")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Efficacy And Safety Of Travoprost Versus Timolol To Treat Early-Onset Ocular Hypertension Secondary To Vitrectomy: A Randomized Trial
Authors Fang Y, Ku H, Gan D, Jiang R, Sun X
Received 11 July 2019
Accepted for publication 18 September 2019
Published 30 September 2019 Volume 2019:13 Pages 3453—3463
DOI https://doi.org/10.2147/DDDT.S222796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianbo Sun
Yuan Fang,1,* Hsiangyu Ku,1,* Dekang Gan,1,2 Rui Jiang,1 Xinghuai Sun1–5
1Department of Ophthalmology and Visual Science, Eye and ENT Hospital, Shanghai Medical College, Fudan University, Shanghai 200031, People’s Republic of China; 2Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai 200031, People’s Republic of China; 3Key Laboratory of Myopia, Chinese Academy of Medical Sciences, Fudan University, Shanghai 200031, People’s Republic of China; 4NHC Key Laboratory of Myopia, Fudan University, Shanghai 200031, People’s Republic of China; 5State Key Laboratory of Medical Neurobiology, Institutes of Brain Science and Collaborative Innovation Center for Brain Science, Fudan University, Shanghai 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinghuai Sun; Rui Jiang
Department of Ophthalmology and Visual Science, Eye and ENT Hospital, Shanghai Medical College, Fudan University, 83 Fenyang Road, Shanghai 200031, People’s Republic of China
Tel +86 21 64377134
Email [email protected]; [email protected]
Purpose: To evaluate the efficacy and safety of travoprost 0.004% versus timolol 0.5% as an initial intraocular pressure (IOP)-lowering medication for ocular hypertension secondary to vitrectomy.
Patients and methods: We performed a randomized, controlled, observer-blinded clinical trial in the Eye & ENT Hospital of Fudan University in China. This trial was registered at www.chictr.org.cn (ChICTR1800014942) before patient enrollment. Seventy-nine adults with IOP of 25–45 mmHg secondary to vitrectomy in the latest one month were enrolled and randomized to receive travoprost 0.004% or timolol 0.5%. More drugs were administered to patients with IOP > 25 mmHg during follow-up.
Results: The mean IOP reduction at day 1 was −10.97 mmHg in the timolol group and −15.02 mmHg in the travoprost group (P = 0.006); no significant difference was observed between the groups at later time points. The number of IOP-lowering medications at day 21 was 0.64 in the timolol group and 1.15 in the travoprost group (P = 0.038), while no significant differences were observed at other time points. The proportion of single IOP-lowering medications used during the 4-week follow-up was 72.73% in the timolol group and 68.42% in the travoprost group (P = 0.692). Inflammation scores were not significantly different in the two groups at any time point. Increased ocular hyperemia occurred in 8 patients (19%) in the travoprost group and none in the timolol group (P = 0.005). There were no significant differences in other adverse events between the two groups. After logistic regression model analysis, IOP ≥ 30 mmHg, inflammation score ≥ 2, and silicone oil as tamponade were found to be the factors with significant effects on the number of IOP-lowering medications used during the 4-week follow-up.
Conclusion: Travoprost and timolol have similar efficacy and safety for treating ocular hypertension secondary to vitrectomy.
Keywords: travoprost, timolol, vitrectomy, ocular hypertension, early-onset
Introduction
Ocular hypertension is a common complication after vitrectomy, occurring in 11–56% of the patients.1–6 Ocular hypertension most often manifests in the first month after vitrectomy,5 and the mechanism involved is complex. Postoperative hemorrhage, inflammation, and pupillary block may contribute to early-onset ocular hypertension.1,2,5 Ocular hypertension secondary to vitrectomy can be classified into the open-angle and closed-angle subtypes. In most cases, it can be controlled by medications alone.5,6 However, there are no guidelines on the use of intraocular pressure (IOP)-lowering medications for treating ocular hypertension secondary to vitrectomy.
The most common IOP-lowering medications used for treating ocular hypertension secondary to vitrectomy are beta-blockers,6,7 which can suppress aqueous humor production.8,9 However, topical application of beta-blockers may trigger asthma, bradycardia, heart block, heart failure, and so on.8,9
Prostaglandin analogs (PGAs), considered as the first-line medication in primary open-angle glaucoma,10,11 have been reported to induce or reactivate inflammation in the anterior chamber,12–14 macular edema,15 and herpes simplex virus.16–18 In recent years, some clinical studies showed that PGAs were safe and effective for the treatment of uveitic glaucoma while keeping inflammation under control.19–22 Postoperative inflammation is the major mechanism underlying early-onset open-angle ocular hypertension after vitrectomy, which is similar to uveitic glaucoma. Moreover, PGAs have been reported to be widely used to treat ocular hypertension after vitrectomy in clinical practice.6,23 However, there are no controlled clinical studies evaluating PGA in the treatment of early-stage ocular hypertension secondary to vitrectomy.
Methods
Study Design
This was a prospective, single center (Eye, Ear, Nose and Throat Hospital of Fudan University, Shanghai, China), 1:1 randomized, investigator-blinded, parallel-group study. The study was conducted in accordance with Good Clinical Practice and in compliance with the ethical principles of the Declaration of Helsinki; it was approved by the Institutional Ethical Review Board of the Eye & ENT Hospital of Fudan University before the study began. The study was conducted between May 2018 and February 2019 and has been registered at www.chictr.org.cn (registration number ChICTR1800014942). Written and signed informed consent was provided by all patients.
Participants
Eligible patients were aged ≥ 18 years, had a history of 23-gauge vitrectomy in the last month, and had an IOP ≥ 25 mmHg and < 45 mmHg. Exclusion criteria were as follows: history of glaucoma or ocular hypertension, ocular trauma, or ocular surgery except cataract surgery; eyes with a closed angle of more than 90 degrees as observed under gonioscopy on the screening day or during follow-up visits; history of low heart rate or pulmonary disease; severe allergic rhinitis; corneal diseases; and use of ocular IOP-lowering medications before the screening visit (Figure 1). All vitrectomies were performed by two skilled retinal specialists.
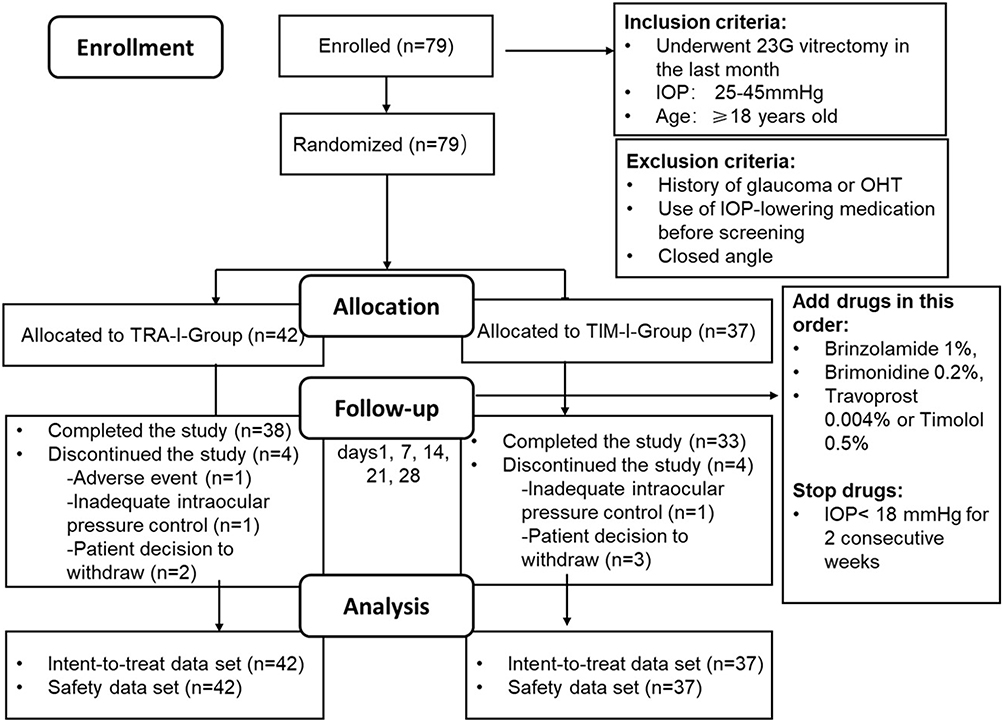 |
Figure 1 Flow-chart of the study. Patients with early-onset ocular hypertension secondary to vitrectomy receiving travoprost 0.004% or timolol 0.5% as the initial IOP-lowering medication were compared. |
Interventions
Eligible patients were randomized 1:1 to receive travoprost 0.004% (TRA-I-Group; Alcon Laboratories Inc, Fort Worth, TX, USA) or timolol 0.5% (TIM-I-Group; Wujing Medicine Co., ltd, Wuhan, Hubei, China) for 4 weeks. The random allocation sequence was generated using Excel 2010 (Microsoft, Redmond, Washington). The investigator responsible for measuring IOP was blinded to the treatment assignment. Patients were instructed to instill travoprost 0.004% in the eye with ocular hypertension once daily at bedtime or to instill timolol 0.5% twice daily at approximately 8 AM and 5 PM. The treatment phase included 5 on-therapy follow-up visits conducted on days 1, 7, 14, 21, and 28 (Figure 1). During follow-up, IOP was measured at approximately 10 AM. If the IOP was still above 25 mmHg at a follow-up visit, brinzolamide 1% (Alcon Laboratories Inc, FortWorth, TX, USA), brimonidine 0.2% (Allergan Inc, Dublin, Ireland), timolol 0.5%, or travoprost 0.004% were added separately or together in this order. If the IOP was still above 40 mmHg in the eye after administration of the four topical IOP-lowering medications, anterior chamber puncture was performed. Ocular inflammation was scored on a scale of 0 to 4 based on the degree of flare and the presence of inflammatory cells in the anterior chamber and the vitreous, as previously reported.24 Prednisolone 1% (Allergan Inc, Dublin, Ireland) was used to reduce ocular inflammation. The administration of prednisolone 1% was stopped when inflammation could not be observed in the eye and was restarted in case of recurrence. If the IOP was less than 18 mmHg for two consecutive weeks, IOP-lowering medications were removed in the reverse order in which they were added.
Efficacy Outcomes
The primary efficacy endpoint was IOP reduction from baseline on days 1, 7, 14, 21, and 28. The additional outcome was the number of additional IOP-lowering medications.
Safety Outcomes
Safety was evaluated based on inflammation scores at all time points, other ocular abnormalities found through physical examination, and adverse events reported by the patients. Most patients have some degree of ocular hyperemia early after vitrectomy; therefore, we considered the increase of ocular hyperemia, rather than ocular hyperemia, as an adverse event.
Risk Factors Analysis
In order to predict whether a patient needs more than one IOP-lowering medication, factors that may influence the number of IOP-lowering medications used were identified and analyzed.25–27 These factors included age, sex, refractive factor of patients, diagnosis, combination with lens surgery, tamponade, time of treatment initiation after vitrectomy, IOP and inflammation scores on screening, and travoprost versus timolol as the initial IOP-lowering medication.
Statistical Analysis
Statistical analysis was performed using IBM SPSS statistics version 25 (IBM, Armonk, New York). Efficacy for the primary endpoint was evaluated with intent-to-treat (ITT) analysis; the ITT set included all patients who received the study medication and completed at least one on-therapy visit. Student’s paired and unpaired t-tests and Pearson’s chi squared test were used in the safety and efficacy analyses. Risk factors were analyzed by logistic regression.
Results
Patients
Of the 79 eyes of 79 patients randomized to treatment, 42 eyes of 42 patients were included in the TRA-I-Group and 37 eyes of 37 patients in the TIM-I-Group. The age of patients in the two groups was 53.67 ± 11.60 and 51.62 ± 14.33 (mean ± standard deviation, SD) years in the TRA-I-Group and TIM-I-Group, respectively. Most patients were male (55.4%; 43/79). The baseline IOPs on screening were 32.93 ± 4.83 and 31.81 ± 5.05 (mean ± SD) mmHg in the TRA-I-Group and TIM-I-Group, respectively. The times after vitrectomy on screening were 9.17 ± 3.60 and 9.51 ± 4.57 (mean ± SD) days in the TRA-I-Group and TIM-I-Group, respectively. There were no significant differences between the groups in demographic or clinical parameters, including age, sex ratio, rate of high myopia, diagnosis, composition of tamponades, composition of combined lens surgery, baseline IOP, times after vitrectomy, or inflammation scores before treatment (Table 1), suggesting that there was no significant bias in the patients’ baseline data. Overall (Figure 1), 10.13% of the randomized patients (8/79) discontinued the study (TRA-I-Group, 9.52%, 4/42; TIM-I-Group, 10.81%, 4/37). The most common reason for discontinuation was patient withdrawal (TRA-I-Group, 4.76%, 2/42; TIM-I-Group, 8.11%, 3/37). The remaining reasons for discontinuation were inadequate intraocular pressure control (TRA-I-Group, 2.38%, 1/42; TIM-I-Group, 2.70%, 1/37) and adverse events (TRA-I-Group, 2.38%, 1/42; TIM-I-Group, 0%).
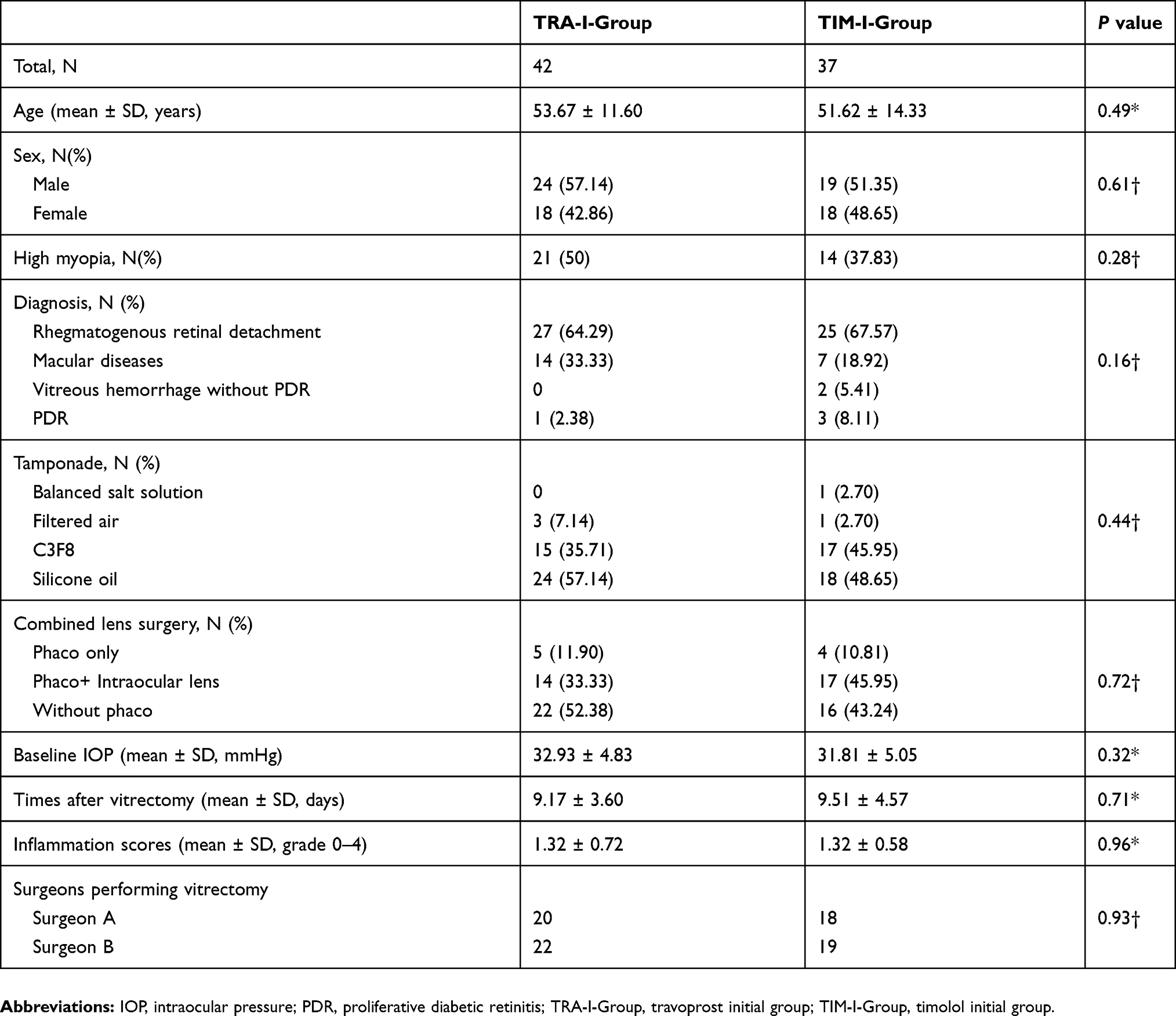 |
Table 1 Subject Demographics And Baseline Characteristics Of Patients With Ocular Hypertension Secondary To Vitrectomy |
Efficacy Outcomes
After 1-day treatment with travoprost 0.004%, IOP decreased from 32.92 ± 0.75 to 17.91 ± 0.81 (mean ± standard error, SE) mmHg in the TRA-I-Group (P < 0.001). Meanwhile, in the TIM-I-Group, IOP decreased from 31.81 ± 0.83 to 20.84 ± 1.05 mmHg after 1 day of treatment with timolol 0.5% (P < 0.001, Figure 2A). Treatment was thus effective on day 1 in both groups. Comparing the IOP reduction between the two groups on day 1, we found it to be −15.02 ± 0.97 mmHg (mean ± SE) in the TRA-I-Group and −10.97 ± 1.05 mmHg in the TIM-I-Group (P = 0.006, Figure 2B). There were no significant differences in IOP reduction between the groups on days 7, 14, 21, or 28 (Figure 2C). The proportion of patients with IOP reduction ≥ 20% was 78.38% (29/37) in the TIM-I-Group vs. 97.62% (41/42) in the TRA-I-Group (P = 0.007). Moreover, the proportion of patients with IOP reduction ≥ 30% was 56.76% (21/37) vs. 90.48% (38/42) in the TIM-I-Group and the TRA-I-Group, respectively (P = 0.001). These data showed that travoprost 0.004% has better efficacy for lowering IOP compared with timolol 0.5% on day 1.
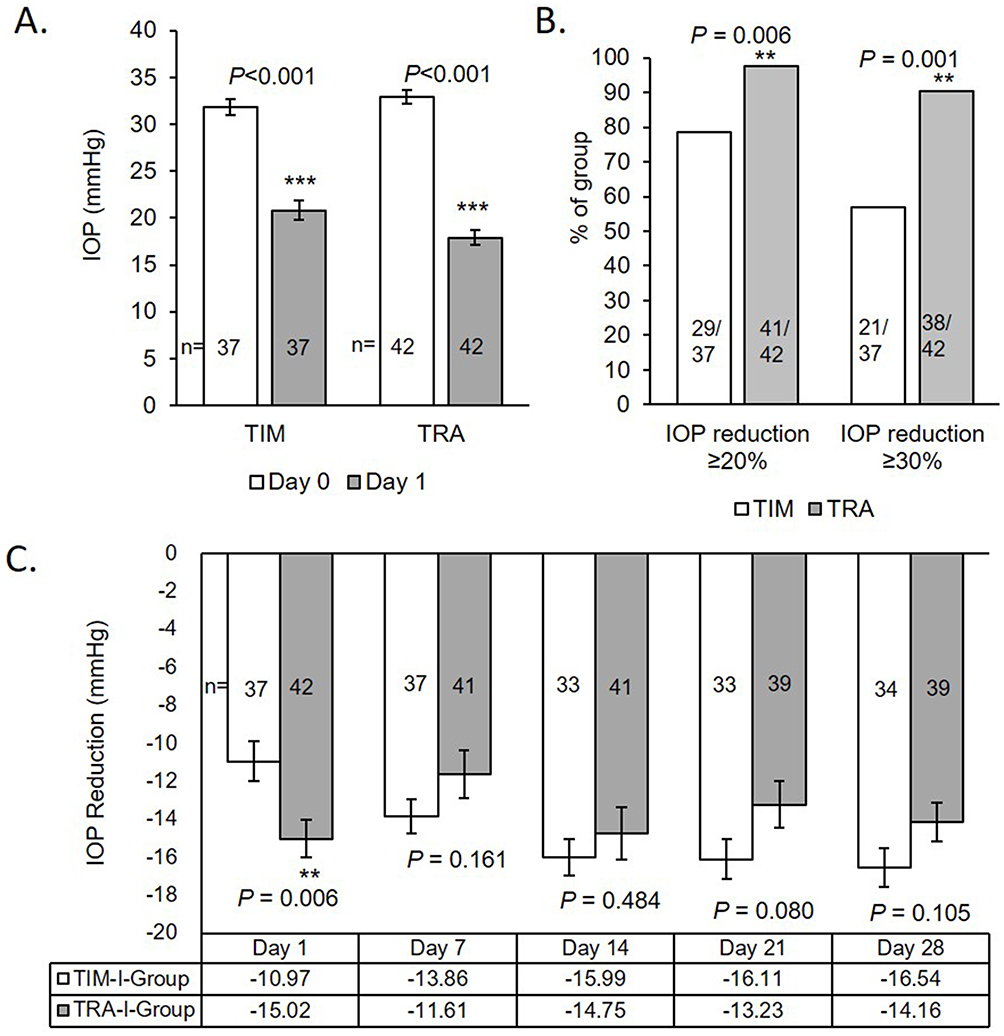 |
Figure 2 IOP reduction in the two groups. (A) After 1 day of treatment with timolol 0.5% or travoprost 0.004%, IOP decreased significantly (data are presented as mean ± standard error; p < 0.001 for both treatments, Student’s paired t-test). (B) The proportion of patients with IOP reduction ≥ 20% was 78.38% (29/37) among timolol-treated patients and 97.62% (41/42) among travoprost-treated patients, and the difference is significant (P = 0.006, Pearson’s chi squared test). The proportion of patients with IOP reduction ≥ 30% was 56.76% (21/37) among timolol-treated patients and 90.48% (38/42) among travoprost-treated patients, and the difference is significant (P = 0.001, Pearson’s chi squared test). (C) IOP reduction on day 1 significantly differed between the timolol-treated and travoprost-treated patients, while IOP reduction on days 7, 14, 21, and 28 did not. Data are presented as mean ± standard error. **P < 0.01; ***P < 0.001. Abbreviations: TIM, timolol; TRA, travoprost. |
After day 1, other IOP-lowering medications were added for patients with IOP > 25 mmHg, and the number of IOP-lowering medications was considered another efficacy index, with fewer added medications indicating better efficacy of the original medication. The number of IOP-lowering medications on day 21 was 1.15 ± 0.17 (mean ± SE) in the TRA-I-Group and 0.64 ± 0.17 in the TIM-I-Group (P = 0.038). The number of IOP-lowering medications did not differ significantly between the two groups on days 7, 14, or 28 (Figure 3A). These data suggested that timolol 0.5% has greater efficacy for lowering IOP on day 21 compared with travoprost 0.004%.
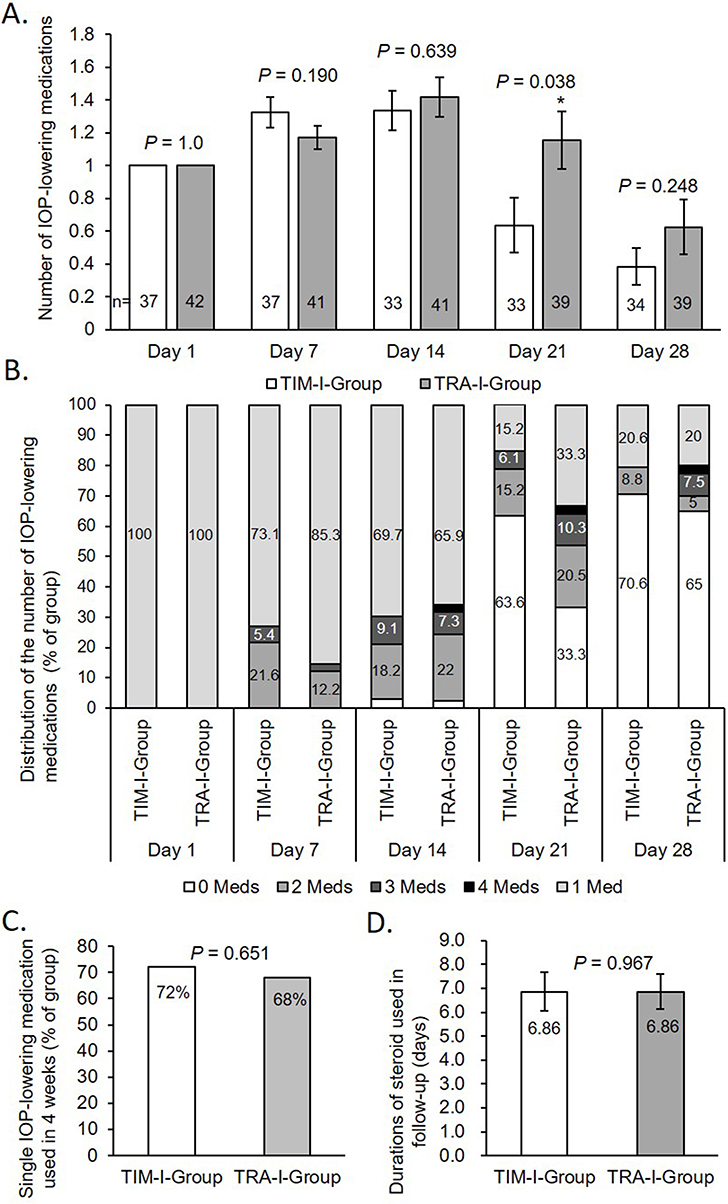 |
Figure 3 Number of medications used in the two groups. (A) The number of IOP-lowering medications in the TIM-I-Group was significantly lower than that in the TRA-I-Group (P = 0.038, Student’s t-test) on day 21, while there were no significant differences between the two groups on days 1, 7, 14, or 28 (data are presented as mean ± standard error). (B). Distribution of the number of IOP-lowering medications used in the two groups. (C) The proportion of patients using only one IOP-lowering medication during the 4-week follow-up was 72% in the TIM-I-Group and 68% in the TRA-I-Group (P = 0.651, Pearson’s chi squared test). (D) The duration of topical steroid medication use in the follow-up was 6.86 ± 0.81 days in the TIM-I-Group and 6.86 ± 0.73 days in the TRA-I-Group (data are presented as mean ± standard error, P = 0.967, Student’s t-test). *P < 0.05. Abbreviations: TRA-I-Group, travoprost initial group; TIM-I-Group, timolol initial group. |
Distribution of the number of IOP-lowering medications used in the two groups is shown in Figure 3B. The proportion of single IOP-lowering medications used during the 4-week follow-up was 72.73% in the TIM-I-Group and 68.42% in the TRA-I-Group (P = 0.692, Figure 3C). Therefore, overall, travoprost 0.004% and timolol 0.5% showed similar efficacy in lowering IOP in early-stage ocular hypertension secondary to vitrectomy.
Considering that the use of steroids might affect IOP, the duration of topical steroid use during follow-up was calculated and was found to be 6.86 ± 0.81 days (mean ± SE) in the TIM-I-Group and 6.86 ± 0.72 days in the TRA-I-Group (P = 0.967, Figure 3D). Therefore, the use of steroids in both groups was comparable and did not lead to bias when comparing the efficacy for lowering IOP in the two groups.
Safety Outcomes
In the TIM-I-Group, inflammation scores were 1.32 ± 0.095, 1.19 ± 0.11, 0.92 ± 0.13, 0.42 ± 0.12, 0.27 ± 0.090, and 0.21 ± 0.092 (mean ± SE) on days 0, 1, 7, 14, 21, and 28, respectively, and continued to decline thereafter. In the TRA-I-Group, the inflammation scores were 1.32 ± 0.11, 1.39 ± 0.12, 0.95 ± 0.13, 0.55 ± 0.15, 0.42 ± 0.11, and 0.26 ± 0.095 on days 0, 1, 7, 14, 21, and 28, respectively, thus slightly increasing from day 0 to day 1 and then gradually decreasing until day 28. Differences in inflammation scores between the two groups were not significant at any time point (Figure 4). These results suggest that travoprost may potentially increase ocular inflammation, but such increase was well-controlled in our study. Overall, the safety of the two treatments in terms of increasing inflammation was similar.
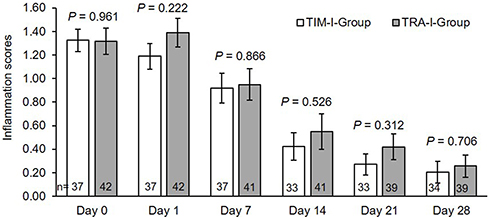 |
Figure 4 Comparison of the inflammation score in the two groups. No significant differences in inflammation score between the two groups were observed at any time point. Data are presented as mean ± standard error. Abbreviations: TRA-I-Group, travoprost initial group; TIM-I-Group, timolol initial group. |
No serious adverse events were reported in either group. In particular, reactivation of herpes simplex virus was not found in any patient. Eight patients (19%) in the TRA-I-Group and none in the TIM-I-Group had increased ocular hyperemia (P = 0.005). Nine patients (21.4%) complained of eye irritation in the TRA-I-Group compared with 3 patients (8.1%) in the TIM-I-Group (P = 0.100). Two patients (4.8%) reported eye pain after treatment in the TRA-I-Group compared to none in the TIM-I-Group (P = 0.179). One patient (2.4%) in the TRA-I-Group needed anterior puncture to decrease IOP, compared to none in the TIM-I-Group (P = 0.345, Table 2). Overall, therefore, increased ocular hyperemia was more common in the TRA-I-Group than in the TIM-I-Group, and there were no significant differences concerning other adverse events between the two groups.
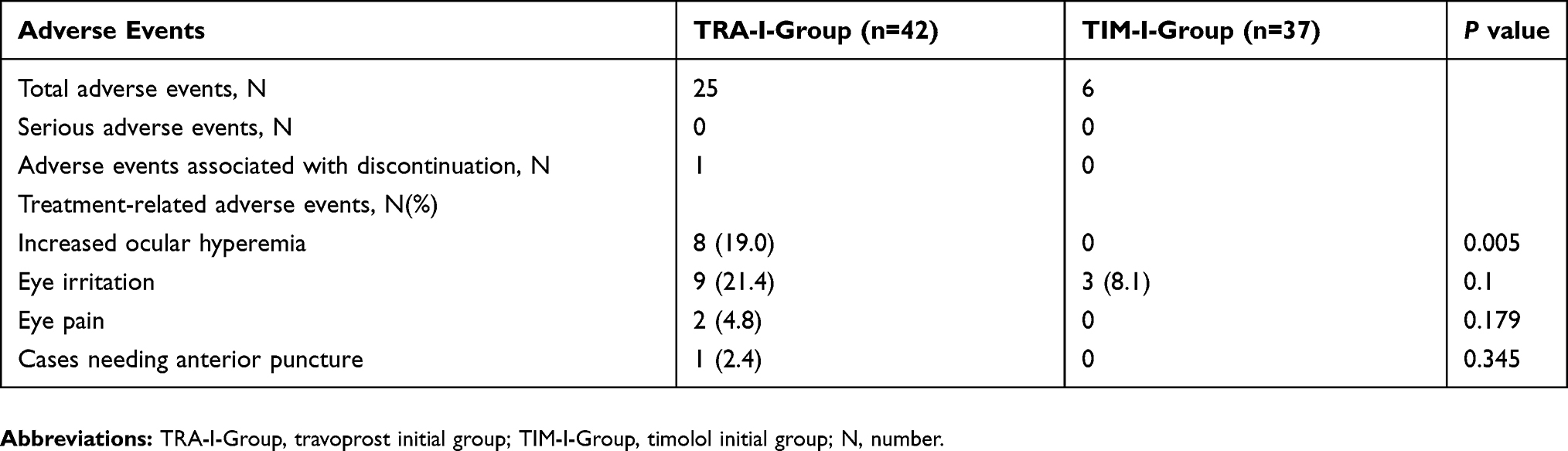 |
Table 2 Summary Of Treatment-Related Adverse Events |
Risk Factor Analysis
As shown in Table 3, three risk factors including inflammation score on screening ≥ 2, silicone oil as tamponade, and IOP on screening ≥ 30 mmHg had significant effects on increasing the number of IOP-lowering medications used in the 4-week follow-up. Other factors including sex, age, high myopia, diagnosis of macular diseases, combination with lens surgery, time of treatment initiation after vitrectomy, and travoprost versus timolol as the initial IOP-lowering medication have no significant impact. In our study, all patients without risk factors were treated using a single IOP-lowering medication. The rates of patients using more than one IOP-lowering medication were 18.52%, 36%, and 77.78% in patient with one, two, and three risk factors, respectively.
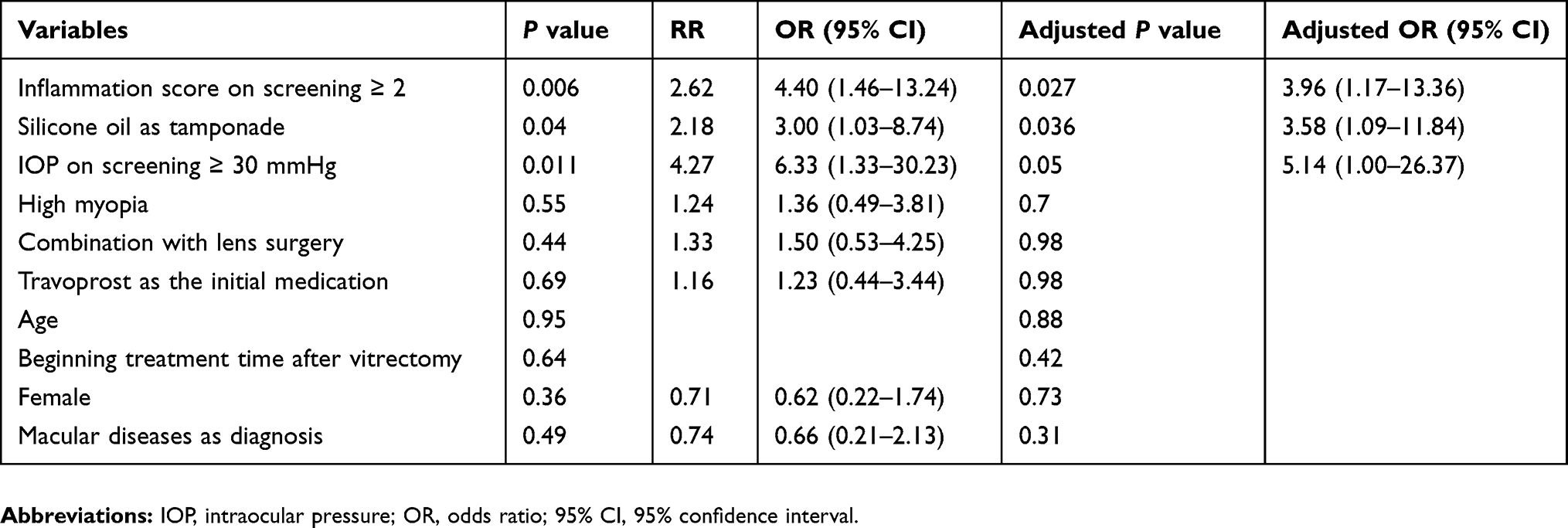 |
Table 3 Multivariate Analysis Of Factors Predicting Patient Needs More Than One IOP-Lowering Medication During 4 Weeks’ Follow-Up |
Discussion
Most patients with ocular hypertension after vitrectomy are medically treated,6 and PGAs have become the second most frequently used IOP-lowering medication for treating ocular hypertension secondary to vitrectomy, as discussed in a previous report.6 However, the efficacy of PGAs in eyes with ocular inflammation is still questioned. Markomichelakis et al reported a one-year, prospective randomized study involving 54 patients with uveitic glaucoma and found latanoprost to be equally effective as a fixed combination of dorzolamide and timolol.19 Fortuna et al reported a retrospective study including 42 patients (59 eyes) with uveitic glaucoma and found that bimatoprost therapy can decrease IOP from 27 ± 13.2 mmHg to 15 ± 5.5 mmHg (44.44% reduction) at the end of six months.21 Chang et al retrospectively compared 163 eyes with uveitis that had been treated with a PGA and found that PGAs significantly reduced IOP in uveitic glaucoma.22 Takeuchi et al reported a retrospective study involving 36 patients (55 eyes) with ocular hypertension associated with uveitis and found the rate of IOP reduction in the travoprost/timolol treated group (50.6%) to be higher than that in the latanoprost/timolol-treated group (37.1%).20 These studies suggest that PGAs have good efficacy in treating uveitic glaucoma in which uveitis is controlled through immunomodulatory therapy.
The mechanism of early-onset ocular hypertension is similar to that of uveitic glaucoma. Our study showed that travoprost 0.004% effectively reduces IOP in ocular hypertension secondary to vitrectomy. The rates of IOP reduction were 45.65% in the TRA-I-Group and 35.27% in the TIM-I-Group on day 1 (P = 0.006). At the follow-up visit on day 1, more patients in the TIM-I-Group than in the TRA-I-Group were advised to add IOP-lowering medications. Therefore, the number of IOP-lowering medications in the TIM-I-Group (1.32 ± 0.095, mean ± SE) was higher than that in the TRA-I-Group (1.17 ± 0.069) on day 7. However, IOP reduction in the TRA-I-Group decreased from −15.02 ± 0.97 mmHg on day 1 to −11.61 ± 1.27 mmHg on day 7. Consequently, the number of IOP-lowering medications in the TRA-I-Group increased from 1.17 ± 0.069 on day 7 to 1.41 ± 0.12 on day 14. On the contrary, the number in the TIM-I-Group on day 14 (1.33 ± 0.12) was similar to that on day 7 (1.32 ± 0.095), suggesting that the efficacy of travoprost decreased, while that of timolol was quite stable, from day 1 to 7. The decreased efficacy of travoprost for treatment of early-onset ocular hypertension secondary to vitrectomy from day 1 to day 7 is a novel finding. The mechanism behind it is still unknown and needs further investigation. The number of IOP-lowering medications was 0.64 ± 0.17 in the TIM-I-Group and 1.15 ± 0.18 in the TRA-I-Group on day 21, and the difference was significant (P = 0.038), suggesting better IOP control efficacy in the TIM-I-Group compared with the TRA-I-Group on day 21. The proportions of single IOP-lowering medication used during follow-up in the two groups were close (P = 0.692). We tested whether administering travoprost or timolol as the initial IOP-lowering medication affects the number of IOP-lowering medications using a logistic regression model and found the adjusted P value in this factor is 0.975. Overall, our results show that travoprost 0.004% doesn’t show a better efficacy that it presents in treating primary open angle glaucoma than timolol 0.5%,11,28 and that the two drugs have comparable efficacy for the treatment of early-onset ocular hypertension secondary to vitrectomy.
Prostaglandins are well-known mediators of ocular inflammation. Some studies reported that the use of prostaglandin analogs leads to anterior uveitis,12–14 macular edema,15 and reactivation of herpes simplex virus.16–18 However, Markomichelakis et al demonstrated that the proportion of uveitic glaucoma patients experiencing recurrences of anterior uveitis was 34% in the latanoprost group vs. 57% in the dorzolamide/timolol group (P = 0.21), while the proportion of patients developing macular edema was 13.3% in the latanoprost group and 17.9% in the dorzolamide/timolol group, indicating that latanoprost is safe in the treatment of uveitic glaucoma.19 Fortuna et al demonstrated that the rate of uveitis flares with the use of antiglaucoma therapies was 52 per 100 person-years of follow-up, and that with the use of bimatoprost therapy was 32.4 per 100 person-years of follow-up (P = 0.206).21 Takeuchi et al found that after fixed latanoprost/timolol and travoprost/timolol combination therapy, the inflammation score in eyes with uveitic glaucoma was improved in 7 eyes and unchanged in 48 eyes, with no eyes showing deterioration.20 Chang et al reported no difference in the frequency of reactivation of anterior uveitis in patients treated with PGAs versus other topical hypotensive agents.22 Taken together, these studies show that PGAs will not increase ocular inflammation in uveitic glaucoma in which uveitis is controlled through immunomodulatory therapy.
In our study, the inflammation scores in the TRA-I-Group slightly increased from day 0 to day 1 and decreased on day 7. Inflammation scores showed no significant differences between the TRA-I-Group and the TIM-I-Group at any time point, suggesting that in combination with anti-inflammation therapy through topical steroids, travoprost shows safety comparable to that of timolol. Because the observation of macular edema is obstructed by explosive gas or air filled in the vitreous as tamponades early after vitrectomy, we did not observe macular edema in this study. There was no case of reactivation of herpes simplex virus. However, the number of cases of increased ocular hyperemia was significantly more in the TRA-I-Group than in the TIM-I-Group, in agreement with other studies on primary open-angle glaucoma or ocular hypertension.28–30 The mechanism of hyperemia induced by PGAs is complex. PGAs were reported to have some affinity to the EP2 receptor, a receptor known to mediate vasodilation.31 Besides that, PGAs can induce the release of nitric oxide to mediate hyperemia.32
Through multivariate analysis, we found three risk factors of using more than one IOP-lowering medication including inflammation score ≥ 2, silicone oil as tamponade and IOP ≥ 30 mmHg. In addition, 77.78% of patients with three risk factors used more than one IOP-lowering medication in our study; this may be evidence for clinicians to consider treating patients with three risk factors using two IOP-lowering medications instead of a single IOP-medication at the beginning of treatment. This treatment strategy may improve IOP control in high-risk patients, thereby decreasing the risk of retinal and optic nerve damage caused by uncontrolled IOP. However, only 18.52% of patients with one risk factor and no patient without risk factor used more than one IOP-lowering medication in our study, suggesting that patients with less than two risk factors may not need to use more than one IOP-lowering medication at the beginning of treatment. This regimen may avoid the overuse of eye drops in low-risk patients, reduce their economic burden, and benefit their eye surface health.
Our study has several limitations, and our results should be interpreted with caution. The baseline inflammation score of patients in our study was 1.32, which is not a high value, so ocular inflammation was easily controlled with topical steroids. Moreover, our study excluded patients affected by the closed-angle subtype; these patients may respond differently to travoprost.
In conclusion, we found that efficacy and safety of travoprost 0.004% were similar to those of timolol 0.5% in the treatment of early-stage ocular hypertension secondary to vitrectomy. Travoprost 0.004% may be effective for treating early-onset ocular hypertension secondary to vitrectomy while controlling inflammation. However, with a higher risk of ocular hyperemia, beta-blockers remain the first choice IOP-lowering medication for treating early-onset ocular hypertension secondary to vitrectomy.
Data Sharing Statement
The individual participant’s data underlying published results reported in this study can be accessed with approval from the corresponding author after 6 months of publication of the main results. The study protocol, statistical analysis plan, and clinical study report will also be available.
Author Contributions
All authors contributed to data analysis, drafted or revised the article, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest with this work.
References
1. Weinberg RS, Peyman GA, Huamonte FU. Elevation of intraocular pressure after pars plana vitrectomy. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1976;200(2):157–161. doi:10.1007/BF00414365
2. Faulbom J, Conway BP, Machemer R. Surgical complications of pars plana vitreous surgery. Ophthalmology. 1978;85(2):116–125. doi:10.1016/S0161-6420(78)35684-0
3. Antoun J, Azar G, Jabbour E, et al. Vitreoretinal surgery with silicone oil tamponade in primary uncomplicated rhegmatogenous retinal detachment. Retina. 2016;36(10):1906–1912. doi:10.1097/IAE.0000000000001008
4. Jonas JB, Knorr HL, Rank RM, Budde WM. Intraocular pressure and silicone oil endotamponade. J Glaucoma. 2001;10(2):102–108. doi:10.1097/00061198-200104000-00006
5. Fang Y, Long Q, Wang X, Jiang R, Sun X. Intraocular pressure 1 year after vitrectomy in eyes without a history of glaucoma or ocular hypertension. Clin Ophthalmol. 2017;11:2091–2097. eCollection 2017. doi:10.2147/OPTH.S144985
6. Al-Jazzaf AM, Netland PA, Charles S. Incidence and management of elevated intraocular pressure after silicone oil injection. J Glaucoma. 2005;14(1):40–46.
7. Mangouritsas G, Mourtzoukos S, Portaliou DM, Georgopoulos VI, Dimopoulou A, Feretis E. Glaucoma associated with the management of rhegmatogenous retinal detachment. Clin Ophthalmol. 2013;7:727–734. doi:10.2147/OPTH.S42792
8. Hathout RM, Gad HA, Abdel-Hafez SM, et al. Gelatinized core liposomes: a new Trojan horse for the development of a novel timolol maleate glaucoma medication. Int J Pharm. 2019;556:192–199. doi:10.1016/j.ijpharm.2018.12.015
9. Shokry M, Hathout RM, Mansour S. Exploring gelatin nanoparticles as novel nanocarriers for Timolol Maleate: augmented in-vivo efficacy and safe histological profile. Int J Pharm. 2018;545(1–2):229–239. doi:10.1016/j.ijpharm.2018.04.059
10. American Academy of Ophthalmology. Primary Open-Angle Glaucoma Preferred Practice Patterns. San Francisco: American Academy of Ophthalmology; 2010. Available from: http://one.aao.org/preferred-practice-pattern/primary-openangle-glaucoma-ppp-october-2010.
11. Li T, Lindsley K, Rouse B, et al. Comparative effectiveness of first-line medications for primary open-angle glaucoma: a systematic review and network meta-analysis. Ophthalmology. 2016;123(1):129–140. doi:10.1016/j.ophtha.2015.09.005
12. Fechtner RD, Khouri AS, Zimmerman TJ, et al. Anterior uveitis associated with latanoprost. Am J Ophthalmol. 1998;126:37–41. doi:10.1016/S0002-9394(98)00071-3
13. Ornek K, Onaran Z, Turgut Y. Anterior uveitis associated with fixed-combination latanoprost and timolol. Can J Ophthalmol. 2008;43:727–728. doi:10.3129/i08-113
14. Smith SL, Pruitt CA, Sine CS, Hudgins AC, Stewart WC. Latanoprost 0.005% and anterior segment uveitis. Acta Ophthalmol Scand. 1999;77:668–672. doi:10.1034/j.1600-0420.1999.770612.x
15. Warwar RE, Bullock JD, Ballal D. Cystoid macular edema and anterior uveitis associated with latanoprost use: experience and incidence in a retrospective review of 94 patients. Ophthalmology. 1998;105:263–268. doi:10.1016/S0161-6420(98)92977-3
16. Wand M, Gilbert CM, Liesegang TJ. Latanoprost and herpes simplex keratitis. Am J Ophthalmol. 1999;127:602. doi:10.1016/S0002-9394(99)00050-1
17. Kroll DM, Schuman JS. Reactivation of herpes simplex viruskeratitis after initiating bimatoprost treatment for glaucoma. Am J Ophthalmol. 2002;133:401–403. doi:10.1016/S0002-9394(01)01360-5
18. Gordon YJ, Yates KA, Mah FS, Romanowski EG. The effects of Xalatan on the recovery of ocular herpes simplex virus type 1 (HSV-1) in the induced reactivation and spontaneous shedding rabbit models. J Ocul Pharmacol Ther. 2003;19(3):233–245. doi:10.1089/108076803321908356
19. Markomichelakis NN, Kostakou A, Halkiadakis I, Chalkidou S, Papakonstantinou D, Georgopoulos G. Efficacy and safety of latanoprost in eyes with uveitic glaucoma. Graefes Arch Clin Exp Ophthalmol. 2009;247(6):775–780. doi:10.1007/s00417-009-1036-3
20. Takeuchi M, Kanda T, Taguchi M, Shibata M, Mine I, Sakurai Y. Evaluation of efficacy and safety of latanoprost/timolol versus travoprost/timolol fixed combinations for ocular hypertension associated with uveitis. Ocul Immunol Inflamm. 2017;25(1):105–110. doi:10.3109/09273948.2015.1092559
21. Fortuna E, Cervantes-Castañeda RA, Bhat P, Doctor P, Foster CS. Flare-up rates with bimatoprost therapy in uveitic glaucoma. Am J Ophthalmol. 2008;146(6):876–882. doi:10.1016/j.ajo.2008.08.022
22. Chang JH, McCluskey P, Missotten T, Ferrante P, Jalaludin B, Lightman S. Use of ocular hypotensive prostaglandin analogues in patients with uveitis: does their use increase anterior uveitis and cystoid macular oedema? Br J Ophthalmol. 2008;92(7):916–921. doi:10.1136/bjo.2007.131037
23. Fang Y, Ku H, Liu Y, Gan D. Trends in the characteristics of vitrectomy in Eastern China. Clin Ophthalmol. 2018;12:1993–2000. doi:10.2147/OPTH.S173251
24. Nussenblatt RB, Palestine AG, Chan CC, Roberge F. Standardization of vitreal inflammatory activity in intermediate and posterior uveitis. Ophthalmology. 1985;92:467–471. doi:10.1016/S0161-6420(85)34001-0
25. Koreen L, Yoshida N, Escariao P, Niziol LM, Koreen IV, Musch DC. Incidence of, risk factors for, and combined mechanism of late-onset open-angle glaucoma after vitrectomy. Retina. 2012;32(1):160–167. doi:10.1097/IAE.0b013e318217fffb
26. Muether PS, Hoerster R, Kirchhof B, Fauser S. Course of intraocular pressure after vitreoretinal surgery: is early postoperative intraocular pressure elevation predictable? Retina. 2011;31(8):1545–1552. doi:10.1097/IAE.0b013e31820f4b05
27. Gupta D, Chen PP. Glaucoma. Am Fam Physician. 2016;93(8):668–674.
28. Netland PA, Landry T, Sullivan EK, et al., Travoprost Study Group. Travoprost compared with latanoprost and timolol in patients with open-angle glaucoma or ocular hypertension. Am J Ophthalmol. 2001;132(4):472–484. doi:10.1016/s0002-9394(01)01177-1.
29. Watson P, Stjernschantz J. A six-month, randomized, double-masked study comparing latanoprost with timolol in open-angle glaucoma and ocular hypertension. The Latanoprost Study Group. Ophthalmology. 1996;103(1):126–137. doi:10.1016/s0161-6420(96)30750-1
30. Li F, Huang W, Zhang X. Efficacy and safety of different regimens for primary open-angle glaucoma or ocular hypertension: a systematic review and network meta-analysis. Acta Ophthalmol. 2018;96(3):e277–e284. doi:10.1111/aos.13568
31. Alm A, Grierson I, Shields MB. Side effects associated with prostaglandin analog therapy. Surv Ophthalmol. 2008;53 Suppl1:S93–S105. doi:10.1016/j.survophthal.2008.08.004
32. Astin M, Stjernschantz J, Sele´n G. Role of nitric oxide in PGF2 alpha-induced ocular hyperemia. Exp Eye Res. 1994;59:401–407. doi:10.1006/exer.1994.1124
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.