")
Back to Journals » Clinical Interventions in Aging » Volume 15
Calcification of Cardiac Valves in Metabolic Bone Disease: An Updated Review of Clinical Studies
Authors Carrai P, Camarri S , Pondrelli CR, Gonnelli S, Caffarelli C
Received 29 December 2019
Accepted for publication 18 May 2020
Published 9 July 2020 Volume 2020:15 Pages 1085—1095
DOI https://doi.org/10.2147/CIA.S244063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Paolo Carrai, Silvia Camarri, Carlo Renato Pondrelli, Stefano Gonnelli, Carla Caffarelli
Department of Medicine, Surgery and Neuroscience, University of Siena, Siena, Italy
Correspondence: Stefano Gonnelli
Department of Medicine, Surgery and Neuroscience, University of Siena, Policlinico Le Scotte, Viale Bracci 2, Siena 53100, Italy
Tel +39 0577 585468
Fax +39 0577 233446
Email [email protected]
Abstract: Epidemiological and clinical data have suggested the existence of a relationship between cardiovascular diseases and metabolic bone disease. Several studies have demonstrated that heart valve calcification presents substantial similarities with that of bone. Literature data indicate that there are many active processes which promote osteogenesis and loss of mineralization inhibitors that lead to the deposition of extracellular matrix and proteins of bone tissue in cardiac valves. This review aimed to synthesize the available data in order to allow a better understanding of the relationship between osteoporosis or other metabolic bone diseases, such as primary hyperparathyroidism, and valvular calcification in humans. Electronic databases of Pubmed-Medline, Cochrane Library, and SCOPUS from inception to March 31, 2019 were searched. The full set of the articles potentially eligible were carefully assessed and reviewed. Finally, 23 studies were eligible and included in the systematic review. The majority of studies reported that osteoporosis and/or osteopenia were independent risk factors for valvular calcifications, even after adjusting for common cardiovascular risk factors. This suggests that this relationship is not only due to the presence of common cardiovascular risk factors but rather to underlying biological factors that connect them. Instead, regarding the association between primary hyperparathyroidism and valve calcification, conflicting data were found in the literature. To sum up, most of the literature data confirm that cardiac valve calcification processes are strongly influenced by alterations in bone metabolism. In particular, the patients with osteoporosis or primary hyperparathyroidism have an acceleration in the process of valvular calcification. Additional studies are needed to specifically address the mechanisms by which metabolic bone diseases could influence cardiac valve calcification.
Keywords: valvular calcification, osteoporosis, primary hyperparathyroidism, bone mineral density
Introduction
Over the years there has been growing interest in studying the relationship between metabolic bone disease and cardiovascular diseases. Nevertheless, at present, literature data on relationships between metabolic bone diseases and valvular calcifications are scarce and inconclusive. Heart valve calcification is common in the elderly, and is associated with increased cardiovascular morbidity and mortality.1 Among valve calcifications, the most studied is aortic valve calcification (AVC), which represents the most frequent cardiovascular disease after coronary artery disease and arterial hypertension, with a prevalence of 0.4% in the general population and 1.7% in the population over 65 years.2 Moreover, if severe aortic stenosis remains untreated, life expectancy is reduced to less than 5 years. As regards mitral valve calcification (MVC), literature data indicate that these mainly affect the posterior part of the annulus and are influenced by advancing age, chronic kidney disease (CKD), and cardiovascular risk factors.3
As demonstrated by several studies, heart valve calcification presents substantial similarities with that of bone, sharing many regulatory pathways and subpopulation cells with osteoblastic phenotype.4 Moreover, literature data indicate that there are many active processes which promote osteogenesis and loss of mineralization inhibitors that lead to the deposition of an extracellular matrix and proteins of bone tissue in cardiac valves. Among these, the endothelial damage induced by mechanical stress is also important.5 The result is an “active and chronic” process, and not “passive or degenerative”, as hypothesized some time ago. Therefore, at present cardiac valve calcification should be considered the final consequence of a complex and gradual filling process of calcium and mineral phosphate on valves.
Although similar to the atherosclerosis and vascular calcification process, there are some important differences in valvular calcification, both from a physiopathological and pharmacological point of view.6,7 Literature data, although often being controversial, allow us to better define the major regulatory pathways influencing the valve calcification process. The source of osteoblast-like cells within the cardiac valves remains one of the most controversial and crucial points. Transforming growth factor beta1 (TGF-β1) has been reported to be the most important factor in the differentiation of valve interstitial cells (VIC) into an osteoblast phenotype, which may represent the first step in the valvular calcification process. Transforming growth factor-β1 also promotes the increase of some important bone morphogenetic proteins (BMP).8,9 In fact, bone formation in heart valves was associated with the expression of BMP-2 and BMP-4 which increase the activity of alkaline phosphatase and osteocalcin in VIC.11 Other studies have reported that in the early stages of aortic valve calcification the differentiation of valve interstitial cells into an osteoblastic phenotype is influenced by the action of proinflammatory cytokines.7,12 On the other hand, pathways able to modulate the process of valvular calcification have been identified. In particular, a recent study reported that Matrix Gla Protein (MGP), a known calcification inhibitor which antagonizes BMP-2, negatively regulates calcification of human aortic valve interstitial cells isolated from calcified aortic valves, so highlighting its role as an anti-calcification protein.13 Fetuin-A is a circulating protein that can exist in isolation or as a complex with MGP. Fetuin-A, similarly to MGP, antagonizes BMP-2 and TGF-β1 and prevents calcification by binding to calcium crystals. Recently, significant correlations between low levels of fetuin-A and aortic valve stenosis or calcification have been reported.14,15 Moreover, high levels of Asymmetric Dimethylarginine (ADMA), an inhibitor of Nitric Oxide (NO) synthase, were found in patients with aortic stenosis; therefore, NO appears to slow aortic valve calcification, probably via of a direct effect on valve interstitial cells.4,8
Wnt/β-catenin and a receptor activator of nuclear factor kappa β (RANK)/receptor activator of nuclear factor kappa β ligand (RANKL)/osteoprotegerin (OPG) pathways play a crucial role in the later stages of the valvular calcification process.7 In vascular cells, TGF-β1 and BMP-2 are able to induce nuclear translocation of β-catenin and increase Wnt signaling expression, stimulating the osteogenic differentiation of mesenchymal progenitor cells.2 The Wnt system is one of the most important regulators in bone formation, leading to expression of RUNX2 and promoting formation of bone tissue by osteoblasts.2,7,16 In heart valves, stimulation of RANK by RANKL induces an osteoblastic phenotype in VIC (contrary to the bone tissue where the stimulation of RANK by RANKL promotes an osteoclastic phenotype). Moreover, while in bone OPG binds RANKL and prevents bone resorption, at a valvular level the inhibition of RANKL by OPG impedes valve calcification. Confirming this, whilst OPG-deficient mice develop osteoporosis, they simultaneously accelerate vascular calcification in association with increased expression of RANKL in both regions.7 These data may explain the “calcification paradox” in osteoporosis which is associated with age-independent increases in vascular calcification and even cardiovascular mortality. Fibroblast Growth Factor-23 (FGF-23) works by inhibiting sodium-phosphate transporter in the kidneys, increasing the excretion of phosphate and inhibiting the enzyme 1-α-hydroxylase, so decreasing the production of active Vitamin D (calcitriol). A loss of its function leads to an increase in serum phosphates, with a potential risk of renal calcinosis. However, the Multi-Ethnic Study of Atherosclerosis (MESA) reported a significant correlation between elevated FGF-23 levels and the annual progression of mitral valve calcification but not that of the aortic valve.17 PTH is a key factor in the regulation of bone metabolism and essential for bone tissue formation; nevertheless, the role of PTH in the valvular calcification process remains unclear. However, the increase in PTH values is correlated with the progression of aortic valve calcification and with an increase of valve calcification area.18,19 Finally, human VIC cells, cultured with high concentrations of extracellular adenosine triphosphate (ATP), enhance the expression of osteoblast cell markers such as alkaline phosphatase, and demonstrates the inhibitory effects of adenosine on this process.4,20
The major regulatory pathways influencing valve calcifications are listed in Table 1.
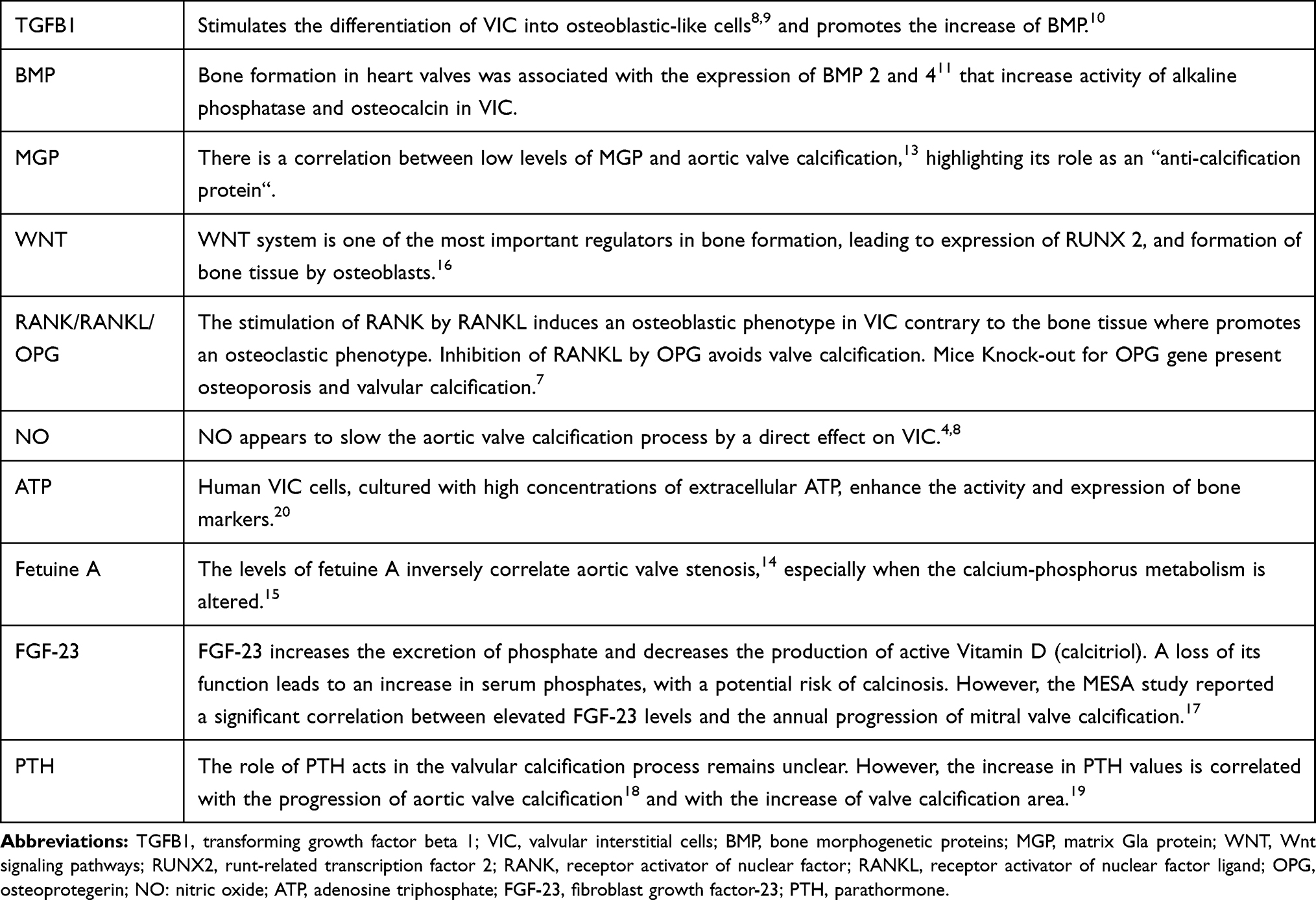 |
Table 1 Factors Influencing Valvular Calcification |
This review aimed to summarize the available data in order to allow a better understanding of the relationship between osteoporosis or other metabolic bone diseases, such as primary hyperparathyroidism, and valvular calcification in humans.
Materials and Methods
A literature review was conducted from inception to May 31, 2019. Pubmed-Medline, Cochrane Library, ClinicalTrials.gov, and SCOPUS databases were searched using the following search terms (“Valvular Calcification” or “Aortic valve calcification” or “Mitral valve calcification”) and (“osteoporosis” or “Bone Mineral Density” or “Primary Hyperparathyroidism” or “Paget’s disease”).
The process of selection of the studies for review was carried out according to the PRISMA checklist and a PRISMA flow diagram has been shown in Figure 1.
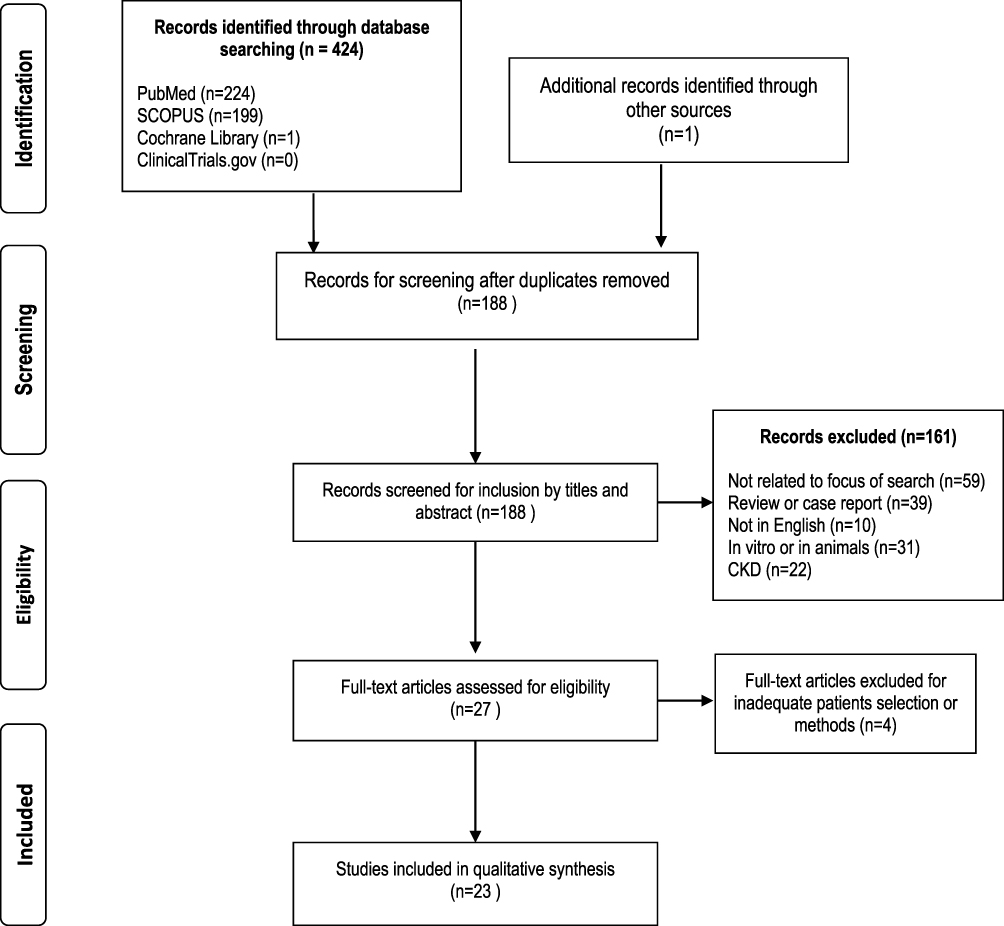 |
Figure 1 Flow chart of the studies identified and included in the review. |
Results
Heart Valve Calcifications and Osteoporosis
Studies on valvular calcification, both in vitro and in animal models, have shown evidence of regulatory pathways and cell types similar to those of bone tissue. Over the years, although the interest in the association between bone metabolism and cardiovascular disease has been the subject of increasing attention, only a few clinical studies correlated valvular calcification and osteoporosis (or decreased bone mineral density) obtaining non-univocal results. The studies reporting the correlations between these two conditions are listed in Table 2.
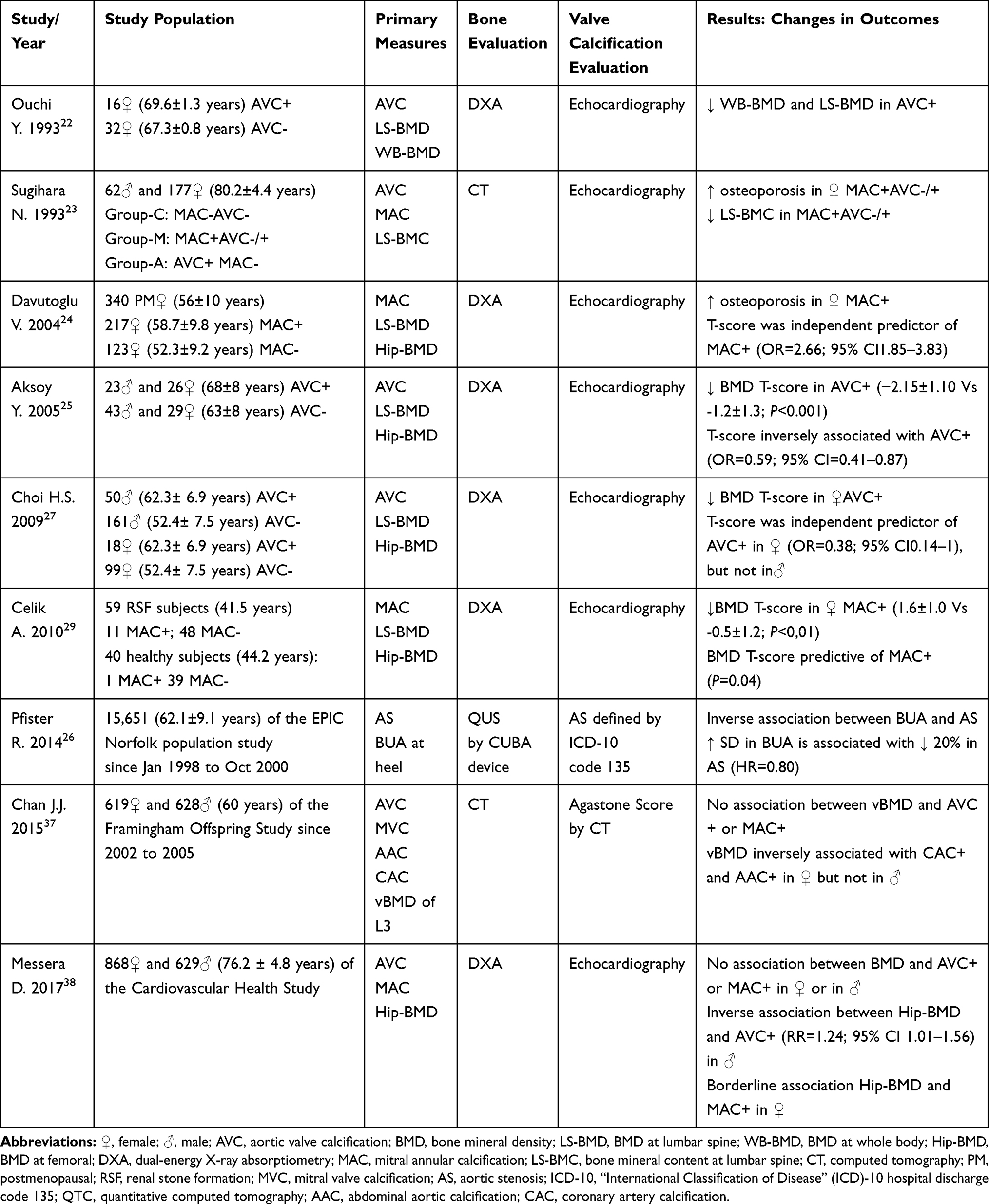 |
Table 2 Main Characteristics of the Nine Studies Included in the Review on Valvular Calcifications in Osteoporosis |
In 1990 Mori et al 21 first observed a statistically significant correlation between the lower values of bone mineral density (BMD) and mitral annular calcification in elderly Japanese women. Similarly, some years later, Ouchy et al22 showed that BMD values were significantly lower in elderly women with aortic valve calcification (AVC). Interestingly, another study carried out on 239 elderly subjects (62 males and 177 females) reported that BMD at lumbar spine (as assessed by Computed Tomography CT) was inversely associated with MVC but not with AVC, in postmenopausal women only.23
In 2004, Davutoglu et al24 in a study of 340 women (mean age 56±10 years), observed that the incidence of MVC was higher in women with osteoporosis and that there was a positive correlation between severity of mitral calcification and severity of osteoporotic disease. Instead, the study by Aksoy et al25 conducted on 114 patients (49 with AVC and 65 without), found that age and hypertension but not gender were independent risk factors for the development of valve calcification; in this study BMD was inversely correlated with the presence of AVC, and this correlation remained significant after adjusting for age. Similarly, a study carried out on a subset of the EPIC population (Norfolk, UK), found an inverse correlation between BMD at calcaneus, as measured by ultrasound, and risk of AVC independently of known risk factors and potential confounders.26
Also Choi et al,27 in a study conducted on 328 Korean patients (211 men and 117 women), reported that the presence of AVC, assessed by echocardiography, was inversely correlated with BMD; however, in this latter study, after adjusting for various comorbidities (age, BMI, cigarette smoking, arterial hypertension, hypercholesterolemia, and diabetes mellitus), the BMD remained independently and inversely related with AVC only in women.27
As previously reported, MVC is correlated not only with common cardiovascular risk factors, but also with the presence of CKD and, consequently, altered phospho-calcic metabolism.28 In fact, the study by Celick29 reported that the prevalence of MVC was higher in patients with renal stones compared to healthy controls, whereas the BMD of patients with MVC was significantly lower with respect to those without.
The incidental finding of vertebral fractures during routine radiographic examinations, such as the CT, is common and has been demonstrated to be correlated with an increase in mortality from all causes.30 Low BMD and vertebral fractures are also associated with cardiovascular diseases and cardiovascular mortality, especially in diabetic patients or those who have suffered coronary events.31,33 On the other hand, the finding of calcifications in the cardiovascular system has been reported to be correlated with the presence of osteoporosis and bone fractures.33,35
In order to clarify if vertebral fractures found during routine radiographic examinations were independent predictors of future cardiovascular events, Gondrie et al36 conducted research in the multi-center PROVIDI study (Prognostic Value of unrequested Information on Diagnostic Imaging). The results showed that having at least one fracture was a predictive element of future cardiovascular events, and this finding remained statistically significant after adjusting for age and sex. However, statistical significance became borderline when adjusted for valvular, aortic, and coronary calcifications.36 However, this study provided further evidence of an association between valvular (mitral and aorta) and coronary calcifications with vertebral fractures that resulted independent of age and gender.
Another two recent studies evaluated the correlation between osteoporosis and valve calcification. Chan et al,37 in a study carried out on 1317 elderly subjects (689 women and 628 men with a mean age of 60±9 years), found no significant correlation between AVC and BMD; however, in both men and women, there was a significant inverse correlation between reduction of BMD and severity of vascular calcification, expeciallyespecially at the level of the abdominal aorta.
Moreover, the study by Messera et al,38 carried out on 1497 elderly patients from the CHS (Cardiovascular Health Study), showed that there were no significant associations between BMD and the presence of any valvular calcification (aortic and/or mitral valve). However, aortic calcification was greater in male patients with osteoporosis at total femur after adjusting for various confounding factors. This result has not been demonstrated for women. Conversely, in women there was a correlation (although not statistically significant) between calcification of the mitral valve and the decrease in BMD at the femur.38
Valvular Calcifications in Primary Hyperparathyroidism
It has long been known that patients with primary hyperparathyroidism (PHP) have structural and functional changes to the heart, with a consequent increasing of cardiovascular events. The principal studies which have evaluated the relationship between valve calcification and primary hyperparathyroidism are reported in Table 3.
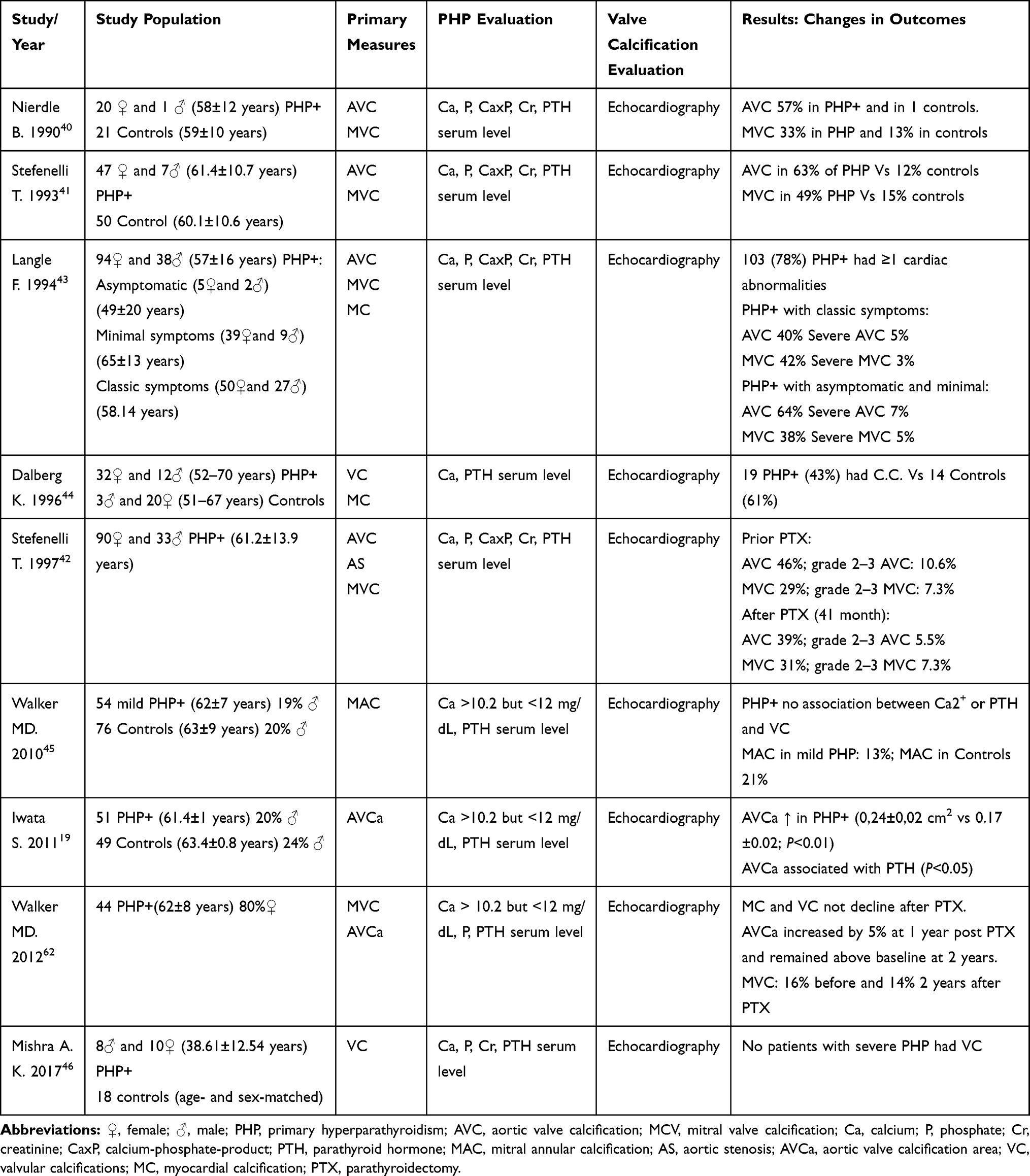 |
Table 3 Main Characteristics of the Nine Studies Included in the Review on Valvular Calcification in Primary Hyperparathyroidism |
Already in 1981, Roberts and Waller, 39 by evaluating morphological aspects in the heart during the autopsies of 18 patients with chronic hypercalcemia, reported that chronic hypercalcemia was associated with an accelerated deposition of calcium in heart valves, in media and intima of coronary arteries and in the myocardium.
More recently, Nierdle et al,40 in a study carried out on 21 PHP patients and compared with 21 age- and sex-matched controls, observed a significant increase in the incidence of aortic valve and mitral annulus calcifications in subjects with PHP compared to controls.
In a prospective study, Stefenelli41 evaluated the effects of PHP on heart valves, myocardium, and myocardial function in 54 PHP patients, who underwent echocardiography examination before and 12±2 months after parathyroidectomy. A control group of 49 people was used for comparison; also in this case, the results highlighted a close correlation between the presence of primary hyperparathyroidism and cardiac valve calcifications. In fact, AVC was found in 63% of subjects with PHP and MVC in 49% (vs controls: 12% and 15%, respectively). Interestingly, while left ventricular hypertrophy presented a regression after parathyroidectomy, valve calcifications remained unchanged and without progression over time.
Some years later, a prospective study by the same authors carried out on 123 PHP patients undergoing parathyroidectomy and controlled up to 41 months later, confirmed regression of left ventricular hypertrophy and no progression of valvular calcifications.42 Also, in the study by Langle et al43 a significant increase of cardiac calcifications in patients with PHP compared to controls was reported, but in this study no significant correlations between cardiac calcification findings and severity of the clinical features were observed.
In contrast, Dalberg et al,44 in a study published several years before, found a non-significant correlation between cardiac and valvular calcifications and PHP.
Also the study by Walker et al,45 carried out on a group of 54 PHP subjects, reported that there was no correlation between PHP and valve calcification or cardiac hypertrophy. In 2011, in a study conducted in the same patients cohort, Iwata et al19 compared the structure and function of the aortic valve of PHP patients with a control population and found that aortic valve calcification area resulted greater in PHP subjects (even when adjusted for risk factors such as age, sex, BMI, cigarette smoking, hypertension, hypercholesterolemia, and GFR estimated). Note that aortic valve calcification area was positively and significantly correlated with parathyroid hormone values, but not with remaining parameters of phospho-calcium metabolism such as serum calcium, serum phosphate, and 25 hydroxy-Vitamin-D.19 This demonstrates a significant role of PTH in the pathophysiology of cardiac valve calcification.
It should be noted, however, that the patients enrolled in the studies of Walker et al, Iwata et al, and Dalberg et al had serum calcium levels below 12 mg/dL, while in other studies the serum calcium levels were higher (>12 mg/dL), implying a possible dose dependent effect of calcemia in the valve calcification process.
Nevertheless, a recent study conducted on a small number of patients suffering from PHP (18 patients), with mean calcemia values higher than 12 mg/dL (12.5±1.4 mg/dL) did not show the presence of valvular calcifications in affected patients.46
Valvular Calcifications in Paget’s Disease of Bone
Also Paget’s disease has been associated with an increase in cardiac calcifications, including myocardium and valve apparatus.47–51 The first studies date back to 1944, when Harrison and Lennox,47 using data from autopsies, reported an increase in incidence of valvular calcifications in patients suffering from Paget’s disease compared to unaffected subjects (17 of 43 cases, 39%, vs 8% in 223 controls of similar age distribution). Later, Strickberger et al, 49 in a study based on autopsy reports, found a higher incidence of aortic valve calcification with respect to mitral valve and that the severity of the calcifications was correlated with the severity of Paget’s disease.
Similarly, the study by Hultgren et al50 showed a strong association between aortic valve calcification and Paget’s severity (22% in severe disease vs 5.5% in moderate disease and 3.5% in controls). Moreover, in this latter study no differences in the severity of atherosclerosis between pagetic patients and controls were found, suggesting that in Paget’s disease cardiac valve calcification may be independent from atherosclerosis.50 Finally, a more recent study carried out on 220 pagetic patients the valvular calcifications were found to be present in 15% of pagetic patients.51
Discussion
Although valvular calcification and osteoporosis share several cardiovascular risk factors such as age, hypertension, dyslipidemia, diabetes, and cigarette smoking,52 the majority of studies of this review reported that osteoporosis and/or osteopenia were independent risk factors for valvular calcifications even after adjusting for common cardiovascular risk factors. This suggests that this relationship is not only due to the presence of common cardiovascular risk factors but most probably also to underlying biological factors that connect them.
Furthermore, it seems unlikely that valvular calcification could be secondary only to the catabolic processes in osteoporotic bone, also considering the lack of any significant impact of bisphosphonate therapy in the progression of aortic valve calcification, as confirmed in a recent retrospective observational study.53 The existence of underlying bio-humoral mechanisms that connect the two pathological conditions would seem more probable. In support of this, it has been proposed that Vitamin D may also represent a common regulator of both bone metabolism and valve calcification.54–56 In fact, in the study by Ortlepp et al54 it was shown that the genetic polymorphism of vitamin D (VDR Bsml allele B with respect to b) associated with low bone mineral density is also associated with a higher risk of developing calcific aortic stenosis.
Interesting results were also noted in gender difference, in particular as reported in the study by Choi et al,27 the association between low bone mineral density and aortic valve calcification seems to be stronger in women than in men. Estrogens could explain this relationship; in fact, estrogens play an important role in the pathophysiology of both osteoporosis and cardiovascular diseases in women. Moreover, an estrogen receptor-alpha gene polymorphism that is associated with BMD in many clinical studies,57,58 has also been observed in post menopausal women with AVC.59
Moreover, in Messera et al’s38 study, BMD values at the femoral neck correlated with AVC in males, while in women they correlated with MVC. Similarly, in the study by Sugihara and Matsuzaki23 a higher incidence of MVC was found in women with low bone mineral density than in men. A stronger association between MVC and low BMD in women than in men could be explained by the fact that mitral valve calcification is more common in women as they have a higher incidence of osteoporosis, also due to the effect of the estrogenic decline in the post menopausal period. Furthermore, alteration in bone metabolism seems to have a greater impact on development of MVC.60 These considerations support a higher risk of MVC in women suffering from bone metabolism disorders.
Also, with regard to the association between primary hyperparathyroidism and valve calcification, conflicting data has been found in the literature.
Normally, PTH plays a central role in the regulation of calcium homeostasis and its release is triggered by a reduction in serum calcium level.61 Certainly, there is a positive correlation between the severity of the disease and valvular calcification. In PHP, the role of hypercalcaemia found in the advanced stages of the disease appears to be a fundamental element for the development of valvular calcifications. This could explain the poor association between these two conditions in the studies where the mean value of calcemia was lower than 12 mg/dL.19,45,62
In the study by Iwata et al,19 the aortic valve calcification area was greater in PHP patients than in controls, implying a role of PTH not only in the beginning of calcification but also in its progression. Also, it is important to emphasize that in PHP patients who have undergone parathyroidectomy there is an absence of regression but also of progression in valve calcification.41,42,62
The fact that in patients without PHP affected by severe AVC there is a significant recurrence of the AA variant of PTH gene63 and that patients with secondary hyperparathyroidism present a significant increase in valvular calcifications19 supports the crucial role of PTH in the valve calcification process.
In pagetic patients the high AVC incidence can be explained by hemodynamic changes that occur in advanced stages of the disease rather than to alterations of serum calcium and phosphate which are usually normal in patients with Paget’s disease.
In fact, due to the increased cardiac output, the aortic valve is affected by a greater stress which would lead to endothelial damage which would favor the triggering of calcification and thickening of leaflet; this hypothesis seems to confirm literature data reporting that the degree of aortic valve calcification was positively correlated with the severity of Paget’s disease.49,50
To date, the fact that the prevalence of valvular calcifications is lower in more recent reports about Paget and PHP is probably due to the early stage of diagnosis in these diseases.
To sum up, most of literature data confirm that cardiac valve calcification processes are strongly influenced by alterations in bone metabolism. In particular, the patients with osteoporosis or primary hyperparathyroidism have an acceleration in the process of valvular calcification. Additional studies are needed to specifically address the mechanisms by which metabolic bone diseases could influence cardiac valve calcification.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barasch E, Gottdiener JS, Marino Larsen EK, Chaves PH, Newman AB. Cardiovascular morbidity and mortality in community-dwelling elderly individuals with calcification of the fibrous skeleton of the base of the heart and aortosclerosis (The Cardiovascular Health Study). Am Cardiol. 2006;97(9):1281–1286. doi:10.1016/j.amjcard.2005.11.065
2. Lindman BR, Clavel MA, Mathieu P, et al. Calcific aortic stenosis. Nature Rev Dis Primers. 2016;3(2):16006. doi:10.1038/nrdp.2016.6
3. Shekar C, Budoff M. Calcification of the heart: mechanisms and therapeutic avenues. Expert Rev Cardiovasc Ther. 2018;16(7):527–536. doi:10.1080/14779072.2018.1484282
4. Chester AH. Molecular and cellular mechanisms of valve calcification. Aswan Heart Centre Sci Pract Series. 2011;4. doi:10.5339/ahcsps.2011.4
5. Gomel MA, Lee R, Grande-Allen KJ. Comparing the role of mechanical forces in vascular and valvular calcification progression. Front Cardiovasc Med. 2019;197(5):1–14.
6. Sud K, Agarwal S, Parashar A, et al. Degenerative mitral stenosis: unmet need for percutaneous interventions. Circulation. 2016;133(16):1594–1604. doi:10.1161/CIRCULATIONAHA.115.020185
7. Pawade TA, Newby DE, Dweck MR. Calcification in aortic stenosis: the skeleton key. J Am CollCardiol. 2015;66(5):561–577. doi:10.1016/j.jacc.2015.05.066
8. Kennedy JA, Hua X, Mishra K, Murphy GA, Rosenkranz AC, Horowitz JD. Inhibition of calcifying nodule formation in cultured porcine aortic valve cells by nitric oxide donors. Eur J Pharmacol. 2009;602:28–35. doi:10.1016/j.ejphar.2008.11.029
9. Clark-Greuel JN, Connolly JM, Sorichillo E, et al. Transforming growth Factor-β1 mechanisms in aortic valve calcification: increased alkaline phosphatase and related events. Ann Thorac Surg. 2007;83:946–953. doi:10.1016/j.athoracsur.2006.10.026
10. Walker GA, Masters KS, Shah DN, Anseth KS, Leinwand LA. Valvular myofibroblast activation by transforming growth factor-beta: implications for pathological extracellular matrix remodeling in heart valve disease. Circ Res. 2004;95:253–260. doi:10.1161/01.RES.0000136520.07995.aa
11. Mohler ER, Gannon F, Reynolds C, Zimmerman R, Keane MG, Kaplan FS. Bone formation and inflammation in cardiac valves. Circulation. 2001;103:1522–1528. doi:10.1161/01.CIR.103.11.1522
12. Hjortnaes J, Butcher J, Figueiredo JL, et al. Arterial and aortic valve calcification inversely correlates with osteoporotic bone remodelling: a role for inflammation. Eur Heart J. 2010;31(16):1975–1984. doi:10.1093/eurheartj/ehq237
13. Chiyoya M, Seya K, Yu Z, et al. Matrix Gla protein negatively regulates calcification of human aortic valve interstitial cells isolated from calcified aortic valves. J PharmacolSci. 2018;136(4):257–265.
14. Di Minno A, Zanobini M, Myasoedova VA, et al. Could circulating fetuin A be a biomarker of aortic valve stenosis? Int J Cardiol. 2017;249:426–430. doi:10.1016/j.ijcard.2017.05.040
15. Carracedo M, Back M. Fetuin A in aortic stenosis and valve calcification: not crystal clear. Int J Cardiol. 2018;265(15):77–78. doi:10.1016/j.ijcard.2018.04.115
16. Rajamannan NM, Subramaniam M, Caira F, Stock SR, Spelsberg TC. Atorvastatin inhibits hypercholesterolemia-induced calcification in the aortic valves via the Lrp5 receptor pathway. Circulation. 2005;112:1229–1234.
17. Bortnik AE, Xu S, Kim RS, et al. Biomarkers of mineral metabolism and progression of aortic valve and mitral annular calcification: the multi-ethnic study of atherosclerosis. Atherosclerosis. 2019;285:79–86. doi:10.1016/j.atherosclerosis.2019.04.215
18. Iwata S, Hyodo E, Yanagi S, et al. Parathyroid hormone and systolic blood pressure accelerate the progression of aortic valve stenosis in chronic hemodialysis patients. Int J Cardiol. 2013;163(3):256–259. doi:10.1016/j.ijcard.2011.06.025
19. Iwata S, Walker MD, Di Tullio MR, et al. Aortic valve calcification in mild primary hyperparathyroidism. J Clin Endocrinol Metab. 2012;97(1):132–137. doi:10.1210/jc.2011-2107
20. Osman L, Chester AH, Amrani M, Yacoub MH, Smolenski RT. A novel role of extracellular nucleotides in valve calcification: a potential target for atorvastatin. Circulation. 2006;114:I566–I572. doi:10.1161/CIRCULATIONAHA.105.001214
21. Mori H, Oku Y, Hashiba K, Seto M, Mameya G. The relationship of osteoporosis to mitral annular and aortic valvular calcification in elderly women. J Cardiography. 1990;20(2):393–399.
22. Ouchy Y, Akishita M, de Souza AC, Nakamura T, Orimo H. Age-related loss of bone mass and aortic/aortic valve calcification—re evaluation of recommended dietary allowance of calcium in the elderly. Ann N Y Acad Sci. 1993;676:297–307. doi:10.1111/j.1749-6632.1993.tb38743.x
23. Sugihara N, Matsuzaki M. The influence of severe bone loss on mitral annular calcification in postmenopausal osteoporosis of elderly Japanese women. Jpn Circ J. 1993;57(1):14–26. doi:10.1253/jcj.57.14
24. Davutoglu V, Yilmaz M, Soydinc S, et al. Mitral annular calcification is associated with osteoporosis in women. Am Heart J. 2004;147:1113–1116. doi:10.1016/j.ahj.2003.12.002
25. Aksoy Y, Yagmur C, Tekin GO, et al. Aortic valve calcification: association with bone mineral density and cardiovascular risk factors. Coron Artery Dis. 2005;16:379–383. doi:10.1097/00019501-200509000-00007
26. Pfister R, Michels G, Sharp SJ, Luben R, Wareham NJ, Khaw KT. Inverse association between bone mineral density and risk of aortic stenosis in men and women in EPIC-Norfolk prospective study. Int J Cardiol. 2015;178:29–30. doi:10.1016/j.ijcard.2014.10.065
27. Choi HS, Rhee Y, Hur NW, Chung N, Lee EJ, Lim SK. Association between low bone mass and aortic valve sclerosis in Koreans. Clin Endocrinol. 2009;71:792–797. doi:10.1111/j.1365-2265.2009.03543.x
28. Tohiono S, Tohno Y, Minami T, et al. Accumulation of calcium and phosphorus in the mitral valve in comparison with the abdominal aorta and the scaphoid bone. Biol Trace Elem Res. 2000;77:33–42. doi:10.1385/BTER:77:1:33
29. Celick A, Davutoglu V, Sarica K, et al. Relationship between renal stone formation, mitral annular calcification and bone resorption markers. Ann Saudi Med. 2010;30(4):301–305. doi:10.4103/0256-4947.65264
30. Hasserius R, Karlsson MK, Nilsson BE, Redlund-Johnell I, Johnell O. European vertebral osteoporosis study.Prevalent vertebral deformities predict increased mortality and increased fracture rate in both men and women: a 10-year population-based study of 598 individuals from the Swedish cohort in the European vertebral osteoporosis study. Osteoporos Int. 2003;14(1):61–68. doi:10.1007/s00198-002-1316-9
31. Bandeira E, Neves AP, Costa C, Bandeira F. Association between vascular calcification and osteoporosis in men with type 2 diabetes. J Clin Densitom. 2012;15(1):55–60. doi:10.1016/j.jocd.2011.07.002
32. Silva HC, Pinheiro MM, Genaro PS, et al. Higher prevalence of morphometric vertebral fractures in patients with recent coronary events independently of BMD measurements. Bone. 2013;52(2):562–567. doi:10.1016/j.bone.2012.11.004
33. Buckens CF, de Jong PA, Verkooijen HM, Verhaar HJ, Mali WP, van der Graaf Y. PROVIDI study group. Vertebral fractures on routine chest computed tomography: relation with arterial calcifications and future cardiovascular events. Int J Cardiovasc Imaging. 2015;31(2):437–445. doi:10.1007/s10554-014-0567-9
34. Schulz EJ, Arfai K, Liu X, Sayre J, Gilsanz V. Aortic calcification and the risk of osteoporosis and fractures. J Clin Endocrinol Metab. 2004;89(9):4246–4253. doi:10.1210/jc.2003-030964
35. Szulc P, Kiel DP, Delmas PD. Calcifications in the abdominal aorta predict fractures in men: MINOS study. J Bone Miner Res. 2008;23(1):95–102. doi:10.1359/jbmr.070903
36. Gondrie MJ, Mali WP, Buckens CF, Jacobs PC, Grobbee DE, van derGraaf Y. The PROgnostic value of unrequested information in diagnostic imaging (PROVIDI) study: rationale and design. Eur J Epidemiol. 2010;25(10):751–758. doi:10.1007/s10654-010-9514-9
37. Chan JJ, Cupples LA, Kiel D, O’Donnell CJ, Hoffmann U, Samelson EJ. QCT volumetric bone mineral density and vascular and valvular calcification: the framingham study. J Bone Miner Res. 2015;30(10):1767–1774. doi:10.1002/jbmr.2530
38. Messera D, Xu S, Bartz TM, et al. Relationship of bone mineral density with valvular and annular calcification in community-dwelling older people: the cardiovascular health study. Arch Osteoporos. 2017;12(1):52. doi:10.1007/s11657-017-0347-y
39. Roberts WC, Waller BF. Effect of chronic hypercalcemia on the heart. An analysis of 18 necropsy patients. Am J Med. 1981;71(3):371–384. doi:10.1016/0002-9343(81)90163-7
40. Nierdle B, Stefenelli T, Glogar D, Woloszczuk W, Roka R, Mayr H. Cardiac calcific deposits in patients with primary hyperparathyroidism: preliminary results of a prospective echocardiographic study. Surgery. 1990;108(6):1052–1056.
41. Stefenelli T, Mayr H, Bergler-Klein J, Globits S, Woloszczuk W, Niederle B. Primary hyperparathyroidism: incidence of cardiac abnormalities and partial reversibility after successful parathyroidectomy. Am J Med. 1993;95(2):197–202. doi:10.1016/0002-9343(93)90260-V
42. Stefenelli T, Abela C, Frank H, et al. Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow-up. J Clin Endocrinol Metab. 1997;82(1):106–112. doi:10.1210/jcem.82.1.3666
43. Langle F, Abela C, Koller-Strametz J, et al. Primary hyperparathyroidism and the heart: cardiac abnormalities correlated to clinical and biochemical data. World J Surg. 1994;18(4):619–624. doi:10.1007/BF00353780
44. Dalberg K, Brodin LA, Juhlin-Dannfelt A, Farnebo LO. Cardiac function in primary hyperparathyroidism before and after operation. An echocardiographic study. Eur J Surg. 1996;162(3):171–176.
45. Walker MD, Fleischer JB, Di Tullio MR, et al. Cardiac structure and diastolic function in mild primary hyperparathyroidism. J Clin Endocrinol Metab. 2010;95(5):2172–2179. doi:10.1210/jc.2009-2072
46. Mishra AK, Agarwal A, Kumar S, Mishra SK. Assessment of cardiovascular system abnormalities in patients with advanced primary hyperparathyroidism by detailed echocardiographic analysis: a prospective study. World J Endoc Surg. 2017;9(2):46–50. doi:10.5005/jp-journals-10002-1209
47. Harrison CV, Lennox B. Heart block in osteitis deformans. Br Heart J. 1948;10(3):167–176. doi:10.1136/hrt.10.3.167
48. King M, Huang JM, Glassman E. Paget’s disease with cardiac calcification and complete heart block. Am J Med. 1969;46(2):302–304. doi:10.1016/0002-9343(69)90014-X
49. Strickberger SA, Schulman SP, Hutchins GM. Association of Paget’s disease of bone with calcific aortic valve disease. Am J Med. 1987;82(5):953–956. doi:10.1016/0002-9343(87)90157-4
50. Hultgren HN. Osteitis deformans (Paget’s disease) and calcific disease of the heart valves. Am J Cardiol. 1998;81(12):1461–1464. doi:10.1016/S0002-9149(98)00213-6
51. Merlotti D, Gennari L, Galli B, et al. Characteristics and familial aggregation of Paget’s disease of bone in Italy. J Bone Miner Res. 2005;20(8):1356–1364. doi:10.1359/JBMR.050322
52. Hofbauer LC, Brueck CC, Shanahan CM, Schoppet M, Dobnig H. Vascular calcification and osteoporosis from clinical observation towards molecular understanding. Osteoporos Int. 2007;18(3):251–259. doi:10.1007/s00198-006-0282-z
53. Aksoy O, Cam A, Goel SS, et al. Do bisphosphonates slow the progression of aortic stenosis? J Am Coll Cardiol. 2012;59(16):1452–1459. doi:10.1016/j.jacc.2012.01.024
54. Ortlepp JR, Hoffmann R, Ohme F, Lauscher J, Bleckmann F, Hanrath P. The vitamin D receptor genotype predisposes to the development of calcific aortic valve stenosis. Heart. 2001;85(6):635–638. doi:10.1136/heart.85.6.635
55. Bellavia D, Costa V, De Luca A, et al. Vitamin D level between calcium-phosphorus homeostasis and immune system: new perspective in osteoporosis. Curr Osteoporos Rep. 2016. doi:10.1007/s11914-016-0331-2
56. Etta PK, Sharma RK, Gupta A. Study of chronic kidney disease-mineral bone disorders in newly detected advanced renal failure patients: a hospital-based cross-sectional study. Saudi J Kidney Dis Transpl. 2017;28(4):874–885.
57. Nam HS, Shin MH, Kweon SS, et al. Association of estrogen receptor-alpha gene polymorphisms with bone mineral density in postmenopausal Korean women. J Bone Miner Metab. 2005;23(1):84–89. doi:10.1007/s00774-004-0545-8
58. Long JR, Zhang YY, Liu PY, et al. Association of estrogen receptor alpha and vitamin D receptor gene polymorphisms with bone mineral density in Chinese males. Calcif Tissue Int. 2004;74(3):270–276. doi:10.1007/s00223-003-0087-4
59. Nordstrom P, Glader CA, Dahlén G, et al. Oestrogen receptor alpha gene polymorphism is related to aortic valve sclerosis in postmenopausal women. J Intern Med. 2003;254(2):140–146. doi:10.1046/j.1365-2796.2003.01179.x
60. Bortnik AE, Bartz TM, Ix JH, et al. Association of inflammatory, lipid and mineral markers with cardiac calcification in older adults. Heart. 2016;102(22):1826–1834. doi:10.1136/heartjnl-2016-309404
61. Marx SJ. Hyperparathyroid and hypoparathyroid disorders. N Engl J Med. 2000;343(25):1863–1875. doi:10.1056/NEJM200012213432508
62. Walker MD, Rundek T, Homma S, et al. Effect of parathyroidectomy on subclinical cardiovascular disease in mild primary hyperparathyroidism. Eur J Endocrinol. 2012;167(2):277–285. doi:10.1530/EJE-12-0124
63. Schmitz F, Ewering S, Zerres K, Klomfass S, Hoffmann R, Ortlepp JR. Parathyroid hormone gene variant and calcific aortic stenosis. J Heart Valve Dis. 2009;18(3):262–267.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.