")
Back to Journals » Cancer Management and Research » Volume 12
Clinical Analysis of Risk Factors for Cervical Lymph Node Metastasis in Papillary Thyroid Microcarcinoma: A Retrospective Study of 3686 Patients
Authors Song J, Yan T , Qiu W, Fan Y , Yang Z
Received 17 February 2020
Accepted for publication 24 March 2020
Published 9 April 2020 Volume 2020:12 Pages 2523—2530
DOI https://doi.org/10.2147/CMAR.S250163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jianlu Song,* Ting Yan,* Wangwang Qiu, Youben Fan, Zhili Yang
Center of Thyroid and Parathyroid, Department of Thyroid, Parathyroid, Breast and Hernia Surgery, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai 200233, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhili Yang; Youben Fan
Center of Thyroid and Parathyroid, Department of Thyroid, Parathyroid, Breast and Hernia Surgery, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai 200233, People’s Republic of China
Tel +86 21 24058412
Fax +86 21 24058933
Email [email protected]; [email protected]
Purpose: To investigate the risk factors for cervical lymph node metastasis (LNM) in papillary thyroid microcarcinoma (PTMC).
Patients and Methods: In total, 3686 patients with PTMC who underwent initial surgery in Shanghai Jiao Tong University affiliated Sixth People’s Hospital from January 2010 to December 2019 were retrospectively analyzed. Univariate and multivariate analyses were conducted to identify risk factors associated with cervical LNM.
Results: Male gender [odds ratio (OR) =1.420, P < 0.001], age < 55 years (OR =2.128, P < 0.001), tumor size > 6.5 mm (OR =2.112, P < 0.001), lymphovascular invasion (LVI) (OR =2.110, P =0.016), multifocality (OR =1.358, P =0.022), extrathyroidal extension (ETE) (OR =1.598, P < 0.001), and lateral LNM (LLNM) (OR =6.383, P < 0.001) served as independent risk factors for central LNM (CLNM). Moreover, male gender (OR =1.668, P =0.001), tumor size > 6.5 mm (OR =2.223, P < 0.001), chronic lymphocytic thyroiditis (OR =1.402, P =0.021), LVI (OR =4.582, P < 0.001), ETE (OR =1.393, P=0.023), and CLNM (OR =6.212, P < 0.001) served as independent risk factors for LLNM. Furthermore, solitary PTMC with lesions in the upper third of the thyroid gland were more associated with LLNM than lesions in the other regions.
Conclusion: This study suggests that meticulous evaluation of risk factors associated with LNM is required in order to guide the surgical treatment of PTMC patients in clinical practice.
Keywords: papillary thyroid microcarcinoma, predictors, central lymph node metastasis, lateral lymph node metastasis, extrathyroidal extension
Introduction
Papillary thyroid microcarcinoma (PTMC) is defined by the World Health Organization as a papillary thyroid carcinoma (PTC) measuring ≤10 mm in diameter. In recent years, the incidence of PTMC has increased substantially, and is estimated to account for more than 50% of new cases of thyroid cancer.1 Although PTMC has an indolent clinical course with excellent prognosis, some cases are accompanied by high-risk features at the time of diagnosis, such as extrathyroidal extension (ETE) and lymph node metastasis (LNM).2,3
Previous studies have shown that the incidence rate of central LNM (CLNM) in PTMC is approximately 23–64.1%, and the incidence rate of lateral LNM (LLNM) in PTMC is approximately 3.7–44.5%.4–6 Existing guidelines recommend active surveillance for low-risk PTMC, and immediate surgery for those with high-risk features. However, whether prophylactic central lymph node dissection (CLND) should be performed routinely for clinically node-negative (cN0) PTMC patients is still uncertain, because of the lack of substantial evidence showing any survival benefit for these patients.2,3 Therefore, determining the risk factors associated with LNM is of great significance to determine surgical strategies.
In this study, we retrospectively analyzed clinicopathological features of PTMC patients to identify the risk factors for cervical LNM, which could improve the clinical management of PTMC.
Patients and Methods
Patient Selection
Demographic, operative, clinical, and pathological data from medical records of PTMC patients who underwent surgery at Shanghai Jiao Tong University Affiliated Sixth People’s Hospital from January 2010 to December 2019 were reviewed. For inclusion in the study, a patient had to have a complete medical record, no history of neck radiotherapy or thyroidectomy, and a postoperative pathological diagnosis with PTMC. Patients with mixed PTMC (PTMC with other types of thyroid cancer), or with a history of other malignancies, were excluded from the study. Ultimately, 3686 patients were included in this study. All patients underwent preoperative neck ultrasonography (US) and fiberoptic laryngoscopy. Where preoperative findings indicated possible LLNM, enhanced computed tomography scanning and fine-needle aspiration cytology (FNAC) were usually performed to evaluate suspect lymph nodes (LNs). This retrospective study was approved by the Ethics Committee at the Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. Each patient signed a written informed consent to use their data for research, and that all data was maintained with confidentiality.
Surgical Procedures
All patients underwent CLND (level VI) either therapeutic or prophylactic CLND, which is routinely recommended in China.7 Total thyroidectomy was performed for PTMC patients with bilaterality, gross ETE (gETE), bilateral cervical LNM, or other high-risk features, who would potentially require radioactive iodine ablation therapy. Lateral lymph node dissection (LLND), including neck dissection of level II–IV (level I and V were only dissected when metastatic LNs were present in these compartments), was performed in patients for whom LLNM was confirmed by preoperative FNAC and washout thyroglobulin level.
Histopathological Examination
Surgical specimens were meticulously examined by two experienced pathologists, and the following histopathologic features were determined and assessed: pathological subtypes, chronic lymphocytic thyroiditis (CLT), tumor size (measured as the diameter of the largest lesion), multifocality (defined as the presence of two or more lesions in the thyroid), bilaterality, LVI (defined as the invasion of intracapsular blood or lymphatic vessels), ETE (including capsular invasion), LNM, and the size of positive LNs. Because the diagnosis of ETE is controversial (the true capsule of the thyroid gland is not well-defined), we defined ETE as capsular invasion and extracapsular extension into perithyroid tissue, such as fibroadipose tissue and strap muscle. Tumors were staged in accordance with the eighth edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual.
Statistical Analysis
Continuous variables are presented as a median value with an interquartile range (IQR), and categorical variables are presented as a frequency and percentage. Either Pearson’s chi-squared test or Fisher’s test was used to compare categorical variables. Multivariate logistic regression analysis was performed to assess independent risk factors for cervical LNM, using variables with P <0.05 from univariate analysis. Receiver operating characteristic curve (ROC) analysis was used to determine optimal cutoff points for tumor size and the amount of involved central LNs necessary to identify the risk of CLNM and LLNM, respectively. Statistical significance for two-tailed tests was defined as P <0.05. All statistical analyses were performed using SPSS 26.0 software (IBM Corp., Armonk, NY, USA).
Results
Clinicopathological Characteristics of 3686 PTMC Patients
The clinicopathological characteristics of the 3686 PTMC patients are summarized in Table 1. Conventional open surgery was performed on 3331 (90.4%) patients, and endoscopic thyroidectomy, either via the oral vestibular approach or the areola approach, was performed on 355 (9.6%) patients. Lobectomy was performed in 1856 (50.4%) patients, near-total thyroidectomy in 588 (16.0%) patients, and total thyroidectomy in 1242 (33.7%) patients. All patients underwent CLND, with a median of four LNs dissected. The incidence of CLNM was 30.2% (1114 cases), and the median of LNs in these patients was two. LLNM was present in 256 (6.9%) patients, including 18 cases with bilateral LLNM and 62 cases with skip metastasis (LLNM without CLNM). Six patients presented with distant metastasis, of which three had lung metastasis and three had bone metastasis.
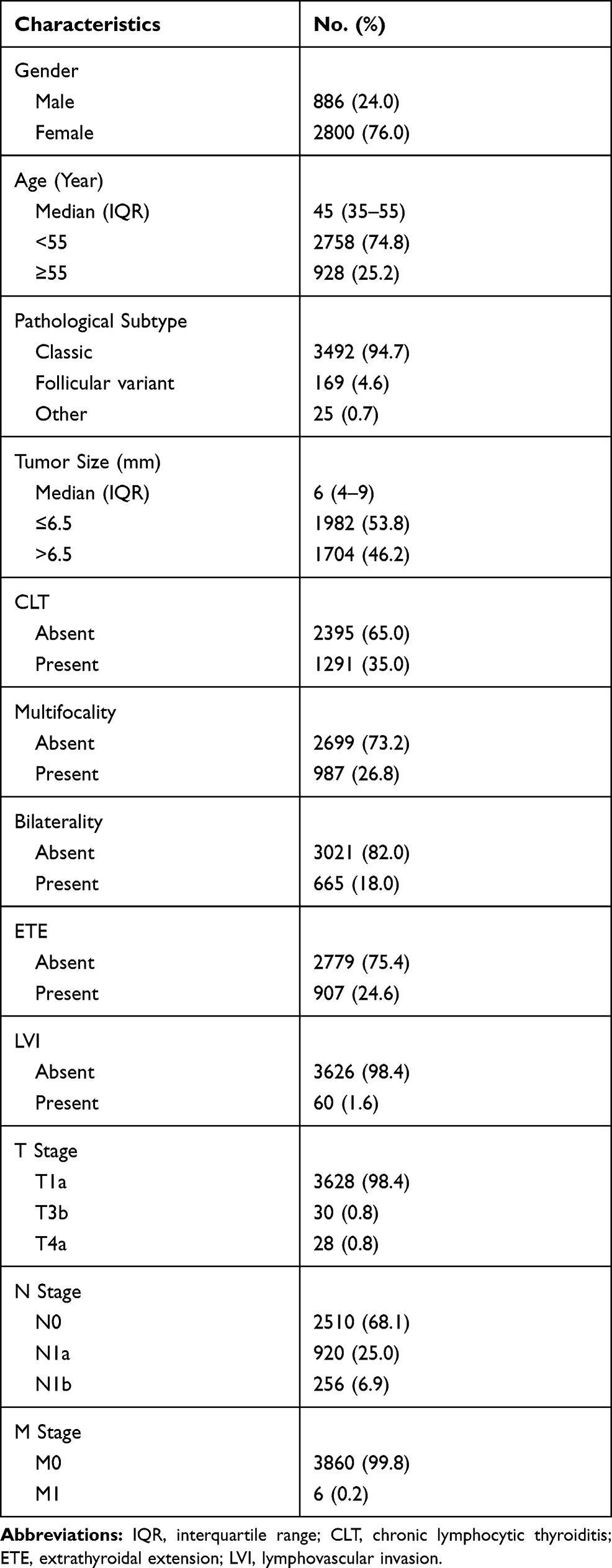 |
Table 1 Clinicopathological Characteristics of 3686 PTMC Patients |
Risk Factors for CLNM
ROC curve analysis showed that the optimal cutoff point for primary tumor size used to determine whether PTMC patients had CLNM was 6.5 mm (area =0.646, standard error =0.010, asymptotic significance =0.000, 95% confidence interval =0.627–0.665).
The risk factors for CLNM were evaluated via univariate and multivariate analyses (Table 2). Univariate analysis showed that male gender, age <55 years, tumor size greater than 6.5 mm, LVI, multifocality, bilaterality, ETE, and LLNM were significantly associated with CLNM (all P <0.001). Using multivariate analysis, male gender [odds ratio (OR) =1.420, P <0.001], age <55 years (OR =2.128, P <0.001), tumor size >6.5 mm (OR =2.112, P <0.001), LVI (OR =2.110, P =0.016), multifocality (OR =1.358, P =0.022), ETE (OR =1.598, P <0.001), and LLNM (OR =6.383, P <0.001) were determined to be independent risk factors for CLNM for patients with PTMC.
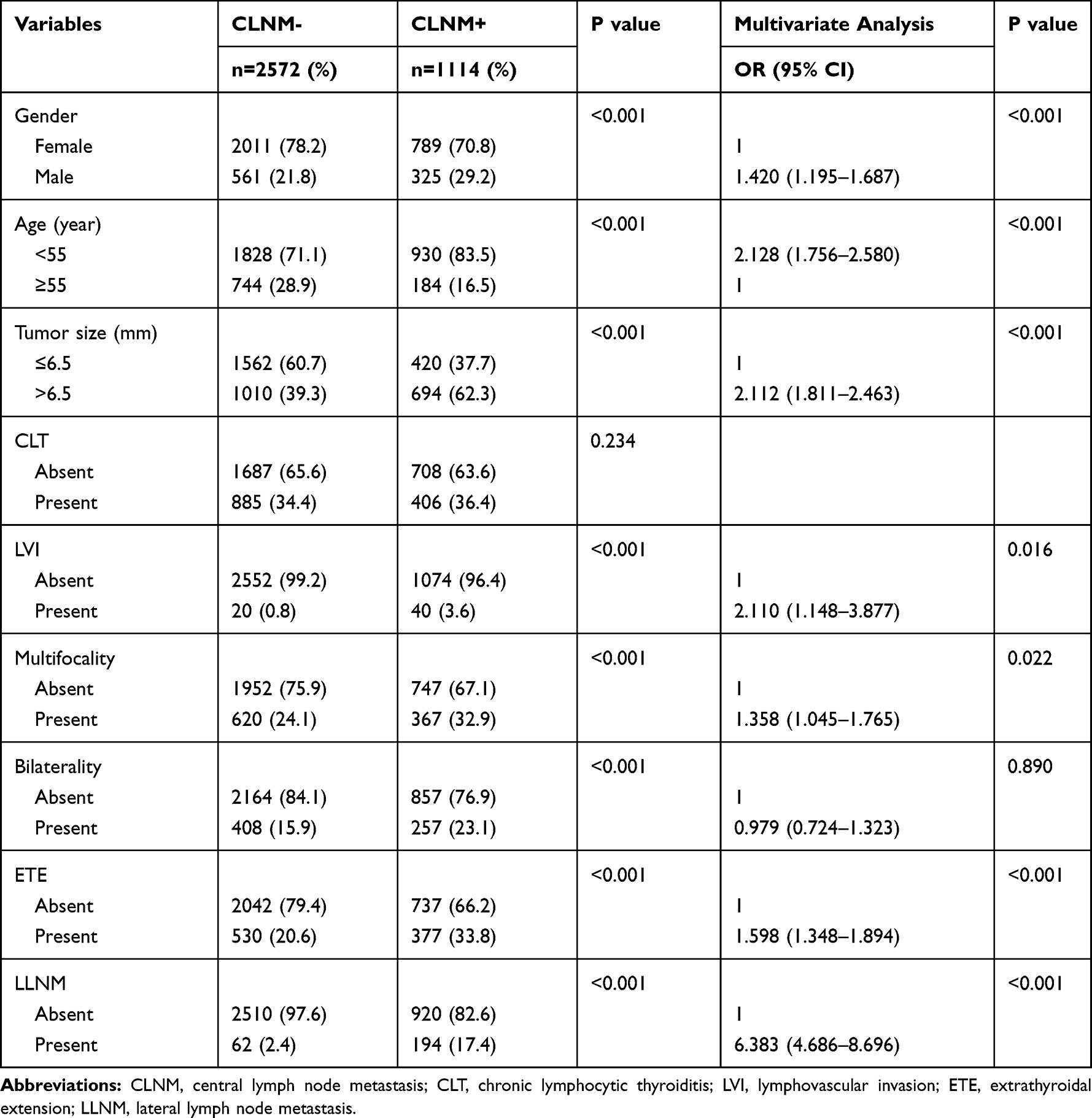 |
Table 2 Risk Factors for CLNM in PTMC Patients |
Risk Factors for LLNM
ROC curve analysis showed that the optimal cutoff point for the number of central LNs that had to be present in order to determine whether PTMC patients had LLNM, was three (area =0.682, standard error =0.022, asymptotic significance =0.000, 95% confidence interval =0.639–0.726).
Several clinicopathological factors were significantly associated with LLNM in univariate analysis (Table 3): male gender, tumor size >6.5 mm, LVI, multifocality, bilaterality, ETE, CLNM, more than three central LNs present (all P <0.001), and CLT (P =0.026). Multivariate analysis demonstrated that male gender (OR =1.668, P =0.001), tumor size >6.5 mm (OR =2.223, P <0.001), CLT (OR =1.402, P =0.021), LVI (OR =4.582, P <0.001), ETE (OR =1.393, P =0.023) and CLNM (OR =6.212, P <0.001) served as independent risk factors for LLNM for patients with PTMC.
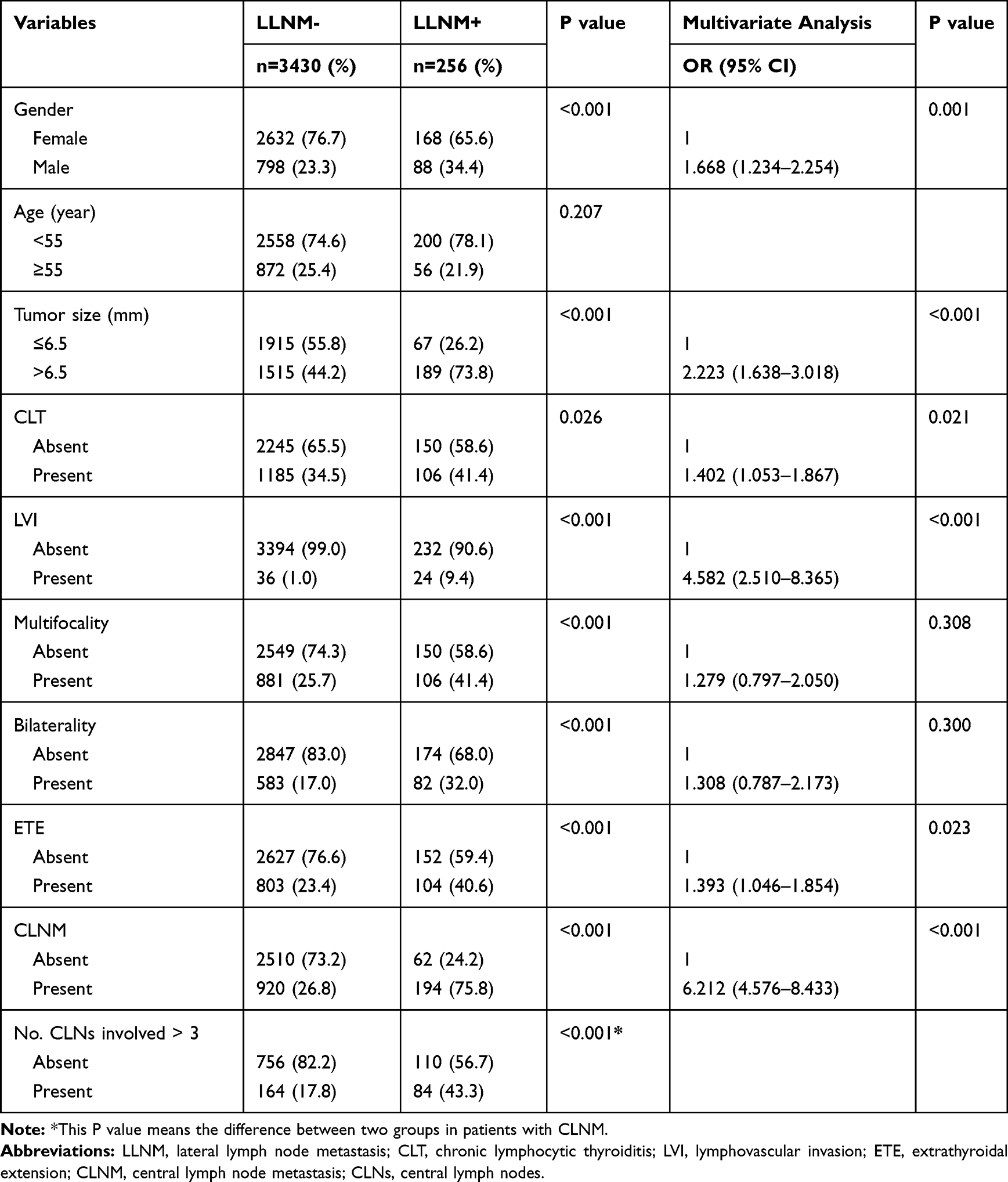 |
Table 3 Risk Factors for LLNM in PTMC Patients |
Association Between Tumor Locations and Cervical Lymph Node Metastasis
Among the 3686 patients, 2699 (73.2%) had solitary PTMC. According to preoperative US findings and postoperative histopathological examinations, tumor locations on the thyroid gland were divided into four parts: upper third, middle third, lower third, and isthmus.
Univariate analysis performed on the solitary PTMC group showed that CLNM was not significantly associated with tumor location (P =0.231) (Table 4). However, for patients with LLNM, there was a significant association (P <0.001) (Table 5). Lesions located in the upper third of the thyroid gland were prone to LLNM, with a metastasis rate of 10.9% (67/615).
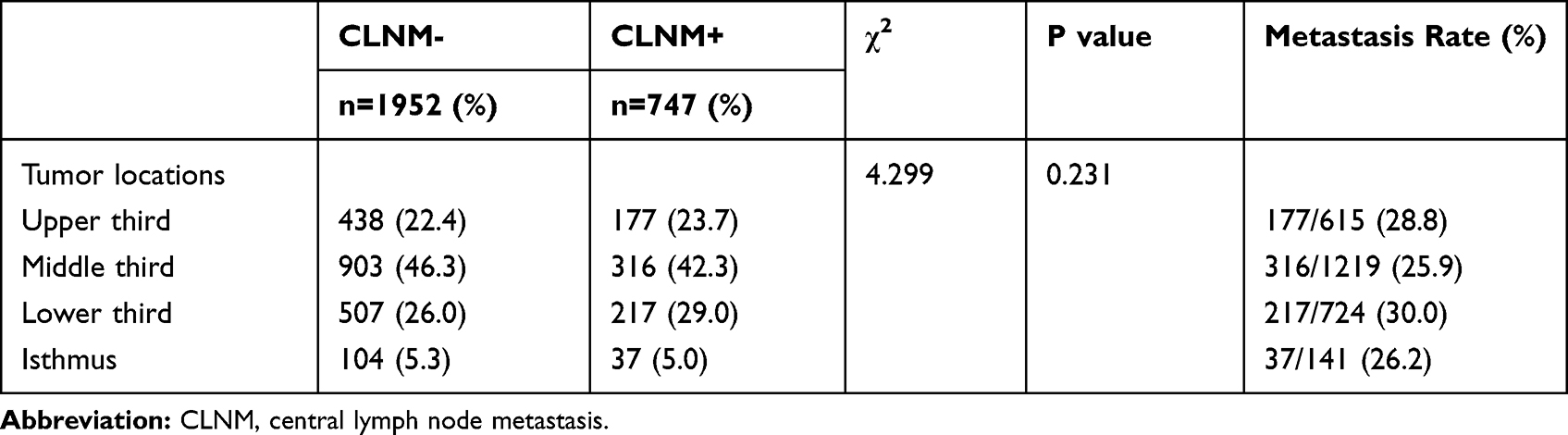 |
Table 4 Relationship Between Tumor Locations and CLNM in Solitary PTMC |
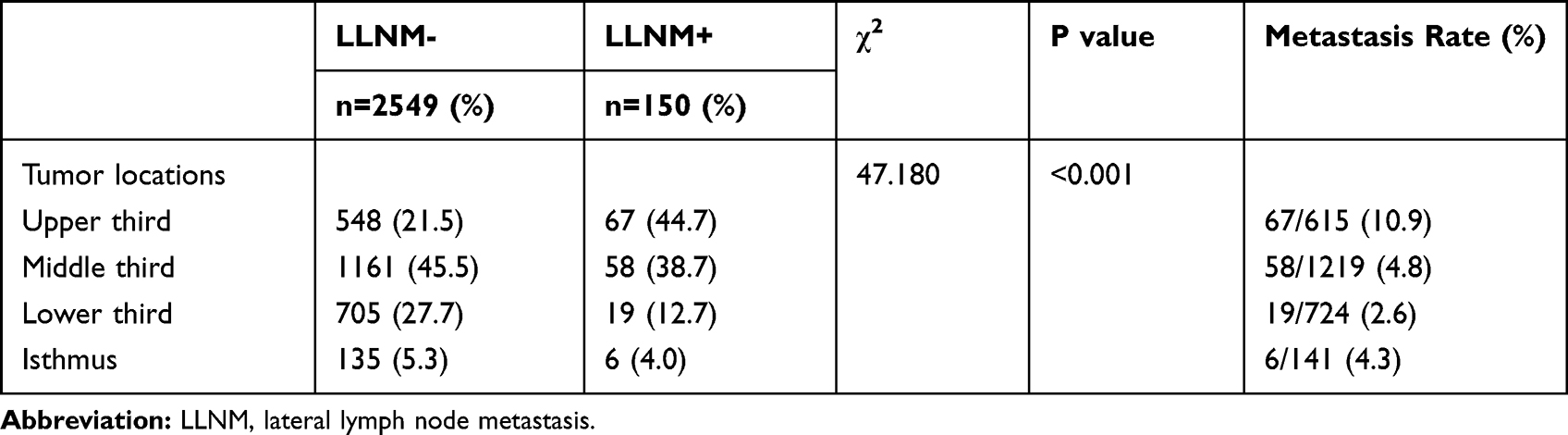 |
Table 5 Relationship Between Tumor Locations and LLNM in Solitary PTMC |
Discussion
In this retrospective study, we analyzed clinicopathological features of 3686 PTMC patients and evaluated the risk factors for CLNM and LLNM. Similar to that in previous studies, the prevalence of CLNM in the present study was 30.2% (1114/3686), and that of LLNM was 6.9% (256/3686).
Some characteristics, such as multifocality and bilaterality, have been regarded as independent predictors of CLNM and LLNM in other studies.4–6,8–10 In our study, however, bilaterality was not an independent predictor of either of these forms of LNM, whereas multifocality was only an independent predictor of CLNM, but not of LLNM.
Previous reports have shown that male gender was a risk factor for poor prognosis in PTC. In the present study, male gender was one of the independent risk factors for cervical LNM. Although male gender is associated with aggressiveness of PTMC, whether it affects the prognosis of PTMC patients remains uncertain. In a study that included 18,445 PTMC patients, Yu et al reported that male gender was an independent prognostic factor of overall survival for PTMC patients.11 However, there are conflicting reports. Lee et al adapted propensity score matching analysis to investigate the prognostic role of male gender in PTMC, and their study concluded that it was not an independent prognostic factor for PTMC patients.12
Previous studies demonstrated that PTMC with a larger tumor size might be biologically more similar to PTC.13 However, the definition of PTMC (PTC measuring ≤10 mm in diameter) is still undecided. Therefore, establishing the most appropriate tumor size of PTMC to distinguish it from PTC is conducive toward determining the optimal treatment strategy. Some studies have reported that tumors ≤5 mm are less prone to invasiveness, while others have shown cut-offs of 6, 7, or 8 mm.16,17 Using ROC curve analysis, Gong et al determined 8.5 mm as a favorable tumor size to distinguish PTMC from PTC.13 In the current study, we assessed tumor size by ROC curve analysis and found that primary tumor size (>6.5 mm) was significantly associated with CLNM.
ETE is stratified into minimal ETE (mETE), identified by histopathological examinations, and gross ETE (gETE), detected by intraoperative findings.14,18 The reported incidence rate of ETE ranges from 5% to 55% in PTMC, which is associated with LNM and disease recurrence. According to the eighth edition of the AJCC cancer staging system, gETE significantly affects the prognosis of patients, while mETE no longer applies to tumor staging for PTC.14,18,19 In the present study, 907 (24.6%) patients exhibited ETE, and ETE was identified as an independent risk factor for cervical LNM.
Previous studies have shown an association between tumor location and cervical LNM.10,16,17 Zhang et al reported that tumor location in the lower third or isthmus of the thyroid gland was correlated with CLNM.16 Back et al showed that lesions located in the upper pole of the thyroid gland had a high probability of LLNM in PTMC patients, which is consistent with our results from the current study.10
Although CLNM is not considered to decrease the disease-free survival in PTMC, it has been illustrated to be significantly related to LLNM in many studies, including our current study.4,9,10 The incidence rate of skip metastasis ranges from 6.8% to 27.8% in PTC with LLNM.15,20 In our study, skip metastasis was present in 62 out of 256 patients with LLNM (24.2%), which is a higher rate than in most other studies. The reason may be that all patients enrolled had PTMC, which is considered a risk factor for skip metastasis.20 Furthermore, our results demonstrated that roughly one-third (84/248) of patients with more than three central LNs had LLNM. For such patients, we recommend close observation and strict evaluation in the perioperative period. CLNM is the most common, however, prophylactic CLND remains controversial due to several associated surgical complications, like hypoparathyroidism and recurrent laryngeal nerve injury.21,22 2015 American Thyroid Association (ATA) guidelines recommend prophylactic CLND for patients with T3 and T4 primary tumors without evidence of nodal metastases or with known lateral lymph node metastasis and it is appropriate to not perform a prophylactic CLND for T1 or T2 tumors.2
Recently, genetic analysis yielded insights into gene mutations, signaling pathways, and biological functions playing a role in thyroid cancer.23,24 In our previous study, we described somatic mutations of key genes related to PTMC aggressiveness.23 We found that mutational burden was greater in tumors with aggressive features, which means that the accumulation of mutations may promote ETE and nodal metastasis. The rate of the BRAFV600E mutation is about 30–67% for PTMC, the highest mutation rate we identified in PTMC. This mutation has been demonstrated to be correlated with multifocality, ETE, nodal metastasis, and recurrence.25 We started BRAFV600E mutation analysis at our medical center in 2015; however, considering cost, it is not routinely performed for cases of PTMC. Therefore, the BRAFV600E mutation rate was not included in the present study, and its correlation to cervical LNM was not determined. However, the 2015 ATA guidelines stated that BRAF mutational evaluation appears to have a limited impact in clinical practice.2
This study has several limitations. First, there is a potential selection bias due to the nature of a nonrandomized, retrospective study conducted in a single center. Second, the measured incidence of LLNM may be underestimated, because LLND was performed only for patients with clinically apparent nodal metastasis in this study; therefore, there is the possibility of subclinical LLNM. Third, the current study did not include molecular analysis of enrolled patients. Future research is needed to investigate the significance of these factors.
Conclusion
In conclusion, in the present study, we showed that male gender, age less than 55 years, tumor size larger than 6.5 mm, presence of LVI, multifocality, ETE and LLNM were independent risk factors for CLNM. Furthermore, male gender, tumor size larger than 6.5 mm, CLT, LVI, ETE, and CLNM were factors that conferred an increased risk of LLNM. Notably, patients with solitary PTMC located in the upper third of the thyroid gland were likely to have LLNM. Therefore, meticulous evaluation of nodal metastasis is required in order to guide the surgical treatment of PTMC patients in clinical practice.
Acknowledgments
We would like to thank Editage for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
2. Haugen BR, Alexander EK, Bible KC, et al. American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2015;2016(26):1–133.
3. Haddad RI, Nasr C, Bischoff L, et al. NCCN guidelines insights: thyroid carcinoma, Version 2.2018. J Natl Compr Canc Netw. 2018;16(12):1429–1440. doi:10.6004/jnccn.2018.0089
4. Liu LS, Liang J, Li JH, et al. The incidence and risk factors for central lymph node metastasis in cN0 papillary thyroid microcarcinoma: a meta-analysis. Eur Arch Otorhinolaryngol. 2017;274(3):1327–1338.
5. Kim SK, Park I, Woo JW, et al. Predictive factors for lymph node metastasis in papillary thyroid microcarcinoma. Ann Surg Oncol. 2016;23(9):2866–2873. doi:10.1245/s10434-016-5225-0
6. Wang Y, Guan Q, Xiang J. Nomogram for predicting central lymph node metastasis in papillary thyroid microcarcinoma: a retrospective cohort study of 8668 patients. Int J Surg. 2018;55:98–102. doi:10.1016/j.ijsu.2018.05.023
7. Gao M, Ge M, Ji Q, et al. Chinese expert consensus and guidelines for the diagnosis and treatment of papillary thyroid microcarcinoma. Cancer Biol Med. 2016;2017(14):203–211.
8. Siddiqui S, White MG, Antic T, et al. Clinical and pathologic predictors of lymph node metastasis and recurrence in papillary thyroid microcarcinoma. Thyroid. 2016;26(6):807–815. doi:10.1089/thy.2015.0429
9. So YK, Kim MJ, Kim S, Son YI. Lateral lymph node metastasis in papillary thyroid carcinoma: a systematic review and meta-analysis for prevalence, risk factors, and location. Int J Surg. 2018;50:94–103. doi:10.1016/j.ijsu.2017.12.029
10. Back K, Kim JS, Kim JH, Choe JH. Superior located papillary thyroid microcarcinoma is a risk factor for lateral lymph node metastasis. Ann Surg Oncol. 2019;26(12):3992–4001.
11. Yu XM, Wan Y, Sippel RS, Chen H. Should all papillary thyroid microcarcinomas be aggressively treated? An analysis of 18,445 cases. Ann Surg. 2011;254(4):653–660. doi:10.1097/SLA.0b013e318230036d
12. Lee YH, Lee YM, Sung TY, et al. Is male gender a prognostic factor for papillary thyroid microcarcinoma? Ann Surg Oncol. 2017;24(7):1958–1964. doi:10.1245/s10434-017-5788-4
13. Gong Y, Li G, Lei J, et al. A favorable tumor size to define papillary thyroid microcarcinoma: an analysis of 1176 consecutive cases. Cancer Manag Res. 2018;10:899–906. doi:10.2147/CMAR.S154135
14. Song E, Lee YM, Oh HS, et al. A relook at the t stage of differentiated thyroid carcinoma: focus on gross extrathyroidal extension. Thyroid. 2018;29(2):202–208. doi:10.1089/thy.2018.0300
15. Nie X, Tan Z, Ge M. Skip metastasis in papillary thyroid carcinoma is difficult to predict in clinical practice. BMC Cancer. 2017;17(1):702. doi:10.1186/s12885-017-3698-2
16. Zhang L, Wei WJ, Ji QH, et al. Risk factors for neck nodal metastasis in papillary thyroid microcarcinoma: a study of 1066 patients. J Clin Endocrinol Metab. 2012;97(4):1250–1257. doi:10.1210/jc.2011-1546
17. Lim YC, Choi EC, Yoon YH, Kim EH, Koo BS. Central lymph node metastases in unilateral papillary thyroid microcarcinoma. Br J Surg. 2009;96(3):253–257. doi:10.1002/bjs.6484
18. Turk AT, Asa SL, Baloch ZW, et al. Interobserver variability in the histopathologic assessment of extrathyroidal extension of well differentiated thyroid carcinoma supports the new American Joint Committee on Cancer Eighth Edition criteria for tumor staging. Thyroid. 2019;29(5):619–624. doi:10.1089/thy.2018.0286
19. Diker-Cohen T, Hirsch D, Shimon I, et al. Impact of minimal extra-thyroid extension in differentiated thyroid cancer: systematic review and meta-analysis. J Clin Endocrinol Metab. 2018;103(6):2100–2106. doi:10.1210/jc.2018-00081
20. Zhao H, Huang T, Li H. Risk factors for skip metastasis and lateral lymph node metastasis of papillary thyroid cancer. Surgery. 2019;166(1):55–60. doi:10.1016/j.surg.2019.01.025
21. Conzo G, Polistena A, Calò PG, et al. Efficacy of combined treatment for anaplastic thyroid carcinoma: results of a multinstitutional retrospective analysis. Int J Surg. 2014;12:S178–S182. doi:10.1016/j.ijsu.2014.05.015
22. Shirley LA, Jones NB, Phay JE. The role of central neck lymph node dissection in the management of papillary thyroid cancer. Front Oncol. 2017;7:122. doi:10.3389/fonc.2017.00122
23. Song J, Wu S, Xia X, Wang Y, Fan Y, Yang Z. Cell adhesion-related gene somatic mutations are enriched in aggressive papillary thyroid microcarcinomas. J Transl Med. 2018;16(1):269. doi:10.1186/s12967-018-1642-0
24. Accardo G, Conzo G, Esposito D, et al. Genetics of medullary thyroid cancer: an overview. Int J Surg. 2017;41:S2–S6. doi:10.1016/j.ijsu.2017.02.064
25. Chen Y, Sadow PM, Suh H, et al. BRAF(V600E) is correlated with recurrence of papillary thyroid microcarcinoma: a systematic review, multi-institutional primary data analysis, and meta-analysis. Thyroid. 2016;26(2):248–255. doi:10.1089/thy.2015.0391
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.