")
Back to Journals » Drug Design, Development and Therapy » Volume 9
Effect of oral N-acetylcysteine on COPD patients with microsatellite polymorphism in the heme oxygenase-1 gene promoter
Authors Zhang J , Zhang J , Fang L , Liu L, Fu W, Dai L
Received 5 July 2015
Accepted for publication 13 October 2015
Published 7 December 2015 Volume 2015:9 Pages 6379—6387
DOI https://doi.org/10.2147/DDDT.S91823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Wei Duan
Jia-Qiang Zhang, Jian-Qing Zhang, Li-Zhou Fang, Ling Liu, Wei-Ping Fu, Lu-Ming Dai
The Second Department of Respiratory Medicine, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China
Background: Heme oxygenase-1 (HO-1) plays a protective role as an antioxidant in the lung, and HO-1 gene promoter polymorphism has been shown to be associated with the severity and prognosis of COPD patients. N-acetylcysteine (NAC), an antioxidant/mucous modifier, has shown an uncertain benefit in COPD patients. We hypothesized that this polymorphism could be associated with the effectiveness of oral NAC.
Methods: A total of 368 patients with COPD were recruited and the polymorphisms of their HO-1 gene promoter were classified into three subclasses according to the number of (GT)n repeats, as previously reported: class S (<27 (GT)n repeats), class M (27–32 (GT)n repeats), and class L (>32 (GT)n repeats). These subjects were then classified as L+ group (with the L allele: L/L, L/M, L/S) and L- group (without the L allele: M/M, M/S, S/S). All the patients were allocated to standard therapy plus NAC 600 mg bid over a 1-year period and were observed over that year.
Results: The L- group saw improvements in forced expiratory volume in 1 second (FEV1) (from 1.44±0.37 to 1.58±0.38, P=0.04) and FEV1% predicted (from 56.6±19.2 to 59.7±17.2, P=0.03). No improvement was found in forced vital capacity of each group and the decline of forced vital capacity in both of the groups was not statistical significant. The number of yearly COPD exacerbations of the L- group was 1.5±0.66 which was lower than the 2.1±0.53 of the L+ group (P<0.01). For the changes of St George’s Respiratory Questionnaire (SGRQ) score, only the activity score of the L- group was more significant than that of the L+ group (P=0.02). The improvement of the outcome of 6-minute walking distance test in L- group (from 290.1±44.9 meters to 309.7±46.9 m) was higher than that in the L+ group (from 289.7±46.2 m to 300.3±44.2 m) (P=0.03).
Conclusion: A 600 mg bid oral NAC treatment for 1-year on COPD patients without the L allele can improve the FEV1, FEV1% predicted, the SGRQ activity score, and the result of 6-minute walking distance test, and the exacerbation rate of the L allele carrier in COPD patients is much higher than in the COPD patients without the L allele.
Keywords: chronic obstructive pulmonary disease, COPD prognosis, NAC treatment, gene therapy
Introduction
COPD is a major public health problem. In 2020, COPD is projected to rank fifth worldwide in terms of burden of disease and third in terms of mortality.1 COPD is an inflammatory disease, and lung and systemic inflammation intensifies during most COPD exacerbations.2 In COPD, repeated exposure to noxious particles, usually tobacco smoke, can trigger a distinct inflammatory cascade in the small airways and lung parenchyma involving several different cell types and inflammatory mediators.3 So, reducing oxidative stress and airway inflammation is supposed to be effective in the treatment of COPD. Those inflammatory mediators mentioned earlier have become a hot topic in the study and treatment of COPD in recent years. Many of them are defined as proinflammation cytokines but the network of those cytokines is still not very clear.4 Their role in the inflammation progress has been accepted. In the past few decades, researchers mainly focused on the development of antibodies to block the cytokine or its receptor,5–7 and less focused on targeting intracellular signaling pathways. As a result, cytokine inhibitors have produced disappointing results in patients with COPD.8
N-Acetylcysteine (NAC), an antioxidant/mucous modifier, has shown an uncertain benefit in COPD patients for decades. A number of clinical trials and system reviews have shown that NAC reduces the risk of rehospitalization for COPD and that this risk reduction maybe dose-dependent.9–12 Several recently published reports,13–17 using different monitors such as: inspiratory capacity, forced vital capacity (FVC), forced expiratory flow 25%–75%, and functional residual capacity, have found out that NAC can improve the lung function of COPD patients to different degrees. The traditional view of the precise way the drug works is that NAC increases intracellular reduced glutathione in the lungs and neutralizes oxidant species and also NAC is an effective mucolytic agent as it reduces sulfhydryl moieties to affect the disruption of disulfide bridges within the glycoprotein matrix of mucus.18 However, we may have underestimated the clinical utility of NAC as more recent researches suggest that NAC will affect COPD patients in many aspects from symptoms to prognosis.19 In addition, the molecular pathways of NAC are still not very clear. The different consequences of these clinical studies of NAC are partly due to the different evaluation criteria of lung function and outcomes, but we think that the different genetic backgrounds and gene polymorphism should also be taken into account. HO-1, one of the isoforms of heme oxygenase enzyme, is traditionally thought to be a fundamental “sensor” of cellular stress and directly contributes toward limiting or preventing tissue damage.20 Recent researches that focused on the signaling function of HO-1 indicate that HO-1 is a pleiotropic protein with multiple roles, including a heme degradation function leading to the formation of antioxidant bile pigments and the important signaling gas CO as well as a nonenzymatic signaling function, resulting in the regulation of gene expression, modulation of protein translation, and binding to DNA repair proteins.21 In the last couple of years, several researches have emphasized on the polymorphism of HO-1 gene and its promoter. Yamada et al22 first demonstrated that the large size of 5′-flanking polymorphism ((GT)n repeat number) in the HO-1 gene was associated with chronic pulmonary emphysema susceptibility caused by cigarette smoke in Japanese patients. A similar study conducted in the Japanese population also suggests that polymorphism of the HO-1 promoter gene may be associated with the rate of decline in lung function in Japanese male ex-smokers.23 The results of a multicenter two-stage study named European Community Respiratory Health Survey suggest that a long HO-1 gene promoter, which may lead to low protein expression and activity, is associated with low lung function and accelerated lung function decline, especially in heavy smokers.24 In our previous published study,25 we provided genotyping data of HO-1 gene in southwest Chinese population and the result of the study suggested a strong association between the (GT)n repeat number in the Hox-1 gene promoter and susceptible to COPD in southwest Chinese smokers. But there are still different opinions. No association was found between HO-1 (GT)n alleles and the rate of decline in lung function in smokers in the north American population according to the studies conducted by Tanaka et al26 and the National Heart, Lung, and Blood Institute Lung Health Study of Canada.27 Despite the different sample size of these studies, the discrepant results also attributed to the different distribution of (GT)n repeat in subjects from different population and region. We hypothesized that this polymorphism of HO-1 gene promoter could be associated with the effectiveness of oral NAC. This study was conducted to explore whether the effect of the NAC treatment would vary or not when applied to COPD patients with different length of (GT)n repeat in the HO-1 gene promoter. To our knowledge, there is no related report.
Materials and methods
This study received ethics approval from the Ethics Committee of Kunming Medical University and all aspects of the experiments were performed according to the guidelines of the ethics committee. All of the patients involved in the study provided written informed consent.
Study population
Patients with COPD attending the Second Department of Respiratory of the First Affiliated Hospital of Kunming Medical University were recruited. COPD was diagnosed in accordance with Global Initiative of Obstructive Lung Disease 2011. All patients were from southwest Chinese Han population and ex-smokers since at least 1 year, with a smoking history of at least 10 pack-years, but they were clinically stable for at least 4 weeks prior to the present study. Other criteria were forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) <70% and physician diagnosis of COPD with compatible symptoms, such as cough, dyspnea, etc. Patients were excluded in the following situations: a history of asthma, lung surgery, oral steroids, any other antioxidant supplements, and respiratory tract infection that needed antibiotics.
DNA genotyping
Genomic DNAs were extracted from peripheral venous blood leucocytes using the QIAamp DNA Blood Mini Kit (Qiagen NV, Venlo, the Netherlands). The (GT)n repeat polymorphism was amplified by polymerase chain reaction (PCR) using the forward primer 5′-ACG CCT GGG GTG CAT CAA GTC-3′ and the reverse primer 5′-GTG GGG TGG AGA GGA GCA GTC ATA-3′, which were designed according to the published sequence in our previous study.25 PCR was performed over 30 cycles of 20 seconds at 94°C, 10 seconds at 60°C, and 20 seconds at 72°C using a fluorescently labeled deoxycytidine triphosphate (Applied Biosystems Inc., Waltham, MA, USA) as described by the manufacturer’s protocol. The PCR products were electrophoresed on a denaturing polyacrylamide gel using ABI PRISM 377 sequencer (Applied Biosystems Inc.). The results were analyzed with DNASTAR.Lasergene v7.1 (DNAStar Inc., Madison, WI, USA) software package.
Study protocol
The polymorphisms of the Hox-1 gene promoter were classified into three subclasses according to the number of (GT)n repeats25: class S (<25 (GT)n repeats), class M (26–31 (GT)n repeats), and class L (≥32 (GT)n repeats). These subjects were then classified as having L/L, L/M, L/S, M/M, M/S, or S/S genotypes. Eligible patients were allocated to either the L+ group (patients genotyped as L/L, L/M, L/S) or the L− group (patients genotyped as M/M, M/S, S/S) based on the different genotypes of with or without L allele. Once enrolled in this research, each patient was allocated to NAC 600 mg bid (Hainan Zambon Pharmaceutical, Haikou, People’s Republic of China) over a 1-year period. There were four visits: the baseline and the following time points of every 16 weeks until the end of the trial. The study design is illustrated in Figure 1.
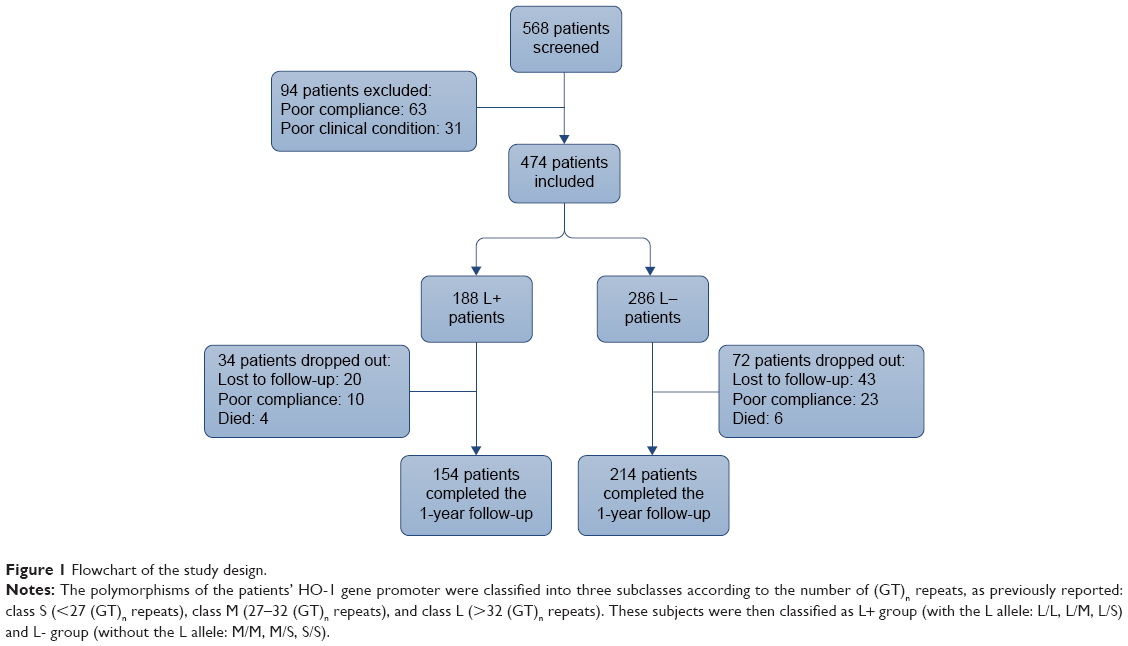 | Figure 1 Flowchart of the study design. |
Outcome measures
Once included, patients’ basic characteristics were recorded by questionnaire. Every patient completed the Chinese version of St George’s Respiratory Questionnaire (SGRQ) at each follow-up visit and meanwhile the 6-minute walking distance (6MWD) test was also conducted and recorded. Lung function testing was conducted by Cosmed Pony FX portable pulmotester (COSMED, Rome, Italy) for the following parameters: FEV1, FEV1% predicted, and FVC. The COPD exacerbation rate (per year) was defined as having the following symptoms: an increase in cough, purulence of sputum, or dyspnea, necessitating of a change in regular medication in a patient such as: using antibiotics and (or) oral corticosteroid, or hospitalizations to emergency room or a respiratory clinic. Adverse events were recorded at each study visit.
Statistical methods
The study was designed to enroll at least a total of 340 subjects to achieve 80% power to detect the genetic association of oral NAC and COPD. The SPSS Version 21.0 (SPSS Inc., Chicago, IL, USA) software was used in the statistical analysis of this study. Data were expressed as mean ± standard deviation, unless otherwise stated.
The frequencies of Hox-1 gene promoter genotypes between different groups were compared by two-tailed chi-square test. The baseline differences of enumeration data between the two groups (such as age, smoking index, FEV1% predicted, and FEV1/FVC) were compared with unpaired t-test, and measurement data (such as sex) were compared with chi-square test. P<0.05 was taken as statistically significant. Data in different group of each measurement time were compared pairwise with multivariate analysis of variance.
Results
Study population and baseline characteristics
Of 568 eligible patients with COPD who were screened, 94 were excluded in the run-in period: 28 subjects withdrew consent, 24 were lost to follow-up, eleven refused lung function testing or 6MWD, and 31 could not finish a receivable lung function test or 6MWD due to poor clinical condition. During the 1-year follow-up, 106 subjects out of the remaining 474 subjects dropped out the study for lost follow-up, poor compliance, or death and 368 patients completed the study (Figure 1). The baseline characteristics of the population studied are shown in Table 1 and there were no significant differences between groups at the baseline. The number of (GT)n repeats in the HO-1 gene promoter ranged from eleven to 39. In the total population, the distribution of (GT)n repeat peaks were at 22 and 30 GT repeats (Figure 2).
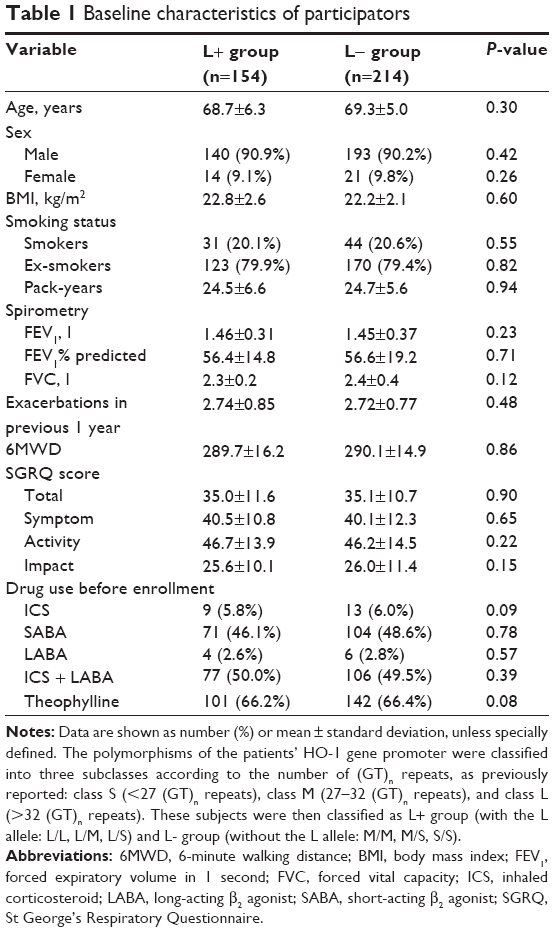 | Table 1 Baseline characteristics of participators |
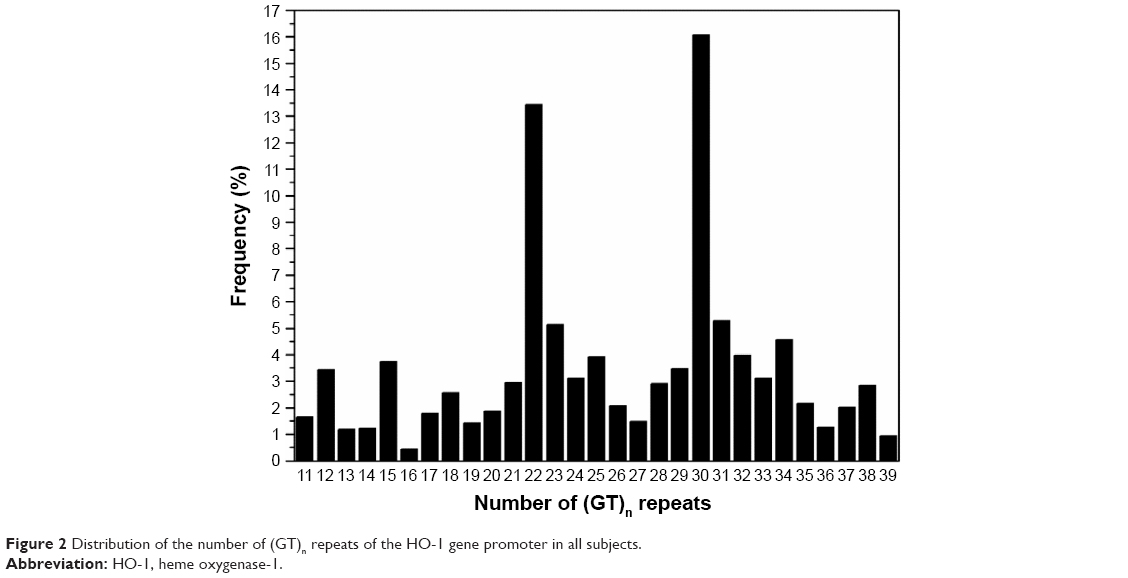 | Figure 2 Distribution of the number of (GT)n repeats of the HO-1 gene promoter in all subjects. |
Follow-up visit
Lung function test
The improvements in FEV1 (from 1.44±0.37 to 1.58±0.38, P=0.04) and FEV1% predicted (from 56.6±19.2 to 59.7±17.2, P=0.03) of the L− group were significant after the study, while there were no significant differences for changes of FEV1 and FEV1% predicted in the L+ group (Figures 3 and 4; Table 2). There was no improvement in FVC of each group and the decline of FVC in both of the groups was not statistical significant (Table 2).
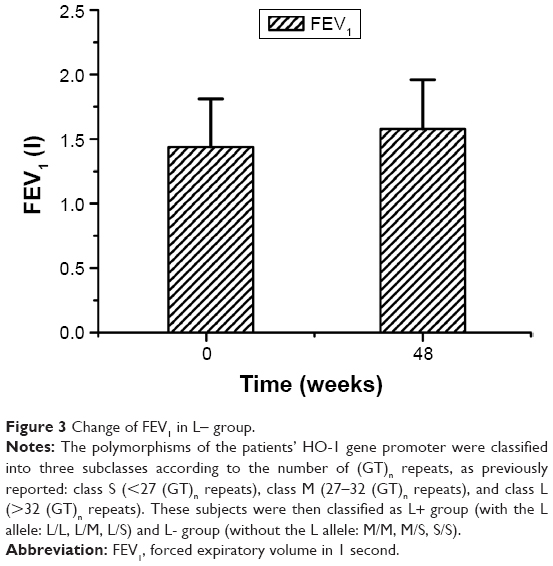 | Figure 3 Change of FEV1 in L− group. |
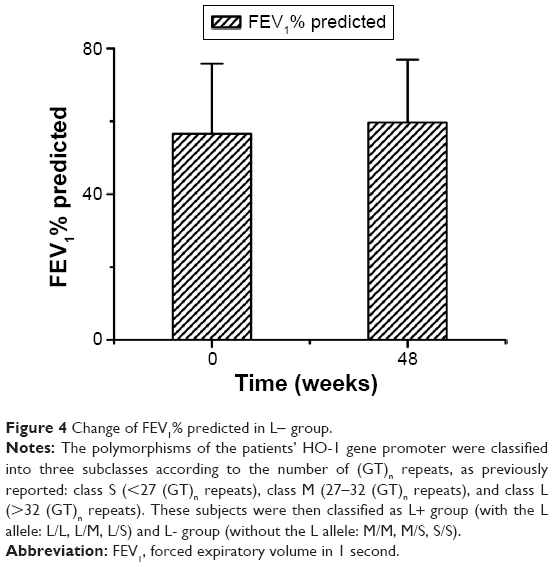 | Figure 4 Change of FEV1% predicted in L− group. |
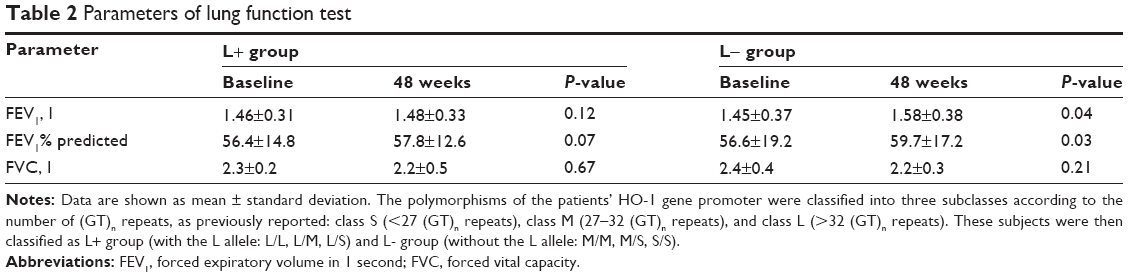 | Table 2 Parameters of lung function test |
Exacerbation rate
The total number of COPD exacerbations recorded during the 1-year follow-up was 176 (92 in L+ group and 84 in L− group). The rate of patients which had one or more COPD exacerbations of the L+ group and L− group were significantly different (40.3% vs 25.2%) (P=0.01) (Figure 5). The number of yearly COPD exacerbations of the L− group was 1.5±0.66, which was significantly lower than the 2.1±0.53 of the L+ group (P<0.01).
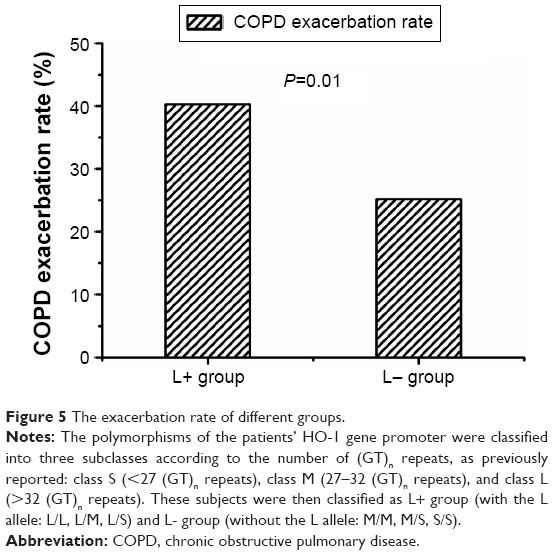 | Figure 5 The exacerbation rate of different groups. |
SGRQ score and 6MWD test
The changes of SGRQ score and 6MWD test of each visit in different groups are shown in Table 3. There was no significant differences in the changes of SGRQ total score (P=0.08), impact score (P=0.1), or symptom score (P=0.06) of the two groups after 1-year follow-up. But the change of activity score of the L− group was more significant than that of the L+ group (P=0.02) (Figure 6). During the 1-year follow-up, there was an improvement of the outcome of 6MWD test in both groups, but the improvement of the outcome of 6MWD test in L− group (from 290.1±44.9 to 309.7±46.9 m) was significantly higher than that in the L+ group (from 289.7±46.2 to 300.3±44.2 m) (P=0.03) (Figure 7).
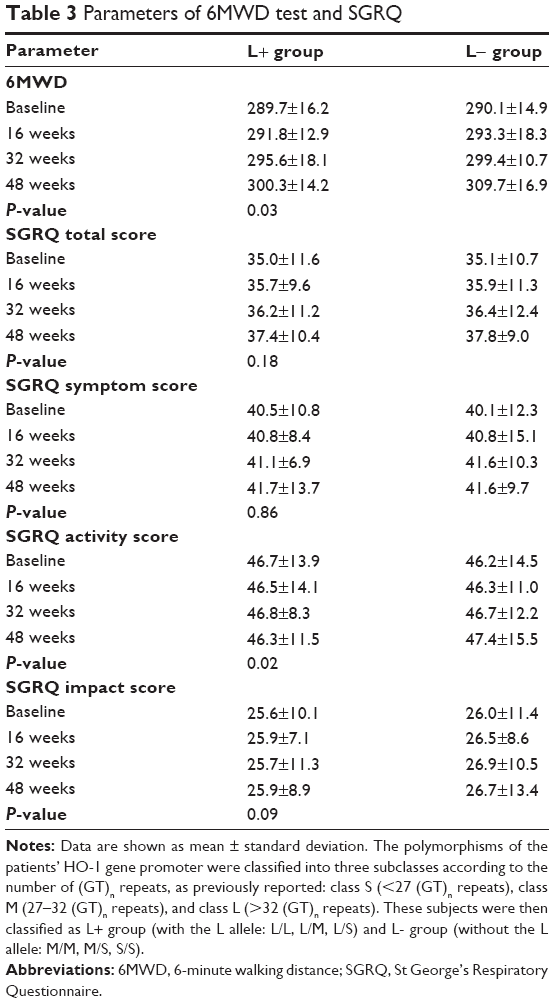 | Table 3 Parameters of 6MWD test and SGRQ |
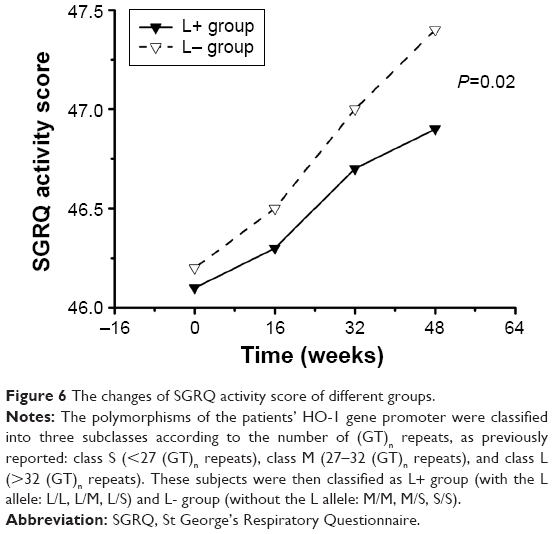 | Figure 6 The changes of SGRQ activity score of different groups. |
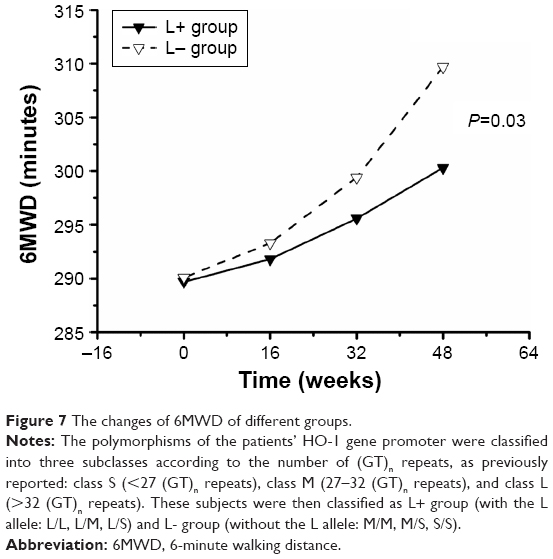 | Figure 7 The changes of 6MWD of different groups. |
Adverse effects
Twenty-three patients reported gastrointestinal complaints (eight in the L+ group and 15 in the L− group) and no other major adverse event occurred in both groups. Ten patients died during the study, including four patients in the L+ group (three from acute exacerbations of COPD, one from pneumonia) and six patients in the L− group (three from acute exacerbations of COPD, one from pneumonia, one from acute renal failure, and one from acute ischemic stroke). No deaths were regarded by investigators as related to the study products.
Discussion
The present study conducted in the southwest population of the People’s Republic of China showed that the use of NAC (600 mg bid for 1 year) improved the FEV1 and FEV1% predicted of COPD patients without L allele. In the study by Pela et al, a small but significant improvement in FEV1 and maximal expiratory flow 50 was found in COPD patients with 600 mg NAC once a day compared with COPD patients without NAC.28 However, many large, multicenter studies, such as the BRONCUS,10 PEACE,29 ECRSH,24 and PANTHEON17 which used FEV1 as the outcome parameter of lung function found no significant improvement of the FEV1 or prevention of FEV1 reduction rate between the NAC group and the control group. In spite of this, a subgroup analysis of the study of BRONCUS10 mentioned above showed a significant reduction in hyperinflation in COPD patients. In the study such as HIACE,15 the forced expiratory flow 25%–75% and resonance frequency, frequency dependency, and reactance and resistance at low oscillation frequency (X6 Hz and R6 Hz) were used as the outcome parameters of lung function and they found out that NAC had a beneficial role in small airway function as well as in reduction of lung hyperinflation in patients with COPD. The result of these different trials may be due to the different dose of NAC treatment and the different lung function parameters in use. In our present study, we took the gene polymorphism into account and grouped the COPD patients by the different microsatellite polymorphism in the HO-1 gene promoter and that may have attributed to the different outcome of our study.
The possible mechanism of NAC on the expression of HO-1 gene and the small airway function is still not very clear. Many in vivo and in vitro factors are involved in the pathological process of emphysema, the mucus hypersecretion as a prominent factor in airway can directly aggravate the small air trapping. As defined as a chronic inflammatory disease, the airway remodeling of COPD is strongly related to the disequilibrium of oxidation and antioxidation in airway. Both NAC and HO-1 have been mistaken for single mucus modifier or antioxidant for a long time until recent decades, the former had been proved to be not only mucous modifier, but also antioxidant. But as a classical enzyme in the redox system, there are not so many studies emphasized on the relation between HO-1 and the mucus secretion. Almolki et al30 assessed the relationship between the expression of the HO-1 and the airway mucus secretion in cigarette smoke-exposed Sprague Dawley rats and found the expression of HO-1 had a strong affection on several enzymes (EGF-R, MUC5AC, DUOX1/NADPH oxidase, TGF-α), which were involved in the airway mucus secretion pathway. A secondary analysis was also made in the same study using the data from the multicenter longitudinal European Community Respiratory Health Survey24 to evaluate the relation between HO-1 gene promoter polymorphism (the same grouping strategy of L+ and L− group as the present study) and chronic sputum prevalence in smokers. We can infer from the result of this study that HO-1 do have a significant protective effect against airway mucus hypersecretion in both Sprague Dawley rats and smokers.
Unlike the outcome of lung function, more studies drew the same conclusion on the positive effect of NAC in the prevention of COPD exacerbations. On one hand, the bacteria play a very important role in COPD exacerbations, so the hypersecretion state in the airway may stimulate the colonization of bacteria and influence the susceptibility of COPD patients to exacerbations. On the other hand, NAC as an antioxidant can increase the resistance against acute oxidative stress by providing cysteine extracellularly for the enhanced production of glutathione.9 The present study demonstrates that the 5′-flanking polymorphism in the HO-1 gene promoter is associated with the exacerbation rate of COPD patients and the exacerbation rate of COPD is much lower in the patients without the L allele. The NAC may sharpen the different expression of HO-1 in patients with different polymorphism in the HO-1 gene promoter. In consequence, the low content of HO-1 may have an adverse effect on the natural synergy of NAC and HO-1.
Although NAC may have a beneficial effect in reducing COPD exacerbations, the role of improving symptoms and quality of life is still not clear in COPD patients. In the prior BRONCUS10 trial, NAC (600 mg daily) did not improve results on the SGRQ over a 3-year period. In contrast, result of the recently published PANTHEON17 study showed that the mean SGRQ symptom scores were reduced in the NAC group compared with placebo, but did not differ in total score and other domains, which was consistent with PEACE29 study. According to the authors of those studies, different dose of NAC, sample from different ethnic origins, or the length of treatment times may be the causes of different results. The SGRQ activity score along with the result of 6MWD test were significantly improved in the L− group in our present study. But beyond all those reasons above, the different grouping method should also be taken into account.
Conclusion
A 600 mg bid oral NAC treatment for 1 year has different effect in COPD patients with different genotypes. For COPD patients without the L allele, NAC can significantly improve the FEV1, FEV1% predicted, the SGRQ activity score, and the result of 6MWD test and the exacerbation rate of the L allele carrier in COPD patients is much higher than the COPD patients without the L allele. These differences could be due to the complex molecular interactions between NAC and the HO-1 or its gene promoter. A clearer understanding of these differences will allow practitioners to choose the optimal therapy in different conditions. To understand the relationship between NAC and the modification of the HO-1 expression, we still need to do more researches in COPD genetics that will integrate multiple genomic types in order to build a model to understand the complex molecular interactions involved in COPD pathogenesis.
Acknowledgment
This study was funded by the Science and Technology Committee of Yunnan Province (2005NG07), Chinese Academy of Sciences, and National Natural Science Foundation of China (NSFC: 81160006).
Author contributions
All authors contributed toward data analysis, drafting and revising the paper, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187:347–365. | ||
Kirkham PA, Barnes PJ. Oxidative stress in COPD. Chest. 2013;144(1):266–273. | ||
Sethi S, Mahler DA, Marcus P, Owen CA, Yawn B, Rennard S. Inflammation in COPD: implications for management. Am J Med. 2012;125:1162–1170. | ||
European Innovation Partnership on A, Healthy Ageing APB, Mechanisms of the Development of Allergy WP, et al. Integrated care pathways for airway diseases (AIRWAYS-ICPs). Eur Respir J. 2014;44:304–323. | ||
Gronke L, Beeh KM, Cameron R, et al. Effect of the oral leukotriene B4 receptor antagonist LTB019 on inflammatory sputum markers in patients with chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2008;21:409–417. | ||
Vlahos R, Bozinovski S, Chan SP, et al. Neutralizing granulocyte/macrophage colony-stimulating factor inhibits cigarette smoke-induced lung inflammation. Am J Respir Crit Care Med. 2010;182:34–40. | ||
Woodruff PG, Albert RK, Bailey WC, et al. Randomized trial of zileuton for treatment of COPD exacerbations requiring hospitalization. COPD. 2011;8:21–29. | ||
Dunn LL, Midwinter RG, Ni J, Hamid HA, Parish CR, Stocker R. New insights into intracellular locations and functions of heme oxygenase-1. Antioxid Redox Signal. 2014;20:1723–1742. | ||
Gerrits CMJM, Herings RMC, Leufkens HGM, Lammers JW. N-Acetylcysteine reduces the risk of re-hospitalisation among patients with chronic obstructive pulmonary disease. Eur Respir J. 2003;21:795–798. | ||
Decramer M, Rutten-van Mölken M, Dekhuijzen PNR, et al. Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost-Utility Study, BRONCUS): a randomised placebo-controlled trial. Lancet. 2005;365:1552–1560. | ||
Sutherland ER, Crapo JD, Bowler RP. N-Acetylcysteine and exacerbations of chronic obstructive pulmonary disease. COPD. 2006;3:195–202. | ||
Shen Y, Cai W, Lei S, Zhang Z. Effect of high/low dose N-acetylcysteine on chronic obstructive pulmonary disease: a systematic review and meta-analysis. COPD. 2014;11(3):351–358. | ||
Stav D, Raz M. Effect of N-acetylcysteine on air trapping in COPD. Chest. 2009;136(2):381–386. | ||
De Backer J, Vos W, Van Holsbeke C, et al. Effect of high-dose N-acetylcysteine on airway geometry, inflammation, and oxidative stress in COPD patients. Int J Chron Obstruct Pulmon Dis. 2013;8:569–579. | ||
Tse HN, Raiteri L, Wong KY, et al. High-dose N-acetylcysteine in stable COPD. Chest. 2013;144(1):106–118. | ||
Sinojia R, Shaikh M, Kodgule R, et al. Priming of beta-2 agonist and antimuscarinic induced physiological responses induced by 1200 mg/day NAC in moderate to severe COPD patients: a pilot study. Respir Physiol Neurobiol. 2014;191:52–59. | ||
Zheng JP, Wen FQ, Bai CX, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med. 2014;2(3):187–194. | ||
Rushworth GF, Megson IL. Existing and potential therapeutic uses for N-acetylcysteine: the need for conversion to intracellular glutathione for antioxidant benefits. Pharmacol Ther. 2014;141(2):150–159. | ||
Tse HN, Tseng CZ. Update on the pathological processes, molecular biology, and clinical utility of N-acetylcysteine in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:825–836. | ||
Motterlini R, Foresti R. Heme oxygenase-1 as a target for drug discovery. Antioxid Redox Signal. 2014;20(11):1810–1826. | ||
Dennery PA. Signaling function of heme oxygenase proteins. Antioxid Redox Signal. 2014;20(11):1743–1753. | ||
Yamada N, Yamaya M, Okinaga S, et al. Microsatellite polymorphism in the heme oxygenase-1 gene promoter is associated with susceptibility to emphysema. Am J Hum Genet. 2000;66(1):187–195. | ||
Nakayama K, Kikuchi A, Yasuda H, et al. Heme oxygenase-1 gene promoter polymorphism and decline in lung function in Japanese men. Thorax. 2006;61(10):921. | ||
Guénégou A, Leynaert B, Bénessiano J, et al. Association of lung function decline with the heme oxygenase-1 gene promoter microsatellite polymorphism in a general population sample. Results from the European Community Respiratory Health Survey (ECRHS), France. J Med Genet. 2006;43:e43. | ||
Fu WP, Sun C, Dai LM, Yang LF, Zhang YP. Relationship between COPD and polymorphisms of HOX-1 and mEPH in a Chinese population. Oncol Rep. 2007;17(2):483–488. | ||
Tanaka G, Aminuddin F, Akhabir L, et al. Effect of heme oxygenase-1 polymorphisms on lung function and gene expression. BMC Med Genet. 2011;12:117. | ||
He JQ, Ruan J, Connett JE, Anthonisen NR, Paré PD, Sandford AJ. Antioxidant gene polymorphisms and susceptibility to a rapid decline in lung function in smokers. Am J Respir Crit Care Med. 2002;166(3):323–328. | ||
Pela R, Calcagni AM, Subiaco S, Isidori P, Tubaldi A, Sanguinetti CM. N-Acetylcysteine reduces the exacerbation rate in patients with moderate to severe COPD. Respiration. 1999;66(6):495–500. | ||
Zheng JP, Kang J, Huang SG, et al. Effect of carbocisteine on acute exacerbation of chronic obstructive pulmonary disease (PEACE study): a randomised placebo-controlled study. Lancet. 2008;371(9629):2013–2018. | ||
Almolki A, Guénégou A, Golda S, et al. Heme oxygenase-1 prevents airway mucus hypersecretion induced by cigarette smoke in rodents and humans. Am J Pathol. 2008;173(4):981–992. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.