")
Back to Journals » Clinical Interventions in Aging » Volume 11
Height and sex is strongly associated with radial augmentation index in Korean patients with never-treated hypertension
Authors Ahn KT, Park K, Kim MJ, Oh JK, Han J, Kwon HJ, Jin SA, Kim J, Park J, Lee J, Choi S, Seong I, Jeong J
Received 25 November 2015
Accepted for publication 23 January 2016
Published 11 April 2016 Volume 2016:11 Pages 415—422
DOI https://doi.org/10.2147/CIA.S101302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Kye Taek Ahn, Kwang-In Park, Mi Joo Kim, Jin Kyung Oh, Ji Hye Han, Hee Jin Kwon, Seon-Ah Jin, Jun-Hyung Kim, Jae-Hyeong Park, Jae-Hwan Lee, Si Wan Choi, In-Whan Seong, Jin-Ok Jeong
Department of Internal Medicine, Division of Cardiology, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Republic of Korea
Objectives: Central hemodynamics may better represent the load imposed on the coronary and cerebral arteries and thereby bear a stronger relationship to cardiovascular outcomes.
Methods: Patients who had confirmed hypertension as assessed by daytime 24-hour ambulatory blood pressure monitoring (≥135/85 mmHg) were enrolled. Central blood pressure and radial augmentation index (AIx) corrected for a heart rate of 75 bpm (radial AIx 75) were measured for all patients. We evaluated the association of age, height, and sex with central hemodynamics in patients with never-treated hypertension.
Results: A total of 203 patients were enrolled, of whom men numbered 101 (49.7%). The median height of all patients was 162 cm, and mean age was 53.2 years. In the Pearson correlation analysis, regardless of sex difference (R=-0.627 for height, R=0.035 for age, P-value =0.005), a stronger relationship was observed between height and radial AIx 75 than between age and radial AIx 75. In the multiple regression analysis, the sex difference and height were strongly associated with elevated radial AIx 75 in all patients (adjusted R2=0.428, β=6.237, 95% confidence interval [CI] for women 1.480–10.995, P-value =0.011 and β=-0.632, 95% CI for height -0.929 to -0.335, P-value =0.009, respectively).
Conclusion: In patients with never-treated hypertension, female sex and shorter height are the important risk factors of elevated radial AIx 75.
Keywords: hypertension, augmentation index, height, sex
Introduction
Central hemodynamics could better explain the load imposed on the coronary and cerebral arteries and thereby bear a stronger relationship to cardiovascular outcomes than brachial blood pressure (BP) does.1,2
Augmentation index (AIx) can be easily and noninvasively recorded by radial applanation tonometry and is well-known as an important predictor of cardiovascular events and all-cause mortality over brachial BP parameter.1,2 It is well-known that radial AIx is strongly correlated with aortic AIx.3
Arterial stiffness and early wave reflections lead to the augmentation of central aortic pressure wave amplitude, and height would be inversely related to AIx. Several studies showed that height is inversely related to the risk of cardiovascular disease.4–8 It was initially reported in 1951 by Gertler et al,9 and has since been repeatedly reported in the recent era also. A recent large study reported that height is inversely and independently related to central hemodynamics, including AIx.10 However, most of these results are derived from patients with established disease (ie, hypertension, end-stage renal disease, or coronary artery disease), and conflicting opinions that the increased central hemodynamics were strongly related to sex and aging than lower height exist.10–14
Therefore, we evaluated the association between central hemodynamics and age, height, and sex in patients with never-treated hypertension.
Patients and methods
Study population
Between August 2011 and July 2014, a total of 203 patients were retrospectively enrolled in the Chungnam National University Hospital. Enrolled patients were diagnosed with hypertension by daytime 24-hour ambulatory blood pressure monitoring (ABPM; ≥135/85 mmHg) and had no experience of taking antihypertensive agents. The study was approved by the Institutional Review Board of Chungnam National University Hospital. This study was exempt from written informed consent due to the fact that it was a retrospective study.
Methods and definitions
Multiple measurements of the out-of-office brachial BP were obtained from the oscillometric ABPM recorders (TONOPORT V, GM Medical System, Berlin, Germany; Mobil-O-Graph new generation, I.E.M., Stolberg, Germany), as previously validated.15,16 Central BPs and radial AIx were noninvasively measured by using a validated device (HEM-9000AI, Omron Healthcare, Kyoto, Japan),17 while the patient was made to sit on the prepared chair with the cuff wrapped around the upper part of patient’s right arm and the aortic insufficiency pulse wave sensor unit placed on the radial artery of patient’s left wrist. Central systolic BP (SBP), diastolic BP (DBP), pulse pressure (PP), augmentation pressure, and radial AIx were measured using the technique of pulse waveform analysis. PP was calculated as the difference between respective systolic and diastolic pressure. Radial AIx was calculated as follows: (second peak SBP2 – DBP)/(first peak SBP – DBP) ×100 (%). In addition, given that the AIx is influenced by heart rate, the index was corrected for a heart rate of 75 bpm. PP amplification was calculated as the ratio of the peripheral to central PP, in percentage, as well.
Early-morning BP was defined as the average of BP readings taken 2 hours after waking up. Early-morning BP surge (EMBPS) was defined as the difference of the mean early-morning SBP and the lowest night SBP. Recorders were programmed to measure brachial BP at 30-minute intervals during the daytime (from 7 am to 10 pm) and at 60-minute intervals during the nighttime (from 10 pm to 7 am). Degree of dipping was calculated as 1 minus the ratio of daytime mean SBP to nighttime mean SBP and was presented in percentage.
Height and weight were measured along with central BP measurement. Height was measured with each participant’s head in the Frankfurt plane to the nearest 0.1 cm by using a DS-102 apparatus (Dong Shan JENIX Co. Ltd., Seoul, Republic of Korea), and body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared.
Statistical analysis
This study is a cross-sectional study. Continuous variables were expressed as the mean ± standard deviation and then were compared using the independent Student’s t-test. Statistical significances were also tested by one-way analysis of variance (ANOVA) combined with Tukey’s post hoc analysis. Categorical variables were compared with Pearson’s chi-square or Fisher’s exact tests and were presented as absolute and relative frequencies (%). Pearson’s simple correlation analyses were performed to determine the association between AIx and height and age. Differences between the slopes association of AIx 75 with height and age were assessed by Pearson’s correlation and Hotelling test. Differences between the slopes association of radial AIx 75 with height and age of men and women were assessed by Pearson’s correlation using Fisher’s Z-transformation. Simple linear regression analysis was performed to determine the independent association of radial AIx 75 with clinical variables and hemodynamic parameters. The following variables were included in the multivariate analysis when they were available from all patients and were significantly related to radial AIx 75 on univariate analysis: age, height, sex, diabetes mellitus (DM), smoker, high density lipoprotein (HDL), 24hr-ABPM day SBP, 24hr-ABPM mean heart rate (HR), and EMBPS.
Results
Baseline characteristics according to sex and height
A total 203 patients were enrolled. The median height of all patients was 162 cm. The data in Table 1 shows the comparison between the clinical variables according to the sex. Height and BMI were significantly lower in women. Although blood urea nitrogen and creatinine were significantly different in both groups, they were in the normal range. The incidence of smoking was lower in women. The shorter height group was defined as a group with height less than median value and the taller height group was defined as a group with height more than median value. When the clinical variables were compared according to the median height in each sex, the shorter height group was found to be older in both men and women, but BMI was increased only in taller height group of men. Other than age and BMI, no other difference was observed between shorter height group and taller height group in both sexes (Table 2).
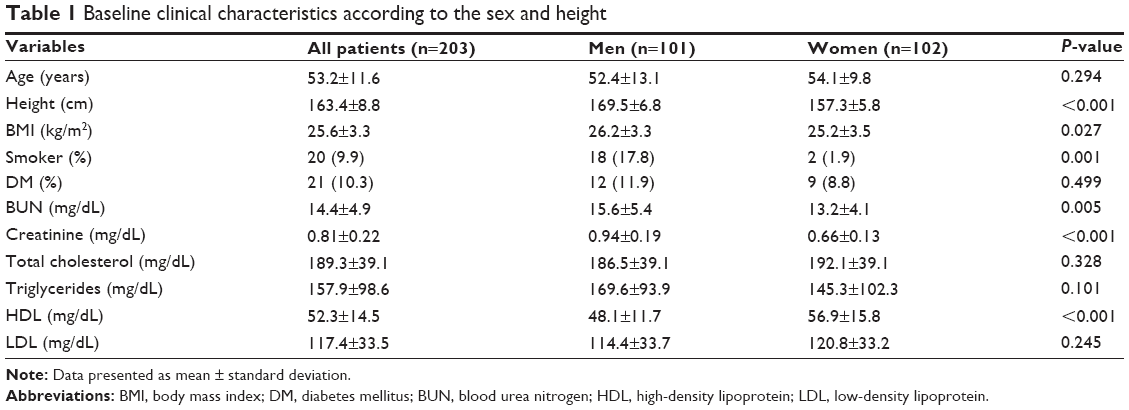 | Table 1 Baseline clinical characteristics according to the sex and height |
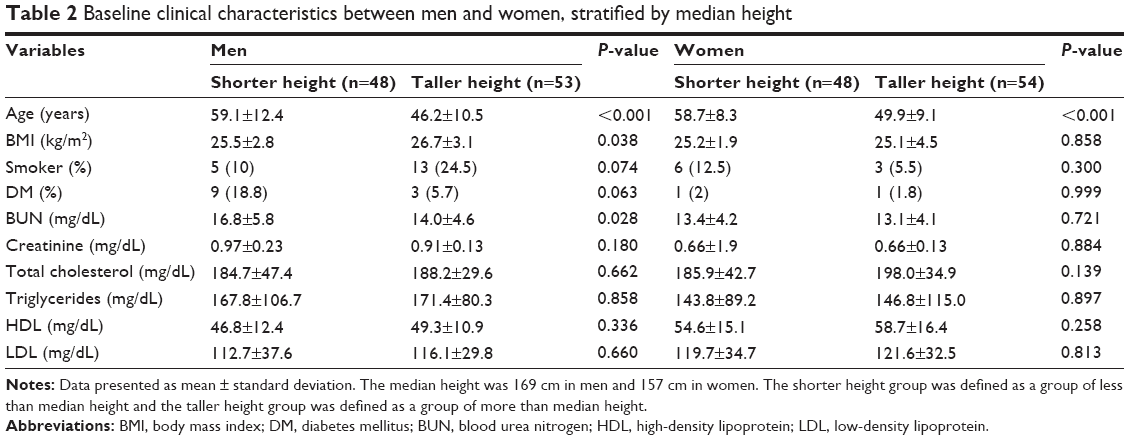 | Table 2 Baseline clinical characteristics between men and women, stratified by median height |
Hemodynamic characteristics according to sex and height
When the 24-hour ABPM data and central BP were compared according to the median height in each sex, radial AIx 75 and central PP were elevated in the shorter height group in both sexes. However, the 24-hour ABPM parameters showed no difference between shorter height group and taller height group in men, except EMBPS and morning mean SBP. In women, only 24-hour ABPM DBP parameters were elevated in taller height group, but the other parameters showed no differences between shorter height group and taller height group (Table 3).
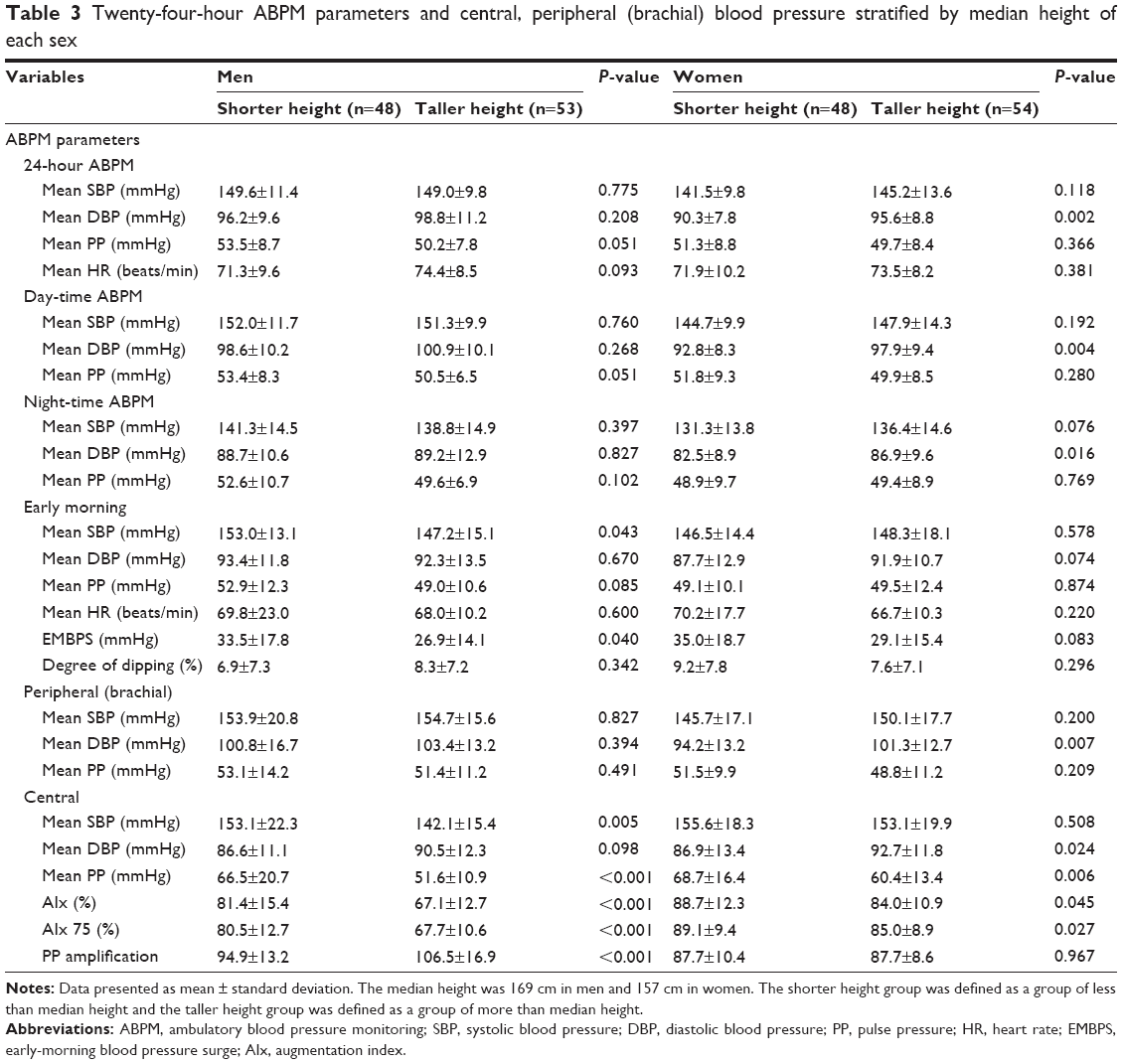 | Table 3 Twenty-four-hour ABPM parameters and central, peripheral (brachial) blood pressure stratified by median height of each sex |
Relationship between height and central hemodynamics
In the one-way ANOVA, as the quartile of height increases with statistical significance, radial AIx 75 showed a gradually decreasing tendency (Figure 1). Radial AIx 75 was inversely correlated with height but was positively correlated with age in Pearson’s correlation analysis (Figure 2). In the Pearson correlation and Hotelling test, the slope of the association between height and radial AIx 75 was significantly stronger than the slope of the association between age and radial AIx 75 (Pearson R=−0.627 for height and 0.035 for age, P-value =0.005; Figure 2A and D). In Pearson’s correlation analysis using Fisher’s Z-transformation, the slope of the association between height and radial AIx 75 showed no difference between men and women (Pearson R=−0.539 for men and −0.309 for women, P-value =0.222; Figure 2B and C). The slope of the association between age and radial AIx 75, however, was significantly stronger in men (Pearson R=0.450 for men and 0.198 for women, P-value =0.043; Figure 2E and F). A statistically significant association with the radial AIx 75 in multiple regression analysis was observed in all patients and according to sex difference (Table 4). Each model included traditional cardiovascular risk factors or variables that showed significant association in simple linear regression analysis (P-value <0.05; Table 5). The global R2 is 0.428 in all patients and is 0.280 in men and 0.154 in women. Associated variables were age (β coefficient =0.232; 95% confidence interval [CI] =0.060–0.404; P-value =0.009) and female sex (β coefficient =6.237; 95% CI =1.480–10.995; P-value =0.011), showing that these factors had adverse effect on elevation of AIx 75 in all patients. Taller height (β coefficient =−0.632; 95% CI =−0.929 to −0.335; P-value <0.001) was related to decrease of radial AIx 75. The radial AIx 75 was significantly associated with age (β coefficient =0.296; 95% CI =0.054–0.538; P-value <0.017) and height (β coefficient =−0.789; 95% CI =−1.247 to −0.330; P-value =0.001) in men, and with height (β coefficient =−0.396; 95% CI =−0.782 to −0.011; P-value =0.44) in women.
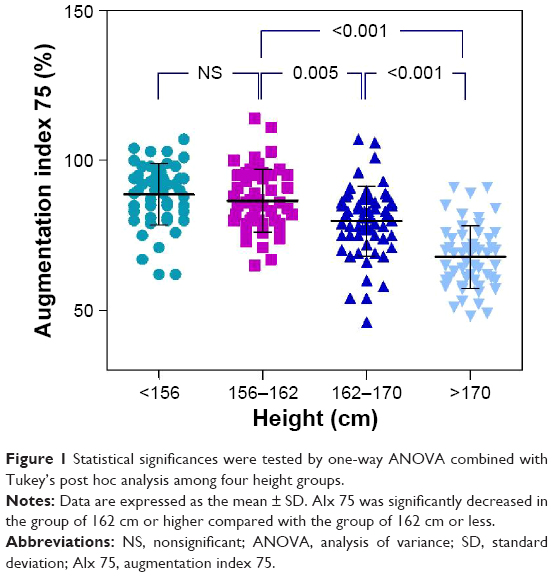 | Figure 1 Statistical significances were tested by one-way ANOVA combined with Tukey’s post hoc analysis among four height groups. |
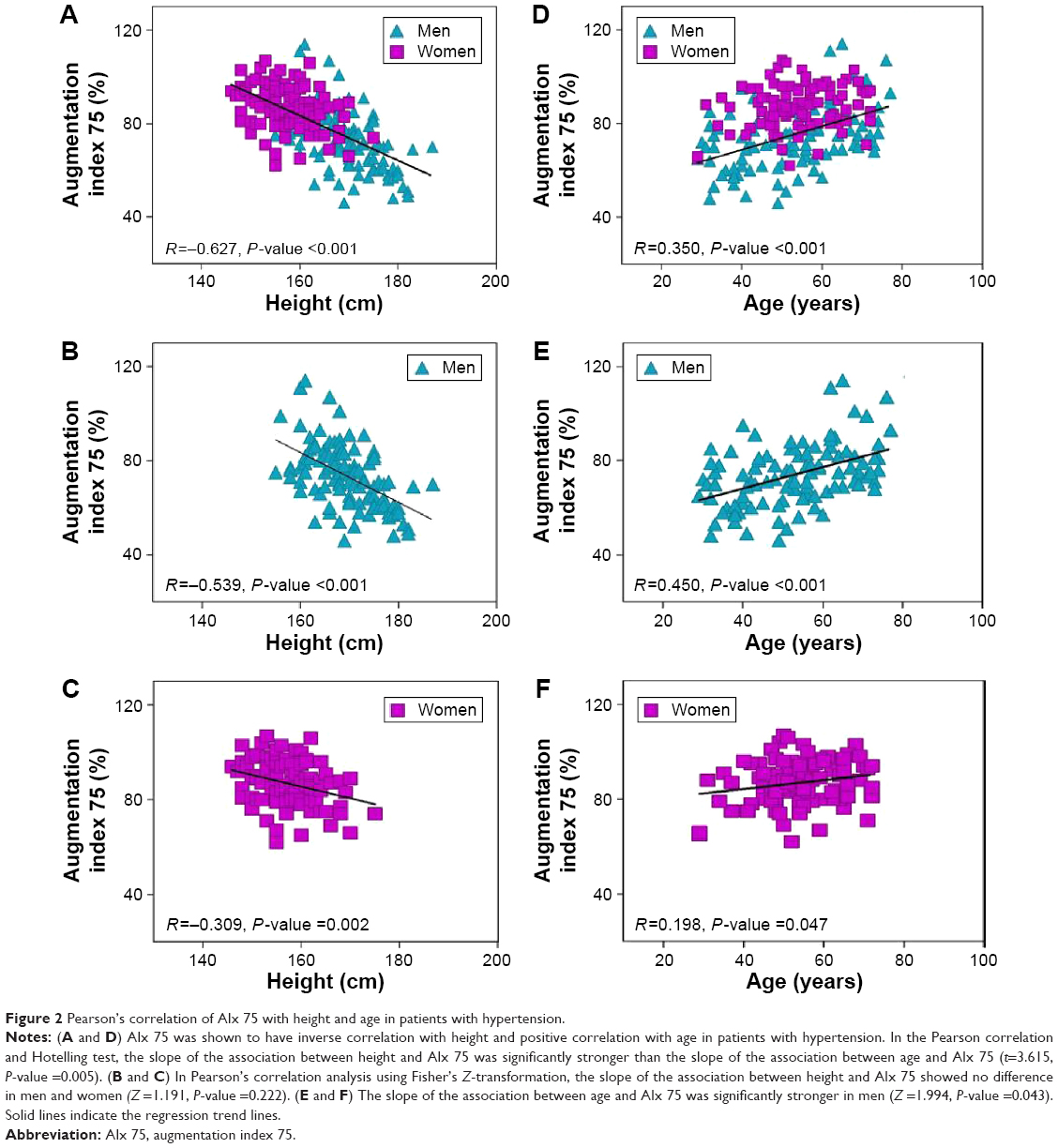 | Figure 2 Pearson’s correlation of AIx 75 with height and age in patients with hypertension. |
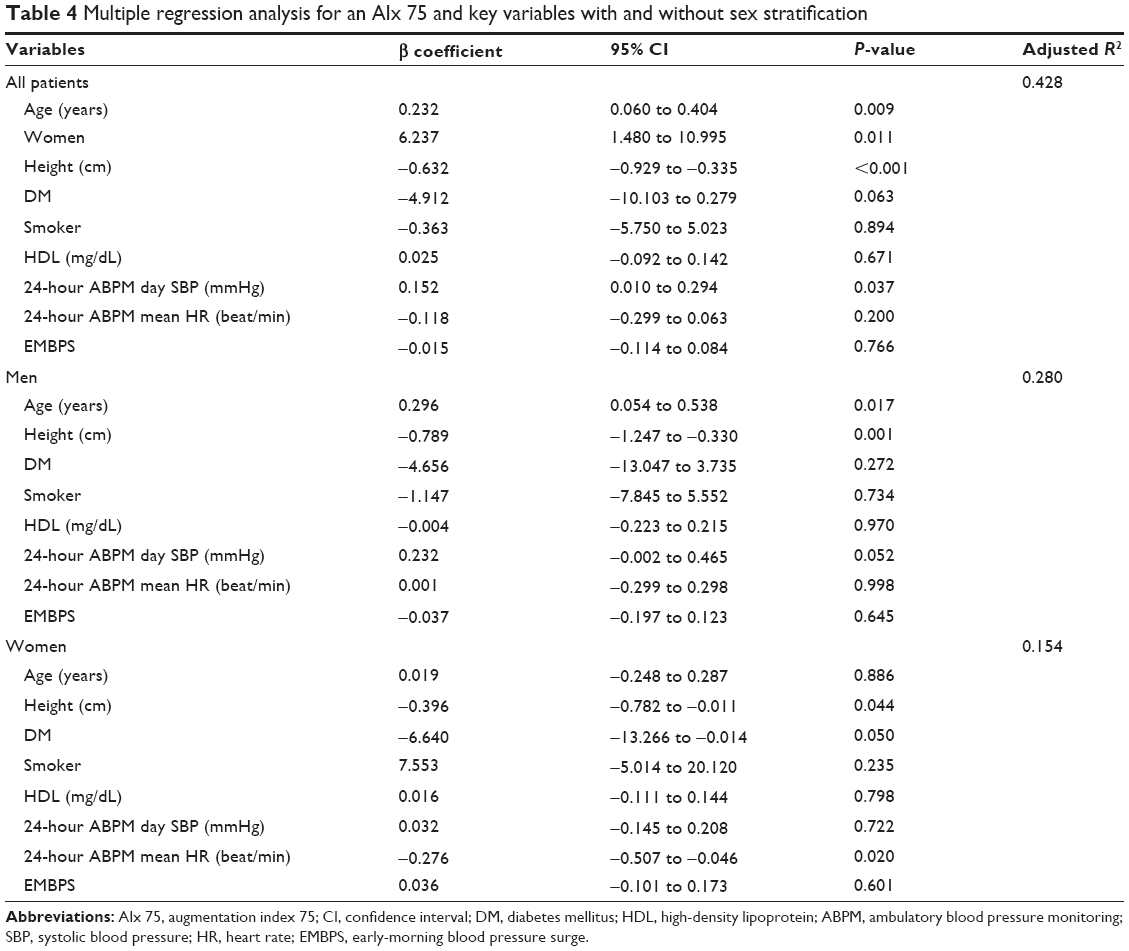 | Table 4 Multiple regression analysis for an AIx 75 and key variables with and without sex stratification |
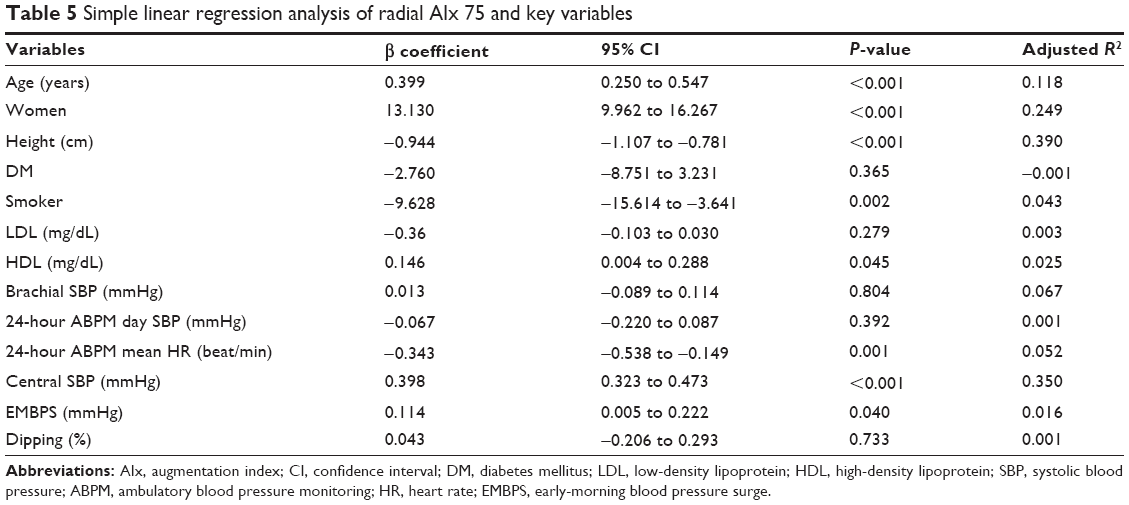 | Table 5 Simple linear regression analysis of radial AIx 75 and key variables |
Discussion
The main finding of our study is that the height, sex, and age are strongly correlated with radial AIx 75 in patients with never-treated hypertension; the radial AIx 75 was significantly associated with age and height in men. However, only height was associated with radial AIx 75 in women.
Elevated arterial stiffness is a strong prognostic marker for cardiovascular mortality. Previously, several studies evaluated whether various central hemodynamics could predict cardiovascular events.12,18,19 Roman et al19 reported that noninvasively determined central PP is more strongly related to vascular hypertrophy, extent of atherosclerosis, and cardiovascular events than to brachial BP.19 Recent meta-analysis showed central hemodynamics including AIx and central SBP and PP are important predictive values of CV events. Among these central hemodynamics, only AIx is a predictive value of all-cause mortality in a wide variety of the population.2 Elevated central hemodynamics is known to be strongly related to aging process, sex, and low stature.10,13,14,20 However, there are some conflicting opinions about the importance of these factors in affecting central hemodynamics. Shim et al13 reported that women had more elevated central hemodynamics compared to men; the elevation of central hemodynamics and the change of diastolic function are mainly due to sex difference rather than height, although height was significantly lower in women than in men. Mitchell et al14 also evaluated the relationship between arterial stiffness and advancing age in a healthy population and reported that height was not sufficient to fully explain the higher reflected wave pressure in women in multivariable analyses. Kohara et al3 reported that the radial AIx is higher in women than in men, and the difference persists even after body height was adjusted. In contrast to these opinions, Smulyan et al8 showed that stiff aorta is related to short stature. Reeve et al10 reported that height is inversely and independently related to central hemodynamics after correction for traditional cardiovascular risk factor, regardless of sex difference.
In our study, radial AIx 75 and central PP are elevated in the shorter height group in both sexes. In the multiple regression analysis, only shorter height was an important factor of elevated radial AIx 75, regardless of sex. However, the adjusted R2 of women was lower than that of all patients in the multiple regression analyses, and thus, these results imply that the shorter height has less influence on the elevation of radial AIx 75 in women than it does in men; sex difference is significantly related to the elevation of radial AIx 75.
With shorter height, the reflected wave is transmitted faster and arrives in systole, resulting in augmentation of systolic pressure, increased cardiac workload, loss of augmentation of diastolic pressure, and decreased coronary perfusion. Finally, AIx reflects the overall interaction between the arterial tree and the left ventricle. In addition, increased AIx could deteriorate cardiac function and arterial stiffness. Moreover, sex difference is important in affecting the elevation of AIx. Women had larger reflected waves than men, because of shorter height and closer physical proximity between the heart and reflecting sites.14 Mismatch between femoral-to-abdominal aortic dimension also contributes to the elevation of augmentation pressure in women.21 The smaller diameter of the radial artery and higher pulse wave velocity in women has also been reported to account for the higher AIx in women.22
These physical differences and the mismatch of arterial dimension would result in change of AIx between men and women. Hormonal effect could also influence the elevation of augmentation pressure in women. There are some reports on the unfavorable effect of a lack of estrogen due to menopause, as well as the favorable effects of administered estrogen. The absence of estrogen in older women could contribute to the elevation of SBP.8,23,24 Although we did not check the menopausal state of women, the mean age of women was 54 years; so, many postmenopausal women have probably been recruited in our study.
Peripheral BP parameters were obtained from 24-hour ABPM (different from other study), as they represent the circadian variation of the reported variables, which is better than the single measurement.25 Especially, EMBPS was significantly different between shorter height group and taller height group in men. Twenty-four-hour ABPM parameters might be related with height, aging, and sex difference.
The results of this study were similar to those of earlier studies that reported the link between central hemodynamics and height and sex. What is different from those data is that we analyzed patients with newly diagnosed hypertension who had no history of taking any antihypertensive agents. We collected patients with relatively low cardiovascular risk. It is evident that sex and height play an important role in changing the arterial stiffness in our study.
Limitations
We did not evaluate the relationship between height and cardiovascular mortality. This study is retrospectively evaluated and has a small sample size. There were significant differences in baseline clinical characteristics according to the sex and height differences. As we included only Korean patients, the ethnic character might influence our results. We did not identify menopausal status of women.
Conclusion
In this study of patients with never-treated hypertension, shorter height and sex difference are the important risk factors for elevated radial AIx 75, in addition to aging.
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2014R1A6A1029617) and Chungnam National University Hospital Research Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
Vlachopoulos C, Aznaouridis K, O’Rourke MF, Safar ME, Baou K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur Heart J. 2010;31(15):1865–1871. | ||
Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318–1327. | ||
Kohara K, Tabara Y, Oshiumi A, Miyawaki Y, Kobayashi T, Miki T. Radial augmentation index: a useful and easily obtainable parameter for vascular aging. Am J Hypertens. 2005;18(Suppl 1):11S–14S. | ||
Rich-Edwards JW, Manson JE, Stampfer MJ, et al. Height and the risk of cardiovascular disease in women. Am J Epidemiol. 1995;142(9):909–917. | ||
Lee CM, Barzi F, Woodward M, et al. Adult height and the risks of cardiovascular disease and major causes of death in the Asia-Pacific region: 21,000 deaths in 510,000 men and women. Int J Epidemiol. 2009;38(4):1060–1071. | ||
Weber T, Auer J, O’Rourke MF, et al. Increased arterial wave reflections predict severe cardiovascular events in patients undergoing percutaneous coronary interventions. Eur Heart J. 2005;26(24):2657–2663. | ||
Smulyan H, Marchais SJ, Pannier B, Guerin AP, Safar ME, London GM. Influence of body height on pulsatile arterial hemodynamic data. J Am Coll Cardiol. 1998;31(5):1103–1109. | ||
Smulyan H, Asmar RG, Rudnicki A, London GM, Safar ME. Comparative effects of aging in men and women on the properties of the arterial tree. J Am Coll Cardiol. 2001;37(5):1374–1380. | ||
Gertler MM, Garn SM, White PD. Young candidates for coronary heart disease. J Am Med Assoc. 1951;147(7):621–625. | ||
Reeve JC, Abhayaratna WP, Davies JE, Sharman JE. Central hemodynamics could explain the inverse association between height and cardiovascular mortality. Am J Hypertens. 2014;27(3):392–400. | ||
Németh ZK, Studinger P, Kiss I, et al. The method of distance measurement and torso length influences the relationship of pulse wave velocity to cardiovascular mortality. Am J Hypertens. 2011;24(2):155–161. | ||
Weber T, Auer J, O’Rourke MF, et al. Arterial stiffness, wave reflections, and the risk of coronary artery disease. Circulation. 2004;109(2):184–189. | ||
Shim CY, Park S, Choi D, et al. Sex differences in central hemodynamics and their relationship to left ventricular diastolic function. J Am Coll Cardiol. 2011;57(10):1226–1233. | ||
Mitchell GF, Parise H, Benjamin EJ, et al. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension. 2004;43(6):1239–1245. | ||
Haensel A, Utech K, Langewitz W. Validation of TONOPORT V blood-pressure measuring monitor in adults. J Hum Hypertens. 2005;19(9):745–749. | ||
Franssen PM, Imholz BP. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press Monit. 2010;15(4):229–231. | ||
Ding F-H, Fan W-X, Zhang R-Y, Zhang Q, Li Y, Wang J-G. Validation of the noninvasive assessment of central blood pressure by the SphygmoCor and Omron devices against the invasive catheter measurement. Am J Hypertens. 2011;24(12):1306–1311. | ||
Williams B, Lacy PS, Thom SM, et al. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes principal results of the Conduit Artery Function Evaluation (CAFE) Study. Circulation. 2006;113(9):1213–1225. | ||
Roman MJ, Devereux RB, Kizer JR, et al. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: the Strong Heart study. Hypertension. 2007;50(1):197–203. | ||
Cho SK, Cho SK, Kim KH, et al. Impacts of age on arterial stiffness and blood pressure variables in patients with newly diagnosed untreated hypertension. Korean Circ J. 2015;45:44–50. | ||
Cecelja M, Jiang B, McNeill K, et al. Increased wave reflection rather than central arterial stiffness is the main determinant of raised pulse pressure in women and relates to mismatch in arterial dimensions: a twin study. J Am Coll Cardiol. 2009;54(8):695–703. | ||
Gatzka CD, Kingwell BA, Cameron JD, et al. Gender differences in the timing of arterial wave reflection beyond differences in body height. J Hypertens. 2001;19(12):2197–2203. | ||
Staessen JA, Ginocchio G, Thijs L, Fagard R. Conventional and ambulatory blood pressure and menopause in a prospective population study. J Hum Hypertens. 1997;11(8):507–514. | ||
Szekacs B, Vajo Z, Acs N, et al. Hormone replacement therapy reduces mean 24-hour blood pressure and its variability in postmenopausal women with treated hypertension. Menopause. 2000;7(1):31–35. | ||
Bassareo PP, Marras AR, Pasqualucci D, Mercuro G. Increased arterial rigidity in children affected by Cushing’s syndrome after successful surgical cure. Cardiol Young. 2010;20(6):610–614. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.