")
Back to Archived Journals » Journal of Neurorestoratology » Volume 3
Clinical neurorestorative progress in multiple sclerosis
Received 29 September 2014
Accepted for publication 8 January 2015
Published 31 March 2015 Volume 2015:3 Pages 83—90
DOI https://doi.org/10.2147/JN.S74146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Hari Shanker Sharma
Tong Chao Geng,1 Victor W Mark2
1Department of Neurology, Yuquan Hospital of Tsinghua University, Beijing, People's Republic of China; 2Department of Physical Medicine and Rehabilitation, University of Alabama at Birmingham, Birmingham, AL, USA
Abstract: With the chronic progress of the disease, the majority of patients with multiple sclerosis will eventually become severely disabled and unable to live independently. Neurorestorative strategies, including cell therapy and neuromodulation, combined with neurorehabilitation, have shown encouraging signs that may benefit multiple sclerosis patients. This review indicates current progress in this area.
Keywords: demyelinating disease, immunosuppression, cell therapy, neuromodulation, neurorehabilitation
Introduction
Multiple sclerosis (MS) is an autoimmune demyelinating disease of the central nervous system (CNS). Typical MS starts between 20 and 40 years of age, and women are affected approximately twice as often as men.1 The pathological changes of the CNS in MS involve invasion by inflammatory cells, demyelination, deposition of immunoglobulin and complement, gliosis, remyelination, and axonal loss.2,3
Patients with MS suffer from transmission functions of the CNS due to tissue damage, which are manifested by a wide range of neurological symptoms, such as numbness, motor weakness, visual impairment, diplopia, ataxia, fatigue, urinary urgency or retention, pain, depression, and cognitive dysfunction, among others. Clinical manifestations vary among patients, as well as in different phases of the disease in each patient.4
Intravenous high-dose steroids have become the standard for treating an acute relapse of MS to reduce inflammatory damage to the myelin sheath and axon and hasten recovery from inflammation.5 Plasma exchange by removing the immunoinflammatory substances can improve clinical manifestation in patients who are unresponsive to steroids.
Immunomodulatory agents, also called disease-modifying drugs, such as IFNβ, glatiramer acetate, and fingolimod, are currently considered first-line therapies for relapsing–remitting MS.6 Symptomatic management is an important part of care of patients. Baclofen, tizanidine, and gabapentin may reduce spasticity.7,8 Oral oxybutynin9 and injection of botulinum toxin A10 can effectively reduce bladder overactivity to improve bladder symptoms. Carbamazepine,11 lamotrigine, gabapentin,12 or oxcarbazepine13 can benefit paroxysmal pain in MS patients. Treatment with amantadine or modafinil can improve fatigue in patients with relapsing–remitting MS.14 Donepezil improved learning and memory in MS patients with cognitive impairment in one clinical trial,15 but was not superior to placebo in another clinical trial for improving MS-related cognitive dysfunction.16 These conventional treatment strategies can reduce inflammatory reaction and improve clinical symptoms, but do not halt neurodegeneration (Table 1). Recently, neurorestorative strategies have shown the potential to extend results beyond conventional treatment, and are briefly summarized in this review.
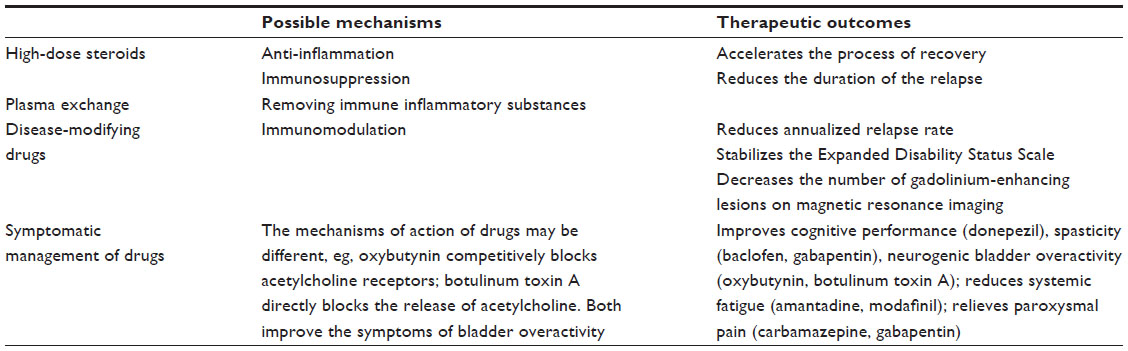 | Table 1 Conventional therapies for multiple sclerosis |
Cell therapies
Hematopoietic stem cells
In an initial small clinical trial, patients with MS who received hematopoietic stem cells (HSCs) showed a stable or improved Expanded Disability Status Scale (EDSS) score without new lesions on magnetic resonance imaging (MRI).17 HSC therapy in subsequent trials has been associated with sustained clinical improvement.18–22 Maintenance treatment was not needed in the absence of disease progression. However, patients who experienced neurological relapse and deterioration after cell transplantation needed further immunosuppression treatment.23 More than 600 cases of HSC transplantation have been reported worldwide in the medical literature since 1995.24 Patients with severe, highly active forms of progressive MS unresponsive to conventional treatments experienced a high rate of sustained remissions following HSC transplantation,25 although some patients developed infections, CNS toxicity, and even mortality.24
Mesenchymal stromal cells
Bone marrow mesenchymal stromal cells
The mean EDSS score in MS patients after transplantation of autologous bone marrow mesenchymal stromal cells (B-MSCs) improved in one study.26 In another study, visual acuity and visual evoked response latency in patients with secondary progressive MS also improved, with an increase in optic nerve area.27 Patients in a small trial showed visual improvement, but without arrest of progression of lesions on MRI after B-MSC transplantation.28 Patients in another pilot study also failed to show treatment effects on EDSS score or MRI assessment.29 The limited therapeutic efficacy after B-MSC transplantation may be related to the absence of immunosuppressive preconditioning.
Umbilical cord mesenchymal stromal cells
The course of patients with refractory progressive MS became stable after receiving transplantation of umbilical cord MSCs (U-MSCs).30,31 The treatments were tolerated well without significant adverse events.31
Olfactory ensheathing cells
The symptoms and signs of patients with MS have been shown to improve for several months with transplantation of olfactory ensheathing cells.32,33
Mechanisms of cell therapies
Preclinical animal studies indicate that functional recovery after cell transplantation does not correlate with the amount of neural cells originating from transplanted cells or replacing damaged cells, and may be associated with other mechanisms exhibited by transplanted cells.34
Reconstitution of immune system
Transplantation of HSCs can produce long-term remission by destroying the autodestructive immune system and reconstituting it in MS patients.24
Immunomodulation
Previous studies have demonstrated that stem cells from different sources have immunosuppressive properties. Neural progenitor cells can inhibit T-cell activation and proliferation, accompanied by suppression of proinflammatory cytokines.35 MSCs inhibit the activation of T cells, B cells, natural killer cells, and dendritic cells.36 MSCs modulate local allogeneic responses through the secretion of prostaglandin 2, which switches the host immune response from a T-helper (Th)-1/Th17- toward an anti-inflammatory Th2-like secretory profile.37 U-MSCs increase regulatory T cells and reestablish the balance between Th1- and Th2-related functions.38 Other soluble factors, such as indoleamine 2,3-dioxygenase, TGFβ1, and hepatocyte growth factor, have been implicated in the immunomodulation of B-MSCs.34 Transplantation cells reduce the inflammatory process and ameliorate disease activity by peripheral immunosuppression.
Neuroprotective and neuroregenerative effects
A variety of evidence suggests that stem cells from different sources have the properties of neuroprotection and neuroregeneration. B-MSCs enhance endogenous neural repair in animal models of MS.39 Neural stem cells in vivo and in vitro have been demonstrated to produce a variety of trophic factors, including NGF, BDNF, and GDNF.40 U-MSCs secrete antioxidants, NGF, VEGF, and bFGF.41,42 These factors may modulate the molecular composition of the environment to evoke responses from resident cells and induce axonal outgrowth, remyelination, and regeneration, and protect and rescue degenerating neurons.
Angiogenesis
U-MSCs express more genes and secrete more factors contributing to angiogenesis and neurogenesis than B-MSCs.43 Grafted B-MSCs can differentiate into endothelial cells44 and promote the proliferation of endogenous neural stem/progenitor cells through vascular niche regulation in injured regions.45 Sharma et al showed that the metabolic function of many parts of the CNS significantly changed after cell treatment in patients with chronic stroke and autism.46,47 Angiogenesis and neovascularization induced by MSCs increase cerebral blood- and oxygen-flow perfusion, thus contributing to neurorestoration.
Neuromodulation
The majority of patients with MS must endure chronic sensory and motor disabilities, such as spasticity, pain, fatigue, and tremor. Some devices of neuromodulation therapy that target the brain, cranial nerves, spinal cord, or peripheral nerves can be used to treat various refractory neurological diseases by the modulation of nervous system activity rather than the modification of damaged structure.48,49
Neuromodulation of the CNS
Transcranial magnetic stimulation (TMS) induces long-term excitability changes of the cerebral cortex, and has been applied to treat MS. MS patients who received intermittent theta-burst TMS50 and repetitive TMS (rTMS)51 had ameliorated spasticity. rTMS can also be used to treat cerebellar impairment in MS patients52 and improve bladder dysfunction.53 However, rTMS, as a more powerful modality, can also increase the risk of seizures.54–56
Motor-cortex stimulation has been confirmed to be effective for central neuropathic pain, including in MS, but higher-intensity stimulation parameters are needed to gain adequate pain relief.57 Single-pulse TMS relieves chronic neuropathic pain in patients with various neurological diseases, including MS.
Severe tremor might be the main cause of disability in some MS patients. Deep-brain stimulation (DBS) of the thalamic nucleus ventralis intermedius can significantly reduce the intensity of contralateral limb tremor in persons with essential tremor, and thus may be considered for MS. The therapeutic effect of DBS begins intraoperatively, and can extend to the postoperative months. This treatment also partly improves activities of daily living scores without mortality or morbidity.58 If tremors have a poor response to one DBS electrode, two electrodes may improve results.59 However, DBS for MS tremor has often produced an unreliable and inconsistent therapeutic intervention, and has to be evaluated individually with caution.60
Spinal cord stimulation significantly improves bladder dysfunction, pain, and possibly spasticity in MS patients.61 Epidural spinal cord stimulation by means of chronically implanted electrodes can provide significant long-term pain relief with improved quality of life and employment for persons with lower-limb pain caused by MS.62
Although disease-modifying drugs are considered mainly to suppress autoimmune activity to prevent relapse of MS, some agents have also shown neurorestorative effects. Glatiramer acetate increased BDNF production in a rat model of optic nerve damage.63 Laquinimod significantly and persistently increased BDNF serum levels in patients with MS.64 Neurological impairment of patients who received alemtuzumab improved for up to 6 months, and then remained stable for at least 3 years. Cultures of peripheral blood mononuclear cells from those patients contained high concentrations of BDNF, PDGF, and ciliary neurotrophic factor.65 Both preclinical and clinical studies have demonstrated that dimethyl fumarate reduced the relapse rate and MRI activity of inflammation, and preserved myelin, axons, and neurons via the antioxidant-response pathway.66
Neuromodulation of the peripheral nervous system
The implantation of a sacral neurostimulator device in patients with MS has significantly decreased urgency, frequency, upper urinary tract infections, and fever, slightly improved bowel function, and improved quality of life and emotional well-being.67 Other clinical studies have also demonstrated that peripheral electrical stimulation of the posterior tibial nerve improves clinical and urodynamic outcome and provides long-term efficacy though suppressing neurogenic detrusor overactivity in MS patients.68,69 However, MS patients with urinary retention due to detrusor underactivity are not suitable for this treatment.70 The LION (laparoscopic implantation of neuroprosthesis) procedure on the sacral plexus is worth trying if the classical percutaneous technique has been unsuccessful.71
The gait of MS patients has been shown to significantly improve with the combination of exercise and a device that electrically stimulated the tongue to enhance the plasticity of the brain.72
Functional electrical stimulation (FES) produces a contraction in a paralyzed or weak muscle that can improve function through electrical excitation of the innervating nerve. FES can be used clinically to manage foot drop in people suffering from diverse neurological conditions. Patients with MS who underwent FES had significantly improved walking speed and a significant reduction in the physiological cost of gait.73 However, a randomized trial demonstrated that the effects of exercise therapy for people with secondary progressive MS were superior to single-channel common peroneal nerve stimulation on objective aspects of gait in MS.74
Transcutaneous electrical nerve stimulation may relieve segmental pain by evoking paresthesia in the painful area, while central neurostimulation in contrast has been largely unsuccessful.75
Other approaches
Few studies have suggested that acupuncture can improve MS-related symptoms, such as fatigue, spasticity, and pain. Conclusions on the efficacy of this intervention must await further research, owing to the lack of statistical rigor and poor design in studies to date.76 In one randomized controlled pilot trial, MS patients received massage therapy, exercise therapy, or combined massage–exercise therapy, while the control group continued their standard medical care. The results indicated that massage therapy resulted in significantly larger improvement in pain reduction, dynamic balance, and walking speed than exercise therapy. Patients receiving combined massage–exercise therapy showed significantly larger improvement in pain reduction than those in exercise therapy.77
The exact mechanisms of action of neurostimulation (neuromodulation) remain unclear. They may act on different aspects of the CNS by modulating the activities of neurotransmitters and other neuroactive compounds, enhancing cortical reorganization, inducing network compensation, or increasing blood flow for promoting functional recovery in MS patients.78–80
Neurorehabilitation
Considerable evidence has indicated that neurorehabilitation can improve symptoms, functional capacities, and social participation.81,82 Preliminary evidence, indicated in the following sections, suggests that efficacious neurorehabilitation may have a neuromodulatory effect. Rehabilitation interventions should be considered early for maintaining functional capacity.83
Physical exercise
Neurorehabilitation studies in MS have used a large range of exercises, including strengthening exercises with weight lifting, aerobics exercises on the bicycle or treadmill, and various balancing and stretching exercises. Cessation of exercise may cause recurrence of symptoms. Continuous rather than short-period exercises may be needed to support effects in patients.84
Fatigue is a common symptom of MS, with negative effects on various components of the patient’s health and well-being. Clinical evidence suggests that exercise is superior to medication for reducing the effects of fatigue.85 Rehabilitation interventions may also be effective in improving impairment or disability, even in MS patients who have experienced a relapse.86
MS patients with severely impaired ambulation have improved their muscle strength, spasticity, endurance, balance, walking speed, and quality of life after finishing locomotor body weight-supported treadmill training without fatigue or other adverse effects.87 With or without locomotor assistance, body weight-supported treadmill training can improve gait impairment in patients with MS.88 In a randomized trial, researchers concluded that robot-assisted gait training is feasible and safe, and may be an effective additional therapeutic option for MS patients with severe walking disabilities.89 However, robot-assisted step training was no better than overground walking training in patients in another randomized study.90 Cycling progressive resistance training may improve balance, fatigue, and depression, and reduce fear of falling in patients with MS without worsening MS signs and symptoms.91
Constraint-induced movement therapy (CIMT) is a physical training method that has been recently adapted from the stroke field for use in MS to overcome learned nonuse, the behaviorally conditioned suppression of paretic limb use for real-life activities. CIMT combines massed practice training of the more impaired limb(s), restraint of compensatory behaviors, shaping on training tasks, and incorporating behavioral procedures to reinforce transfer of treatment effects from the clinic to the real world (behavioral contracting, home practice, maintaining an activities diary, daily problem-solving discussions with the therapist).92 CIMT has been shown to be safe and well tolerated for progressive MS patients with either upper-extremity hemiparesis or impaired lower-extremity use.93,94 Improvements in real-world limb use may remain for as much as 4–5 years following the single course (2 or 3 weeks) of treatment.94,95 Moreover, a recent randomized controlled trial of upper-extremity CIMT versus a program of holistic physical complementary and alternative medicine treatments (massage, yoga, relaxation exercises, aquatic therapy) indicated superiority of CIMT not only for improving real-world paretic arm use but also for inducing increased cortical gray-matter structure on MRI,96 thus suggesting that CIMT may have a neuromodulatory effect by stimulating structural CNS plasticity.
Each MS patient has his or her own unique physical characteristics and rehabilitation needs. As a result, adaptive personalized training should be selected to meet every patient’s rehabilitation needs.97 Physical exercise in patients with MS may contribute to neurorestoration by upregulating expression of neurotrophic BDNF, IGF, NGF, and others, which may help neuroregeneration, synaptic plasticity, neural protection, and anti-inflammatory effects.98–100
Cognitive rehabilitation
Fifty percent of patients with MS are estimated to have cognitive impairments resulting in considerable decline in quality of life. Cognitive intervention has been recommended to complement pharmacological treatments. Attention, information processing, and executive functions have been effectively improved in relapsing–remitting MS patients who received intensive computer-assisted cognitive rehabilitation for 3 months.101 However, systematic reviews and meta-analyses have shown a lack of agreement concerning the efficacy of cognitive interventions for MS.102,103
Conclusion
This review briefly mentioned neurorestorative treatments in MS (Table 2). The treatment of MS remains a great challenge today. Conventional strategies, including steroids, disease-modifying medications, and symptomatic treatments (eg, baclofen, dalfampridine) may influence the course of MS, partly relieve the symptoms, or slow the neurodegenerative process, but they cannot halt neurodegeneration. Neurorestorative strategies not only improve the clinical course and relieve the symptoms but also promote the remodeling of CNS structure and function by neuroprotection, neuroregeneration, and immunomodulation. Early use of disease-modifying medications in combination with neurorestorative therapies may be expected to improve the prognosis of patients with severe disability. Neurorestorative treatments, alone or combined with these different measures, should be further explored in clinical practice to provide the patient with the best help and improve quality of life.
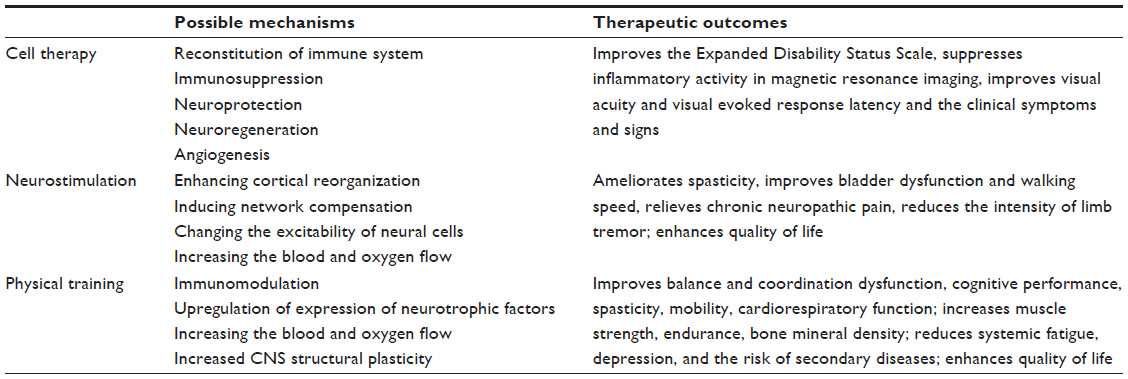 | Table 2 Neurorestorative therapies for multiple sclerosis |
Disclosure
The authors report no conflicts of interest in this work.
References
Tullman MJ. Overview of the epidemiology, diagnosis, and disease progression associated with multiple sclerosis. Am J Manag Care. 2013;19:S15–S20. | |
Lucchinetti C, Brück W, Parisi J, Scheithauer B, Rodriguez M, Lassmann H. Heterogeneity of multiple sclerosis lesions: implications for the pathogenesis of demyelination. Ann Neurol. 2000;47:707–717. | |
Frohman EM, Racke MK, Raine CS. Multiple sclerosis – the plaque and its pathogenesis. N Engl J Med. 2006;354:942–955. | |
Sá MJ. Physiopathology of symptoms and signs in multiple sclerosis. Arq Neuropsiquiatr. 2012;70:733–740. | |
Sinha A, Bagga A. Pulse steroid therapy. Indian J Pediatr. 2008;75: 1057–1066. | |
Minagar A. Current and future therapies for multiple sclerosis. Scientifica. 2013;2013:249101. | |
Bass B, Weinshenker B, Rice GP, et al. Tizanidine versus baclofen in the treatment of spasticity in patients with multiple sclerosis. Can J Neurol Sci. 1988;15:15–19. | |
Tullman MJ. A review of current and emerging therapeutic strategies in multiple sclerosis. Am J Manag Care. 2013;19:S21–S27. | |
Nicholas RS, Friede T, Hollis S, Young CA. Anticholinergics for urinary symptoms in multiple sclerosis. Cochrane Database Syst Rev. 2009:CD004193. | |
Cameron MH, Bethoux F, Davis N, Frederick M. Botulinum toxin for symptomatic therapy in multiple sclerosis. Curr Neurol Neurosci Rep. 2014;14:463. | |
Leandri M. Therapy of trigeminal neuralgia secondary to multiple sclerosis. Expert Rev Neurother. 2003;3:661–671. | |
Solaro C, Messmer Uccelli M, Uccelli A, Leandri M, Mancardi GL. Low-dose gabapentin combined with either lamotrigine or carbamazepine can be useful therapies for trigeminal neuralgia in multiple sclerosis. Eur Neurol. 2000;44:45–48. | |
Solaro C, Restivo D, Mancardi GL, Tanganelli P. Oxcarbazepine for treating paroxysmal painful symptoms in multiple sclerosis: a pilot study. Neurol Sci. 2007;28:156–158. | |
Ledinek AH, Sajko MC, Rot U. Evaluating the effects of amantadin, modafinil and acetyl-L-carnitine on fatigue in multiple sclerosis – result of a pilot randomized, blind study. Clin Neurol Neurosurg. 2013;115 Suppl 1:S86–S89. | |
Christodoulou C, Melville P, Scherl WF, et al. Effects of donepezil on memory and cognition in multiple sclerosis. J Neurol Sci. 2006;245:127–136. | |
O’Carroll CB, Woodruff BK, Locke DE, et al. Is donepezil effective for multiple sclerosis-related cognitive dysfunction? A critically appraised topic. Neurologist. 2012;18:51–54. | |
Saiz A, Carreras E, Berenguer J, et al. MRI and CSF oligoclonal bands after autologous hematopoietic stem cell transplantation in MS. Neurology. 2001;56:1084–1089. | |
Saiz A, Blanco Y, Carreras E, et al. Clinical and MRI outcome after autologous hematopoietic stem cell transplantation in MS. Neurology. 2004;62:282–284. | |
Roccatagliata L, Rocca M, Valsasina P, et al. The long-term effect of AHSCT on MRI measures of MS evolution: a five-year follow-up study. Mult Scler. 2007;13:1068–1070. | |
Fassas A, Kimiskidis VK, Sakellari I, et al. Long-term results of stem cell transplantation for MS: a single-center experience. Neurology. 2011;76:1066–1070. | |
Mancardi GL, Sormani MP, Di Gioia M, et al. Autologous haematopoietic stem cell transplantation with an intermediate intensity conditioning regimen in multiple sclerosis: the Italian multi-centre experience. Mult Scler. 2012;18:835–842. | |
Burman J, Iacobaeus E, Svenningsson A, et al. Autologous haematopoietic stem cell transplantation for aggressive multiple sclerosis: the Swedish experience. J Neurol Neurosurg Psychiatry. 2014;85:1116–1121. | |
Xu J, Ji BX, Su L, et al. Clinical outcome of autologous peripheral blood stem cell transplantation in opticospinal and conventional forms of secondary progressive multiple sclerosis in a Chinese population. Ann Hematol. 2011;90:343–348. | |
Atkins HL, Freedman MS. Hematopoietic stem cell therapy for multiple sclerosis: top 10 lessons learned. Neurotherapeutics. 2013;10:68–76. | |
Saccardi R, Di Gioia M, Bosi A. Haematopoietic stem cell transplantation for autoimmune disorders. Curr Opin Hematol. 2008;15:594–600. | |
Karussis D, Karageorgiou C, Vaknin-Dembinsky A, et al. Safety and immunological effects of mesenchymal stem cell transplantation in patients with multiple sclerosis and amyotrophic lateral sclerosis. Arch Neurol. 2010;67:1187–1194. | |
Connick P, Kolappan M, Crawley C, et al. Autologous mesenchymal stem cells for the treatment of secondary progressive multiple sclerosis: an open-label phase 2A proof-of-concept study. Lancet Neurol. 2012;11: 150–156. | |
Yamout B, Hourani R, Salti H, et al. Bone marrow mesenchymal stem cell transplantation in patients with multiple sclerosis: a pilot study. J Neuroimmunol. 2010;227:185–189. | |
Mohyeddin Bonab M, Yazdanbakhsh S, Lotfi J, et al. Does mesenchymal stem cell therapy help multiple sclerosis patients? Report of a pilot study. Iran J Immunol. 2007;4:50–57. | |
Liang J, Zhang H, Hua B, et al. Allogeneic mesenchymal stem cells transplantation in treatment of multiple sclerosis. Mult Scler. 2009;15: 644–646. | |
Hou ZL, Liu Y, Mao XH, et al. Transplantation of umbilical cord and bone marrow-derived mesenchymal stem cells in a patient with relapsing-remitting multiple sclerosis. Cell Adh Migr. 2013;7:404–407. | |
Chen L, Huang HY, Wang R, et al. Transplantation of olfactory ensheathing cells for multiple sclerosis: one case report. Chin J Neurosurg Dis Res. 2004;3:60. Chinese. | |
Huang HY, Chen L, Xi HT, Wang QM, Liu YC, Zhang F. Olfactory ensheathing cells transplantation for central nervous system diseases in 1255 patients. [Chinese General of reparative and Reconstructive surgery]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2009;23:14–20. Chinese. | |
Ben-Hur T. Cell therapy for multiple sclerosis. Neurotherapeutics. 2011;8:625–642. | |
Einstein O, Fainstein N, Vaknin I, et al. Neural precursors attenuate autoimmune encephalomyelitis by peripheral immunosuppression. Ann Neurol. 2007;61:209–218. | |
Stagg J, Galipeau J. Mechanisms of immune modulation by mesenchymal stromal cells and clinical translation. Curr Mol Med. 2013;13:856–867. | |
Aggarwal S, Pittenger MF. Human mesenchymal stem cells modulate allogeneic immune cell responses. Blood. 2005;105:1815–1822. | |
Sun L, Wang D, Liang J, et al. Umbilical cord mesenchymal stem cell transplantation in severe and refractory systemic lupus erythematosus. Arthritis Rheum. 2010;62:2467–2475. | |
Bai L, Lennon DP, Eaton V, et al. Human bone marrow-derived mesenchymal stem cells induce Th2-polarized immune response and promote endogenous repair in animal models of multiple sclerosis. Glia. 2009;57:1192–1203. | |
Lu P, Jones LL, Snyder EY, Tuszynski MH. Neural stem cells constitutively secrete neurotrophic factors and promote extensive host axonal growth after spinal cord injury. Exp Neurol. 2003;181:115–129. | |
Zwart I, Hill AJ, Al-Allaf F, et al. Umbilical cord blood mesenchymal stromal cells are neuroprotective and promote regeneration in a rat optic tract model. Exp Neurol. 2009;216:439–448. | |
Arien-Zakay H, Lecht S, Bercu MM, et al. Neuroprotection by cord blood neural progenitors involves antioxidants, neurotrophic and angiogenic factors. Exp Neurol. 2009;216:83–94. | |
Hsieh JY, Wang HW, Chang SJ, et al. Mesenchymal stem cells from human umbilical cord express preferentially secreted factors related to neuroprotection, neurogenesis, and angiogenesis. PLoS One. 2013;8:e72604. | |
Goodell MA, Jackson KA, Majka SM, et al. Stem cell plasticity in muscle and bone marrow. Ann N Y Acad Sci. 2001;938:208–218. | |
Nakano-Doi A, Nakagomi T, Fujikawa M, et al. Bone marrow mononuclear cells promote proliferation of endogenous neural stem cells through vascular niches after cerebral infarction. Stem Cells. 2010;28: 1292–1302. | |
Sharma A, Gokulchandran N, Sane H, et al. Autologous bone marrow mononuclear cell therapy for autism: an open label proof of concept study. Stem Cells Int. 2013;2013:623875. | |
Sharma A, Sane H, Gokulchandran N, et al. Autologous bone marrow mononuclear cells intrathecal transplantation in chronic stroke. Stroke Res Treat. 2014;2014:234095. | |
Sakas DE, Panourias IG, Simpson BA. An introduction to neural networks surgery, a field of neuromodulation which is based on advances in neural networks science and digitised brain imaging. Acta Neurochir Suppl. 2007;97:3–13. | |
Minassian K, Hofstoetter U, Tansey K, Mayr W. Neuromodulation of lower limb motor control in restorative neurology. Clin Neurol Neurosurg. 2012;114:489–497. | |
Mori F, Codecà C, Kusayanagi H, et al. Effects of intermittent theta burst stimulation on spasticity in patients with multiple sclerosis. Eur J Neurol. 2010;17:295–300. | |
Centonze D, Koch G, Versace V, et al. Repetitive transcranial magnetic stimulation of the motor cortex ameliorates spasticity in multiple sclerosis. Neurology. 2007;68:1045–1050. | |
Koch G, Rossi S, Prosperetti C, et al. Improvement of hand dexterity following motor cortex rTMS in multiple sclerosis patients with cerebellar impairment. Mult Scler. 2008;14:995–998. | |
Centonze D, Petta F, Versace V, et al. Effects of motor cortex rTMS on lower urinary tract dysfunction in multiple sclerosis. Mult Scler. 2007;13:269–271. | |
Haupts MR, Daum S, Ahle G, Holinka B, Gehlen W. Transcranial magnetic stimulation as a provocation for epileptic seizures in multiple sclerosis. Mult Scler. 2004;10:475–476. | |
Wassermann EM. Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5–7, 1996. Electroencephalogr Clin Neurophysiol. 1998;108:1–16. | |
Lefaucheur JP, André-Obadia N, Antal A, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin Neurophysiol. 2014;125:2150–2206. | |
Tanei T, Kajita Y, Noda H, et al. Efficacy of motor cortex stimulation for intractable central neuropathic pain: comparison of stimulation parameters between post-stroke pain and other central pain. Neurol Med Chir (Tokyo). 2011;51:8–14. | |
Mandat T, Koziara H, Tutaj M, Rola R, Bonicki W, Nauman P. Thalamic deep brain stimulation for tremor among multiple sclerosis patients. Neurol Neurochir Pol. 2010;44:542–545. | |
Foote KD, Seignourel P, Fernandez HH, et al. Dual electrode thalamic deep brain stimulation for the treatment of posttraumatic and multiple sclerosis tremor. Neurosurgery. 2006;58:ONS-280-5. | |
Nandi D, Aziz TZ. Deep brain stimulation in the management of neuropathic pain and multiple sclerosis tremor. J Clin Neurophysiol. 2004;21:31–39. | |
Illis LS, Read DJ, Sedgwick EM, Tallis RC. Spinal cord stimulation in the United Kingdom. J Neurol Neurosurg Psychiatry. 1983;46:299–304. | |
Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic benign pain: challenges in treatment planning and present status, a 22-year experience. Neurosurgery. 2006;58:481–496. | |
Kipnis J, Yoles E, Porat Z, et al. T cell immunity to copolymer 1 confers neuroprotection on the damaged optic nerve: possible therapy for optic neuropathies. Proc Natl Acad Sci U S A. 2000;97:7446–7451. | |
Thöne J, Ellrichmann G, Seubert S, et al. Modulation of autoimmune demyelination by laquinimod via induction of brain-derived neurotrophic factor. Am J Pathol. 2012;180:267–274. | |
Jones JL, Anderson JM, Phuah CL, et al. Improvement in disability after alemtuzumab treatment of multiple sclerosis is associated with neuroprotective autoimmunity. Brain. 2010;133:2232–2247. | |
Linker RA, Lee DH, Ryan S, et al. Fumaric acid esters exert neuroprotective effects in neuroinflammation via activation of the Nrf2 antioxidant pathway. Brain. 2011;134:678–692. | |
Minardi D, Muzzonigro G. Lower urinary tract and bowel disorders and multiple sclerosis: role of sacral neuromodulation: a preliminary report. Neuromodulation. 2005;8:176–181. | |
Kabay S, Kabay SC, Yucel M, et al. The clinical and urodynamic results of a 3-month percutaneous posterior tibial nerve stimulation treatment in patients with multiple sclerosis-related neurogenic bladder dysfunction. Neurourol Urodyn. 2009;28:964–968. | |
Zecca C, Digesu GA, Robshaw P, Singh A, Elneil S, Gobbi C. Maintenance percutaneous posterior nerve stimulation for refractory lower urinary tract symptoms in patients with multiple sclerosis: an open label, multicenter, prospective study. J Urol. 2014;191:697–702. | |
Minardi D, Muzzonigro G. Sacral neuromodulation in patients with multiple sclerosis. World J Urol. 2012;30:123–128. | |
Possover M. The laparoscopic implantation of neuroprothesis to the sacral plexus for therapy of neurogenic bladder dysfunctions after failure of percutaneous sacral nerve stimulation. Neuromodulation. 2010;13: 141–144. | |
Tyler ME, Kaczmarek KA, Rust KL, Subbotin AM, Skinner KL, Danilov YP. Non-invasive neuromodulation to improve gait in chronic multiple sclerosis: a randomized double blind controlled pilot trial. J Neuroeng Rehabil. 2014;11:79. | |
Paul L, Rafferty D, Young S, Miller L, Mattison P, McFadyen A. The effect of functional electrical stimulation on the physiological cost of gait in people with multiple sclerosis. Mult Scler. 2008;14:954–961. | |
Barrett CL, Mann GE, Taylor PN, Strike P. A randomized trial to investigate the effects of functional electrical stimulation and therapeutic exercise on walking performance for people with multiple sclerosis. Mult Scler. 2009;15:493–504. | |
Sjölund BH. Pain and rehabilitation after spinal cord injury: the case of sensory spasticity? Brain Res Rev. 2002;40:250–256. | |
Karpatkin HI, Napolione D, Siminovich-Blok B. Acupuncture and multiple sclerosis: a review of the evidence. Evid Based Complement Alternat Med. 2014;2014:972935. | |
Negahban H, Rezaie S, Goharpey S. Massage therapy and exercise therapy in patients with multiple sclerosis: a randomized controlled pilot study. Clin Rehabil. 2013;27:1126–1136. | |
Rothwell JC. Techniques and mechanisms of action of transcranial stimulation of the human motor cortex. J Neurosci Methods. 1997;74: 113–122. | |
Wildenberg JC, Tyler ME, Danilov YP, Kaczmarek KA, Meyerand ME. Electrical tongue stimulation normalizes activity within the motion-sensitive brain network in balance-impaired subjects as revealed by group independent component analysis. Brain Connect. 2011;1:255–265. | |
Karas PJ, Mikell CB, Christian E, Liker MA, Sheth SA. Deep brain stimulation: a mechanistic and clinical update. Neurosurg Focus. 2013;35:E1. | |
Latimer-Cheung AE, Pilutti LA, Hicks AL, et al. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults with multiple sclerosis: a systematic review to inform guideline development. Arch Phys Med Rehabil. 2013;94:1800–1828. | |
Sá MJ. Exercise therapy and multiple sclerosis: a systematic review. J Neurol. 2014;261:1651–1661. | |
Beer S, Khan F, Kesselring J. Rehabilitation interventions in multiple sclerosis: an overview. J Neurol. 2012;259:1994–2008. | |
Sangelaji B, Nabavi SM, Estebsari F, et al. Effect of combination exercise therapy on walking distance, postural balance, fatigue and quality of life in multiple sclerosis patients: a clinical trial study. Iran Red Crescent Med J. 2014;16:e17173. | |
Asano M, Finlayson ML. Meta-analysis of three different types of fatigue management interventions for people with multiple sclerosis: exercise, education, and medication. Mult Scler Int. 2014;2014:798285. | |
Asano M, Raszewski R, Finlayson M. Rehabilitation interventions for the management of multiple sclerosis relapse: a short scoping review. Int J MS Care. 2014;16:99–104. | |
Giesser B, Beres-Jones J, Budovitch A, Herlihy E, Harkema S. Locomotor training using body weight support on a treadmill improves mobility in persons with multiple sclerosis: a pilot study. Mult Scler. 2007;13:224–231. | |
Lo AC, Triche EW. Improving gait in multiple sclerosis using robot-assisted, body weight supported treadmill training. Neurorehabil Neural Repair. 2008;22:661–671. | |
Schwartz I, Sajin A, Moreh E, et al. Robot-assisted gait training in multiple sclerosis patients: a randomized trial. Mult Scler. 2012;18: 881–890. | |
Vaney C, Gattlen B, Lugon-Moulin V, et al. Robotic-assisted step training (Lokomat) not superior to equal intensity of over-ground rehabilitation in patients with multiple sclerosis. Neurorehabil Neural Repair. 2012;26:212–221. | |
Çakit BD, Nacir B, Genç H, et al. Cycling progressive resistance training for people with multiple sclerosis: a randomized controlled study. Am J Phys Med Rehabil. 2010;89:446–457. | |
Morris DM, Taub E, Mark VW. Constraint-induced movement therapy (CI therapy): characterizing the intervention protocol. Eura Medicophys. 2006;42:257–268. | |
Mark V, Taub E, Bashir K, et al. Constraint-induced movement therapy can improve hemiparetic progressive multiple sclerosis. Preliminary findings. Mult Scler. 2008;14:992–994. | |
Mark VW, Taub E, Uswatte G, et al. Constraint-induced movement therapy for the lower extremities in multiple sclerosis: case series with 4-year follow-up. Arch Phys Med Rehabil. 2013;94:753–760. | |
Mark VW, Taub E, Uswatte G, et al. Constraint-induced movement therapy for multiple sclerosis: up to 5-year follow-up. Int J MS Care. 2012;14:9. | |
Mark V, Taub E, Uswatte G, Cutter G, Morris D, McKay S, et al. Randomized controlled trial of CI therapy for progressive MS: increased real-world function and neuroplasticity on MRI [abstract]. Neurology. 2014;82:007. | |
Octavia JR, Coninx K. Adaptive personalized training games for individual and collaborative rehabilitation of people with multiple sclerosis. Biomed Res Int. 2014;2014:345728. | |
White LJ, Castellano V. Exercise and brain health – implications for multiple sclerosis: Part 1 – neuronal growth factors. Sports Med. 2008;38:91–100. | |
White LJ, Castellano V. Exercise and brain health – implications for multiple sclerosis: Part II – immune factors and stress hormones. Sports Med. 2008;38:179–186. | |
Heesen C, Romberg A, Gold S, Schulz KH. Physical exercise in multiple sclerosis: supportive care or a putative disease-modifying treatment. Expert Rev Neurother. 2006;6:347–355. | |
Mattioli F, Stampatori C, Zanotti D, Parrinello G, Capra R. Efficacy and specificity of intensive cognitive rehabilitation of attention and executive functions in multiple sclerosis. J Neurol Sci. 2010;288: 101–105. | |
Magalhães R, Alves J, Thomas RE, et al. Are cognitive interventions for multiple sclerosis effective and feasible? Restor Neurol Neurosci. 2014;32:623–638. | |
das Nair R, Ferguson H, Stark DL, Lincoln NB. Memory rehabilitation for people with multiple sclerosis. Cochrane Database Syst Rev. 2012;3:CD008754. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.