")
Back to Journals » Journal of Blood Medicine » Volume 11
Correlation of Cardiac and Liver Iron Level with T2*MRI and Vitamin D3 Serum Level in Patients with Thalassemia Major
Authors Shaykhbaygloo R, Moradabadi A, Taherahmadi H, Rafiei M, Lotfi F, Eghbali A
Received 13 August 2019
Accepted for publication 26 February 2020
Published 11 March 2020 Volume 2020:11 Pages 83—87
DOI https://doi.org/10.2147/JBM.S227012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Roya Shaykhbaygloo,1 Alireza Moradabadi,2 Hassan Taherahmadi,1 Mohammad Rafiei,3 Fariborz Lotfi,1 Aziz Eghbali1
1Pediatric Department, Arak University of Medical Science, Arak, Iran; 2Hematology Department, Arak University of Medical Science, Arak, Iran; 3Biostatistics and Epidemiology Department, Arak University of Medical Science, Arak, Iran
Correspondence: Aziz Eghbali
Pediatric Department, Arak University of Medical Science, Basij Square, Arak, Iran
Tel +989 187982460
Email [email protected]
Introduction: Thalassemia is a hypochromic microcytic anemia, which is characterized by congenital disorders. In thalassemia patients, bone diseases are one of the causes of mortality. Our goal was to investigate the association between vitamin D deficiency and increased iron uptake by cardiac myocytes and hepatocytes.
Materials and Methods: Forty patients with thalassemia major were studied in Amir Kabir Hospital, Arak, Iran. The information obtained through clinical examination. Serum ferritin level was determined by ELISA and T2*MRI performed for measuring iron content in the heart and the liver.
Results: The average age of the patients was 23.8 ± 10.7 years. The mean T2*MRI values were 23.7 ± 7. The vitamin D3 level in 33 patients (82.5% cases) was less than 20 ng/dl, 2 patients (5%) in the range of 20– 30 ng/dl, and the others had above 30 ng/dl. Correlation between vitamin D and age was 0.611. Correlation coefficient between heart and liver T2*MRI with ferritin level in patients was 0.437 and 0.335, respectively.
Conclusion: Due to significant associations, the periodic measurement of vitamin D, as well as PTH, is recommended for patients with thalassemia major.
Keywords: thalassemia major, T2*MRI, cardiac and liver iron level, vitamin D3
Introduction
Thalassemia is a microcytic hypochromic anemia characterized by congenital abnormalities in hemoglobin production. It is estimated that 3% of the world population carry one of the characteristics of β-thalassemia traits. It is the most common genetic disease in the world.1,2 In the next 20 years, it is expected that around 900,000 thalassemic people will be born in the world, 95% of them in Asia, especially in India and the Middle East.3,4 Thalassemia is predominantly found in underdeveloped countries, and the prevalence of this disease is lower in Europe and North America.5,6 According to the Thalassemia Association in Iran, the number of patients with thalassemia in 2005 was 18,616, this number is more than 20,000 in 2016, and most of these patients are in the Mazandaran and Fars provinces.7,8 The disease is autosomal recessive and is inherited from the parents. A beta thalassemic baby is seen in about 300 cases every born in Iran. This is three times more than the highest hereditary diseases incidence, such as Down syndrome (it’s about 1 in 1000).9 Patients with β-thalassemia major need to have a lifelong blood transfusion, since they suffer from severe anemia (hemoglobin 6 g/dL).10 Each blood unit contains 200–250 mg iron.9,11-13 Repeated blood transfusions cause iron deposition in vital organs like heart, liver and endocrine glands.14 Iron overload may initiate structural changes in the myocardium which can eventually lead to heart failure which is considered as the major cause of death in thalassemic patients who depend on blood transfusion.1
The liver is the first organ to deposited iron and stores about 70% of visceral iron. Therefore, liver iron reflects the whole body of iron in the body. The heart is another important organ that iron deposited in. So iron deposition in this organ causes impairment of performance and is also the most important cause of death in thalassemic patients, measuring the amount of iron deposited is very important.8
In thalassemia patients, bone diseases are one of the causes of mortality, including osteoporosis, bone softness, changes in the shape of the spine and other large bones, and thinning the bone cartilage. Meanwhile, vitamin D is considered as one of the factors involved in the absorption of minerals which made bone matrix. Calcium and phosphorus are minerals that their absorption need for vitamin D in the intestines. The imbalance in body calcium in cases of increased iron load caused by thalassemia worsens bone disease in these patients. Vitamin D deficiency also is associated with a decrease in cardiac function, muscle weakness and glucose intolerance. In addition to vitamin D deficiency, PTH increases the expression of L-type or LVGCC-induced calcium channels,11,15–20 that these channels, in addition to calcium, absorb iron. This absorption caused iron deposition in muscles. Therefore, there was a relative correlation between low levels of vitamin D, increased iron deposition in liver and ventricular disorders in thalassemia.1,8
In this study, we aimed to investigate the association between vitamin D deficiency and increased iron uptake by liver and heart which measurable by T2 * MRI.
Materials and Methods
In this cross-sectional study, thalassemia major patients who were older than 5 years of age were investigated in Arak Amir Kabir Hospital, Iran. We used the Cochran formula for sample size by the effect of the thalassemia patients in Arak Amir Kabir Hospital, Iran. Thalassemia diagnosis was done by hemoglobin electrophoresis, target cells in the blood smear, and presence of isolated microcytic anemia. Ethics Committee approved the study (IR.ARAKMU.REC.1394.271) and written informed consent was taken from patients or parent(s) or by the legal representative prior to trial participation with the Declaration of Helsinki. Forty with diagnosed thalassemia major by the molecular methods were included in study. MRI was performed using Tesla magneto symphony Graniand 32.5/1 (Siemens Healthineers Germany).
The serum ferritin level was evaluated by ELISA (Abcam, Cambridge, England). The method of measuring serum vitamin D3 level was luminescence electroencephalography which uses polyclonal antibodies and specifically antibodies against 25OH vitamin D3. The unit of vitamin D is ng/dl and the range of measurements by the method is from 1/1 ng/dl to 1500 ng/dl. Participants were excluded if they had liver disorders, hepatitis B, C, HIV, changing chelation regimen within the last 6 months, and renal failure. Patients were discontinued from the study for these reasons: safety, lost to follow-up and voluntary discontinuation.
Statistical Analysis
Data were analyzed using SPSS 16 software (Chicago, USA). Normal distribution of data was checked by Kolmogorov–Smirnov. The results of quantitative and qualitative data were tested by ANOVA, T-test and linear regression. The P value <0.05 in was considered statistically significant. The intraclass correlation (ICC) was computed in order to determine the reproducibility of each method. For each method, the ICC amount was close to one, and the appropriate statistical analysis used in study.
Results
Of the 40 thalassemia major patients were transfusion dependent (Td), 27 (67.5%) and 13 (32.5%) patients were female and males respectively, the mean age of the patients was 23.8 ± 10.7 years, change between 7 and 55 years old. Three patients (7.5%) had been splenectomy.
The mean of T2 MRI values in all patients was 23.8 ± 7.7, the maximum and minimum were 38 and 7.5, respectively. The serum vitamin D3 levels in 33 patients (82.5% of cases) were less than 20 ng/dl, 2 (5%) patients were in the range of 20–30 ng/dl, and the other five patients had more than 30 ng/dl. The vitamin D level compared to reference range and categorized in deficient, insufficient and adequate categories. The mean serum vitamin D3 level in all patients was 16.1 ± 8.1 ng/dl. Ferritin and Parathyroid hormone measurements are also carried out and summarized in Table 1.
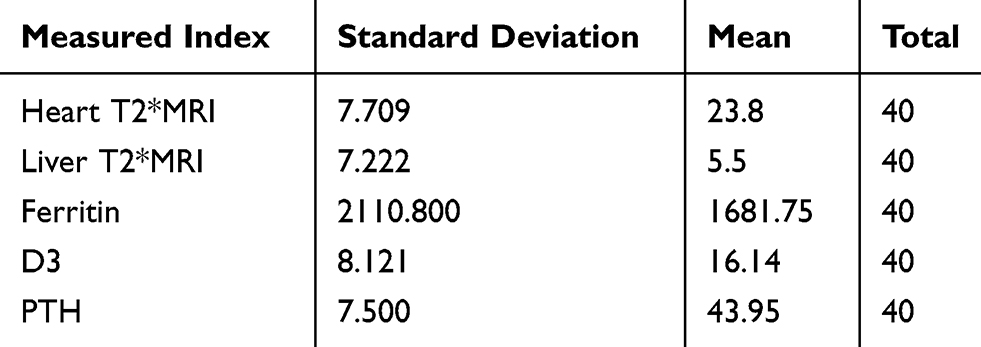 |
Table 1 Summarized Measured Criteria in the Patients |
Relationship Between Vitamin D3 Serum Levels and Age
As shown in Table 2, we found a significant correlation between vitamin D3 serum level and age in our studied subjects. The correlation suggests a reciprocal relationship between age and vitamin D3.
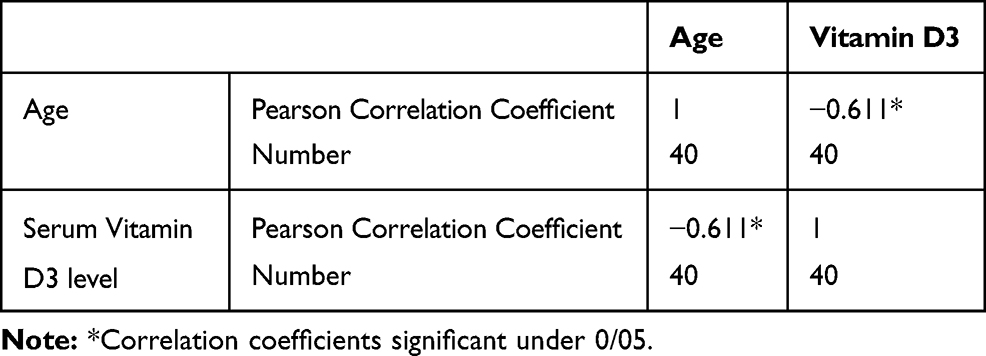 |
Table 2 Pearson Correlation Coefficient Between Age and Vitamin D3 |
The T-tests, showed no difference in Vitamin D3 serum levels in men and women (Table 3).
 |
Table 3 t-Test Vitamin D3 Serum Levels in Men and Women |
Correlation Between Heart T2*MRI and Ferritin, Vitamin D3, PTH
Correlation coefficient between Heart T2*MRI and ferritin levels was 0.437 and was significant. However, as presented in Table 4, there was no correlation between Heart T2*MRI, serum vitamin D3 and PTH levels.
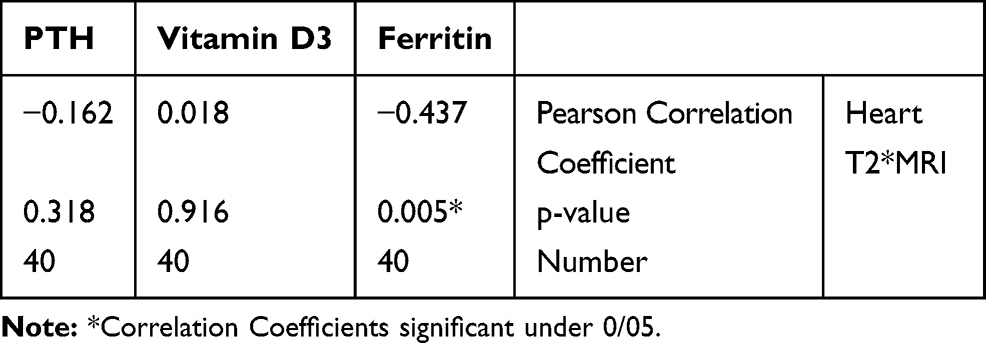 |
Table 4 Pearson Correlation Coefficient Between Heart T2 * MRI and Vitamin D3, Ferritin, PTH |
Correlation Between Liver T2*MRI and Ferritin, Vitamin D3, PTH
A significant association between liver T2*MRI and ferritin levels was seen. However, as shown in Table 5, there was no correlation between liver T2*MRI and serum vitamin D3 and PTH levels.
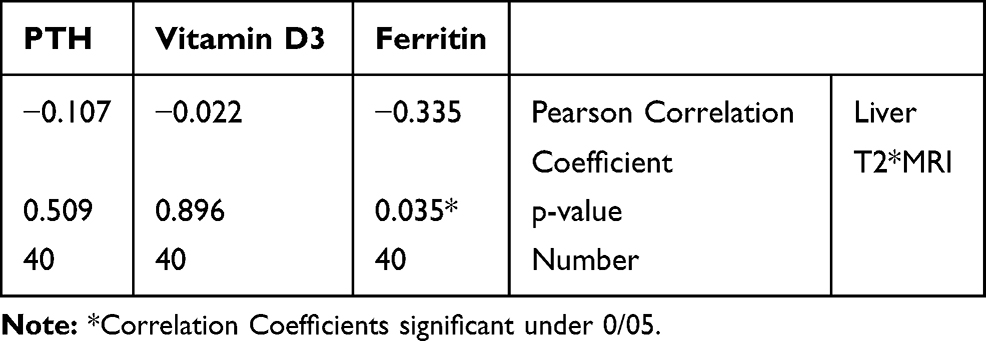 |
Table 5 Pearson Correlation Coefficient Between Liver T2 * MRI and Vitamin D3, Ferritin, PTH |
Correlation Between Ferritin and, Vitamin D3, PTH
As shown in Table 6, there was a positive correlation between the two variables. In addition, there was no correlation between serum ferritin and Vitamin D3.
 |
Table 6 Pearson Correlation Coefficient Between Ferritin, Vitamin D3, PTH |
Discussion
We found that there was a correlation between serum ferritin and PTH levels. This can be indicative of the fact that PTH, in contrast to Vitamin D3, is a better indicator of endocrine and osteoporosis in these patients. In this descriptive analytical study, 40 blood transfusion- dependent thalassemia patients were examined, the mean Vitamin D3 serum levels were 16.1 ± 8.1 in all patients, which showed an insufficient level. In a study in North America, the relationship between thalassemia syndrome and vitamin D deficiency was found in 361 patients, which 12.8% of subjects had less than 27 nmol/l and 82% had less than 75 nmol/l vitamin D.18 Another study on 96 thalassemic patients showed that 43% of patients had a deficiency of vitamin D, and 30% of them had insufficient level of vitamin D.21 In addition, a study on 220 thalassemia patients in showed that 37.2% of patients have serum vitamin D levels, less than 23 nmol/L.22 The percentage of patients with vitamin D deficiency in these studies varies with the present study, and it may be partially explained by underlying illness of patients, the difference in average age and the type of climate where they live. In this study, there was a correlation between heart and liver T2*MRI and serum ferritin levels. This finding correlates with the results of the study by Taghizadeh Sarvestani et al, which showed a negative correlation between serum ferritin levels and liver iron levels, measured by T2*MRI. Of note, serum ferritin levels and iron heart level there had no correlation.23
In our study, there was no correlation between ferritin and vitamin D3 in serum. This finding is consistent with the findings of nakavachara et al, in which 109 children between 5.9 to 14.1-year-old with HbE/B thalassemia were investigated.24
In our study, age increase caused a drop in the serum level of Vitamin D3. It suggests that old patients may require more Vitamin D3 supplementation.
Conclusion
Vitamin D measurement in thalassemic patients indicate a deficiency of this vitamin, though they get enough sunlight, this may suggest to administer vitamin D3. Also, deficiency of this vitamin is associated with an imbalance in the absorption of essential minerals for bone matrix and on the other hand, disruption of the endocrine in the thalassemic patients due to iron over load. The measurement of PTH level can be used to assess the degree of endocrine disruption in such patients. Therefore, periodic monitoring of other hormones is recommended. Accordingly, it can be concluded that a periodic and regular assessment of PTH levels is necessary in such patients.
Acknowledgment
The authors are thankful to staff of pediatric department in Arak University of Medical Sciences.
Disclosure
The authors report no conflicts of interest.
References
1. Origa R. β-thalassemia. Genet Med. 2017;19(6):609. doi:10.1038/gim.2016.173
2. Gregg X, Agarwal A, Prchal JT. Congenital Hemolytic Anemias. Concise Guide to Hematology. Springer; 2019:59–66.
3. Tender KE. Risk Factors for Severe Hyperbilirubinemia (Jaundice) Among Neonates in Accra. University of Ghana; 2018.
4. Mousavi Z, Yazdani Z, Moradabadi A, Hoseinpourkasgari F, Hassanshahi G. Role of some members of chemokine/cytokine network in the pathogenesis of thalassemia and sickle cell hemoglobinopathies: a mini review. Exp Hematol Oncol. 2019;8(1):1–6. doi:10.1186/s40164-019-0145-x
5. Angastiniotis M, Modell B. Global epidemiology of hemoglobin disorders. Ann N Y Acad Sci. 1998;850(1):251–269. doi:10.1111/j.1749-6632.1998.tb10482.x
6. Kemp G. The East Moves West: India, China, and Asia’s Growing Presence in the Middle East. Brookings Institution Press; 2012.
7. Weatherall DJ. The evolving spectrum of the epidemiology of thalassemia. Hematol Oncol Clin North Am. 2018;32(2):165–175. doi:10.1016/j.hoc.2017.11.008
8. Habibzadeh F, Yadollahie M, Merat A, Haghshenas M. Thalassemia in Iran; an overview. Arch Iran Med. 1998;1(1):27–33.
9. Cao A, Galanello R. Beta-thalassemia. Genet Med. 2010;12(2):61. doi:10.1097/GIM.0b013e3181cd68ed
10. Lucarelli G, Gaziev J. Advances in the allogeneic transplantation for thalassemia. Blood Rev. 2008;22(2):53–63. doi:10.1016/j.blre.2007.10.001
11. Kontoghiorghes GJ, Pattichi K, Hadjigavriel M, Kolnagou A. Transfusional iron overload and chelation therapy with deferoxamine and deferiprone (L1). Transfus Sci. 2000;23(3):211–223. doi:10.1016/S0955-3886(00)00089-8
12. Gordeuk VR, Bacon BR, Brittenham GM. Iron overload: causes and consequences. Annu Rev Nutr. 1987;7(1):485–508. doi:10.1146/annurev.nu.07.070187.002413
13. Taherahmadi H, Moradabadi AR, Arjomand Shabestari A, Nazari J, Kahbazi MK. Antibiotic induced hemolytic anemia and thrombocytopenia among pediatric patients admitted to intensive care unit. Iran J Pediatr Hematol Oncol. 2019;9(1):9–16.
14. Eghbali A, Taherahmadi H, Shahbazi M, Bagheri B, Ebrahimi L. Association between serum ferritin level, cardiac and hepatic T2-star MRI in patients with major β-thalassemia. Iran J Pediatr Hematol Oncol. 2014;4(1):17.
15. Vernejoul MCDE, Girot R, Gueris J, et al. Calcium phosphate metabolism and bone disease in patients with homozygous thalassemia. J Clin Endocrinol Metab. 1982;54(2):276–281. doi:10.1210/jcem-54-2-276
16. Wolfe L, Olivieri N, Sallan D, et al. Prevention of cardiac disease by subcutaneous deferoxamine in patients with thalassemia major. N Engl J Med. 1985;312(25):1600–1603. doi:10.1056/NEJM198506203122503
17. Lucarelli G, Galimberti M, Polchi P, et al. Bone marrow transplantation in patients with thalassemia. N Engl J Med. 1990;322(7):417–421. doi:10.1056/NEJM199002153220701
18. Vogiatzi MG, Macklin EA, Fung EB, et al. Bone disease in thalassemia: a frequent and still unresolved problem. J Bone Miner Res. 2009;24(3):543–557. doi:10.1359/jbmr.080505
19. Jensen C, Tuck S, Agnew J, et al. High prevalence of low bone mass in thalassaemia major. Br J Haematol. 1998;103(4):911–915. doi:10.1046/j.1365-2141.1998.01108.x
20. Vichinsky EP. The morbidity of bone disease in thalassemia. Ann N Y Acad Sci. 1998;850(1):344–348. doi:10.1111/j.1749-6632.1998.tb10491.x
21. Fung EB, Aguilar C, Micaily I, Haines D, Lal A. Treatment of vitamin D deficiency in transfusion‐dependent thalassemia. Am J Hematol. 2011;86(10):871–873. doi:10.1002/ajh.22117
22. Shamshirsaz AA, Bekheirnia MR, Kamgar M, et al. Metabolic and endocrinologic complications in beta-thalassemia major: a multicenter study in Tehran. BMC Endocr Disord. 2003;3(1):4. doi:10.1186/1472-6823-3-4
23. Taghizadeh Sarvestani R, Moradveisi B, Kompany F, Ghaderi E. Correlation between heart and liver iron levels measured by MRI T2* and serum ferritin in patients with β-thalassemia major. Int J Pediatr. 2016;4(3):1559–1567.
24. Nakavachara P, Chaichanwattanakul K, Viprakasit V. Non-transfusion dependent hemoglobin E/β thalassemia had high prevalence of vitamin D deficiency than more severe patients who received regular blood transfusion and iron chelation therapy. Int J Pediatr Endocrinol. 2013;2013(S1):P165. doi:10.1186/1687-9856-2013-S1-P165
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.