")
Back to Journals » Clinical Interventions in Aging » Volume 13
High-speed jaw-opening exercise in training suprahyoid fast-twitch muscle fibers
Authors Matsubara M, Tohara H , Hara K , Shinozaki H, Yamazaki Y, Susa C, Nakane A, Wakasugi Y, Minakuchi S
Received 28 September 2017
Accepted for publication 23 November 2017
Published 22 January 2018 Volume 2018:13 Pages 125—131
DOI https://doi.org/10.2147/CIA.S152821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker

Mariko Matsubara,1,2 Haruka Tohara,1 Koji Hara,1 Hiromichi Shinozaki,1 Yasuhiro Yamazaki,1 Chiaki Susa,1 Ayako Nakane,1 Yoko Wakasugi,1 Shunsuke Minakuchi1
1Gerodontology and Oral Rehabilitation, Department of Gerontology and Gerodontology, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, 2Department of Oral Surgery, Ichigao Carillon Hospital, Kanagawa, Japan
Purpose: This study was aimed to examine the effectiveness of a high-speed jaw-opening exercise, which targets the contraction of fast-twitch muscle fibers, in improving swallowing function.
Subjects and methods: Twenty-one subjects (mean age 74.0±5.7 years) with dysphagia-related symptoms, such as coughing or choking during eating, performed the exercise. None of the included subjects had neurological symptoms or history of surgery that could cause significant dysphagia. All subjects took regular meals, and maintained independent activities of daily life. The exercise schedule consisted of 3 sets of 20 repetitions each of rapid and maximum jaw-opening movement with a 10-second interval between sets. The exercise was performed twice daily for 4 weeks.
Results: Following the intervention, there was a significant increase in the vertical position of the hyoid bone at rest. Furthermore, during swallowing, the elevation of the hyoid bone and the velocity of its movement and esophageal sphincter opening increased significantly while the duration of the hyoid elevation and the pharyngeal transit time reduced significantly.
Conclusions: Our results demonstrated that high-speed jaw-opening exercise resulted in increased elevation velocity of the hyoid bone during swallowing, indicating its role in effectively strengthening the fast-twitch muscle fibers of suprahyoid muscles. Furthermore, since the rest position of the hyoid bone appeared to have improved, this exercise may be especially useful in elderly individuals with a lower position of the hyoid bone at rest and those with decreased elevation of the hyoid bone during swallowing, which are known to be associated with an increased risk of aspiration.
Keywords: deglutition disorders, jaw, exercise, rehabilitation, fast-twitch muscle fibers, high speed
Introduction
Suprahyoid muscle training is important for managing dysphagia, and it primarily aims at improving the insufficient upper esophageal sphincter (UES) opening during swallowing. Among the invasive1–5 and noninvasive treatments6–11 available, the Shaker exercise is one of the most popular exercises.9 This exercise is noninvasive and aims to strengthen the muscles that elevate the hyoid bone and larynx. In this method, first, the subject lifts the head off the ground in the supine position for 1 minute, as an isometric exercise. This is repeated thrice with a 1-minute interval between the sets. Subsequently, head-raising is repeated 30 times (1 set) in the supine position as an isotonic exercise. Subjects perform three sets per day. It was observed that performing this exercise for 6 weeks continuously resulted in an increase in the anterior–posterior diameter and the cross-sectional area of the UES during swallowing. However, a recent study demonstrated that the required training load was not imposed on the suprahyoid muscles, which are the target of the exercise, unless the Shaker exercise caused fatigue in the sternocleidomastoid muscles.12
Since the suprahyoid muscles work to reinforce jaw opening, we focused on developing a jaw-opening exercise to improve the suprahyoid muscle strength.11 This training involved isometric exercise, wherein the subject opened the jaw to its maximum and maintained this position for 10 seconds. Each exercise set consisted of five repetitions with a 10-second interval between the sets. A total of two sets were performed daily for 4 weeks. Our results demonstrated that this training resulted in elevating the hyoid bone, elevating the UES, improving its opening, and decreasing the pharyngeal transit time. This study demonstrated that the isometric jaw-opening exercise was effective in training the suprahyoid muscles.
The fast-twitch muscle fibers (FTMFs) are selectively reduced in age-related muscle atrophy.12 The FTMFs constitute more than half of the muscle fibers of the suprahyoid muscles.13 These fibers are influenced by sarcopenia,14 leading to a reduction in the velocity of hyoid bone elevation during the deglutition reflex.15 So, conventional isometric exercise with maximal jaw opening is not adequate to specifically train the FTMFs. Therefore, we examined the possibility and extent of improvement in swallowing function with high-speed jaw-opening exercise targeting the contraction of FTMFs.
Subjects and method
Subjects
The subjects were community-dwelling elderly individuals (11 females and 10 males) who visited the Ichigao Carillon Hospital for symptoms suggestive of swallowing disorders such as coughing or choking during eating. The mean participant age was 74.0±5.7 years. One male subject had a history of ischemic stroke sustained for 17 years prior to the study but had no obvious disabilities including dysphagia. The other subjects had cardiovascular disease (one subject), hypertension (four subjects), and diabetes mellitus (one subject). Some participants took medicine, such as antihypertensive or antidiabetic. None took medicine that is possible to affect swallowing function. None of the included subjects had neurological symptoms or history of surgery that could cause significant dysphagia. All subjects took regular meals, and maintained independent activity of daily living. Furthermore, none of the subjects in our study had dementia or history of temporomandibular arthrosis.
This study was approved by the ethics committee of the Dentistry department of Tokyo Medical and Dental University (approval number: 1143), and written informed consent was obtained from all subjects including publication of images in this study.
Method
High-speed jaw-opening exercise
The high-speed jaw-opening exercise was performed as follows. A metronome was set to 30 beats per minute, and the subject opened the jaw once every 2 seconds (Figure 1). The person in Figure 1 has provided written informed consent for the images to be published.
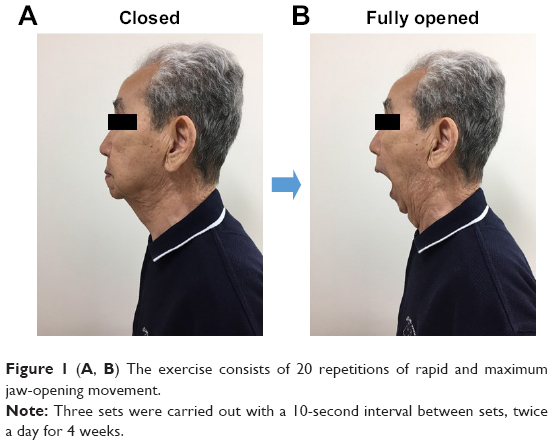 | Figure 1 (A, B) The exercise consists of 20 repetitions of rapid and maximum jaw-opening movement. |
The subjects opened the jaw maximally as fast as possible and repeated the movement for 20 times (1 set). Three sets were performed with a 10-second interval in between. The exercise was performed twice daily for 4 weeks. Furthermore, subjects were instructed to feel the strong tension in their suprahyoid muscles during jaw opening and were instructed to stop the exercise if they felt any abnormality in their temporomandibular joints. The subjects recorded their training history and submitted it at the end of the 4-week training program.
Videofluoroscopic measurement
Videofluoroscopic examination of swallowing was performed at baseline and following the completion of the 4-week training program to analyze the effect of training. The Camper plane was used as the reference plane for analysis.16
Since the Camper plane is a straight line passing through the upper tragal edge and the lower alar edge, 6-mm disc-shaped leads were fixed at these points. The X-axis was defined as the Camper plane, and the Y-axis was a line perpendicular to the Camper plane passing through the tragus (Figure 2).
 | Figure 2 Lateral radiogram demonstrating the X- and the Y-axis. |
A 14.3-mm metal ball was placed on the neck to standardize the radiographic image magnification at every instance. Subjects remained seated during the examination and swallowed 5 mL of nectar barium (40% w/v) twice. Radiographic scanning (Shimadzu Medical Systems Corp, Osaka, Japan) was performed at 30 fps from the lateral aspect of the neck, and the images were recorded on a digital video recorder (DV-AC82; Sharp Corporation, Osaka, Japan). The videos were subsequently analyzed on a computer by using the Adobe premiere CS4 software (Adobe Systems Incorporated, San Jose, CA, USA).
The difference between the positions of the hyoid bone on the Y-axis at rest (YR) and at its maximum anterior position (YH) was defined as the elevation of the hyoid bone (YR – YH). The difference between the position of the hyoid bone on the X-axis at rest (XR) and its maximum anterior position (XH) was defined as the forward displacement of the hyoid bone (XH – XR). The measurement point of the hyoid bone was set at the upper edge of the hyoid bone body for measuring its displacement following the training program.
The UES opening was measured when the esophagus was maximally opened during the barium swallow, by identifying the minimum anterior–posterior distance in the segment between C3 and C617,18 (Figure 3).
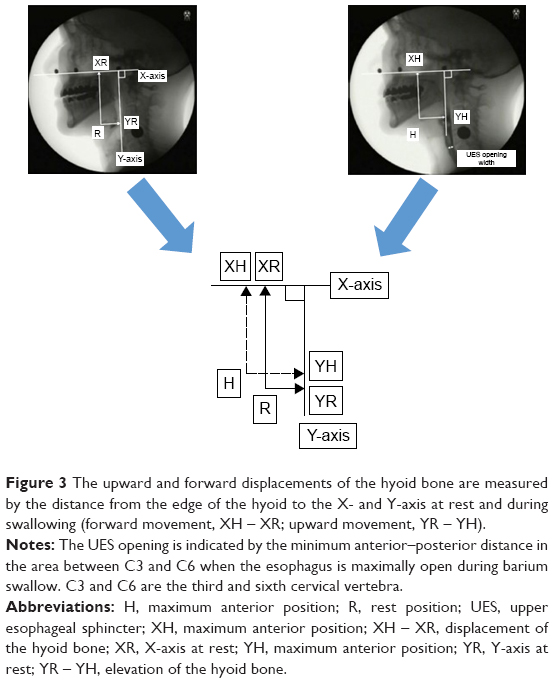 | Figure 3 The upward and forward displacements of the hyoid bone are measured by the distance from the edge of the hyoid to the X- and Y-axis at rest and during swallowing (forward movement, XH – XR; upward movement, YR – YH). |
We calculated the time from the onset of hyoid bone elevation (A) to its conclusion (B) as the duration of hyoid bone elevation during the barium swallow (B – A).
For determining the elevation velocity, we first calculated the displacement of the hyoid bone on the X-axis (FM) and Y-axis (UM) during swallowing, and defined them as elevation movements. The velocity was calculated by dividing the elevation movement by the elevation duration (Table 2). The pharyngeal transit time was measured as the time taken from the first edge of food bolus reaching the mandibular ramus to the tail part of the food bolus passing the UES. We also evaluated the presence or absence of aspiration and food residue before and after the training program. The absence and presence of laryngeal penetration were scored as 0 and 1, respectively, and aspiration was rated as 2. The absence and presence of food residue in the vallecula or pyriform sinus were rated as 0 and 1, respectively.
All assessments were performed by a dentist who was blinded to all patient-related data.
Statistical analyses
We used SPSS Statistics 20.0J (IBM Japan Ltd, Tokyo, Japan) for all statistical analyses. The Wilcoxon signed-rank test was used to examine the pre–post differences of the hyoid bone position at rest, its elevation and forward displacement, pharyngeal transit time, the duration of hyoid bone elevation, the size of the UES, and the elevation velocity of the hyoid bone during swallowing. We calculated a sample size by using G*power (G*Power 3.1 software; Kiel University, Kiel, Germany). In this study, regarding an appropriate effect, we could not refer a previous study because this is a newly developed training. Therefore, the value of effect size was set as a medium level. The effect size of the difference was examined by using the Cohen’s d. As a result, we determined at least 21 subjects with a power of 0.8, alpha of 0.05, and effect size of 0.6.
Results
All 21 subjects were able to complete two sets of exercise per day, and none of them complained of temporomandibular joint pain during the 4-week training period.
Following the training program, the rest position of the hyoid bone YR, elevation of the hyoid bone during swallowing, and size of the UES increased significantly (Table 1). Further, there was a significant increase in the elevation velocity of the hyoid bone, decrease in the duration of the hyoid bone elevation, and reduction in the pharyngeal transit time (P<0.05) (Table 2). We did not find any significant improvement in the forward displacement of the hyoid bone during swallowing.
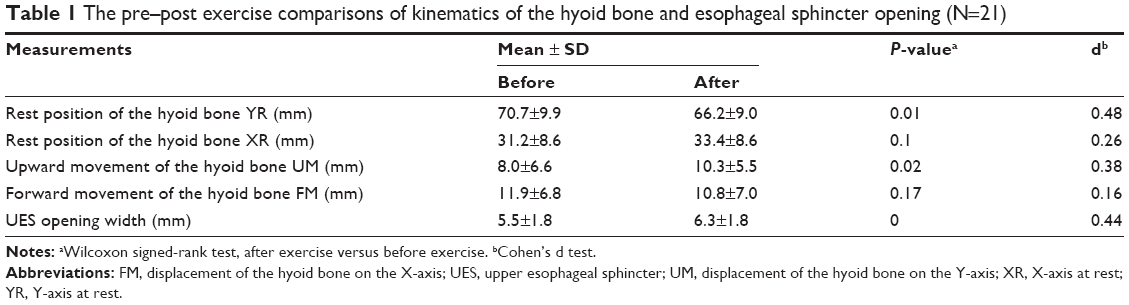 | Table 1 The pre–post exercise comparisons of kinematics of the hyoid bone and esophageal sphincter opening (N=21) |
 | Table 2 The pre–post exercise comparisons of the duration and velocity of hyoid elevation and pharyngeal transition time (N=21) |
None of the subjects reported aspiration during swallowing, or food residue in the pharynx, either before or after the training. One subject had laryngeal penetration prior to the exercise training, which persisted even after the completion of the training.
Discussion
Validity of the exercise
The number of repetitions of the high-speed jaw-opening exercise was determined based on our previous studies.19 We measured the activity of the hyoid muscles by using surface electrode while 12 healthy subjects performed maximum jaw opening once every 2 seconds for 90 repetitions. The electrodes was taped to the skin under the chin on both sides of the midline which detects the electromyography (EMG) of suprahyoid muscle activity.20 We analyzed the mean power frequency (MPF), which decreases with muscle fatigue,21–25 and found that there was a reduction in the MPFs (on EMG measurements) under the genitals as well as under the hyoid bone, on an average, following the 20th repetition. Based on this finding, we defined one set (unit) of exercise as comprising 20 repetitions. Although this may not be an optimal number, our results demonstrated that the high-speed jaw-opening exercise with 20-repetition sets was effective in improving our outcome measures. Furthermore, since none of the patients complained of temporomandibular joint symptoms or dropped out of the training program, the training program may be considered as being safe and convenient.
Effect of exercise on the hyoid bone position at rest and during swallowing
It is known that, in the elderly, the hyoid bone and larynx are lower in the vertical axis owing to age-related atrophy of the suprahyoid muscle fibers and reduced tension and increased laxity of the ligaments.26 In our previous study, we confirmed that a decline in the force of jaw opening was an indicator of reduced suprahyoid muscle strength, which also resulted in the lower position of the hyoid bone in the neck.27
The higher position of the hyoid (Y) at rest following the intermittent jaw-opening exercise indicated that the exercise may have contributed to muscle hypertrophy and improved muscle tone, especially of the mylohyoid muscle. It is important to determine whether the exercise has an effect on muscle volume and quality, and the extent to which it influences the same.
The upward displacement of the hyoid bone on swallowing was significantly greater in the post-intervention period compared with the pre-intervention status. However, the increase in the forward displacement after intervention was not found. Although the reason for this disparity is unclear, it may be related to the mandibular movement and its suprahyoid attachments, when performing the jaw-opening action.
The mylohyoid muscle runs horizontally along the mylohyoid line on the mandible while the geniohyoid muscle is attached to the mental spine. These muscles influence the direction of the mandibular movement during jaw opening. In the early phase of jaw opening, the downward movement of the jaw is along the vertical axis, which is similar to the direction of contraction of the mylohyoid muscle. On the other hand, the direction of the contraction of the geniohyoid muscle indicates that it pulls the mandible backward, rather than downward. Thus, the jaw-opening exercise may be more effective in activating the mylohyoid muscle rather than the geniohyoid muscle. Our finding that the hyoid bone was at a higher position at rest as well as on swallowing indicates the effectiveness of the jaw-opening exercise in elevating the hyoid bone. Our previous finding that the isometric jaw-opening exercise significantly improved the elevation of the hyoid bone during swallowing without any change in its forward movement11 may be explained by the same reasons.
Therefore, this exercise may be especially useful in elderly individuals with a lower position of the hyoid bone at rest28 and those with decreased elevation of the hyoid bone during swallowing.29,30 It is known that both these factors are associated with an increased risk of aspiration.
Effect of exercise on the elevation velocity of the hyoid bone during swallowing
Previous studies have demonstrated that there is a gradual decline in muscle strength, which starts at around the age of 30 and accelerates at around 50. In the period between 30 and 80 years, there is approximately a 30%–50% reduction in muscle strength. This reduction is contributed by the alteration in the composition of the muscle fibers to slow-twitch fibers, as well as a reduction in muscle volume. In elderly people, significant muscle atrophy selectively occurs in the FTMFs,12 while the slow-twitch muscle fibers are relatively spared.31
Cervical muscles are among the muscles that are significantly influenced by age-related atrophy.32 The suprahyoid muscle, wherein FTMFs comprise more than half of the muscle fibers,13 is significantly affected by sarcopenia.14 The consequence of this age-related change on the swallowing function is large since this results in a reduction in the elevation velocity of the hyoid bone during the deglutition reflex.15 Furthermore, the velocity of muscle contraction also decreases secondary to aging. Several studies have reported that hyoid velocity was decreased in patients with dysphagia.33–37 The Shaker’s exercise8 and the jaw-opening exercise are recommended to improve the elevation of the hyoid bone during swallowing. Previous studies have also made use of electrical stimulations38 and the MDTP (McNeill dysphagia therapy program)39 for improving the elevation velocity of the hyoid bone. The application of electrical stimulation may be limited since it is a complex process and requires stimulation devices. The MDTP also has its limitations, as it is applicable only in subjects who can swallow food; the program is not appropriate for patients who have difficulties in swallowing. The jaw-opening exercise does not require any specific training, location, or instruments. Further, it can be performed safely and easily without the risk of aspiration even in patients who have difficulties in swallowing.
To summarize, our study demonstrated that intermittent training of the suprahyoid muscle resulted in increased elevation velocity of the hyoid bone during swallowing, indicating its role in effectively strengthening the FTMFs.
Clinical implication
The high-speed jaw-opening exercise was effective in improving the rest position and kinematics of the hyoid bone. This exercise may be effective especially in elders with a higher risk of aspiration owing to a lower position of the hyoid bone at rest28 and during swallowing.29,30 Furthermore, this exercise may also be beneficial to patients with stroke or those with tracheotomy, who have decreased elevation velocity of the hyoid bone during swallowing.15,40
It is known that among the various motor elements, equilibrium, flexibility, and agility undergo marked decline with advanced age.41 High-speed muscle training may effectively improve agility. Decreased muscle strength42 and volume, and fat infiltration43 are the main age-related changes observed in the suprahyoid muscles. There is a need for further studies to analyze the association between the factors of muscle strength and volume, fat infiltration, the outcomes of elevation velocity, the position at rest, and the swallowing of the hyoid bone during the deglutition reflex.
Limitations
Our study has a few limitations. First, we included only those patients who had mild or no dysphagia and not those with severe dysphagia. Second, we were unable to distinguish the clinical indications for the isometric jaw-opening exercise that was performed in our previous study from those for the high-speed jaw-opening exercise performed in this study. Further study that compares high-speed jaw-opening exercise and original jaw-opening exercise should be addressed. Third, although the high-speed jaw-opening exercise targeted FTMFs, our confirmation of this was achieved only by indirect evaluation of muscle velocity on videofluoroscopic examination of swallowing. Future studies may include other methods of measurement of muscle strength, including computed tomography or ultrasonography, to evaluate the effects of training on muscle volume and quality. The present study did not directly examine the effect of the jaw-opening exercise on type II fibers. However, a previous study confirmed the role of high-speed muscle strengthening exercise in effectively improving the skeletal peak muscle power in the lower limb.44
Conclusions
High-speed jaw-opening exercise resulted in a significant increase in the vertical resting position of the hyoid bone and its elevation during swallowing, elevation velocity, and esophageal sphincter opening, and a significant decrease in the duration of the hyoid bone elevation and the pharyngeal transit time. Our results suggest that the high-speed jaw-opening exercise may be effective in increasing the strength of the FTMFs of the suprahyoid muscles.
Disclosure
The authors report no conflicts of interest in this work.
References
Kaplan S. Paralysis of deglutition, a post-poliomyelitis complication treated by section of the cricopharyngeus muscle. Ann Surg. 1951;33(4):572–573. | ||
Buchholz DW. Cricopharyngeal myotomy may be effective treatment for selected patients with neurogenic oropharyngeal dysphagia. Dysphagia. 1995;10(4):255–258. | ||
Lacau St Guily J, Zhang KX, Perie S, Copin H, Butler-Browne GS, Barbet JP. Improvement of dysphagia following cricopharyngeal myotomy in a group of elderly patients. Histochemical and biochemical assessment of the cricopharyngeal muscle. Ann Otol Rhinol Laryngol. 1995;104(8):603–609. | ||
Schneider I, Thumfart WF, Pototoschnig C, Eckel HE. Treatment of dysfunction of the cricopharyngeal muscle with botulinum A toxin: introduction of a new, noninvasive method. Ann Otol Rhinol Laryngol. 1994;103(1):31–35. | ||
Shaw GY, Searl JP. Botulinum toxin treatment for cricopharyngeal dysfunction. Dysphagia. 2001;16(3):161–167. | ||
Kahrilas PJ, Logemann JA, Gibbons P. Food intake by maneuver: an extreme compensation for impaired swallowing. Dysphagia. 1992;7(3):155–159. | ||
Logemann JA, Kahrilas PJ. Relearning to swallow after stroke – application of maneuvers and indirect biofeedback: a case study. Neurology. 1990;40(7):1136–1138. | ||
Kahrilas PJ, Logemann JA, Kruger C, Flanagan E. Volitional augmentation of upper esophageal sphincter opening during swallowing. Am J Physiol. 1991;260(3 Pt 1):G450–G456. | ||
Shaker R, Kern M, Bardan E, et al. Augmentation of deglutitive upper esophageal entrance opening in the elderly by exercise. Am J Physiol. 1997;272(6 Pt 1):G1518–G1522. | ||
Ferdjallah M, Wertsch JJ, Shaker R. Spectral analysis of surface electromyography (EMG) of upper esophageal sphincter-opening muscles during head lift exercise. J Rehabil Res Dev. 2000;37(3):335–340. | ||
Wada S, Tohara H, Iida T, Inoue M, Sato M, Ueda K. Jaw-opening exercise for insufficient opening of upper esophageal sphincter. Arch Phys Med Rehabil. 2012;93(11):1995–1999. | ||
Larsson L, Yu F, Höök P, Ramamurthy B, Marx JO, Pircher P. Effects of aging on regulation of muscle contraction at the motor unit, muscle cell, and molecular levels. Int J Sport Nutr Exerc Metab. 2001;11(Suppl):S28–S43. | ||
Korfage JA, Schueler YT, Brugman P, Van Eijden TM. Differences in myosin heavy-chain composition between human jaw-closing muscles and supra- and infrahyoid muscles. Arch Oral Biol. 2001;46(9):821–827. | ||
Feng X, Todd T, Hu Y, et al. Age-related changes of hyoid bone position in healthy older adults with aspiration. Laryngoscope. 2014;124(6):E231–E236. | ||
Seo HG, Oh BM, Han TR. Swallowing kinematics and factors associated with laryngeal penetration and aspiration in stroke survivors with dysphagia. Dysphagia. 2016;31(2):160–168. | ||
Nakane A, Tohara H, Ouchi Y, Goto S, Uematsu H. Videofluoroscopic kinesiologic analysis of swallowing: defining a standard plane. J Med Dent Sci. 2006;53(1):7–15. | ||
Jacob P, Kahrilas PJ, Logemann JA, Shah V, Ha T. Upper esophageal sphincter opening and modulation during swallowing. Gastroenterology. 1989;97(6):1469–1478. | ||
Kendall KA, Leonald RJ. Videofluoroscopic upper esophageal sphincter function in elderly dysphagic patients. Laryngoscope. 2002;112(2):332–337. | ||
Mariko M, Haruka H, Mai O, Shunsuke M. Fatigue During Jaw-opening exercise. Poster presented at: The 20th Annual Meeting of the Japanese Society of Dysphagia Rehabilitation; September 2014; Tokyo, Japan. | ||
Reimers-Neils L, Logemann J, Larson C. Viscosity effects on EMG activity in normal swallow. Dysphagia. 1994;9(2):101–106. | ||
Oberg T. Muscle fatigue and calibration of EMG measurements. J Electromyogr Kinesiol. 1995;5(4):239–243. | ||
Signorile JF, Digel S, Moccia G, Applegate B, Perry A. Effects of partial occlusion of circulation on frequency and amplitude of surface electromyography. J Electromyogr Kinesiol. 1991;1(2):124–129. | ||
Gerdle B, Elert J. The temporal occurrence of the mean power frequency shift of the electromyogram during maximum prolonged dynamic and static working cycles. Int J Sports Med. 1994;15(Suppl 1):S32–S37. | ||
Shi CS, Ouyang G, Guo TW. Frequency analysis of electromyographic signals in mandibular elevators at maximum clench level. J Oral Rehabil. 1992;19(4):427–433. | ||
Moritani T, Muro M, Nagata A. Intramuscular and surface electromyogram changes during muscle fatigue. J Appl Physiol (1985). 1986;60(4):1179–1185. | ||
Kaneko I. [A cinefluorographic study of hyoid bone movement during deglutition]. Nippon Jibiinkoka Gakkai Kaiho. 1992;95(7):974–987. Japanese. | ||
Shinozaki H, Tohara H, Matsubara M, et al. The relationship between jaw opening force and hyoid bone dynamics in healthy elderly subjects. Clin Interv Aging. 2017;12:629–634. | ||
Furukawa K. [Cine radiographic analysis of laryngeal movement during deglutition]. Nippon Jibiinkoka Gakkai Kaiho. 1984;87(2):169–181. Japanese. | ||
Logemann JA, Pauloski BR, Rademaker AW, Kharilas PJ. Oropharyngeal swallow in younger and older women: videofluoroscopic analysis. J Speech Lang Hear Res. 2002;45(3):434–445. | ||
Logemann JA, Pauloski BR, Rademaker AW, Colangelo LA, Kahrilas PJ, Smith CH. Temporal and biomechanical characteristics of oropharyngeal swallow in younger and older men. J Speech Lang Hear Res. 2000;43(5):1264–1274. | ||
Shinya K, Haruka M, Shino B, Jun Dong K, Masashi K. [Effect of strength training on aging muscles of elderly people]. Jpn J Phys Fitness Sports Med. 2003:52(Suppl):S17–S30. Japanese. | ||
Ishii N, Shimada Y, Suzuki T. The Relationship Between Exercise and Prevention of Sarcopenia. Basic and Clinical Practice of Sarcopenia. Shinko Trading Company Publication Department of Medical Books; Tokyo, Japan: 2011:155–162. Japanese. | ||
Paik NJ, Kim SJ, Lee HJ, Jeon JY, Lim JY, Han TR. Movement of the hyoid bone and the epiglottis during swallowing in patients with dysphagia from different etiologies. J Electromyogr Kinesiol. 2008; 18(2):329–335. | ||
Nagy A, Molfenter SM, Peladeau-Pigeon M, Stokely S, Steele CM. The effect of bolus volume on hyoid kinematics in healthy swallowing. Biomed Res Int. 2014;2014:738971. | ||
Ueda N, Nohara K, Tanaka N, Kaneko N, Sakai T. A comparison of the maximum hyoid velocity in healthy adults and dysphagic patients. Dysphagia. 2013;28:646. | ||
Ueda N, Nohara K, Kotani Y, Tanaka N, Okuno K, Sakai T. Effects of the bolus volume on hyoid movements in normal individuals. J Oral Rehabil. 2013;40(7):491–499. | ||
Raj IS, Bird SR, Shield AJ. Aging and the force-velocity relationship of muscles. Exp Gerontol. 2010;45(2):81–90. | ||
Nam HS, Beom J, Oh BM, Han TR. Kinematic effects of hyolaryngeal electrical stimulation therapy on hyoid excursion and laryngeal elevation. Dysphagia. 2013;28(4):548–556. | ||
Sia I, Carvajal P, Lacy AA, Carnaby GD, Crary MA. Hyoid and laryngeal excursion kinematics – magnitude, duration and velocity – changes following successful exercise-based dysphagia rehabilitation: MDTP. J Oral Rehabil. 2015;42(5):331–339. | ||
Seo HG, Kim JG, Nam HS, Lee WH, Han TR, Oh BM. Swallowing function and kinematics in stroke patients with tracheostomies. Dysphagia. 2017;32(3):393–400. | ||
Maruyama H. Standard physical therapy Professional Area Therapeutic Exercise Detailed Exposition. 2nd ed. Yoshio M, editors. Therapeutic Exercise in Elderlies. IGAKU-SHOIN; Tokyo, Japan: 2006:382–388. Japanese. | ||
Machida N, Tohara H, Hara K, et al. Effects of aging and sarcopenia on tongue pressure and jaw-opening force. Geriatr Gerontol Int. 2017;17(2):295–301. | ||
Feng X, Todd T, Lintzenich CR, et al. Aging-related geniohyoid muscle atrophy is related to aspiration status in healthy older adults. J Gerontol A Biol Sci Med Sci. 2013;68(7):853–860. | ||
Fielding RA, LeBrasseur NK, Cuoco A, Bean J, Mizer K, Fiatarone Singh MA. High-velocity resistance training increases skeletal muscle peak power in older women. J Am Geriatr Soc. 2002;50(4): 655–662. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.