")
Back to Journals » Drug Design, Development and Therapy » Volume 14
Evaluation of the Efficacy of Neoadjuvant Chemotherapy for Breast Cancer
Received 14 March 2020
Accepted for publication 7 May 2020
Published 18 June 2020 Volume 2020:14 Pages 2423—2433
DOI https://doi.org/10.2147/DDDT.S253961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Huan Wang, Xiaoyun Mao
Department of Breast Surgery, The First Affiliated Hospital of China Medical University, Shenyang City, Liaoning Province, People’s Republic of China
Correspondence: Xiaoyun Mao
Department of Breast Surgery, The First Affiliated Hospital of China Medical University, 155 Nanjing North Street, Heping District, Shenyang City, Liaoning Province 110001, People’s Republic of China
Tel/ Fax +86 24 83282618
Email [email protected]
Abstract: Neoadjuvant chemotherapy is increasingly used in breast cancer, especially for downstaging the primary tumor in the breast and the metastatic axillary lymph node. Accurate evaluations of the response to neoadjuvant chemotherapy provide important information on the impact of systemic therapies on breast cancer biology, prognosis, and guidance for further therapy. Moreover, pathologic complete response is a validated and valuable surrogate prognostic factor of survival after therapy. Evaluations of neoadjuvant chemotherapy response are very important in clinical work and basic research. In this review, we will elaborate on evaluations of the efficacy of neoadjuvant chemotherapy in breast cancer and provide a clinical evaluation procedure for neoadjuvant chemotherapy.
Keywords: neoadjuvant chemotherapy, breast cancer, evaluations of response
Background
Breast cancer is the most commonly diagnosed cancer in women worldwide. Neoadjuvant chemotherapy (NAC) has been demonstrated to be of great clinical value in locally advanced and inoperable breast cancer.1 NAC can convert a previous locally advanced and inoperable breast tumor into an operable tumor,2,3 and in largely operable tumors, downstaging results in a small increase (7% to 12%) in breast conservation rates.4–6 NAC is a useful tool that provides information on the impact of systemic therapies on breast cancer biology,7 eg further Capecitabine adjuvant therapy is efficacious against Her-2 negative breast cancer in patients with residual cancer following NAC.8 Previous research has indicated that patients who attain pathological complete response (pCR) to NAC have significantly longer overall survival (OS) and disease-free survival (DFS), particularly for triple negative and HER2+ breast cancer.9–11 It is therefore important to identify those patients who are most likely to benefit from NAC treatment and to understand the advantages of NAC with respect to long-term outcomes. The purpose of this review is to describe the evaluations of NAC efficacy in breast cancer.
Clinical Evaluation
Response Evaluation Criteria In Solid Tumors (RECIST) is based upon a one-dimensional measurement of tumors as described by Therasse et al in 2000.12,13 RECIST adopted a simplified measurement method using the sum of the longest diameters of target lesions, whereas previous WHO criteria used the sum of the products of the two longest diameters in perpendicular dimensions.14 In 2009, this method was modified and became the standard assessment of response to solid tumors in patients in clinical trials. The RECIST Working Group considers that RECIST should adapt in order to remain current.15 In 2009, RECIST 1.1 was published and was developed to evaluate the efficacy and activity of new cancer treatment for solid tumors.16,17 According to RECIST 1.1, Complete Response (CR) is the disappearance of all target lesions and the regression of any pathological lymph nodes (whether targeted or non-targeted) to <10 mm. Partial Response (PR) is considered if the sum of the diameters of target lesions has at least a 30% decrease, with the baseline of the total diameters used as a reference. Progressive Disease (PD) requires at least a 20% increase in the sum of diameters of target lesions, with the smallest sum on record (this includes the baseline sum if that is the smallest on record) or the appearance of a new lesion (at least 5 mm absolute increase in version 1.1) used as a reference. In addition to the relative increase of 20%, the sum must also demonstrate an absolute increase of more than 5 mm as well to guard against over calling PD when total sum is very small. (Note: one or more new lesions is also considered progression). Stable Disease (SD) is considered when shrinkage is not sufficient to qualify for PR or if an increase is not sufficient to qualify for PD, and uses the smallest sum diameters of the study as a reference.16 The total number of target lesions ranges from 5 to 2 per organ, while the minimum short axis for the measurement of lymph nodes is 1.5 cm, and they must be assessable as target lesions.16,18 RECIST 1.1 is best adapted to gauge the effect of tumor size and the assessment of lymph nodes in breast cancer patients, but these are poor indicators of outcome with pathology change. The patterns of tumor shrinkage as revealed by MR imaging were categorized into two types: concentric shrinkage and nests or dendritic shrinkage.19–21 It can be used to accurately evaluate the concentric shrinkage, but it is of limited value since it is influenced by different morphologies and different shrinkage patterns (concentric or dendritic).22 How then can we measure this accurately? Current methods for clinical evaluation consist of physical examination and conventional breast imaging with mammography and ultrasound. Physical examination is often unsatisfactory for assessment of the response of locally advanced breast cancer to neoadjuvant chemotherapy. However, advancements of imaging have made physical examination an indispensable component of accurate response evaluation that includes modalities such as two-dimensional and three-dimensional mammography ultrasound, magnetic resonance imaging, nuclear medicine techniques (positron emission tomography, PET), fusion techniques (PET-CT, PET-MRI), as well as others (eg, optical imaging).23–26
Mammographic Evaluation
Standard bilateral mammography and ultrasound imaging of the breast prior to the start of NAC are the routine screening and diagnostic examinations and are reliable tools used to determine the tumor size at diagnosis.27 Mammographic evaluation is based on the density measurement and architectural distortion, but sometimes the measurement is not accurate if the mass margin is indistinct or speculated and if masking from adjacent normal tissue is observed.28 The pre-NAC and the post-NAC mammography can provide some useful information about the response to NAC, eg decreases in the size and density of the mass on mammography are indicators of treatment response. The accuracy of the mammography measurement increases with the difference in echogenicity or densities, especially when the limits of the tumor are sharp. The post-NAC residual microcalcifications on mammography showed an overall lower correlation with the extent of the pathologic residual tumor than enhancing lesions on MRI.29 And mammography cannot provide more information about axillary metastasis.
Ultrasound Evaluation
Ultrasound is widely used in breast disease, is easy to perform, is fast and does not result in radiation exposure. It can provide a more accurate assessment of NAC-associated reduction of tumor size. Importantly, it is a better predictor of pathologic tumor size than mammography or physical examination after treatment with NAC. The decrease of tumor stiffness by ultrasound is a good predictor of pCR after 6 cycles.30 The ultrasonic signal statistics and integrated backscatter can monitor the response to NAC effectively.31 Ultrasound can measure the axillary lymph node response to NAC accurately also32.However, ultrasound is operator-dependent, and breast cancer typically becomes less cellular after NAC, even if no marked decrease in size is observed.33 Sometimes ultrasound imaging of residual tumor burden is insufficient to predict the actual response to neoadjuvant chemotherapy with adequate accuracy.34 The accuracy can be improved by patients’ characteristics such as stage, grade, subtype and biologic markers.34,35
MRI Evaluation
Previous studies indicated that breast MRI has better accuracy than mammography, ultrasound or clinical breast examination for the assessment of tumor response to NAC,36,37 especially tumor size evaluation.38 NAC can induce histopathological changes based on tumor cellularity, such as concentric or shrinkage patterns. In tumors with a scattered shrinkage pattern, if a response is present, it might not be evident by simply measuring the tumor size, as these individual scattered foci cannot be measured independently on MRI.39,40 Dynamic contrast-enhanced MRI (DCE-MRI) and quantitative diffusion-weighted imaging MRI (DWI-MRI) are new and promising techniques for breast cancer characterization and treatment monitoring during NAC.41–44 Moreover, the DWI apparent diffusion coefficient (ADC) and quantitative intravoxel incoherent motion (IVIM) are useful to accurately predict residual cancer burden (RCB).45–48 The MRI-ADC values of different types (concentric shrinkage, dendritic or nest shrinkage, and mixed shrinkage) of breast cancer shrinkage are independent factors for evaluating the pCR.19,39,49–51 The accuracy of the evaluation of tumor extent after NAC with mammography or MRI is affected by the molecular subtype.29,52 MRI can provide more reliable information to guide cancer surgery by measuring residual tumor size post-NAC with high sensitivity, but it is not currently reliable enough to allow patients to avoid surgical resection after complete imaging response. More clinical research and experience should be explored in future.
PET/CT Evaluation
PET/CT has played an important clinical role in detecting breast cancer metastasis. The metabolism-based PET-CT has shown an advantage in the discrimination of fibrosis or histiocytosis in breast cancer and metastatic lymph nodes after NAC, which may lead to no or ambiguous morphologic changes on mammography or ultrasound imaging; even smaller nodes may contain viable tumor cells.53 Based on PET, metabolic response criteria were established, including the PET Response Criteria in Solid Tumors (PERCIST) and the European Organization for Research and Treatment of Cancer (EORTC) criteria.54 Previous studies indicated that PET had higher specificity in the evaluation of axillary lymph node response to NAC.55–57 PET/CT does not stand for pathology, its sensitivity to diagnose micrometastases is limited, and the high cost of PET/CT does not allow wide application.
Pathologic Evaluation
The clinical response and pathologic response may be different in how they are evaluated, but the clinical response is related to the pathologic response. They provide valuable information on the evaluation of NAC from different standpoints. So how about the pathologic evaluation of breast cancer to NAC? Several publications have attempted to provide pathologic response criteria for NAC evaluation (Table 1).
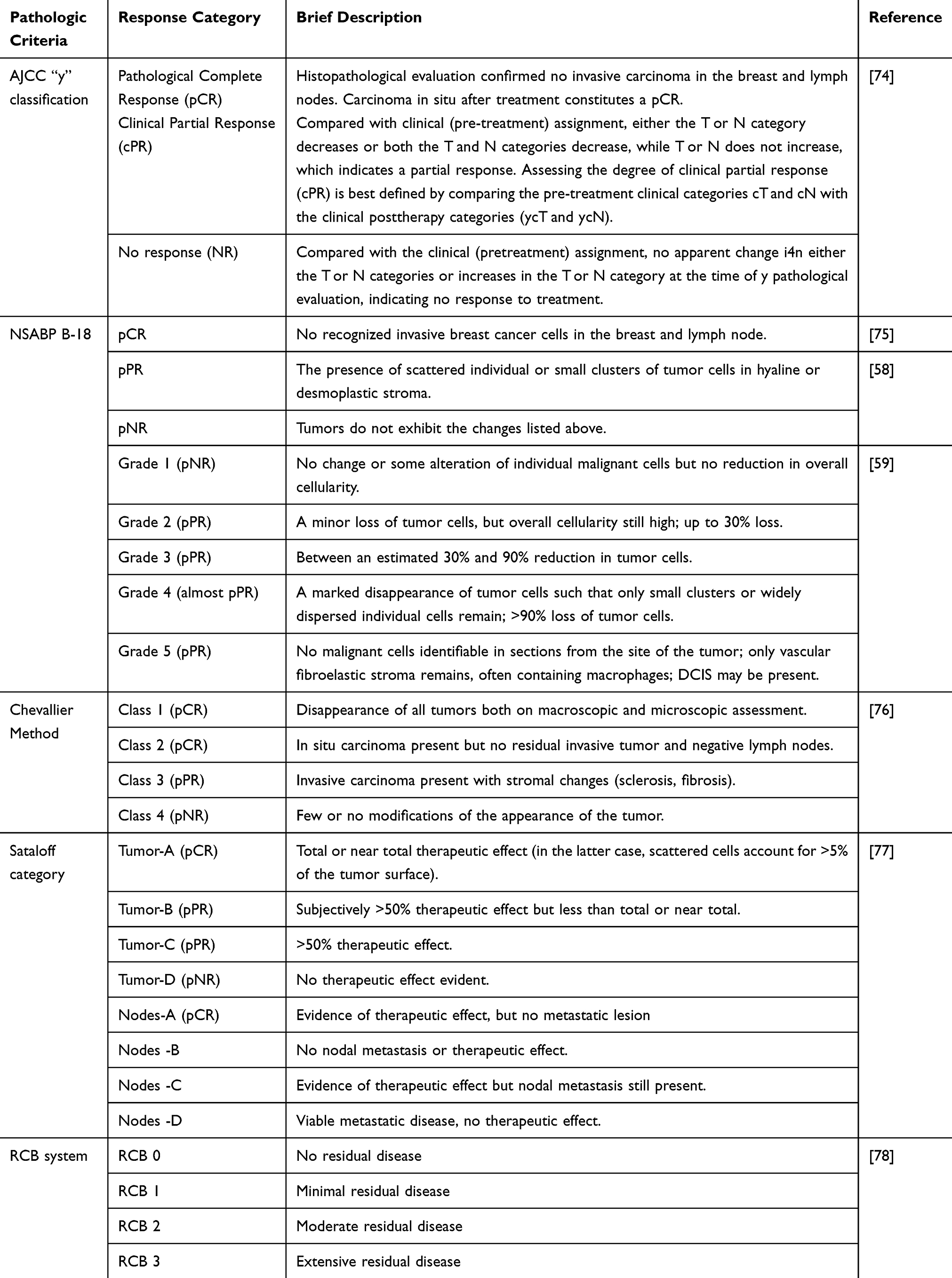 |
Table 1 Criteria of Different Pathologic Systems for Evaluation of NAC Response |
American Joint Committee on Cancer System for NAC Evaluation
The American Joint Committee on Cancer for NAC has a pretreatment clinical staging defined by radiographic and clinical findings and a postoperative pathologic stage classification based on the findings in the breast and regional lymph nodes removed at surgery with the prefix “y”. The pathological (post-treatment) Tumor category is determined by the pathological size and extent of disease. It is the greatest single focus of residual invasive breast cancer, with the modifier “m” indicating multiple foci of residual tumor. It also includes the distance over the tumor foci, tumor foci number and measurement of the largest tumor focus (not including areas of fibrosis within the tumor bed). We used the largest contiguous focus of residual tumor for classification in the postoperative pathologic node evaluation.
National Surgical Adjuvant Breast and Bowel Project Criteria System for NAC Evaluation
According to NSABP B-18 (the criteria of the National Surgical Adjuvant Breast and Bowel Project), pCR is defined as a complete pathological response without identifiable invasive tumor cells present. pPR is defined as a partial pathological response when small clusters or scattered individual tumor cells are found in the hyaline or desmoplastic stroma, and pNR denotes pathological no response, where the tumor does not exhibiting any changes.58 However, lymph node metastasis is analyzed separately.
Miller–Payne System for NAC Evaluation
The Miller–Payne system is a five-point scale that is based on cell reduction after treatment even without a marked decreased in tumor size.59 Loss in cellularity seen by pathology is associated with clinical response and prognosis. The specific morphological features shown by residual tumor cells include cytoplasmic vacuolation, cytoplasmic enlargement and gross nuclear pleomorphism.60 However, the evaluation of axillary lymph nodes is not within the Miller–Payne system. Measurement of the size of residual tumor cells by macroscopic or microscopic assessment is also not reviewed in the system.
Chevallier System for NAC Evaluation
The Chevallier system includes a 4-step algorithm to grade the response in the breast and lymph nodes. For this classification, cases with residual ductal carcinoma in situ are classified as Class 2, while cases with no residual carcinoma are classified as Class 1. The DFS and OS are different in the partial response category from the no response category in the outcome analysis.61–63
Sataloff Classification for NAC Evaluation
The Sataloff classification is based on the response of the primary carcinoma and the lymph nodes. The Sataloff T-A category is defined as a “total or near-total therapeutic effect” on the tumor, which includes small foci of invasive carcinoma and scattered tumor cells that account for less than 5% of the tumor surface. However, Sataloff’s system does not include lymphovascular infiltration (LVI). A previous study showed that patients with a Sataloff T-A response had a better 5-year survival than other categories of patients.60,64,65
Residual Cancer Burden for NAC Evaluation
Residual cancer burden is prognostic for DFS and OS among breast cancers treated with NAC.66–69 Residual cancer burden is evaluated from the two-dimensional diameter of the primary tumor from the resected specimen, the numbers of positive lymph nodes, the proportion of primary tumor beds containing invasive cells, and the maximum diameter of axillary lymph node metastases after NAC.70 To predict DFS, the RCB system is divided into 4 categories in a multiple Cox regression analysis model (RCB-0 to RCB-III).70,71 Six variables are included in a calculation formula.
Clinical-Pathologic Scoring System for NAC Evaluation
The Clinical-Pathologic Scoring System (CPS) is a Cox proportional hazard model with factors that are gradually eliminated in a backward manner. In all the clinical and pathological substage models, p <0.05 was used as a criterion for retention factors. CPS includes the clinical stage before treatment and the pathological stage after treatment. CPS+EG introduces estrogen receptor (ER) status and nuclear grade (NG), which provides an accurate prognosis for breast cancer patients.72 The CPS+EG staging system can facilitate a refined stratification of HR+/HER2 breast cancer subgroups with respect to survival after NAC.73 The Neo-Bioscore system adds HER2 status to the CPS+EG system, which incorporates preclinical stage, estrogen receptor status, histological nuclear grade and post-treatment pathologic stage, thereby allowing for more precise prognostic stratification of all breast cancer subtypes.72
The Evaluation of Axillary Lymph Nodes with NAC
The accurate evaluation of axillary lymph nodes before and after NAC may affect disease management. Ultrasonography is a fast, noninvasive inexpensive modality used to assess lymph node status, and it is also the most accurate predictor of response in lymph nodes compared with mammography and physical examination. However, ultrasonography is operator-dependent, and its sensitivity and specificity vary among different facilities. MRI also has prognostic value for the assessment of lymph node status.79 pCR was previously defined as a complete response in the breast, irrespective of axillary nodal involvement, because it was believed that the pathologic nodal status in the preoperative group was down-staged by treatment, and such an adjustment would have been invalid.80 However, no one has denied the prognostic value of pathologic nodal status. Some research groups focused on clinical early-stage breast cancer have defined pCR as the absence of invasive tumor in the breast,81,82 and their opinions suggested that nodal status was highly correlated with the pathologic response of breast tumors to neoadjuvant chemotherapy and that the primary tumor pCR was prognostic because most such patients also achieve axillary lymph node pCR.81 Now, most published research indicates that lymph node status is a similarly important prognostic factor comparable to the primary breast tumor in patients who receive NAC and that the evaluation of axillary lymph nodes is very important. For node-positive patients, either breast-only or node-only pCR indicated a better prognosis than non pCR, but those patients had a worse prognosis compared with those who experienced pCR in both the breast and axilla.83 Targeted axillary dissection (TAD) with a clip placed in the biopsy-confirmed node to evaluate the pathologic changes seen in this node compared with before NAC is a valuable tool used to assess nodal response after systemic therapy and is associated with a false-negative rate of only 4.2%.84–86 Moreover, specifically localizing and removing the clipped node in addition to removal of the sentinel lymph node (TAD procedure) can improve the pathologic evaluation for residual nodal disease after NAC. The TAD procedure involves no radioactive materials and is more stable than the tattooed nodes.84
Toxicity Evaluation of NAC
The toxicity of NAC should be evaluated also. The National Cancer Institute of USA has developed the Common Terminology Criteria for Adverse Events to standardize the reporting of adverse events by grade (level of severity) on a scale of 1 to 5.87 For the degree of severity, Grade 1: Mild, with mild or no symptoms; no interventions required. Grade 2: Moderate; minimal intervention indicated; some limitation of activities. Grade 3: Severe but not life threatening; hospitalization required; limitation of patient’s ability to care for him/herself. Grade 4: Life threatening; urgent intervention required. Grade 5: Death related to adverse event. The toxicity evaluation of NAC is composed of both the adverse event term plus the grade.
The Association of Clinical Evaluation and Pathologic Evaluation
Actually, clinical evaluation based on conventional imaging modalities is helpful in the prediction of pCR early in treatment and can provide useful information for alternate treatment options and avoid unnecessary toxicity in patients who do not experience a response. Approximately 80% of cases will experience a clinical response to NAC, and disease progression is rare. The lumpectomy volume as seen during surgery after neoadjuvant chemotherapy is based upon clinical evaluation. Before surgery, the clinical evaluation of NAC accurately predicts the pathologic response and guides individualized cancer therapy. The pathologic evaluation of the tumor and lymph nodes after surgery is the gold standard. Chemotherapy-induced histopathologic changes in breast cancer cells include dissociation, dyscohesion, shrinkage, loss of tumor cell organization and necrobiotic changes such as necrosis, nuclear and cytoplasmic vacuolation, karyorrhexis, pyknosis, and karyolysis.88 Chemotherapy-induced histopathologic changes in the stroma include fibrosis, elastosis, collagenization, and the infiltration of lymphocytes, plasma cells, fibroblasts, histiocytes and giant cells.88 Reduced tumor size and cellularity are correlated with different neoadjuvant responses.89 The focal loss of cellularity (cell density) or other focal histopathologic changes in the breast cancer bed after NAC can be imaged by mammography, ultrasound or MRI.90 Pathologic evaluation is the gold standard to determine response and is based on microscopic observations and clinical evaluation focused on the gross characteristics of the tumor as assessed by current imaging techniques or physical examination. A small number of pathological changes in tumors may not affect gross changes, but quantitative accumulation of pathological changes can lead to qualitative transformation of gross changes. Change in tumor size alone does not represent the response entirely. NAC can reduce tumor cellularity which can result in clinical and macroscopic investigation. There is no known report on the joint evaluation. It is complex and thus, more research is needed to elucidate and take advantage of these findings. None of the pathological changes can significantly predict the response to NAC.91,92 For the evaluation of NAC, the clinical and pathological evaluations each have their own advantages and disadvantages and they play different roles at different stages or angles. Can some characteristic pathological or molecular changes act as surrogate markers for predicting the pCR for NAC in breast cancer? More research is needed to answer this question.
The Clinical Evaluation Procedure of NAC
A normative standard procedure for the clinical evaluation of NAC does not exist. Before NAC, it is essential to provide information about the pathological characteristics and accurate clinical stages of breast cancer based on the physical examination and conventional imaging techniques such as mammography and ultrasound. The axillary lymph node status should be evaluated by US or should be confirmed by biopsy. New imaging techniques such as CT, MRI, PET and others can be used to glean some useful information that may assist in the accurate evaluation of response. We need more clinical trails on it. For pathological preoperative assessment, the tumor histological types, molecular breast cancer subtypes (based on the hormone receptor marker Her-2 and Ki67), the tumor cell nucleus grade, and cellularity should be evaluated by core needle biopsy. We recommend that multiple core biopsies be performed on different tumor areas or multiple tumors to define the precise nature of the lesion or the hereditary nature of the breast cancer. Regular physical examination and ultrasound, which are used to evaluate the primary tumor and axilla, should be performed to assess the response to NAC before the next chemotherapy cycle. The NAC-related adverse events should be graded using Common Terminology Criteria for Adverse Events constantly. Serious or intolerable adverse events lead to discontinuation of NAC. Ultrasound and mammography are routinely performed after completion of NAC, and MRI is recommended to help with surgical planning and response to NAC. After NAC, identification of the tumor bed is important for the accurate evaluation of NAC response. The inserted metallic clip or tattoo on the skin may help to locate the tumor bed and to ensure that the appropriate area is excised. The post-NAC breast cancer specimen should be measured in three dimensions and should be diagnosed by a pathologist. Its histological type, tumor cellularity, grade, margins, and ER/PR/HER2/Ki67 status help to accurately assess the response. If the lesion is unapparent on gross pathological examination or imaging modalities, large section processing or examination of multiple foci with microscopic evaluation will help determine the areas that contain cancer cells. This is important for documentation, especially in cases with pCR. The two dimensions of the largest cross section of an entire area involved by scatter residual tumor foci and the extent of the largest contiguous focus help to determine the size and extent of the residual tumor. Clipping the involved positive lymph node before NAC helps to verify nodal response, and the clip in the node should be identified to specify the histologic finding in that lymph node. The number of lymph nodes with metastases, the size of the largest metastasis, evidence of treatment response in metastases, and the number of lymph nodes with evidence of treatment response but no tumor cells can be used to evaluate the response of the axillary lymph node, and it is very important to note the treatment effect in lymph nodes.
Conclusions
pCR is associated with substantially longer times to recurrence and death. Even when pCR is not achieved following NAC, NAC nevertheless allows us to triage patients who did not achieve pCR so that they can be treated using additional therapy. Therefore, accurate evaluation of the response to NAC is the key factor that influences therapeutic decision-making.
Clinical evaluation by conventional imaging modalities helps to predict pCR early in treatment to provide useful information for clinical decision-making. If the ultrasound indicates that the tumor has increased in size, the tumor would actually need to be evaluated cautiously. Some cases showed no difference in tumor size except decreased cellularity. This would require additional assessment such as by MR imaging or pathologic evaluation. Sometimes tumor size assessment itself on MRI might also be challenging if NAC induced a scattered shrinkage pattern. The pathologic evaluation is then assessed by core needle biopsy after NAC. These are valuable tools for NAC evaluation, but the addition of these modalities into guidelines for NAC is challenging. Therefore, the individualized assessment of evaluations for NAC is very important. Now, we have both clinical evaluation and pathologic evaluation of the NAC response. Each type of evaluation has its own valuable information at different standpoints and has its own advantages and disadvantages. However, they also have some overlapping features. Clinical evaluation is focused on a general assessment, while pathological evaluation is focused on the microscopic assessment, but the object evaluated in both cases is the same tumor. The two evaluations should be connected to clinical application in the future. Patients with pathologic residual invasive disease after NAC have a higher risk for relapse and require individualized intensive therapy. Clinical trials based on NAC efficacy prediction will bring more inspiration to clinical practice in the real world.
Abbreviations
NAC, neoadjuvant chemotherapy; pCR, pathological complete responses; OS, overall survival; DFS, disease-free survival; RECIST, Response Evaluation Criteria In Solid Tumors; CR, complete response; PR¸ partial response; PD, progressive disease; SD, stable disease; PET¸ positron emission tomography; CT¸ computed tomography; DCE-MRI, dynamic contrast-enhanced MRI; DWI-MRI¸ quantitative diffusion-weighted imaging MRI; ADC, apparent diffusion coefficient; IVIM, quantitative Intravoxel incoherent motion; RCB¸ residual cancer burden; EORTC, European Organization for Research and Treatment of Cancer; PERCIST, PET Response Criteria in Solid Tumors; LVI, lymphovascular infiltration; CPS, Clinical-Pathologic Scoring System; ER, estrogen receptor; NG, nuclear grade; TAD, targeted axillary dissection.
Research Involving Human Participants and/or Animals
Not applicable. This article does not contain any studies with animals performed by any of the authors. This article does not contain any studies with human participants or animals performed by any of the authors.
Acknowledgment
This work was supported by the National Natural Science Foundation of China (No. 81972791). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Schegerin M, Tosteson ANA, Kaufman PA, Paulsen KD, Pogue BW. Prognostic imaging in neoadjuvant chemotherapy of locally-advanced breast cancer should be cost-effective. Breast Cancer Res Treat. 2009;114(3):537–547. doi:10.1007/s10549-008-0025-2
2. Charfare H, Limongelli S, Purushotham A. Neoadjuvant chemotherapy in breast cancer. Br J Surg. 2005;92(1):14–23. doi:10.1002/bjs.4840
3. Costa SD, Loibl S, Kaufmann M. Neoadjuvant chemotherapy shows similar response in patients with inflammatory or locally advanced breast cancer when compared with operable breast cancer: a secondary analysis of the GeparTrio trial data. J Clin Oncol. 2010;28(1):83–91. doi:10.1200/JCO.2009.23.5101
4. Katz SJ. Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. Obstet Gynecol Surv. 2009;65(14):1551–1556.
5. Buchholz TA, Mittendorf EA, Hunt KK. Surgical considerations after neoadjuvant chemotherapy: breast conservation therapy. J Natl Cancer Inst Monogr. 2015;51:51.
6. Schott AF, Hayes DF. Defining the benefits of neoadjuvant chemotherapy for breast cancer. J Clin Oncol. 2012;30(15):1747–1749. doi:10.1200/JCO.2011.41.3161
7. Vaidya JS, Massarut S, Vaidya HJ, et al. Rethinking neoadjuvant chemotherapy for breast cancer. BMJ. 2018; 360:j5913. doi:10.1136/bmj.j5913
8. Masuda N, Lee SJ, Ohtani S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. 2017;376(22):2147–2159. doi:10.1056/NEJMoa1612645
9. von Minckwitz G, Blohmer JU, Costa SD, et al. Response-guided neoadjuvant chemotherapy for breast cancer. J Clin Oncol. 2013;31(29):3623–3630. doi:10.1200/JCO.2012.45.0940
10. Spring LM, Fell G, Arfe A, et al. Pathological complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis. Clin Cancer Res. 2020. doi:10.1158/1078-0432.CCR-19-3492
11. Krishnan Y, Alawadhi SA, Sreedharan PS, Gopal M, Thuruthel S. Pathological responses and long-term outcome analysis after neoadjuvant chemotheraphy in breast cancer patients from Kuwait over a period of 15 years. Ann Saudi Med. 2013;33(5):443–450. doi:10.5144/0256-4947.2013.443
12. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000;92(3):205–216. doi:10.1093/jnci/92.3.205
13. Schwartz LH, Litière S, de Vries E, et al. RECIST 1.1-update and clarification: from the RECIST committee. Eur J Cancer. 2016;62:132–137. doi:10.1016/j.ejca.2016.03.081
14. Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer. 1981;47(1):207–214. doi:10.1002/1097-0142(19810101)47:1<207::AID-CNCR2820470134>3.0.CO;2-6
15. Schwartz LH, Seymour L, Litière S, et al. RECIST 1.1 - standardisation and disease-specific adaptations: perspectives from the RECIST working group. Eur J Cancer. 2016;62:138–145. doi:10.1016/j.ejca.2016.03.082
16. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
17. Litière S, Collette S, de Vries EG, Seymour L, Bogaerts J. RECIST - learning from the past to build the future. Nat Rev Clin Oncol. 2017;14(3):187–192. doi:10.1038/nrclinonc.2016.195
18. Muenzel D, Engels HP, Bruegel M, Kehl V, Rummeny EJ, Metz S. Intra- and inter-observer variability in measurement of target lesions: implication on response evaluation according to RECIST 1.1. Radiol Oncol. 2012;46(1):8–18. doi:10.2478/v10019-012-0009-z
19. Fukada I, Araki K, Kobayashi K, et al. Pattern of tumor shrinkage during neoadjuvant chemotherapy is associated with prognosis in low-grade luminal early breast cancer. Radiology. 2018;286(1):49–57. doi:10.1148/radiol.2017161548
20. Li M, Xu B, Shao Y, Liu H, Du B, Yuan J. Magnetic resonance imaging patterns of tumor regression in breast cancer patients after neo-adjuvant chemotherapy, and an analysis of the influencing factors. Breast J. 2017;23(6):656–662. doi:10.1111/tbj.12811
21. Eom HJ, Cha JH, Choi WJ, Chae EY, Shin HJ, Kim HH. Predictive clinicopathologic and dynamic contrast-enhanced MRI findings for tumor response to neoadjuvant chemotherapy in triple-negative breast cancer. AJR Am J Roentgenol. 2017;208(6):W225–W230. doi:10.2214/AJR.16.17125
22. Hylton NM, Blume JD, Bernreuter WK, et al. Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy–results from ACRIN 6657/I-SPY TRIAL. Radiology. 2012;263(3):663–672. doi:10.1148/radiol.12110748
23. Rauch GM, Adrada BE, Kuerer HM, van la Parra RF, Leung JW, Yang WT. Multimodality imaging for evaluating response to neoadjuvant chemotherapy in breast cancer. AJR Am J Roentgenol. 2017;208(2):290–299. doi:10.2214/AJR.16.17223
24. Li H, Yao L, Jin P, et al. MRI and PET/CT for evaluation of the pathological response to neoadjuvant chemotherapy in breast cancer: a systematic review and meta-analysis. Breast (Edinburgh, Scotland). 2018;40:106–115. doi:10.1016/j.breast.2018.04.018
25. van der Noordaa MEM, van Duijnhoven FH, Straver ME, et al. Major reduction in axillary lymph node dissections after neoadjuvant systemic therapy for node-positive breast cancer by combining PET/CT and the MARI procedure. Ann Surg Oncol. 2018;25(6):1512–1520. doi:10.1245/s10434-018-6404-y
26. Christin OL, Kuten J, Even-Sapir E, Klausner J, Menes TS. Node positive breast cancer: concordance between baseline PET/CT and sentinel node assessment after neoadjuvant therapy. Surg Oncol. 2019;30:1–5. doi:10.1016/j.suronc.2019.05.006
27. Thomassin-Naggara I, Tardivon A, Chopier J. Standardized diagnosis and reporting of breast cancer. Diagn Interv Imaging. 2014;95(7–8):759–766. doi:10.1016/j.diii.2014.06.006
28. Fowler AM, Mankoff DA, Joe BN. Imaging neoadjuvant therapy response in breast cancer. Radiology. 2017;285(2):358–375. doi:10.1148/radiol.2017170180
29. Kim YS, Chang JM, Moon HG, Lee J, Shin SU, Moon WK. Residual mammographic microcalcifications and enhancing lesions on MRI after neoadjuvant systemic chemotherapy for locally advanced breast cancer: correlation with histopathologic residual tumor size. Ann Surg Oncol. 2016;23(4):1135–1142. doi:10.1245/s10434-015-4993-2
30. Evans A, Whelehan P, Thompson A, et al. Prediction of pathological complete response to neoadjuvant chemotherapy for primary breast cancer comparing interim ultrasound, shear wave elastography and MRI. Ultraschall Med. 2018;39(4):422–431. doi:10.1055/s-0043-111589
31. Piotrzkowska-Wróblewska H, Dobruch-Sobczak K, Klimonda Z, et al. Monitoring breast cancer response to neoadjuvant chemotherapy with ultrasound signal statistics and integrated backscatter. PLoS One. 2019;14(3):e0213749. doi:10.1371/journal.pone.0213749
32. Mattingly AE, Mooney B, Lin HY, et al. Magnetic resonance imaging for axillary breast cancer metastasis in the neoadjuvant setting: a prospective study. Clin Breast Cancer. 2017;17(3):180–187. doi:10.1016/j.clbc.2016.11.004
33. Rajan R, Poniecka A, Smith TL, et al. Change in tumor cellularity of breast carcinoma after neoadjuvant chemotherapy as a variable in the pathologic assessment of response. Cancer. 2004;100(7):1365–1373. doi:10.1002/cncr.20134
34. Baumgartner A, Tausch C, Hosch S, et al. Ultrasound-based prediction of pathologic response to neoadjuvant chemotherapy in breast cancer patients. Breast (Edinburgh, Scotland). 2018;39:19–23. doi:10.1016/j.breast.2018.02.028
35. Marinovich ML, Houssami N, Macaskill P, von Minckwitz G, Blohmer JU, Irwig L. Accuracy of ultrasound for predicting pathologic response during neoadjuvant therapy for breast cancer. Int J Cancer. 2015;136(11):2730–2737. doi:10.1002/ijc.29323
36. Abedi M, Farrokh D, Shandiz Homaei F, et al. The validity of MRI in evaluation of tumor response to neoadjuvant chemotherapy in locally advanced breast cancer. Iran J Cancer Prev. 2013;6(1):28–35.
37. Choi WJ, Kim HH, Cha JH, Shin HJ, Chae EY. Comparison of pathologic response evaluation systems after neoadjuvant chemotherapy in breast cancers: correlation with computer-aided diagnosis of MRI features. AJR Am J Roentgenol. 2019;213(4):944–952. doi:10.2214/AJR.18.21016
38. Taydaş O, Durhan G, Akpınar MG, Demirkazık FB. Comparison of MRI and US in tumor size evaluation of breast cancer patients receiving neoadjuvant chemotherapy. Eur J Breast Health. 2019;15(2):119–124. doi:10.5152/ejbh.2019.4547
39. Goorts B, Dreuning KMA, Houwers JB, et al. MRI-based response patterns during neoadjuvant chemotherapy can predict pathological (complete) response in patients with breast cancer. Breast Cancer Res. 2018;20(1):34. doi:10.1186/s13058-018-0950-x
40. Lobbes MB, Lalji UC, Nelemans PJ, et al. The quality of tumor size assessment by contrast-enhanced spectral mammography and the benefit of additional breast MRI. J Cancer. 2015;6(2):144–150. doi:10.7150/jca.10705
41. Türkbey B, Thomasson D, Pang Y, Bernardo M, Choyke PL. The role of dynamic contrast-enhanced MRI in cancer diagnosis and treatment. Diagn Interv Radiol. 2010;16(3):186–192. doi:10.4261/1305-3825.DIR.2537-08.1
42. Kim Y, Kim SH, Lee HW, et al. Intravoxel incoherent motion diffusion-weighted MRI for predicting response to neoadjuvant chemotherapy in breast cancer. Magn Reson Imaging. 2018;48:27–33. doi:10.1016/j.mri.2017.12.018
43. Newitt DC, Zhang Z, Gibbs JE, et al. Test-retest repeatability and reproducibility of ADC measures by breast DWI: results from the ACRIN 6698 trial. J Magn Reson Imaging. 2019;49(6):1617–1628. doi:10.1002/jmri.26539
44. Tahmassebi A, Wengert GJ, Helbich TH, et al. Impact of machine learning with multiparametric magnetic resonance imaging of the breast for early prediction of response to neoadjuvant chemotherapy and survival outcomes in breast cancer patients. Invest Radiol. 2019;54(2):110–117. doi:10.1097/RLI.0000000000000518
45. You C, Li J, Zhi W, et al. The volumetric-tumour histogram-based analysis of intravoxel incoherent motion and non-Gaussian diffusion MRI: association with prognostic factors in HER2-positive breast cancer. J Transl Med. 2019;17(1):182. doi:10.1186/s12967-019-1911-6
46. Che S, Zhao X, Ou Y, et al. Role of the intravoxel incoherent motion diffusion weighted imaging in the pre-treatment prediction and early response monitoring to neoadjuvant chemotherapy in locally advanced breast cancer. Medicine. 2016;95(4):e2420. doi:10.1097/MD.0000000000002420
47. Cho GY, Moy L, Kim SG, et al. Evaluation of breast cancer using intravoxel incoherent motion (IVIM) histogram analysis: comparison with malignant status, histological subtype, and molecular prognostic factors. Eur Radiol. 2016;26(8):2547–2558. doi:10.1007/s00330-015-4087-3
48. Mao X, Zou X, Yu N, Jiang X, Du J. Quantitative evaluation of intravoxel incoherent motion diffusion-weighted imaging (IVIM) for differential diagnosis and grading prediction of benign and malignant breast lesions. Medicine. 2018;97(26):e11109. doi:10.1097/MD.0000000000011109
49. Zhang D, Zhang Q, Suo S, et al. Apparent diffusion coefficient measurement in luminal breast cancer: will tumour shrinkage patterns affect its efficacy of evaluating the pathological response? Clin Radiol. 2018;73(10):
50. Moy L. Do tumor shrinkage patterns at breast MR imaging predict survival? Radiology. 2018;286(1):58–59. doi:10.1148/radiol.2017171975
51. Tomida K, Ishida M, Umeda T, et al. Magnetic resonance imaging shrinkage patterns following neoadjuvant chemotherapy for breast carcinomas with an emphasis on the radiopathological correlations. Mol clin oncol. 2014;2(5):783–788. doi:10.3892/mco.2014.333
52. Negrão EMS, Souza JA, Marques EF, Bitencourt AGV. Breast cancer phenotype influences MRI response evaluation after neoadjuvant chemotherapy. Eur J Radiol. 2019;120:108701. doi:10.1016/j.ejrad.2019.108701
53. Caresia Aroztegui AP, García Vicente AM, Alvarez Ruiz S, et al. 18F-FDG PET/CT in breast cancer: evidence-based recommendations in initial staging. Tumour Biol. 2017;39(10):1010428317728285. doi:10.1177/1010428317728285
54. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving Considerations for PET response criteria in solid tumors. J Nucl Med. 2009;50 Suppl 1(Suppl 1):122s–150s. doi:10.2967/jnumed.108.057307
55. Sidaway P. Early PET response predicts complete response. Nat Rev Clin Oncol. 2019;16(4):208. doi:10.1038/s41571-019-0189-1
56. Hieken TJ, Boughey JC, Jones KN, Shah SS, Glazebrook KN. Imaging response and residual metastatic axillary lymph node disease after neoadjuvant chemotherapy for primary breast cancer. Ann Surg Oncol. 2013;20(10):3199–3204. doi:10.1245/s10434-013-3118-z
57. Berriolo-Riedinger A, Touzery C, Riedinger JM, et al. [18F]FDG-PET predicts complete pathological response of breast cancer to neoadjuvant chemotherapy. Eur J Nucl Med Mol Imaging. 2007;34(12):1915–1924. doi:10.1007/s00259-007-0459-5
58. Fisher B, Brown A, Mamounas E, et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-18. J Clin Oncol. 1997;15(7):2483–2493. doi:10.1200/JCO.1997.15.7.2483
59. Ogston KN, Miller ID, Payne S, et al. A new histological grading system to assess response of breast cancers to primary chemotherapy: prognostic significance and survival. Breast (Edinburgh, Scotland). 2003;12(5):320–327.
60. Sahoo S, Lester SC. Pathology of breast carcinomas after neoadjuvant chemotherapy: an overview with recommendations on specimen processing and reporting. Arch Pathol Lab Med. 2009;133(4):633–642.
61. Arkhypchuk AI, Santoni MP, Ott S. Cascade reactions forming highly substituted, conjugated phospholes and 1,2-oxaphospholes. Angew Chem Int Ed Engl. 2012;51(31):7776–7780. doi:10.1002/anie.201202153
62. Penault-Llorca F, Abrial C, Raoelfils I, et al. Comparison of the prognostic significance of Chevallier and Sataloff’s pathologic classifications after neoadjuvant chemotherapy of operable breast cancer. Hum Pathol. 2008;39(8):1221–1228. doi:10.1016/j.humpath.2007.11.019
63. Shien T, Shimizu C, Seki K, et al. Comparison among different classification systems regarding the pathological response of preoperative chemotherapy in relation to the long-term outcome. Breast Cancer Res Treat. 2009;113(2):307–313. doi:10.1007/s10549-008-9935-2
64. Delage E, Ruelland E, Zachowski A, Puyaubert J. Eat in or take away? How phosphatidylinositol 4-kinases feed the phospholipase C pathway with substrate. Plant Signal Behav. 2012;7(9):1197–1199. doi:10.4161/psb.21305
65. Amat S, Bougnoux P, Penault-Llorca F, et al. Neoadjuvant docetaxel for operable breast cancer induces a high pathological response and breast-conservation rate. Br J Cancer. 2003;88(9):1339–1345. doi:10.1038/sj.bjc.6600916
66. Asano Y, Kashiwagi S, Goto W, et al. Prediction of survival after neoadjuvant chemotherapy for breast cancer by evaluation of tumor-infiltrating lymphocytes and residual cancer burden. BMC Cancer. 2017;17(1):888. doi:10.1186/s12885-017-3927-8
67. Lee SM, Bae SK, Kim TH, et al. Value of 18F-FDG PET/CT for early prediction of pathologic response (by residual cancer burden criteria) of locally advanced breast cancer to neoadjuvant chemotherapy. Clin Nucl Med. 2014;39(10):882–886. doi:10.1097/RLU.0000000000000531
68. Sheri A, Smith IE, Johnston SR, et al. Residual proliferative cancer burden to predict long-term outcome following neoadjuvant chemotherapy. Ann Oncol. 2015;26(1):75–80. doi:10.1093/annonc/mdu508
69. Symmans WF, Wei C, Gould R, et al. Long-term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049–1060. doi:10.1200/JCO.2015.63.1010
70. Symmans WF, Peintinger F, Hatzis C, et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J Clin Oncol. 2007;25(28):4414–4422. doi:10.1200/JCO.2007.10.6823
71. Abrial C, Thivat E, Tacca O, et al. Measurement of residual disease after neoadjuvant chemotherapy. J Clin Oncol. 2008;26(18):
72. Marmé F, Lederer B, Blohmer JU, et al. Utility of the CPS+EG staging system in hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer treated with neoadjuvant chemotherapy. Eur J Cancer. 2016;53:65–74. doi:10.1016/j.ejca.2015.09.022
73. Mittendorf EA, Jeruss JS, Tucker SL, et al. Validation of a novel staging system for disease-specific survival in patients with breast cancer treated with neoadjuvant chemotherapy. J Clin Oncol. 2011;29(15):1956–1962. doi:10.1200/JCO.2010.31.8469
74. Boughey JC, Peintinger F, Meric-Bernstam F, et al. Impact of preoperative versus postoperative chemotherapy on the extent and number of surgical procedures in patients treated in randomized clinical trials for breast cancer. Ann Surg. 2006;244(3):464–470. doi:10.1097/01.sla.0000234897.38950.5c
75. Horii R, Akiyama F. Histological assessment of therapeutic response in breast cancer. Breast Cancer (Tokyo, Japan). 2016;23(4):540–545. doi:10.1007/s12282-013-0499-6
76. Chevallier B, Roche H, Olivier JP, Chollet P, Hurteloup P. Inflammatory breast cancer. Pilot study of intensive induction chemotherapy (FEC-HD) results in a high histologic response rate. Am J Clin Oncol. 1993;16(3):223–228. doi:10.1097/00000421-199306000-00006
77. Sataloff DM, Mason BA, Prestipino AJ, Seinige UL, Lieber CP, Baloch Z. Pathologic response to induction chemotherapy in locally advanced carcinoma of the breast: a determinant of outcome. J Am Coll Surg. 1995;180(3):297–306.
78. Abrial SC, Penault-Llorca F, Delva R, et al. High prognostic significance of residual disease after neoadjuvant chemotherapy: a retrospective study in 710 patients with operable breast cancer. Breast Cancer Res Treat. 2005;94(3):255–263. doi:10.1007/s10549-005-9008-8
79. Park J, Chae EY, Cha JH, et al. Comparison of mammography, digital breast tomosynthesis, automated breast ultrasound, magnetic resonance imaging in evaluation of residual tumor after neoadjuvant chemotherapy. Eur J Radiol. 2018;108:261–268. doi:10.1016/j.ejrad.2018.09.032
80. Lombard I, Vincent-Salomon A, Validire P, et al. Human papillomavirus genotype as a major determinant of the course of cervical cancer. J Clin Oncol. 1998;16(8):2613–2619. doi:10.1200/JCO.1998.16.8.2613
81. Bear HD, Anderson S, Brown A, et al. The effect on tumor response of adding sequential preoperative docetaxel to preoperative doxorubicin and cyclophosphamide: preliminary results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2003;21(22):4165–4174. doi:10.1200/JCO.2003.12.005
82. Powles TJ, Hickish TF, Makris A, et al. Randomized trial of chemoendocrine therapy started before or after surgery for treatment of primary breast cancer. J Clin Oncol. 1995;13(3):547–552. doi:10.1200/JCO.1995.13.3.547
83. Fayanju OM, Ren Y, Thomas SM, et al. The clinical significance of breast-only and node-only pathologic complete response (pCR) after neoadjuvant chemotherapy (NACT): a review of 20,000 breast cancer patients in the national cancer data base (NCDB). Ann Surg. 2018;268(4):591–601. doi:10.1097/SLA.0000000000002953
84. Caudle AS, Yang WT, Krishnamurthy S, et al. Improved axillary evaluation following neoadjuvant therapy for patients with node-positive breast cancer using selective evaluation of clipped nodes: implementation of targeted axillary dissection. J Clin Oncol. 2016;34(10):1072–1078. doi:10.1200/JCO.2015.64.0094
85. Racz JM, Caudle AS. Sentinel node lymph node surgery after neoadjuvant therapy: principles and techniques. Ann Surg Oncol. 2019;26(10):3040–3045. doi:10.1245/s10434-019-07591-6
86. Tadros AB, Yang WT, Krishnamurthy S, et al. Identification of patients with documented pathologic complete response in the breast after neoadjuvant chemotherapy for omission of axillary surgery. JAMA Surg. 2017;152(7):665–670. doi:10.1001/jamasurg.2017.0562
87. US Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0; Updated November 27, 2017. Available from: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.
88. Sethi D, Sen R, Parshad S, Khetarpal S, Garg M, Sen J. Histopathologic changes following neoadjuvant chemotherapy in various malignancies. Int J Appl Basic Med Res. 2012;2(2):111–116. doi:10.4103/2229-516X.106353
89. Kumar S, Badhe BA, Krishnan KM, Sagili H. Study of tumour cellularity in locally advanced breast carcinoma on neo-adjuvant chemotherapy. J Clin Diagn Res. 2014;8(4):Fc09–Fc13. doi:10.7860/JCDR/2014/7594.4283
90. Atuegwu NC, Arlinghaus LR, Li X, et al. Parameterizing the logistic model of tumor growth by DW-MRI and DCE-MRI data to predict treatment response and changes in breast cancer cellularity during neoadjuvant chemotherapy. Transl Oncol. 2013;6(3):256–264. doi:10.1593/tlo.13130
91. Khanna AK, Saxena SK, Khanna S, Kumar A. Histopathological changes following anterior chemotherapy in advanced breast cancer. Indian J Cancer. 1990;27(2):109–115.
92. Aktepe F, Kapucuoğlu N, Pak I. The effects of chemotherapy on breast cancer tissue in locally advanced breast cancer. Histopathology. 1996;29(1):63–67. doi:10.1046/j.1365-2559.1996.d01-485.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.