")
Back to Journals » Clinical Interventions in Aging » Volume 9
Cognitive effects of testosterone and finasteride administration in older hypogonadal men
Authors Borst S, Yarrow J, Fernandez C, Conover C, Ye F, Meuleman J, Morrow M, Zou B, Shuster J
Received 2 February 2014
Accepted for publication 16 April 2014
Published 12 August 2014 Volume 2014:9 Pages 1327—1333
DOI https://doi.org/10.2147/CIA.S61760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Stephen E Borst,1 Joshua F Yarrow,2 Carmen Fernandez,1 Christine F Conover,2 Fan Ye,2 John R Meuleman,1 Matthew Morrow,3 Baiming Zou,4 Jonathan J Shuster5
1Geriatric Research, Education and Clinical Center, 2Research Service, 3Pharmacy Service, Malcom Randall VA Medical Center, Gainesville Florida; 4Department of Biostatistics, 5Department of Health Outcomes and Policy, University of Florida, Gainesville, FL, USA
Abstract: Serum concentrations of neuroactive androgens decline in older men and, in some studies, low testosterone is associated with decreased cognitive function and incidence of depression. Existing studies evaluating the effect of testosterone administration on cognition in older men have been largely inconclusive, with some studies reporting minor to moderate cognitive benefit, while others indicate no cognitive effect. Our objective was to assess the cognitive effects of treating older hypogonadal men for 1 year with a supraphysiological dose of testosterone, either alone or in combination with finasteride (a type II 5α-reductase inhibitor), in order to determine whether testosterone produces cognitive benefit and whether suppressed dihydrotestosterone influences cognition. Sixty men aged ≥60 years with a serum testosterone concentration of ≤300 ng/dL or bioavailable testosterone ≤70 ng/dL and no evidence of cognitive impairment received testosterone-enanthate (125 mg/week) versus vehicle, paired with finasteride (5 mg/day) versus placebo using a 2×2 factorial design. Testosterone caused a small decrease in depressive symptoms as assessed by the Geriatric Depression Scale and a moderate increase in visuospatial memory as assessed by performance on a recall trial of the Rey-Osterrieth Complex Figure Test. Finasteride caused a small increase in performance on the Benton Judgment of Line Orientation test. In total, major improvements in cognition were not observed either with testosterone or finasteride. Further studies are warranted to determine if testosterone replacement may improve cognition in other domains.
Keywords: cognition, depression, 5 alpha reductase, testosterone enanthate
Introduction
Loss of testosterone in older men is associated with a substantial long-term impairment in visual and verbal memory, visuospatial functioning, visuomotor scanning, and visual memory,1 and with increased incidence and earlier onset of depression.2 These findings are supported by rodent studies in which orchiectomy has been shown to impair spatial memory in Y-maze testing3 and Morris water maze testing,4 with testosterone administration preserving memory. Despite this evidence, a recent clinical study indicates that short-term (6 weeks) androgen deprivation does not significantly impair cognition (assessed in a variety of domains) in men.5
Existing studies of testosterone administration in older men are typically 1 year or less in duration and have demonstrated only moderate improvements in visuospatial cognition, but not in other domains such as verbal cognition or mood. For example, Janowsky et al treated older eugonadal men for 3 months with testosterone by transdermal patch (15 mg/day). Testosterone improved performance on the block design subtest of the Wechsler Adult Intelligence Scale (WAIS) – Revised, but did not improve performance on other cognitive tests. The latter included vocabulary subtest of the WAIS, California Verbal Learning Test, Profile of Mood States, Trail Making Tests A and B, and Grooved Pegboard Test.6 Gray et al7 administered graded doses of testosterone (25 to 600 mg/week) to older men and observed that testosterone did not alter mood (measured by the Hamilton Depression Inventory and Young Mania Rating Scale) and produced a marginal improvement in visuospatial cognition (computer-based checkerboard test). Cherrier et al8 treated older men with testosterone (100 mg/week, intramuscularly [IM]) for 6 weeks and observed improved spatial memory (route test) and constructional abilities (WAIS block design subtest) and increased route test and word list recall.9 In contrast, Vaughan et al10 administered testosterone (200 mg biweekly, IM) and failed to demonstrate improvement in visuospatial function or visual memory using the Benton Judgment of Line Orientation test and Benton Visual Retention test, respectively. As such, some inconsistency exists in the literature regarding the effects of testosterone administration on cognitive function in older men.
Our objective was to determine whether treatment of older hypogonadal men with a supraphysiological dose of testosterone for 1 year reduces depressive symptoms, improves wellbeing, and improves visuospatial cognition, and whether co-treatment with finasteride influences these results. We have recently shown that treatment with testosterone plus finasteride provides musculoskeletal and lipolytic benefits without prostate enlargement,11 providing sound rationale for this combination pharmacologic therapy. A second objective was to determine whether finasteride has any effects on cognition.
Methods
Study design and subject selection
Qualifying participants were men aged 60 years or more who had a total serum testosterone level of ≤300 ng/dL or a bioavailable testosterone (BioT) level of ≤70 ng/dL. Participants were randomized to one of four treatment groups – vehicle–placebo, testosterone-enanthate (TE)–placebo, vehicle–finasteride, or TE–finasteride – using a 2×2 factorial design. A total of 60 subjects were randomized, 16 to vehicle plus placebo, 13 to vehicle plus finasteride, 14 to TE plus placebo, and 17 to TE plus finasteride. Treatment lasted 12 months and consisted of Proscar® (Merck & Co., Inc., Whitehouse Station, NJ, USA) (5 mg/day finasteride, per oral) versus placebo, and Delatestryl® (Novartis International AG, Basel, Switzerland) (125 mg/week TE, IM) versus vehicle. Proscar® and matching placebo were donated by Merck & Co., Inc. Delatestryl® was donated by Novartis International AG and matching vehicle was prepared by WestLab Pharmacy, Gainesville, FL, USA. Participants were not paid for participation other than receiving reimbursement for travel mileage.
This study was approved by the Institutional Review Board of the University of Florida. All participants gave written informed consent. Potential participants underwent screening to determine eligibility, including structured medical history, blood acquisition (performed twice between 8 am and 10 am, separated by at least 30 minutes), and a physical exam, as previously reported.11 Two blood samples were obtained during screening because the Endocrine Society recommends repeated measurements to confirm low testosterone prior to initiating testosterone treatment.12
We excluded individuals who failed the Mini-Cog test13 to ensure that participants did not present with dementia and that they could fully understood the study protocol. We also excluded: those with a history of prostate or breast cancer, severe benign prostatic hypertrophy, American Urological Society/International Prostate Symptom Score (AUA/IPSS) score ≥25, class 3 or 4 congestive heart failure, sleep apnea, hematocrit >49%, prostate specific antigen ≥2.6 ng/mL, body mass index >35, or orthopedic limitations (precluding strength testing); or those who had received testosterone within 4 weeks, finasteride/dutasteride within 6 months, or who were taking Coumadin® (a contraindication for IM injections).
Protection from risks
Participants underwent thorough health screenings every 3 months throughout the study, as previously reported.11 Participants were removed from the study if the following occurred: hematocrit ≥54%; serum prostate specific antigen ≥4.0; increase in AUA/IPSS ≥4 points; or if gynecomastia or peripheral edema were noted at physical exam.
Hormone assays
Serum samples were obtained 1 week after TE/vehicle injection. Total testosterone was assessed in the Clinical Laboratory, Malcom Randall VA Medical Center by Cobas® (Hoffman-La Roche Ltd., Basel, Switzerland) electrochemiluminescence immunoassay (intra-assay coefficient of variance [CV] =2.9%, inter-assay CV =3.4%). Serum samples were stored at −80°C and analyzed for estradiol (E2) by ELISA (enzyme-linked immunosorbent assay; American Laboratory Products, Salem, NH, USA) (intra-assay CV =7.6%, inter-assay CV =8.8%). BioT and bioavailable estradiol (BioE2) were assessed by ammonium sulfate precipitation of samples spiked with 3H-testosterone or 3H-E2.14 Dihydrotestosterone (DHT) was assessed by liquid chromatography – mass spectroscopy – mass spectroscopy at Laboratory Corp of America (Calabasas Hills, CA, USA) (intra-assay CV =8.6%, inter-assay CV =9.9%).
Cognitive testing
Cognitive testing was performed at baseline and after 3, 6, 9, and 12 months of treatment. Life Satisfaction Index A and B were used to measure multiple components of psychological wellbeing, with a higher score indicating greater wellbeing.15 The Geriatric Depression Scale (GDS) short form was used to assess depressive symptoms, with a higher score indicating more depressive symptoms.16,17 The GDS short form consists of the 15 items from the GDS long form that have the highest correlation with depressive symptoms.
Trail Making Test A (subject draws a line connecting a sequence of numbers in ascending order with a pencil) was used to assess attention. Trail Making Test B (subject draws a line connecting an alternating sequence of numbers and letters in ascending order with a pencil) was used to assess executive functioning.18 Trail making tests are scored as time (seconds) taken to successfully complete the task. Benton Judgment of Line Orientation test Form H was used to assess visuospatial skills, with a higher score indicating better performance.19 This is a 30-item task in which the subject must match a pair of angled lines appearing on the stimulus drawing to two identically oriented lines (out of eleven choices) drawn below the stimulus. The Rey-Osterrieth Complex Figure Test was used to assess visuospatial constructional functions, visuographic memory, and some aspects of planning.20 The subject was asked to make a copy of a stimulus drawing comprised of a complex design, which was then scored on 18 identifiable details with a maximum score of 36 points possible and a higher score indicating better performance. The subject then drew the figure from memory 5 minutes later, and again 30 minutes later. Drawings were scored by a licensed neuropsychologist (CF).
Musculoskeletal assessment
Muscle strength was assessed as one-repetition maximal strength on a selectorized resistance exercise machine for six upper- and lower-body exercises. Body composition was assessed by dual x-ray absorptiometry using a General Electric Lunar Prodigy fan-beam densitometer (Fairfield, CT, USA). Prostate volume was assessed by transrectal ultrasound sizing using a General Electric LOGICQ P5 scanning system (General Electric, Fairfield, CT, USA).
Statistical model and analysis
The following mixed effects models were used to fit the data with three covariance structures considered – compound symmetry, autoregressive (Equation 1), and unstructured – as shown in the following:
yijk = α0 + αtrt I(I=1) + α1 I(k=3) + α2 I(k=6) + α3 I(k=9) + α4 I(I=1) I(k=3) + α5 I(I=1) I(k=6) + α6 I(I=1) I(k=9) + uij + εijk | (1) |
yijk = α0 + αtrt I(i=1) + α1 I(k=3) + α2 I(k=6) + α3 I(k=9) + uij + εijk | (2) |
where yijk is the response (ie, change-depression, etc) of subject j, measured at time point k with respect to the change from the baseline, under treatment I; I(x= value) is the indicator function (ie, 1 if x= value and 0 otherwise); αtrt represents the treatment effect; α1–α3 represent the time effect; α4–α6 represent the interactions between time and treatment effects; uij is the cluster effect due to subject j under treatment i and is assumed to follow N(0,Σ) with Σ being the covariance matrix of 4×4 dimension; and uij characterizes the correlation for the responses from subject j. Three model selection criteria were used to select the best-fit model among the six candidate models for the data, namely Akaike information criterion, corrected Akaike information criterion, and Bayesian information criterion. εijk is the random measurement error following normal distribution. P-values ≤0.05 were considered statistically significant. Analyses of results reported are based on the selected best-fit model.
Nontechnical description of statistics
We chose the linear mixed model above for two reasons: first, it has the advantage over the alternative of pre-/post-differences in that it utilizes all the time point data; and second, it is more robust against missing data. As a secondary analysis, for the variable that we found to be significant on the main testosterone effect, we applied the same analysis separately to the two subgroups (one with and one without finasteride) to see if testosterone differences were dependent on finasteride. The study was powered on the primary outcomes of Borst et al11 and not for cognitive end points.
Results
The musculoskeletal findings and hormone concentrations from this study have been published.11 Briefly, testosterone administration increased maximal muscle strength by 8%–14% (on all six exercises), increased bone mineral density by 1.96% in the hip and by 4.19% in the lumbar spine, reduced fat mass by 3.87 kg, and increasing prostate volume by 11.4 cm3. Coadministration of finasteride prevented testosterone-induced prostate enlargement, but did not affect other responses to testosterone. TE elevated nadir testosterone and BioT, representing 1.8-fold and 2.2-fold increases over baseline, respectively. Coadministration of finasteride did not affect those increases. TE elevated E2 and BioE2, representing 1.7-fold and 2.2-fold increases over baseline, respectively. Coadministration of finasteride did not affect those increases. TE elevated serum DHT by 2.4-fold and finasteride lowered DHT by 65%.
Subject baseline characteristics are shown in Table 1. Treatment effects of testosterone and finasteride are shown in Table 2. TE administration resulted in statistically significant reduction in depressive symptoms on the GDS by 0.74 points on a 15 point scale, with most of the change occurring within the first 3 months of treatment. TE also significantly improved performance on the 30-minute recall trial of the Rey-Osterrieth Complex Figure Test (Rey30) by 2.87 points on a 36 point scale. In order to test the hypothesis that the true population effect size on GDS or Rey30 for testosterone versus placebo is the same whether finasteride is given or not, we applied the same analyses to the two subgroups (ie, with finasteride versus without). P-values of 0.48 and 0.72 were obtained for GDS and Rey30, respectively, indicating that no testosterone and finasteride interaction exists for either end point. Finasteride significantly improved performance in the Benton Judgment of Line Orientation test by 1.89 points on a 30 point scale.
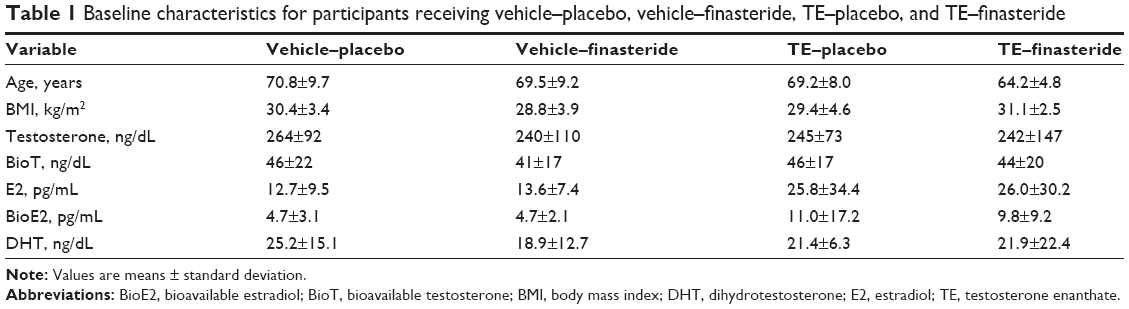 | Table 1 Baseline characteristics for participants receiving vehicle–placebo, vehicle–finasteride, TE–placebo, and TE–finasteride |
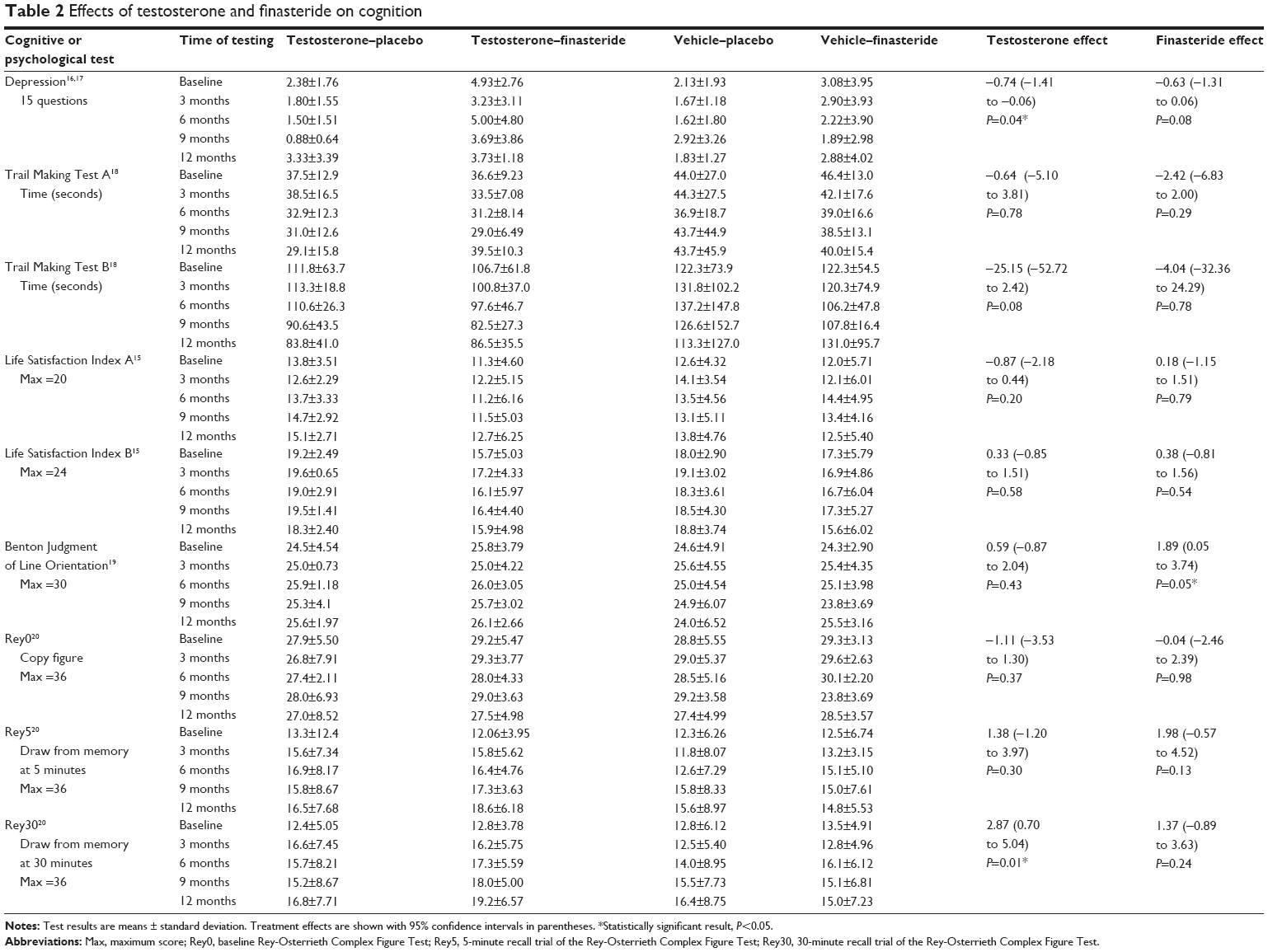 | Table 2 Effects of testosterone and finasteride on cognition |
Correlations between serum hormones and cognitive performance at baseline are shown in Table 3. Higher baseline E2 (P=0.039) and BioE2 (P=0.050) were positively associated with wellbeing on the Life Satisfaction Index A test, but not on the Life Satisfaction Index B. Increased age was associated with fewer depressive symptoms on the GDS (P=0.014), and with increased wellbeing as assessed by Life Satisfaction Index A (P=0.006) and B (P=0.047), but with poorer performance on the Trail Making Test A (P<0.001) and Trail Making Test B (P=0.006) tests. The positive effect of TE on depressive symptoms was unchanged when the data were reanalyzed and controlled for age as a covariate.
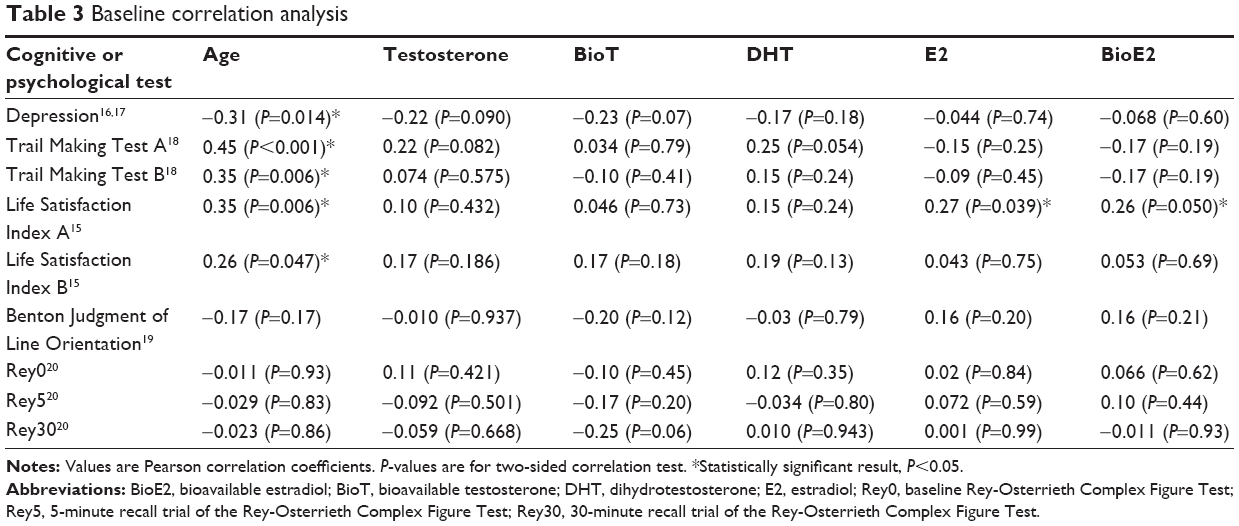 | Table 3 Baseline correlation analysis |
Discussion
The main findings of this study are that testosterone treatment reduced depressive symptoms and improved visuospatial memory on the Rey30. The presence of finasteride did not inhibit these effects. In addition, finasteride administration produced an unexpected minor increase in visuospatial skill on the Benton Judgment of Line Orientation test. Higher serum E2 and BioE2 values at baseline were correlated with a greater sense of wellbeing on Life Satisfaction Index A and B. Increased age was associated with improved scores on the GDS and Life Satisfaction Index A and B.
A review by Holland et al shows that existing studies on the effects of testosterone administration on depression in older men have produced mixed results.21 Haren et al treated older men for 1 year with an oral dose of testosterone undecanoate that produced only a small increase in serum testosterone and found that treatment did not affect scores on the GDS.22 Vaughan et al treated older men with a supraphysiologic dose of testosterone for 36 months and found that scores on the Beck Depression Scale were unchanged.10 However, other studies have reported positive effects of testosterone on mood. Pope et al treated older hypogonadal men with refractory depression for 8 weeks with a moderate dose of testosterone and found improvement on the Hamilton Depression Rating Scale.23 Wang et al treated older hypogonadal men with testosterone gel for 3 months and found that testosterone increased self-assessed positive moods and decreased negative moods.24 Perry et al treated older men with major depression for 6 weeks with a supraphysiological dose of testosterone and found an improvement in Hamilton Depression Rating Scale scores only in men with onset of depression at age ≥45 years.25 Shores et al reported that testosterone gel improved Hamilton Depression Rating Scale scores in hypogonadal men with minor depression.26 We observed that 12 months of testosterone administration produced an improvement in scores on the GDS.
Existing studies on the effects of testosterone on visuospatial cognition have also produced mixed results. Janowsky et al treated older men for 12 weeks with a transdermal dose of testosterone sufficient to raise serum testosterone by 50% and found a significant improvement on the block design subtest of the WAIS.6 Cherrier et al treated older men with mild cognitive impairment with supraphysiological testosterone for 6 weeks and also found improved performance on the block design subtest of the WAIS.8 However, Vaughan et al,10 Haren et al,22 Gray et al,7 and Young et al5 have all treated older men with testosterone and found no changes in visuospatial cognition. However, we found that testosterone improved visuospatial cognition as assessed by the Rey-Osterrieth Complex Figure Test. We also found that finasteride improved visuospatial performance on the Benton Judgment of Line Orientation test. Finasteride blocks tissue-specific conversion of testosterone to DHT, resulting in somewhat higher serum concentrations of testosterone and E2. However, the mechanism by which finasteride might improve visuospatial cognition is unclear.
We found that increased age was associated with poorer performance on the Trail Making Tests A and B, with fewer depressive symptoms on the GDS, and with increased wellbeing as assessed by Life Satisfaction Index A and B. Normative studies show that performance on Trail Making tests declines with age.27 However, in similar studies, age is not associated with lower depression scores28 or improved Life Satisfaction Index scores.29 The association of increased age with improved depression and Life Satisfaction Index scores may result from the fact that the oldest subjects in our study would have had to be exceptionally healthy in order to participate in a study demanding intensive subject participation.
Beneficial cognitive effects of testosterone may result directly from binding of testosterone to androgen receptors or indirectly following conversion of testosterone to DHT 5-alpha reductase. There is evidence that DHT specifically reduces neuroinflammation.30 In humans, it has been shown that the cerebral cortex31 and hippocampus32 express 5-alpha reductase isoform I, but not isoform II. Therefore, it is unlikely that finasteride significantly lowers DHT concentrations in these regions. Our data are consistent with the hypothesis that, whether or not cognitive benefits of testosterone require conversion of testosterone to DHT, finasteride would not be expected to reduce those benefits.
Consistent strong cognitive benefits resulting from testosterone administration have not been identified to date. However, a limited number of cognitive domains have been the subject of past studies, leaving the question of whether benefits may occur in domains that have not yet been tested. A large amount of literature supports the role of testosterone in social dominance and approach motivation.33,34 Anecdotally, some subjects report that testosterone treatment increases feelings of energy and motivation. However, the effects of testosterone treatment on motivation in hypogonadal men has not been tested. Aarts and van Honk have reported that acute administration of testosterone to young women increased motivation, as assessed by a computerized test of responses to neutral nonsexual cues.35 Future studies are warranted to investigate the potential benefits of testosterone on the areas of drive, motivation, and other as yet untested cognitive domains.
In conclusion, we report that testosterone produced small improvements in depressive symptoms and visuospatial cognition. Our results are generally consistent with the literature, which shows that testosterone treatment produces somewhat inconsistent improvements in cognition.
Disclosure
The authors report no conflicts of interest in this work.
References
Moffat SD, Zonderman AB, Metter EJ, Blackman MR, Harman SM, Resnick SM. Longitudinal assessment of serum free testosterone concentration predicts memory performance and cognitive status in elderly men. J Clin Endocrinol Metab. 2002;87(11):5001–5007. | ||
Shores MM, Moceri VM, Sloan KL, Matsumoto AM, Kivlahan DR. Low testosterone levels predict incident depressive illness in older men: effects of age and medical morbidity. J Clin Psychiatry. 2005;66(1):7–14. | ||
Hawley WR, Grissom EM, Martin RC, Halmos MB, Bart CL, Dohanich GP. Testosterone modulates spatial recognition memory in male rats. Horm Behav. 2013;63(4):559–565. | ||
Ota H, Akishita M, Akiyoshi T, et al. Testosterone deficiency accelerates neuronal and vascular aging of SAMP8 mice: protective role of eNOS and SIRT1. PloS One. 2012;7(1):e29598. | ||
Young LA, Neiss MB, Samuels MH, Roselli CE, Janowsky JS. Cognition is not modified by large but temporary changes in sex hormones in men. J Clin Endocrinol Metab. 2010;95(1):280–288. | ||
Janowsky JS, Oviatt SK, Orwoll ES. Testosterone influences spatial cognition in older men. Behav Neurosci. 1994;108(2):325–332. | ||
Gray PB, Singh AB, Woodhouse LJ, et al. Dose-dependent effects of testosterone on sexual function, mood, and visuospatial cognition in older men. J Clin Endocrinol Metab. 2005;90(7):3838–3846. | ||
Cherrier MM, Matsumoto AM, Amory JK, et al. Testosterone improves spatial memory in men with Alzheimer disease and mild cognitive impairment. Neurology. 2005;64(12):2063–2068. | ||
Cherrier MM, Matsumoto AM, Amory JK, et al. Characterization of verbal and spatial memory changes from moderate to supraphysiological increases in serum testosterone in healthy older men. Psychoneuroendocrinology. 2007;32(1):72–79. | ||
Vaughan C, Goldstein FC, Tenover JL. Exogenous testosterone alone or with finasteride does not improve measurements of cognition in healthy older men with low serum testosterone. J Androl. 2007;28(6): 875–882. | ||
Borst SE, Yarrow JF, Conover CF, et al. Musculoskeletal and prostate effects of combined testosterone and finasteride administration in older hypogonadal men: a randomized, controlled trial. Am J Physiol Endocrinol Metab. 2014;306(4):E433–442. | ||
Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536–2559. | ||
Costa D, Severo M, Fraga S, Barros H. Mini-Cog and Mini-Mental State Examination: agreement in a cross-sectional study with an elderly sample. Dement Geriatr Cogn Disord. 2012;33(2–3):118–124. | ||
Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999;84:3666–3672. | ||
Subaşi F, Hayran O. Evaluation of life satisfaction index of the elderly people living in nursing homes. Arch Gerontol Geriatr. 2005;41(1):23–9. | ||
Granger CV, Cotter AC, Hamilton BB, Fiedler RC, Hens MM. Functional assessment scales: a study of persons with multiple sclerosis. Arch Phys Med Rehabil. 1990;71(11):870–875. | ||
Stineman MG, Shea JA, Jette A, et al. The Functional Independence Measure: tests of scaling assumptions, structure, and reliability across 20 diverse impairment categories. Arch Phys Med Rehabil. 1996; 77(11):1101–1108. | ||
Hankee LD, Preis SR, Beiser AS, et al. Qualitative neuropsychological measures: normative data on executive functioning tests from the Framingham offspring study. Exp Aging Res. 2013;39(5):515–35. | ||
Woodard JL, Benedict RH, Salthouse TA, Toth JP, Zgaljardic DJ, Hancock HE. Normative data for equivalent, parallel forms of the Judgment of Line Orientation Test. J Clin Exp Neuropsychol. 1998;20(4):457–62. | ||
Reedy SD, Boone KB, Cottingham ME, et al. Cross validation of the Lu and colleagues (2003) Rey-Osterrieth Complex Figure Test effort equation in a large known-group sample. Arch Clin Neuropsychol. 2013;28(1):30–7. | ||
Holland J, Bandelow S, Hogervorst E. Testosterone levels and cognition in elderly men: a review. Maturitas. 2011;69(4):322–337. | ||
Haren MT, Wittert GA, Chapman IM, Coates P, Morley JE. Effect of oral testosterone undecanoate on visuospatial cognition, mood and quality of life in elderly men with low-normal gonadal status. Maturitas. 2005;50(2):124–133. | ||
Pope HG Jr, Cohane GH, Kanayama G, Siegel AJ, Hudson JI. Testosterone gel supplementation for men with refractory depression: a randomized, placebo-controlled trial. Am J Psychiatry. 2003;160(1): 105–111. | ||
Wang C, Swerdloff RS, Iranmanesh A, et al. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. J Clin Endocrinol Metab. 2000;85(8):2839–2853. | ||
Perry PJ, Yates WR, Williams RD, et al. Testosterone therapy in late-life major depression in males. J Clin Psychiatry. 2002;63(12): 1096–1101. | ||
Shores MM, Kivlahan DR, Sadak TI, Li EJ, Matsumoto AM. A randomized, double-blind, placebo-controlled study of testosterone treatment in hypogonadal older men with subthreshold depression (dysthymia or minor depression). J Clin Psychiatry. 2009;70(7):1009–1016. | ||
Tombaugh TN. Trail Making Test A and B: normative data stratified by age and education. Arch Clin Neuropsychol. 2004;19(2):203–214. | ||
Knight RG, Chisholm BJ, Marsh NV, Godfrey HP. Some normative, reliability, and factor analytic data for the revised UCLA Loneliness Scale. J Clin Psychol. 1988;44(2):203–206. | ||
Pavot W, Diener E, Colvin CR, Sandvik E. Further validation of the Satisfaction with Life Scale: evidence for the cross-method convergence of well-being measures. J Pers Assess. 1991;57(1):149–161. | ||
Giatti S, Boraso M, Melcangi RC, Viviani B. Neuroactive steroids, their metabolites, and neuroinflammation. J Mol Endocrinol. 2012;49(3): R125–R134. | ||
Steckelbroeck S, Watzka M, Reichelt R, et al. Characterization of the 5alpha-reductase-3alpha-hydroxysteroid dehydrogenase complex in the human brain. J Clin Endocrinol Metab. 2001;86(3):1324–1331. | ||
Stoffel-Wagner B, Beyenburg S, Watzka M, et al. Expression of 5alpha-reductase and 3alpha-hydroxisteroid oxidoreductase in the hippocampus of patients with chronic temporal lobe epilepsy. Epilepsia. 2000;41(2):140–147. | ||
Eisenegger C, Haushofer J, Fehr E. The role of testosterone in social interaction. Trends Cogn Sci. 2011;15(6):263–271. | ||
Mazur A, Booth A. Testosterone and dominance in men. Behav Brain Sci. 1998;21(3):353–363; discussion 363–397. | ||
Aarts H, van Honk J. Testosterone and unconscious positive priming increase human motivation separately. Neuroreport. 2009;20(14): 1300–1303. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.