycerides are associated with preserved cognitive function in Chinese oldest-old. Age Ageing. 2012;41(5):600–606. doi:10.1093/ageing/afs033
14. Lv YB, Yin ZX, Chei CL, et al. Serum cholesterol levels within the high normal range are associated with better cognitive performance among Chinese elderly. J Nutr Health Aging. 2016;20(3):1–8. doi:10.1007/s12603-016-0701-6
15. Tomonori O, Takehito H, Atsushi H, et al. Lower levels of serum albumin and total cholesterol associated with decline in activities of daily living and excess mortality in a 12-year cohort study of elderly Japanese. J Am Geriatr Soc. 2010;56(3):529–535. doi:10.1111/j.1532-5415.2007.01549.x
16. Onder G, Volpato S, Liperoti R, et al. Total serum cholesterol and recovery from disability among hospitalized older adults. J Gerontol a Biol Sci Med Sci. 2006;61(7):736–742. doi:10.1093/gerona/61.7.736
17. Sun L, Clarke R, Bennett D, et al. Causal associations of blood lipids with risk of ischemic stroke and intracerebral hemorrhage in Chinese adults. Nat Med. 2019;25(4):569–574. doi:10.1038/s41591-019-0366-x
18. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA
19. Xi B, Liang Y, He T, et al. Secular trends in the prevalence of general and abdominal obesity among Chinese adults, 1993–2009. Obes Rev. 2012;13(3):287–296. doi:10.1111/j.1467-789X.2011.00944.x
20. Thun MJ, Peto R, Lopez AD, et al. Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med. 1997;337(24):1705–1714. doi:10.1056/NEJM199712113372401
21. He XZ, Baker DW. Body mass index, physical activity, and the risk of decline in overall health and physical functioning in late middle age. Am J Public Health. 2004;94(9):1567. doi:10.2105/AJPH.94.9.1567
22. Brown RT, Diaz-Ramirez LG, Boscardin WJ, Lee SJ, Williams BA, Steinman MA. Association of functional impairment in middle age with hospitalization, nursing home admission, and death. JAMA Intern Med. 2019;179(5):668–675. doi:10.1001/jamainternmed.2019.0008
23. Mahoney FI, Barthel DW. functional evaluation: the Barthel index. Md State Med J. 1965;14(14):61–65.
24. Wade DT, Collin C. The Barthel ADL Index: a standard measure of physical disability. Int Disabil Stud. 1988;10(2):64–67. doi:10.3109/09638288809164105
25. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. doi:10.1016/0895-4356(89)90065-6
26. Yin Z, Shi X, Kraus VB, et al. Gender-dependent association of body mass index and waist circumference with disability in the Chinese oldest old. Obesity(Silver Spring). 2014;22(8):1918–1925. doi:10.1002/oby.20775
27. Herr M, Arvieu JJ, Robine JM, Ankri J. Health, frailty and disability after ninety: results of an observational study in France. Arch Gerontol Geriat. 2016;66:166–175. doi:10.1016/j.archger.2016.06.002
28. Berlau DJ, Corrada MM, Peltz CB, Kawas CH. Disability in the oldest-old: incidence and risk factors in the 90+ study. Am J Geriat Psychiat. 2012;20(2):159–168. doi:10.1097/JGP.0b013e31820d9295
29. Choi H, Kim HC, Stefani KM, et al. Serum high-density lipoprotein cholesterol concentration and functional state: the Korean Urban Rural Elderly (KURE) study. Arch Gerontol Geriatr. 2017;71:115–121. doi:10.1016/j.archger.2017.04.002
30. Chanti-Ketterl M, Gamaldo A, Andel R, Thorpe RJ
31. Jorde R, Grimnes G. Vitamin D and metabolic health with special reference to the effect of vitamin D on serum lipids. Prog Lipid Res. 2011;50(4):303–312. doi:10.1016/j.plipres.2011.05.001
32. Eliassen AH, Hankinson SE. Endogenous hormone levels and risk of breast, endometrial and ovarian cancers: prospective studies. Adv Exp Med Biol. 2008;630:148–165. doi:10.1007/978-0-387-78818-0_10
33. Cesari M, Penninx BW, Pahor M, et al. Inflammatory markers and physical performance in older persons: the InCHIANTI study. J Gerontol a Biol Sci Med Sci. 2004;59(3):242–248. doi:10.1093/gerona/59.3.m242
34. van Vliet P. Cholesterol and late-life cognitive decline. J Alzheimers Dis. 2012;30(Suppl 2):S147–S162. doi:10.3233/jad-2011-111028
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.