")
Back to Journals » Journal of Blood Medicine » Volume 9
Associations between iron deficiency anemia and clinical features among pregnant women: a prospective cohort study
Authors Baradwan S , Alyousef A, Turkistani A
Received 24 May 2018
Accepted for publication 1 August 2018
Published 3 October 2018 Volume 2018:9 Pages 163—169
DOI https://doi.org/10.2147/JBM.S175267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
This paper has been retracted
Saeed Baradwan, Abdullah Alyousef, Abdulrhman Turkistani
Department of Obstetrics and Gynecology, King Fahad Medical City, Riyadh, Saudi Arabia
Background: Iron deficiency anemia (IDA) during pregnancy is a common and preventable disorder. It remains a contributing factor to maternal morbidity and mortality and is associated with high perinatal mortality rates.
Objective: To determine the prevalence of IDA and its associated clinical features among pregnant women.
Methods: This analytical prospective cohort study included 1,579 pregnant women who attended an antenatal clinic, Women’s Specialized Hospital, King Fahad Medical City, Riyadh, Saudi Arabia, between January 2018 and April 2018. The type of anemia and its associated maternal and fetal outcomes were determined.
Results: About 702 women were confirmed to have IDA, with a prevalence of 44.5 %. Most women (79.8%) were younger than 35 years. A low hemoglobin concentration was reported in 45 % of participants. The major type of anemia was microcytic hypochromic anemia (98.7%). More than half of the participants (57.3%) reported use of iron supplementation during pregnancy. IDA anemia was highest in pregnant women with gravidity >8 in 40 (56.3%) compared to normal pregnant women 31 (43.7%), and lowest in those with gravidity ≤2 in 281 (41.4%) compared to normal pregnant women 397 (58.6%). The difference was statistically significant, P=0.024. Similarly, this type of anemia was highest in those with parity of >3 (53.3%) and lowest in nulliparous women (39.3%) compared to normal pregnant women (46.7%) and (60.7%), respectively. This was statistically significant P=0.002. IDA had significantly (P=0.012) lower spontaneous vaginal delivery rates compared with normal pregnant women (44.5% vs 55.5%, respectively). IDA had significantly (P=0.017) lower antenatal fetal distress rates compared with normal pregnant women (68.5% vs 31.5%, respectively).
Conclusion: Anemia in general and microcytic hypochromic anemia in particular were significantly associated with higher gravidity and parity. The significant outcome associated with IDA during pregnancy was a lower rate of spontaneous vaginal delivery and antenatal fetal distress. Compliance with iron supplementation in order to prevent maternal and fetal adverse outcomes was observed.
Keywords: microcytic hypochromic anemia, pregnancy, iron deficiency anemia
Introduction
Iron deficiency anemia (IDA) is the most common nutritional deficiency problem affecting pregnant women worldwide.1 The high prevalence of iron and other micronutrient deficiencies among women during pregnancy in developing countries is of concern, and maternal anemia is still a cause of considerable perinatal morbidity and mortality.2–4 Overall prevalence of iron deficiency in pregnant women in the US is about 18%,5 and in the UK, the prevalence was estimated to be 24% in a recent cross-sectional study.6
IDA in pregnancy has been defined by the National Academy of Sciences panel on nutrition and pregnancy as ferritin levels of less than 12 µg/L.7 Serum ferritin may be a better indicator of iron status, as examination of iron stores in bone marrow is impractical.8 However, historically, blood hemoglobin (Hb) levels have been used, this test being simple and inexpensive. The WHO defines anemia in pregnancy as Hb levels of less than 11 g/dL.9
Most women begin their pregnancy with partially or completely depleted iron reserves.10 During pregnancy, there is an increase in both red cell mass and plasma volume to accommodate the needs of the growing uterus and fetus.11 The plasma volume increases more than the red cell mass does, leading to a fall in the concentration of Hb in the blood, despite an increase in the total number of red cells. This drop in Hb concentration decreases blood viscosity and is thought to enhance placental perfusion, providing better maternal-fetal gas and nutrient exchange.12 Nonetheless, the significance of this physiological hemodilution of pregnancy for women and their babies is controversial, as is the level of Hb at which they would derive a benefit from iron treatment.13 Maternal iron requirements average 1,000 mg/d.14
Severe anemia during pregnancy results in maternal and fetal adverse outcomes. Maternal adverse outcomes include preterm labor, preeclampsia, sepsis, postpartum hemorrhage, and an increased need for blood transfusion.15 The fetal adverse outcome consists of a high fetal mortality rate at the third trimester of gestation.16 In addition, IDA of moderate degree can impact the motor and mental development of children and adolescents.17,18
In the present study, we aimed to determine the prevalence of IDA in pregnant women and its associated clinical features by comparing these outcomes with those of pregnant women with normal Hb levels.
Methods
An analytical prospective cohort study was carried out, which included 1,579 pregnant women who attended Women’s Specialized Hospital, King Fahad Medical City, Riyadh, Saudi Arabia, between January 2018 and April 2018. We examined the hematological status and serum ferritin between 16 and 20 weeks of pregnancy. Exclusion criteria included malignancies, chronic renal or liver diseases, diabetic, hypertension disorder, known cases of thalassemia and hemoglobinopathies, vitamin B12 deficiency anemia, folic acid deficiency anemia, chronic inflammatory diseases, and having had a blood transfusion within 6 months before enrolment in the study.
Data were collected from the perinatal database, which consists of information collected uniformly according to predefined criteria immediately after delivery by an obstetrician. Coding is done after assessing the medical prenatal care records and the routine hospital documents. We analyzed the following characteristics: maternal age, gravidity, parity, abortions, twin pregnancy, medical history (diabetes mellitus, hypertension, and preeclampsia), and iron supplementation. We also examined the following obstetric characteristics: apparent congenital malformation, intrauterine growth (defined as birth weight below the sex-specific 5th percentile of weights for gestational age), antenatal fetal distress, and mode of delivery (vaginal: spontaneous or induced, instrumental: forceps or ventouse, and cesarean: elective or emergency). In addition, we investigated maternal and perinatal outcomes: preterm labor (defined as birth before 37 completed weeks of gestation), postpartum hemorrhage, packed cell transfusion, maternal death, Apgar score at 1 minute and 5 minutes, birth weight, admission to the neonatal intensive care unit (NICU), and perinatal mortality.
As study criteria, we used the WHO definition of anemia in pregnancy (Hb levels of less than 11 g/dL)9 and the definition by the National Academy of Sciences panel on nutrition and pregnancy of IDA (microcytic hypochromic anemia) in pregnancy (ferritin levels of less than 12 µg/L).7 We recorded Hb, hematocrit (HCT), red cell distribution width (RDW; erythrocyte volume), mean corpuscular volume (MCV), and mean corpuscular hemoglobin (MCH). We then determined the types of anemia on the basis of these variables.
The protocol was reviewed and approved by the Institutional Review Board of King Fahad Medical City in Riyadh, Saudi Arabia. All data were entered into an electronic database without personal identifiers to maintain confidentiality. Patient consent was waived as no patient identifiers were included nor was the patient care affected or influenced in any way. This article does not contain any studies with animals performed by any of the authors.
The data were analyzed by using SPSS version 22.0. Demographic characteristics were expressed as mean (± SD) and range. The outcome variables were expressed as the absolute number (percentage). The P-value was based on Fisher’s exact test for categorical data and the Mann–Whitney U test for quantitative variables. A P-value of <0.05 was considered to be statistically significant.
Results
The study included 1,579 pregnant women. About 702 women were confirmed to have IDA, with a prevalence of 44.5%. Patients’ demographics are presented in Table 1. Most of the participants (1,260 [79.8%]) were younger than 35 years. The median value of gravidity was 3, ranged between 1 and 15; of parity was 2, ranged between 1 and 13; and of abortion was 1, ranged between 1 and 11. Intrauterine growth restriction was reported in 52 (3.3%) participants and antenatal fetal distress in 73 (4.6%) participants. Cesarean delivery was reported in 630 (39.9%) participants, whereas instrumental or vacuum-assisted delivery was used in 66 (4.2%). Spontaneous vaginal delivery was reported in almost half of the cases (883 [55.9%]), and most of them were spontaneous (753 [47.7%]). Emergency cesarean section was reported in 383 (24.3%) cases. Preterm labor was reported in 191 (12.1%) cases. The Apgar score at 1 minute ranged between 0 and 10 with a mean of 9.2±1.6, whereas that at 5 minutes ranged between 0 and 9 with a mean of 8.2±1.6. Apparent congenital malformation was observed in 51 (3.2%), admission to NICU in 136 (8.6%), postpartum hemorrhage in 59 (3.7%), and intrauterine fetal death in 29 (1.8%) cases.
 | Table 1 Characteristics of 1,579 study subjects Notes: aData are presented as n (%) except where otherwise indicated. Abbreviations: Hb, hemoglobin; HCT, hematocrit; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; NICU, neonatal intensive care unit; RDW, red cell distribution width. |
From Table 1, low level of Hb concentration was reported in 711 (45%) participants, low HCT values in 975 (61.9%), and low RDW values in 52 (3.4%). The MCH concentration was below normal in 10.8% of the cases. The ferritin level was low in 702 (45%) cases. The MCV was below normal in 486 (30.7%) and the mean corpuscular Hb was below normal in 531 (33.6%) cases. The major reported type of anemia was microcytic hypochromic anemia (702 [98.7%]). More than half of the participants (905 [57.3%]) reported the use of iron supplementation during pregnancy. The birth weight of the first baby was 2.99±0.64 kg and of the twin babies was 2.15±0.67 kg.
From (Table 2), it is evident that the studied factors could be associated with IDA. IDA anemia was highest in pregnant women with gravidity >8 at 40 years (56.3%) compared to normal pregnant women at 31 years (43.7%), and lowest in those with gravidity ≤2 (281 [41.4%]) compared to normal pregnant women (397 [58.6%]). The difference was statistically significant (P=0.024). Similarly, this type of anemia was highest in those with parity of >3 (53.3%) and lowest in nulliparous women (39.3%) compared to normal pregnant women (46.7%) and (60.7%), respectively. This was statistically significant (P=0.002). IDA had significantly (P=0.012) lower spontaneous vaginal delivery rates compared with normal pregnant women (44.5% vs 55.5%, respectively). This anemia was reported in more than half of the women (132 [54.3%]) who delivered by elective cesarean section, in 153 (40.2%) of those who delivered by emergency cesarean section, and in 32 (50%) of those who delivered by ventouse. IDA had significantly (P=0.017) lower antenatal fetal distress rates compared with normal pregnant women (68.5% vs 31.5%, respectively). There is some missing data in this study parameter and hence is not included in this analysis. IDA was not significantly associated with other maternal and fetal characteristics, as illustrated in Table 2.
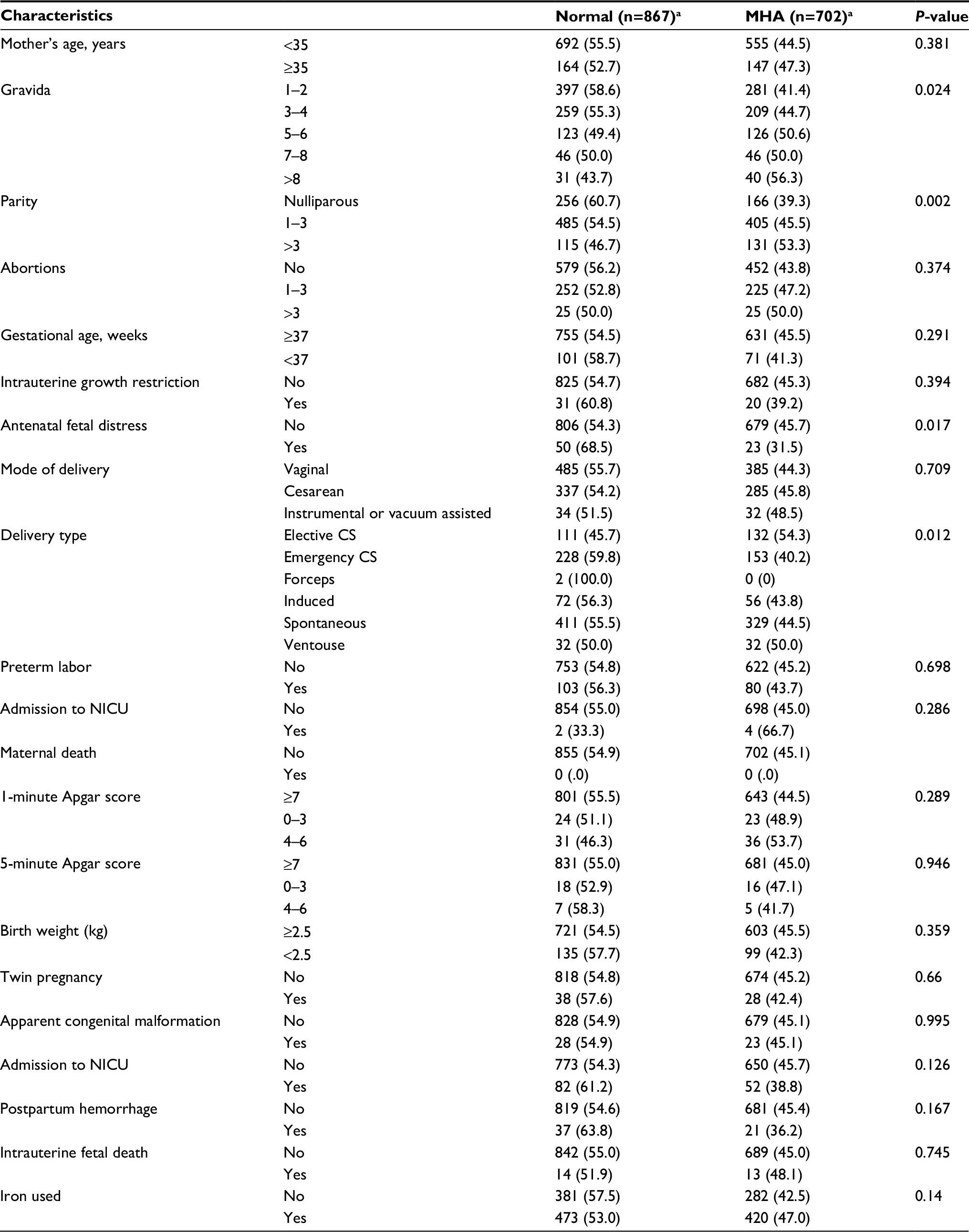 | Table 2 Microcytic hypochromic anemia (MHA) in study subjects Notes: Data are presented as n (%).aStatistically significant. Abbreviation: NICU, neonatal intensive care unit; CS, cesarean section. |
Discussion
The prevalence of anemia was reported to be the highest in Indian women at 29%, while it was 16% in black Caribbean women and 6%–7% in Irish and Chinese women. In this study, the prevalence was 44.5%, which is slightly higher than that reported in these countries, and the prevalence based on low HCT was 61.9%, which is higher than that reported in European countries (at about 50%).19,20 A higher gravidity and parity was reported in women with anemia in general and IDA in particular. Similar results have been reported previously.19
Much of the information regarding IDA in pregnancy and its adverse outcomes is controversial. Two important points should be considered: the gestational age at which the determination of Hb is performed and the degree of anemia identified. Regarding the first point, throughout the first and second trimesters of pregnancy, Hb and HCT levels decline because of the physiological expansion of plasma volume.21 Late in the second to early third trimester, Hb and HCT levels reaches its lowest level and then rises again nearer to term. Therefore, the best time to detect any risk associated with maternal anemia would be early in pregnancy, a fact that has been demonstrated in many studies.22,23 Thus, any estimation of Hb concentration after 20 weeks of gestation is reasonably representative of the fall in concentration induced by pregnancy.24
The second point that should be considered is IDA during pregnancy, as the association with adverse pregnancy outcomes is also controversial. The association between IDA and birth weight has been documented, as has been the association between IDA and preterm delivery.25 However, in the present study, anemia was significantly associated with a lower rate of spontaneous vaginal delivery. This finding might be attributed to the fact that anemia in our study was mostly mild and most participants were taking iron supplements. In agreement with others, we assume that iron supplementation during pregnancy may have a protective effect against adverse outcomes. On the other hand, it has been reported in several studies that severe maternal anemia in the first trimester is associated with adverse outcomes such as preterm birth, intrauterine growth restriction, low birth weight, low Apgar score, and cesarean deliveries.26–31
The association between IDA and adverse outcomes has been confirmed in many studies.26–28,32 In a study conducted by Patra et al,31 very high maternal mortality (6.2%) and perinatal mortality (60%) were observed in severely anemic women during the third trimester of pregnancy. Most women in the present study were at a gestational age of >37 weeks and had mild anemia, which might explain the absence of an association of anemia with adverse outcomes, other than the relatively lower rate of antenatal fetal distress.
The limitations of our study were that it was limited to Women’s Specialized Hospital, and some data regarding the study parameter were missing. Also, we did not classify IDA into mild or severe. We recommend that information, education, and counseling about this disease be provided to pregnant women. This information might aid physicians in guiding their patients and taking optimal clinical decisions together.
In conclusion, IDA during pregnancy continues to be a major health problem worldwide. Anemia in general and microcytic hypochromic anemia in particular are significantly associated with higher gravidity and parity. The significant outcome associated with IDA during pregnancy was a lower rate of spontaneous vaginal delivery and antenatal fetal distress. Compliance with iron supplementation in order to prevent maternal and fetal adverse outcomes was observed.
In light of these results, we recommend hematological screening for Hb and iron status in early pregnancy. There is no need for further checks of these values if the pregnancy is uncomplicated and there is compliance with iron supplementation to prevent maternal and fetal adverse outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harb Perspect Med. 2013;3(7):a011866. | ||
UNICEF/UNU/WHO. Iron Deficiency Anemia: Assessment, Prevention, and Control. Geneva: World Health Organization; 2001. | ||
Thangaleela T, Vijayalakshmi P. Prevalence of anaemia in pregnancy. Indian J Nutr Diet. 1994;31:26–32. | ||
Cutner A, Bead R, Harding J. Failed response to treat anaemia in pregnancy: reasons and evaluation. J Obstet Gynecol. 1999;Suppl 1:S23–27. | ||
Mei Z, Cogswell ME, Looker AC, et al. Assessment of iron status in US pregnant women from the National Health and Nutrition Examination Survey (NHANES), 1999-2006. Am J Clin Nutr. 2011;93(6):1312–1320. | ||
Barroso F, Allard S, Kahan BC, et al. Prevalence of maternal anaemia and its predictors: a multi-centre study. Eur J Obstet Gynecol Reprod Biol. 2011;159(1):99–105. | ||
Institute of Medicine, Committee on Nutritional Status During Pregnancy and Lactation. Nutrition During Pregnancy. Washington, DC: National Academy Press; 1990:272–298. | ||
Hoffman R, Benz E, Shattil SJ, Furie B, Cohen HJ, Silberstein LE. Hematology: Basic Principles and Practice. 3rd ed. New York: Churchill Livingstone, Inc; 2000. | ||
World Health Organization. Iron Deficiency Anaemia, Assessment, Prevention and Control: A Guide for Programme Managers. Geneva: WHO; 2001. | ||
Robson SC, Hunter S, Boys RJ, Dunlop W. Serial study of factors influencing changes in cardiac output during human pregnancy. Am J Physiol. 1989;256(4 Pt 2):H1060–H1065. | ||
Duvekot JJ, Cheriex EC, Pieters FA, Menheere PP, Peeters LH. Early pregnancy changes in hemodynamics and volume homeostasis are consecutive adjustments triggered by a primary fall in systemic vascular tone. Am J Obstet Gynecol. 1993;169(6):1382–1392. | ||
Prakash S, Yadav K. Maternal anemia in pregnancy: an overview. Ijppr Human. 2015;4(3):164–179. | ||
Al RA, Unlubilgin E, Kandemir O, Yalvac S, Cakir L, Haberal A. Intravenous versus oral iron for treatment of anemia in pregnancy: a randomized trial. Obstet Gynecol. 2005;106(6):1335–1340. | ||
Bothwell TH. Iron requirements in pregnancy and strategies to meet them. Am J Clin Nutr. 2000;72(1 Suppl):257S–264. | ||
Bayoumeu F, Subiran-Buisset C, Baka NE, Legagneur H, Monnier-Barbarino P, Laxenaire MC. Iron therapy in iron deficiency anemia in pregnancy: intravenous route versus oral route. Am J Obstet Gynecol. 2002;186(3):518–522. | ||
Khan MM. Effect of maternal anaemia on fetal parameters. J Ayub Med Coll Abbottabad. 2001;13(2):38–41. | ||
Halterman JS, Kaczorowski JM, Aligne CA, Auinger P, Szilagyi PG. Iron deficiency and cognitive achievement among school-aged children and adolescents in the United States. Pediatrics. 2001;107(6):1381–1386. | ||
Algarín C, Peirano P, Garrido M, Pizarro F, Lozoff B. Iron deficiency anemia in infancy: long-lasting effects on auditory and visual system functioning. Pediatr Res. 2003;53(2):217–223. | ||
Bencaiova G, Breymann C. Mild anemia and pregnancy outcome in a Swiss collective. Journal of Pregnancy. 2014; 307535:7. | ||
Hercberg S, Preziosi P, Galan P. Iron deficiency in Europe. Public Health Nutr. 2001;4(2B):537–545. | ||
Mcmullin MF, White R, Lappin T, Reeves J, Mackenzie G. Haemoglobin during pregnancy: relationship to erythropoietin and haematinic status. Eur J Haematol. 2003;71(1):44–50. | ||
Levy A, Fraser D, Katz M, Mazor M, Sheiner E. Maternal anemia during pregnancy is an independent risk factor for low birthweight and preterm delivery. Eur J Obstet Gynecol Reprod Biol. 2005;122(2):182–186. | ||
Xiong X, Buekens P, Alexander S, Demianczuk N, Wollast E. Anemia during pregnancy and birth outcome: a meta-analysis. Am J Perinatol. 2000;17(3):137–146. | ||
Steer P, Alam MA, Wadsworth J, Welch A. Relation between maternal haemoglobin concentration and birth weight in different ethnic groups. BMJ. 1995;310(6978):489–491. | ||
Rasmussen K. Is There a Causal Relationship between Iron Deficiency or Iron-Deficiency Anemia and Weight at Birth, Length of Gestation and Perinatal Mortality? J Nutr. 2001;131(2S–2):590S–603. | ||
Zhou LM, Yang WW, Hua JZ, Deng CQ, Tao X, Stoltzfus RJ. Relation of hemoglobin measured at different times in pregnancy to preterm birth and low birth weight in Shanghai, China. Am J Epidemiol. 1998;148(10):998–1006. | ||
Malhotra M, Sharma JB, Batra S, Sharma S, Murthy NS, Arora R. Maternal and perinatal outcome in varying degrees of anemia. Int J Gynaecol Obstet. 2002;79(2):93–100. | ||
Levy A, Fraser D, Katz M, Mazor M, Sheiner E. Maternal anemia during pregnancy is an independent risk factor for low birthweight and preterm delivery. Eur J Obstet Gynecol Reprod Biol. 2005;122(2):182–186. | ||
Xiong X, Buekens P, Alexander S, Demianczuk N, Wollast E. Anemia during pregnancy and birth outcome: a meta-analysis. Am J Perinatol. 2000;17(3):137–146. | ||
Fareh OI, Rizk DE, Thomas L, Berg B. Obstetric impact of anaemia in pregnant women in United Arab Emirates. J Obstet Gynaecol. 2005;25(5):440–444. | ||
Patra S, Pasrija S, Trivedi SS, Puri M. Maternal and perinatal outcome in patients with severe anemia in pregnancy. Int J Gynaecol Obstet. 2005;91(2):164–165. | ||
Scanlon KS, Yip R, Schieve LA, Cogswell ME. High and low hemoglobin levels during pregnancy: differential risks for preterm birth and small for gestational age. Obstet Gynecol. 2000;96(5 Pt 1):741–748. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.