")
Back to Journals » Drug Design, Development and Therapy » Volume 13
Association between the c.415C > T, c.52G > A, and 36_37insGGAGTC polymorphisms of NUDT 15 and thiopurine-induced leukopenia, thiopurine intolerance, and severe hair loss: an updated meta-analysis
Authors Wang R, Liu B, Li J, Xu J, Wang X, Zhao Z , Zhao L
Received 29 March 2019
Accepted for publication 1 July 2019
Published 5 August 2019 Volume 2019:13 Pages 2729—2744
DOI https://doi.org/10.2147/DDDT.S210512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Ruili Wang,1,2 Baogang Liu,2 Jiapeng Li,1 Jiamin Xu,1 Xiaoling Wang,1 Zhigang Zhao,2 Libo Zhao1
1Clinical Research Center, Beijing Children’s Hospital, National Center for Children’s Health, Capital Medical University, Beijing, People’s Republic of China; 2Department of Clinical Pharmacy, School of Pharmaceutical Sciences, Capital Medical University, Beijing, People’s Republic of China
Purpose: As a common immunosuppressive and anticancer drug, thiopurine has achieved remarkable clinical success. However, higher inter-individual dose variability and unpredictable toxicity still challenge its use in clinical practices. Some studies indicate that NUDT 15 polymorphisms are associated with this variation, but specific correlation remains controversial. This meta-analysis assessed the association between three polymorphisms of NUDT 15 and thiopurine-induced toxicities.
Methods: Three databases were electronically searched: PubMed, Embase, and Web of Science. Only case–control studies and cohort studies were eligible. The overall pooled ORs and corresponding 95% CIs were used to represent the results.
Findings: We included 16 studies that focus on NUDT 15 c.415C > T, c.52G > A, and 36_37insGGAGTC polymorphisms in patients treated with thiopurine. Significant associations between NUDT 15 c.415C > T polymorphism and leukopenia were found in all genetic models (TC/TT vs CC, OR: 7.64, 95% CI: (6.19, 9.44), P<0.00001; TT vs CC/TC, OR: 29.66, 95% CI: (12.31, 71.46), P<0.00001; TT vs CC, OR: 45.60, 95% CI: (18.84, 110.37), P<0.00001; TC vs CC, OR: 6.41, 95% CI: (5.19, 7.94), P<0.00001; TT vs TC, OR: 6.38, 95% CI: (2.59, 15.72), P<0.00001), early/late leukopenia (in recessive and co-dominant model), leukopenia (grade 3–4), and severe hair loss in all genetic models. Besides, c.52G > A and 36_37insGGAGTC polymorphisms were also significantly associated with leukopenia. No significant association between NUDT 15 c.415C > T polymorphism and early/late leukopenia in the Chinese population was determined in the co-dominant model (TC vs CC).
Implications: NUDT 15 c.415C > T polymorphism could increase the risk of leukopenia, early/late leukopenia, leukopenia (grade 3–4), and severe hair loss. Meanwhile, c.52G > A and c.36_37insGGAGTC mutations also probably increase the risk of leukopenia. Preemptive tests for NUDT 15 polymorphisms are highly recommended to individualize the treatment of thiopurine for a better outcome with less toxicity.
Keywords: NUDT 15, polymorphism, leukopenia, thiopurine, intolerance, meta-analysis
Introduction
As indispensable immunosuppressive and anticancer agents, thiopurines (azathioprine and 6-mercaptopurine), are widely used for maintenance therapy of child acute lymphoblastic leukemia (ALL), organ transplantation, autoimmune diseases, including rheumatoid arthritis (RA) and inflammatory bowel disease (IBD).1,2 However, due to highly variable individual response, thiopurines can cause severe toxicities, mainly leukopenia, resulting in therapy disruption, thiopurine dose reduction, even increasing the risk of relapse, and life-threatening infection.3–5
Thiopurines are metabolized into their active metabolites, 6-thioguanine nucleotides (6-TGNs), by a series of enzymes. 6-TGNs consist of 6-thio(d)-GMP, 6-thio(d)-GDP, 6-thio(d)-GTP, and 6-thio(d)-GTPs are incorporated into DNA and RNA, causing inhibition of nucleotide and protein synthesis, and an over accumulation of them can result in toxicity typified by leukopenia.6
Thiopurine methyltransferase (TPMT) is an imperative metabolic enzyme of 6-TGNs. Inherited deficiency of TPMT with a decreased enzymatic activity can lead to an increased level of 6-TGNs, thus causing hematological toxicity.7 The association between thiopurine-induced leukopenia and TPMT variants has been assured, and, consequently, preemptive TPMT testing is recommended to individualize thiopurines dose to reduce the risk of adverse effects by the US Food and Drug Administration without compromising overall therapeutic efficacy.8–10 However, a large proportion of patients with normal TPMT activity still experience severe leukopenia. Intriguingly, despite the fact that the frequency of TPMT variants in Asians is lower than in European descent (~3% vs ~10%),11,12 thiopurine-induced leukopenia, and thiopurines intolerance occur more in Asians, which indicates that additional factors might contribute to the variability among different races.13,14
Recently, Moriyama, T15 reported that a novel indicator, NUDT 15, could convert the thiopurine active metabolites 6-thio-GTP and 6-thio-dGTP into 6-thio-GMP and 6-thio-dGMP and that the variants of NUDT 15 had lower enzyme activity. Thus, NUDT 15 deficiency directly results in excessive levels of thiopurine active metabolites 6-thio-GTP and 6-thio-dGTP, and increased host toxicity. And a series of studies found that NUDT 15 polymorphism was possibly associated with thiopurine-induced leukopenia and thiopurine intolerance and severe hair loss.16,17 Heretofore, both two published systematic reviews/meta-analyses18,19 (Table 1) revealed that the NUDT 15 c.415C > T mutation could increase the risk of thiopurine-induced leukopenia and thiopurine intolerance. However, studies included in the two systematic reviews and meta-analyses did not provide sufficient data to deeply delve into the effects of NUDT 15 c.415C > T polymorphism on other thiopurine-related toxicities such as early/late leukopenia, leukopenia (Grade 3–4), and severe hair loss. Whereas, within the past two years, nearly 10 related studies were newly published and need to be included and reanalyzed to observe whether the results change. In addition, the updated data about whether early leukopenia (<8 weeks), late leukopenia (>8 weeks), leukopenia (grade 3–4), and severe hair loss could be caused by NUDT 15 c.415C > T polymorphism, necessitates to be synthesized to provide a convincing evidence. Besides, several recent studies also explored the effect of two other NUDT 15 polymorphisms (c.52G > A and c.36_37insGGAGTC) on leukopenia. In light of this information, we performed a meta-analysis to assess the possible association between the three NUDT 15 polymorphisms and thiopurine-induced toxicities.
 |
Table 1 Characteristic of published systematic reviews/meta-analyses |
Materials and methods
Search strategy
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement. We searched relevant literature published before 3 June 2018 from three databases: PubMed, Embase, and Web of Science, for cohort studies and case–control studies exploring the association between NUDT 15 polymorphism and thiopurine-induced leukopenia and thiopurine intolerance. We also manually searched references of relevant studies and reviews to identify other additional articles which were not retrieved by the initial search. Only English language articles were searched and only human studies were included. The following subject terms and keywords were used to search those databases: (NUDT 15 protein) odds ratio (OR) (NUDT 15 gene) OR (NUDT 15) OR (NUDT 15 variant) OR (nudix hydrolase 15) OR (nucleoside diphosphate-linked moiety X-type motif 15) OR (MTH2 protein).
Study selection
Two reviewers (RLW and BGL) independently read the article titles and abstracts for relevant papers according to the inclusion and exclusion criteria. If there was any disagreement, a third independent reviewer (JPL) would be consulted. Inclusion criteria: 1) patients were treated with Mercaptopurine (MP/6-MP) or Azathioprine (AZA); 2) studies provided the patients’ genotypes for any one of the newly found NUDT 15 polymorphisms; 3) studies investigated the association between NUDT 15 polymorphism and thiopurine-related toxicities; and 4) case–control studies or cohort studies. Exclusion criteria: 1) case reports, reviews, meeting abstracts, short communication, comments, and studies with inadequate NUDT 15 gene frequency data; 2) full text could not be retrieved for further assessment; and 3) studies with complete duplicated data. If there was incomplete overlapping data in one author’s several papers, we would select the article with the updated data or combine those papers to provide more detailed data.
Data extraction and quality assessment
The following data were extracted from included studies by two independent investigators (RLW and BGL): first author’s name, year of publication, study design, sample size, disease type, ethnicity, age, gender, medication, 6-MP/AZA initial daily dosage, NUDT 15 gene sites, genotype, Hardy–Weinberg equilibrium ( HWE) value for each NUDT 15 polymorphism, thiopurine-induced toxicities, defined grade of leukopenia, and thiopurine tolerated dose. If some specific data were not provided, correspondence authors of papers were contacted by e-mail. The two investigators also applied Newcastle–Ottawa Quality Assessment Scale (NOS) to assess the quality of included studies. A third independent investigator (JPL) was consulted to resolve any discrepancies.
Statistical analysis
We used the Review Manager (Revman) 5.3 version to perform the meta-analysis. We used the overall pooled OR with a corresponding 95% confidence interval (95%CI) to assess each included study. Cochran’s Q statistic and I2 tests were used to assess the heterogeneity among these included studies. A P>0.05 for the Q test or the I2 test value <50% indicates that there was no significant heterogeneity in these studies and a fixed-effects model was used. Otherwise, a random-effects model would be used. And meanwhile, we would explore the reasons for heterogeneity by sensitivity analysis and by performing a subgroup analysis. A Z test was used to evaluate the association between the NUDT 15 polymorphisms and its clinical outcomes by calculating the significance of the pooled ORs and a P<0.05 level represented to be statistically significant.
Results
Selection and characteristics of the eligible studies
Study selection process is depicted in Figure 1. In total, 198 records were initially identified from the three databases. Titles and abstracts of 97 records were screened carefully after overlapping records were removed and 50 records were evaluated to be irrelevant and were excluded. The full-texts of the remaining 47 studies were retrieved and reviewed. Among them, 31 studies were excluded: 7 reviews or meta-analysis; 5 case reports; 2 short communications; 1 comment; 4 studies with continuous variables data, which could not be transformed into dichotomous variables; 5 studies with overlapping data; and 7 articles without available full-texts. Finally, 16 studies met the inclusion criteria, including 5 pediatric studies,15,16,20–23 9 adult studies,24-33 and 2 both pediatric and adult studies.17,34
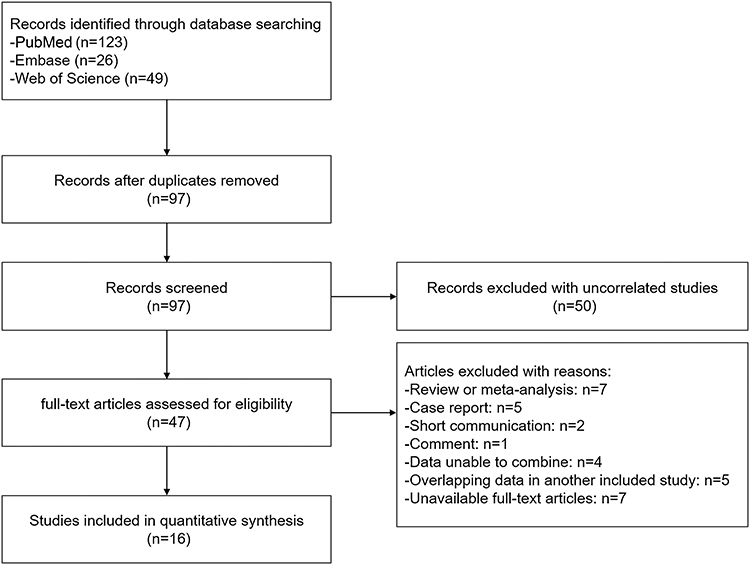 |
Figure 1 Flow diagram of study. |
A total of 4458 subjects were included in the 16 studies, of which, 11 studies16,17,21,22,24–27,31,32,34 only examined NUDT 15 c.415C > T polymorphism, one study23 examined both NUDT 15 c.415C > T and c.52G > A gene, three studies28–30 examined three NUDT 15 polymorphisms: c.415C > T, c.52G > A, and c.36_37insGGAGTC and one study15 examined all the found NUDT 15 polymorphisms: c.415C > T, c.52G > A, c.36_37insGGAGTC, and c.416 G > A. For the ethnicity, population in most of studies were Asians: Japanese in six studies,21,23,25,26,29,32 Korean in three studies,17,24,34 Chinese in three studies,22,27,30 Indian in one study,31 and mixed population in three studies.15,16,28 With regard to disease type, there were five studies15,16,21–23 of ALL, eight studies17,24–30 of IBD or CD, one study32 of RA and two studies31,34 of mixed diseases. The characteristics of studies included in the meta-analysis are provided in Table 2.
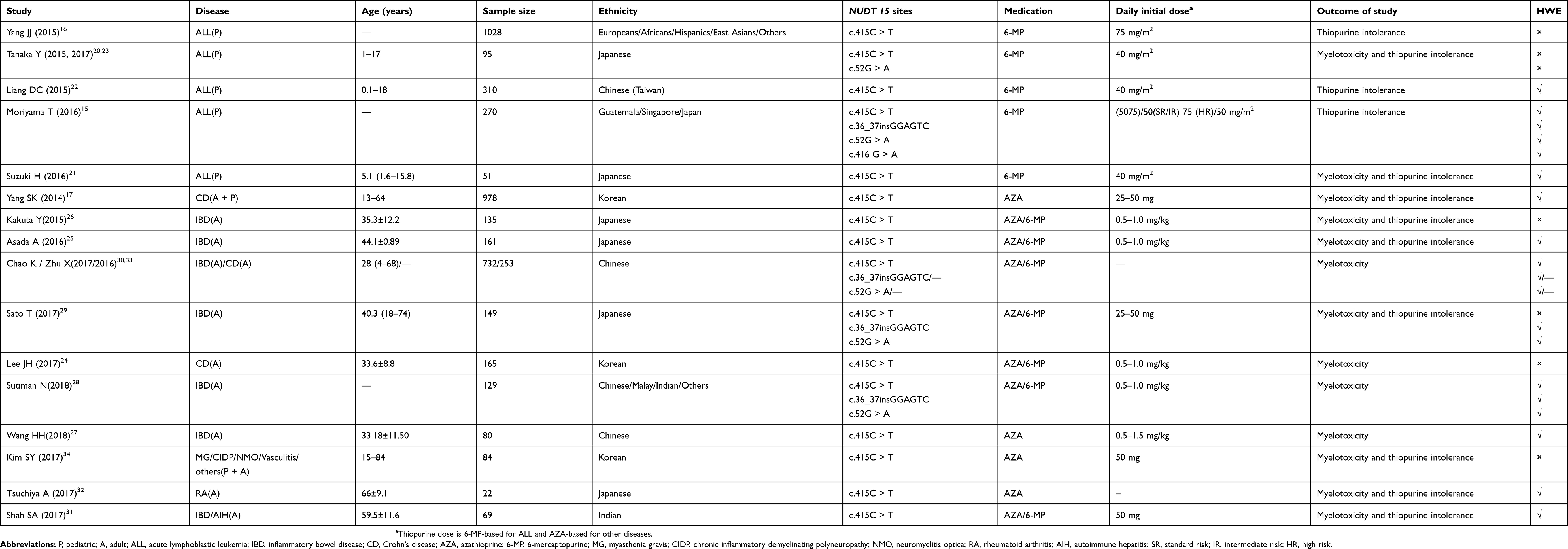 |
Table 2 Characteristics of included studies in the meta-analysis |
Quality of studies
The result of quality assessment for all the 16 cohort studies is shown in Table 3 with a total score ranging from 7 to 9 based on the NOS criteria (cohort study), which indicated a relatively high quality. Most of the studies represented well in selection and comparability but not in outcome due to lack of long-term follow-up.
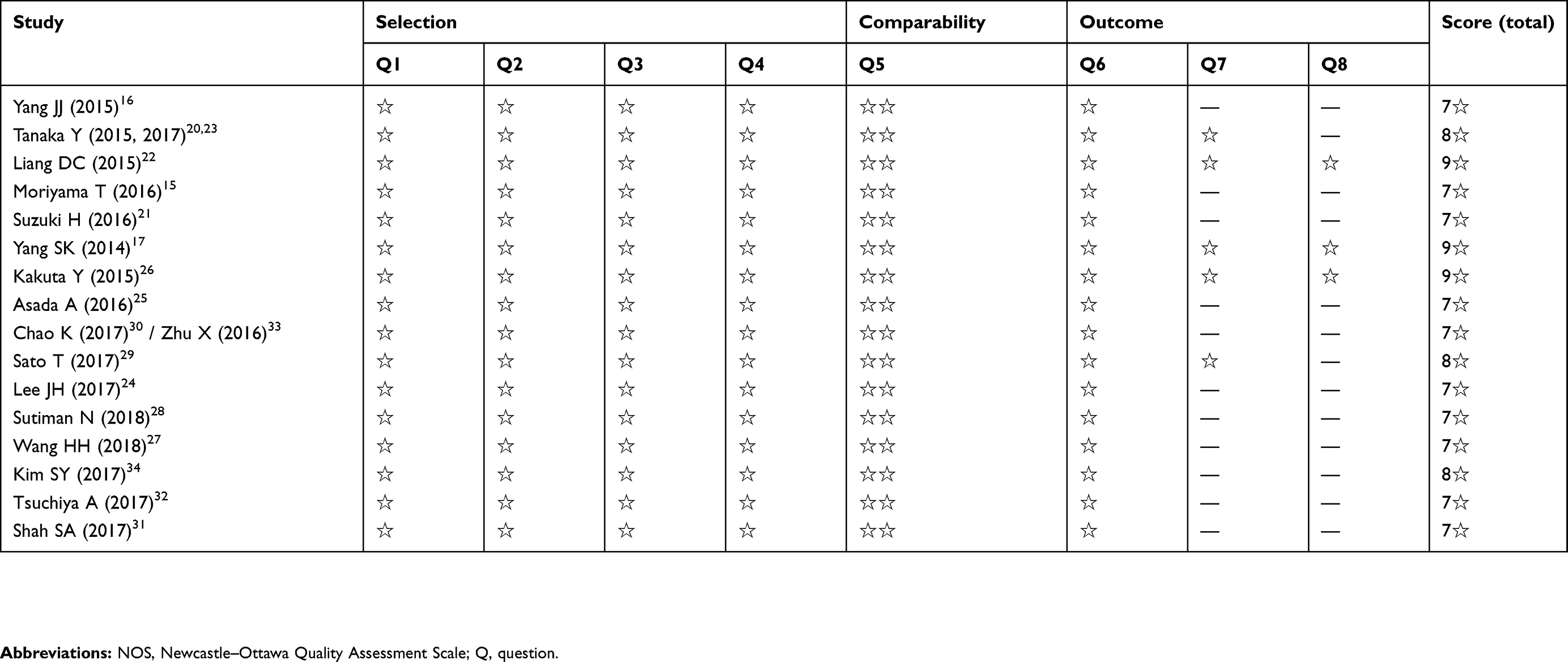 |
Table 3 The quality of studies included in meta-analysis with the method of NOS |
Outcome of all the included studies
The association between NUDT 15 c.415C > T polymorphism and thiopurine-induced toxicities was investigated in the 16 studies. The effects of NUDT 15 c.52G > A and c.36_37insGGAGTC polymorphisms on the thiopurine-induced leukopenia were also separately researched in three,20,29,30 and three28–30 studies. Detailed data are shown in Table 4.
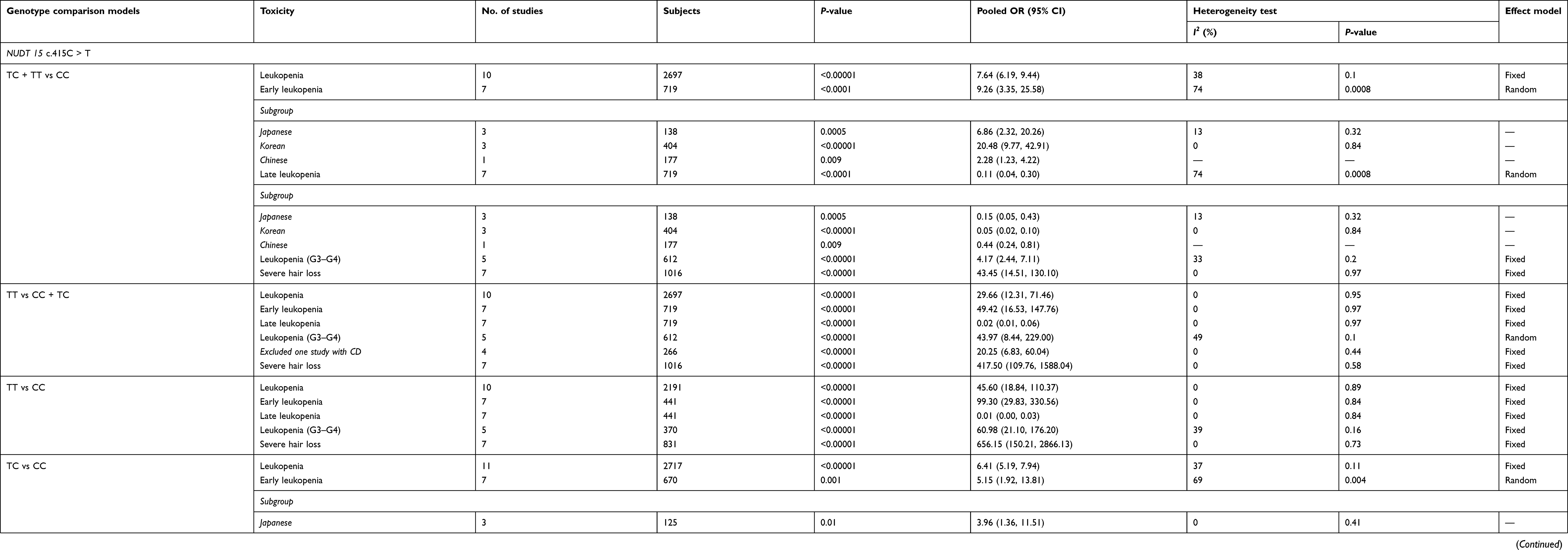 |
Table 4 Pooled odds ratios of the association between NUDT 15 polymorphism and thiopurine-induced toxicities |
Association between NUDT 15 c.415C > T polymorphism and thiopurine-induced toxicities
A statistically significant association between the NUDT 15 c.415C > T polymorphism and leukopenia was found in all genetic models (TC/TT vs CC, OR: 7.64, 95% CI: 6.19–9.44, P<0.00001; TT vs CC/TC, OR: 29.66, 95% CI: 12.31–71.46, P<0.00001; TT vs CC, OR: 45.60, 95% CI: 18.84–110.37, P<0.00001; TC vs CC, OR: 6.41, 95% CI: 5.19–7.94, P<0.00001; TT vs TC, OR: 6.38, 95% CI: 2.59–15.72, P<0.00001; (Figure 2 and Table 4).
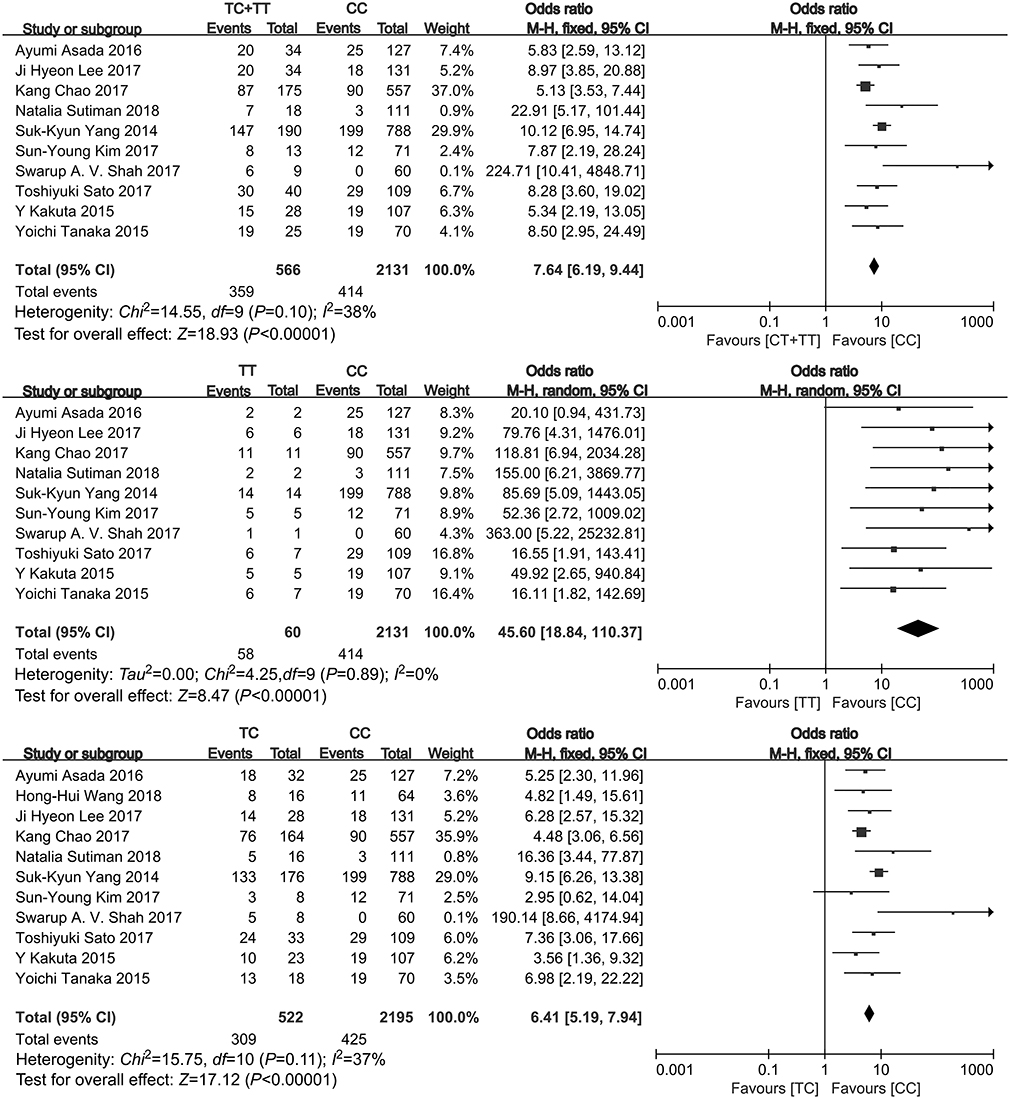 |
Figure 2 The forest plots for the meta-analysis of association between NUDT 15 c.415C > T polymorphism and risk of leukopenia in the dominant model and co-dominant model. |
Seven studies, which provided data on early leukopenia (<8 weeks) and late leukopenia (≥8 weeks), showed that NUDT 15 c.415C > T polymorphism is significantly associated with early leukopenia and late leukopenia in the recessive model (TT vs CC/TC, OR: 49.42, 95% CI: 16.53–147.76, P<0.00001; OR: 0.02, 95% CI: 0.01–0.06, P<0.00001), co-dominant model (TT vs CC, OR: 99.30, 95% CI: 29.83–330.56, P<0.00001; OR: 0.01, 95% CI: 0.00–0.03, P<0.00001) and the model (TT vs TC, OR: 23.73, 95% CI: 7.77–72.46, P<0.00001; OR: 0.04, 95% CI: 0.01–0.13, P<0.00001). A subgroup analysis (Figure 3) was conducted to check the influences of ethnicity on the association between c.415C > T and the early leukopenia and late leukopenia without significant heterogeneity. The results showed a significant effect not only in the Japanese race in the dominant model (TC/TT vs CC, OR: 6.86, 95% CI: 2.32–20.26, P=0.0005; OR: 0.15, 95% CI: 0.05–0.43, P=0.0005) and co-dominant model (TC vs CC, OR: 3.96, 95% CI: 1.36–11.51, P=0.01; OR: 0.25, 95% CI: 0.09–0.73, P=0.01), but also in the Korean race in its dominant model (TC/TT vs CC, OR: 20.48, 95% CI: 9.77–42.91, P<0.00001; OR:0.05, 95% CI: 0.02–0.10, P<0.00001) and co-dominant model (TC vs CC, OR: 13.57, 95% CI: 6.34–29.05, P<0.00001; OR: 0.07, 95% CI: 0.03–0.16, P<0.00001). However, the significant effect was only in the Chinese in the dominant model (TC/TT vs CC, OR: 2.28, 95% CI: 1.23–4.22, P=0.009; OR:0.44, 95% CI: 0.24–0.81, P=0.009), but not in that co-dominant model (TC vs CC, OR: 1.70, 95% CI: 0.89–3.22, P=0.11; OR: 0.59, 95% CI: 0.31–1.12, P=0.11) (Table 4).
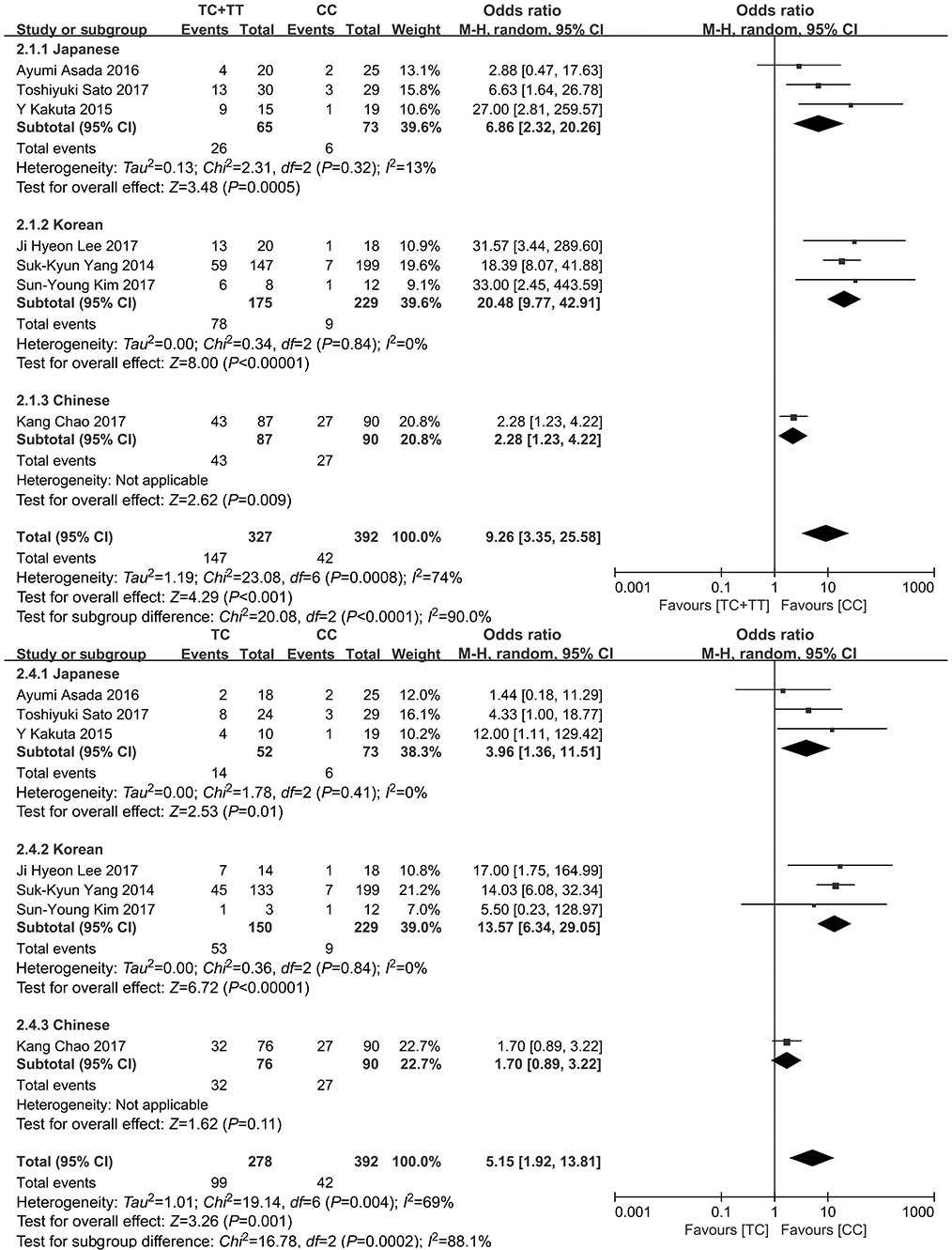 |
Figure 3 The forest plots for the meta-analysis of association between NUDT 15 c.415C > T polymorphism and risk of early leukopenia in the dominant model and co-dominant model. |
Five studies (612 subjects), which mentioned the leukopenia (grade 3–4), revealed significant effects in the dominant model (TC/TT vs CC, OR:4.17, 95% CI: 2.44–7.11, P<0.00001), co-dominant model (TT vs CC, OR: 60.98, 95% CI: 21.10–176.20, P<0.00001), co-dominant model (TC vs CC, OR: 2.38, 95% CI: 1.22–4.64, P=0.01), and the model (TT vs TC, OR: 28.77, 95% CI: 10.89–76.03, P<0.0001). A significant effect was also found in the recessive model (TT vs CC/TC, OR: 20.25, 95% CI: 6.83–60.04, P<0.00001) after excluding one study with CD (Table 4).
An obvious difference between NUDT 15 c.415C > T polymorphism and tolerated thiopurine dose was observed in child ALL and IBD patients. (Figure 4).
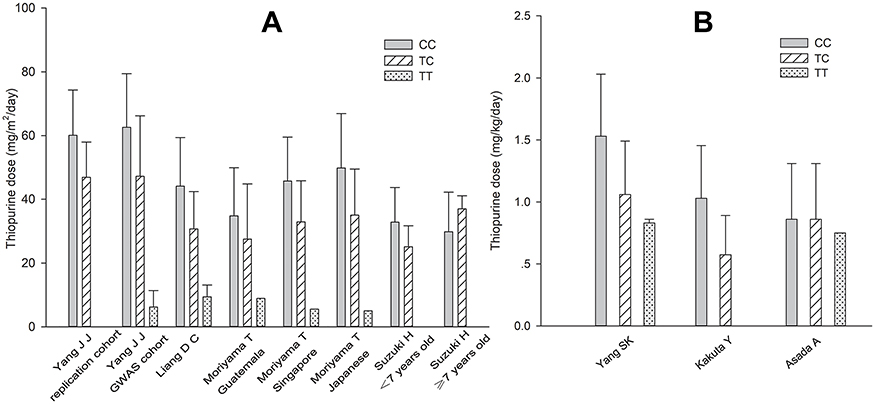 |
Figure 4 Bar plot of NUDT 15 c.415C > T genotype and the average of 6-MP/AZA among child ALL patients with 6-MP (A), and IBD patient with AZA (B) in included studies. Each bar includes data with bar height and error bar separately indicating mean and standard deviation of tolerated thiopurine dose. <7 years, the younger age group (under 7 years old); ≥7 years, the older age group (above 7 years old or older).Abbreviations: ALL, acute lymphoblastic leukemia; IBD, inflammatory bowel disease; 6-MP, 6-mercaptopurine; AZA, azathioprine. |
A significant association between the NUDT 15 c.415C > T polymorphism and severe hair loss was observed in all genetic models (TC/TT vs CC, OR: 43.45, 95% CI: 14.51–130.10, P<0.00001; TT vs CC/TC, OR: 417.50, 95% CI: 109.76–1588.04, P<0.00001; TT vs CC, OR: 656.15, 95% CI: 150.21–2866.13, P<0.00001; TC vs CC, OR: 26.18, 95% CI: 4.73–144.95, P<0.00001; TT vs TC, OR: 66.29, 95% CI: 17.46–251.74, P<0.00001) (Figure 5 and Table 4).
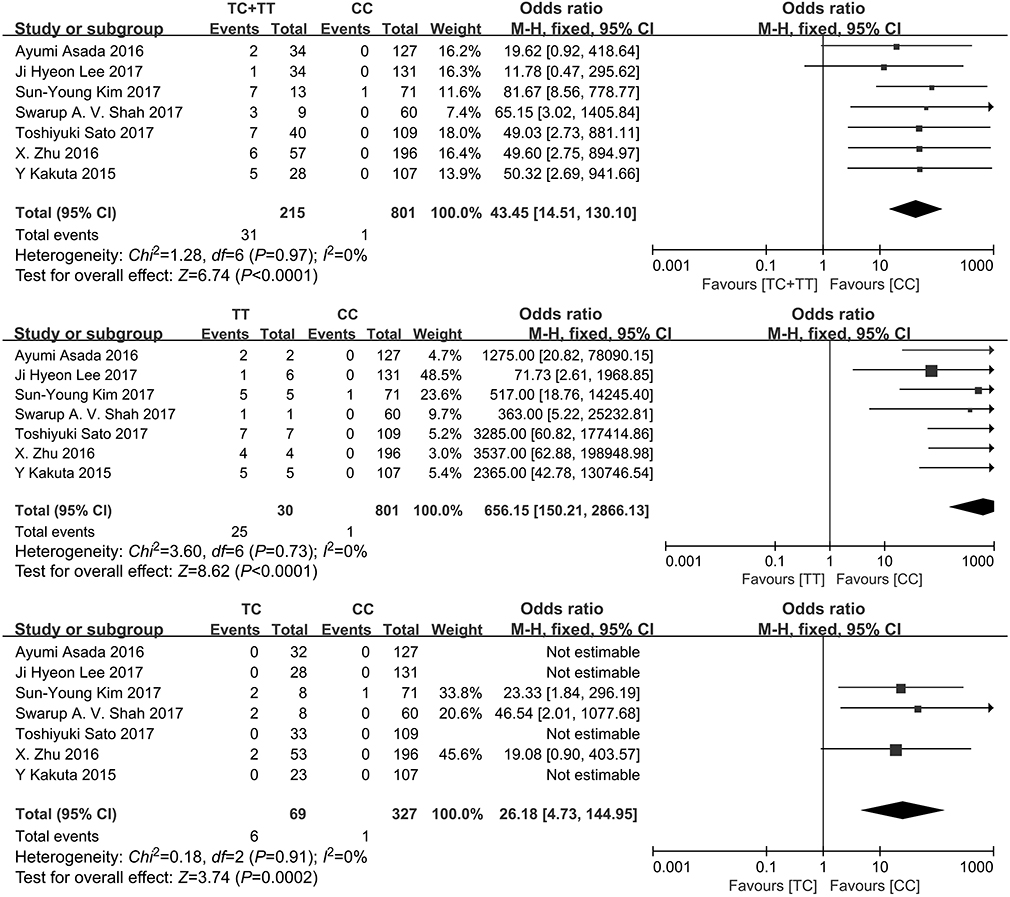 |
Figure 5 The forest plots for the meta-analysis of association between NUDT 15 c.415C > T polymorphism and risk of severe hair loss in the dominant model and co-dominant model. |
Association between NUDT 15 c.52G > A polymorphism and thiopurine-induced leukopenia
Three studies with 975 subjects presented a significant association between c.52G > A polymorphism and thiopurine-induced leukopenia in the co-dominant model (GA vs GG, OR: 3.52, 95% CI: 1.52–8.17, P=0.003) (Figure 6).
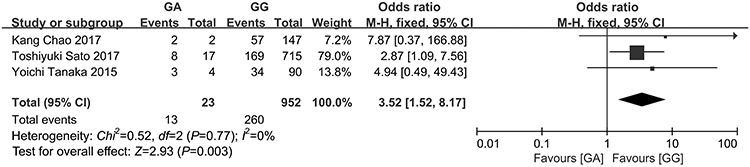 |
Figure 6 The forest plots for the meta-analysis of association between NUDT 15 c.52G > A polymorphism and risk of leukopenia in the co-dominant model. |
Association between NUDT 15 36_37insGGAGTC polymorphism and thiopurine-induced leukopenia
A significant association between 36_37insGGAGTC polymorphism and thiopurine-induced leukopenia was observed in the co-dominant model (-/ins vs -/-, OR: 3.84, 95% CI: 2.50–5.91, P<0.00001) (Figure 7).
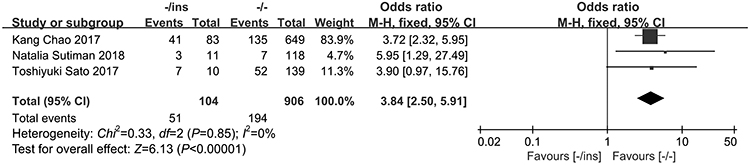 |
Figure 7 The forest plots for the meta-analysis of association between NUDT 15 c.36_37insGGAGTC polymorphism and risk of leukopenia in the co-dominant model. |
Heterogeneity and sensitivity analysis
Some significant heterogeneity results between studies were identified when we conducted the meta-analysis. Thus, a random-effect model was performed and the root of heterogeneity was evaluated by subgroup analysis for ethnicity (Table 4). Heterogeneity might also be derived from different diseases, dosage criteria, sample size, or other factors. One study17 with CD, different from other studies with IBD, was excluded and finally I2 of the recessive model in leukopenia (grade 3–4) remarkably decreased to less than 50%.
Discussion
To the best of our knowledge, this meta-analysis provides a comprehensive assessment of the association between three NUDT 15 polymorphisms and specific types of thiopurine-induced leukopenia, and thiopurine intolerance and severe hair loss. After conducting a systematic search across three databases, 16 articles were identified and were eligible for inclusion. The main findings were that NUDT 15 c.415C > T mutation can significantly increase the risks of thiopurine-induced leukopenia, early leukopenia, leukopenia (grade 3–4), and severe hair loss and thiopurine intolerance. Besides, both c.52G > A and c.36_37insGGAGTC were significantly associated with the increased risk of leukopenia. However, the study number and sample size for the two newly found gene mutation sites were relatively small. Thus, further studies on c.52G > A and c.36_37insGGAGTC are needed to demonstrate the association convincingly.
No significant association between c.415C > T and early leukopenia and late leukopenia by subgroup analysis was found in only one Chinese study in the co-dominant model (TC vs CC) in our meta-analysis, which indicated that more studies about the effect of NUDT 15 c.415C > T polymorphism on early/late leukopenia in Chinese patients were needed to verify this conclusion.
Both the two published systematic reviews/meta-analyses, Yin, D.D.19 (2750 subjects) and Zhang, A.L.18 (1138 subjects) revealed that NUDT 15 c.415C > T mutation could increase the risk of leukopenia, which is in agreement with our findings (4458 subjects). Different from them, we also explore the effect of c.415C > T polymorphism on early/late leukopenia, leukopenia (grade 3–4), and severe hair loss, which could provide physicians with more helpful details such as when leukopenia occurs, how severe leukopenia is, and whether severe hair loss brings patients about anxiety and thiopurine discontinuation. Although, Yin, D.D.19 probed into the impact of NUDT 15 c.415C > T polymorphism on thiopurine intolerance, the results only presented that the c.415C > T is associated with thiopurine intolerance in dominant model (TT + TC vs CC) and did not provide further information in other models, from which more specific relative effects could not be read. Besides, it is not appropriate to combine the thiopurine tolerated dose of patients with TT genotype and patients with TC genotype. While we used a bar plot to represent a visualized relative effect for tolerated thiopurine dose among c.415C > T three genotypes both in child ALL and IBD patients instead of synthesizing the data into a meta-analysis, due to insufficient data and difficulty in dose unit mutual conversion between mg/kg and mg/m2. And from the bar plot, we can observe that in child ALL patients, thiopurine tolerated dose of c.415C > T homozygous variants is lowest and followed by heterozygous variants and wild-type patients except in the older age group (above 7 years old or older) in Suzuki, H.’s study.21 However, this study only included 51 patients, and we need more convincing studies to investigate whether c.415C > T polymorphism has different effects on thiopurine tolerated dose between different age groups. Besides, due to the thiopurine dose for pediatric ALL patients being higher than those for IBD patients, the effect of the c.415C > T polymorphism on thiopurine tolerated dose in IBD patients was not the same obvious effect as the effect in child ALL patients.
Besides the thiopurine-induced specific types of leukopenia, thiopurine intolerance and severe hair loss, several studies also explored whether NUDT 15 c.415C > T polymorphism can affect other aspects in thiopurine treatment, such as co-effect with TPMT mutation, therapy interrupted days, relapse, 5-year event-free survival, and 6-TGNs. Therefore, it can provide us additional information to optimize treatment protocols and improve the clinical outcomes. Yang, J.J.16 revealed that patients with both TPMT and NUDT 15 variants required greater dose reductions compared with heterozygous variants at only one of the two loci, indicating additive effects of the two genes on thiopurine intolerance. Yi, E.S.35 indicated that patients with the NUDT 15 c.415C > T mutation are likely to have longer therapy interrupted days (P<0.01). Both Tanaka, Y.20 and Suzuki, H.21 observed that there existed no significant association between NUDT 15 c.415C > T polymorphism and increased risk of relapse. Similarly, Liang, D. C.22 also found NUDT 15 c.415C > T polymorphism was not significantly associated with 5-year event-free survival. Sutiman, N28 did not discover significant differences between NUDT 15 c.415C > T genotypes and 6-TGNs levels after adjustments for thiopurine doses. And Moriyama, T36 further found the ratio of thio-d-GTP (TdGTP) to TGN (the percent of TGN converted to TdGTP) was significantly higher in NUDT 15-deficient patients (P=3.6×10−9). So far, due to the limit number of studies, the data of those outcomes could not be synthesized to provide a more persuasive conclusion. Thus, further studies with a larger sample size, multiple centers, and rational designs should be conducted to better evaluate the impacts of the NUDT 15 polymorphisms on those newly found outcomes.
Several limitations of our meta-analysis are as follows. Firstly, the diseases of included studies were not limited to a single one and different treatment protocols were applied to different diseases, which possibly influenced the accuracy of the thiopurine-induced toxicities combination. Secondly, studies included in this meta-analysis adopted different chemotherapy regiments of thiopurines even for the same disease, and various thiopurines doses, duration of thiopurines, and combined chemotherapy agents might influence the occurrence of thiopurine toxicities to some extent. Thirdly, different toxicity criteria in those studies would also weaken the reliability of the results in some extent. Therefore, further studies with a larger sample size, multiple centers, and rational designs should be conducted to better evaluate the association between the NUDT 15 polymorphism and increased risk of thiopurine-induced toxicities for each single disease, especially in Asians.
Conclusion
In conclusion, this meta-analysis confirms that the NUDT 15 c.415C > T polymorphism, especially in Asians, is significantly associated with thiopurine-induced leukopenia, early/late leukopenia, leukopenia (grade 3–4), and severe hair loss. Meanwhile, c.52G > A and c.36_37insGGAGTC mutations also probably increase the risk of leukopenia. Thus, preemptive tests for the genotypes of NUDT 15 polymorphisms are highly recommended to individualize the treatment of thiopurines for a better outcome with less toxicity. However, better-designed and larger trials and further investigations for each single disease conducted separately for pediatrics and adults are required to provide more detailed and applicable conclusions for a better thiopurine-based clinical therapeutic outcome.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this study type informed consent is not required.
Acknowledgments
This work was supported by the Natural Science Foundation of Beijing [No. 7171004] and major project of National Science and Technology “creation of major new drugs” [No: 2018ZX09721003].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chande N, Patton PH, Tsoulis DJ, Thomas BS, MacDonald JK. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev. 2015;10:D67. doi:10.1002/14651858.CD000067.pub3.
2. Timmer A, Patton PH, Chande N, McDonald JW, MacDonald JK. Azathioprine and 6-mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2016;5:D478. doi:10.1002/14651858.CD000478.pub4.
3. Goldberg R, Irving PM. Toxicity and response to thiopurines in patients with inflammatory bowel disease. Expert Rev Gastroenterol Hepatol. 2015;9:891–900. doi:10.1586/17474124.2015.1039987
4. Frandsen TL, Abrahamsson J, Lausen B, et al. Individualized toxicity-titrated 6-mercaptopurine increments during high-dose methotrexate consolidation treatment of lower risk childhood acute lymphoblastic leukaemia. A Nordic Society of Paediatric Haematology and Oncology (NOPHO) pilot study. Br J Haematol. 2011;155:244–247. doi:10.1111/j.1365-2141.2011.08835.x
5. Schmiegelow K, Bjork O, Glomstein A, et al. Intensification of mercaptopurine/methotrexate maintenance chemotherapy may increase the risk of relapse for some children with acute lymphoblastic leukemia. J Clin Oncol. 2003;21:1332–1339. doi:10.1200/JCO.2003.04.039
6. Kakuta Y, Kinouchi Y, Shimosegawa T. Pharmacogenetics of thiopurines for inflammatory bowel disease in East Asia: prospects for clinical application of NUDT15 genotyping. J Gastroenterol. 2018;53:172–180. doi:10.1007/s00535-017-1416-0
7. Relling MV, Hancock ML, Rivera GK, et al. Mercaptopurine therapy intolerance and heterozygosity at the thiopurine S-methyltransferase gene locus. J Natl Cancer Inst. 1999;91:2001–2008. doi:10.1093/jnci/91.23.2001
8. Yates CR, Krynetski EY, Loennechen T, et al. Molecular diagnosis of thiopurine S-methyltransferase deficiency: genetic basis for azathioprine and mercaptopurine intolerance. Ann Intern Med. 1997;126:608–614. doi:10.7326/0003-4819-126-8-199704150-00003
9. Tai HL, Krynetski EY, Yates CR, et al. Thiopurine S-methyltransferase deficiency: two nucleotide transitions define the most prevalent mutant allele associated with loss of catalytic activity in Caucasians. Am J Hum Genet. 1996;58:694–702.
10. Schmiegelow K, Forestier E, Kristinsson J, et al. Thiopurine methyltransferase activity is related to the risk of relapse of childhood acute lymphoblastic leukemia: results from the NOPHO ALL-92 study. Leukemia. 2009;23:557–564. doi:10.1038/leu.2008.316
11. Collie-Duguid ES, Pritchard SC, Powrie RH, et al. The frequency and distribution of thiopurine methyltransferase alleles in Caucasian and Asian populations. Pharmacogenetics. 1999;9:37–42.
12. Kumagai K, Hiyama K, Ishioka S, et al. Allelotype frequency of the thiopurine methyltransferase (TPMT) gene in Japanese. Pharmacogenetics. 2001;11:275–278.
13. Takatsu N, Matsui T, Murakami Y, et al. Adverse reactions to azathioprine cannot be predicted by thiopurine S-methyltransferase genotype in Japanese patients with inflammatory bowel disease. J Gastroenterol Hepatol. 2009;24:1258–1264. doi:10.1111/j.1440-1746.2009.05917.x
14. Kim JH, Cheon JH, Hong SS, et al. Influences of thiopurine methyltransferase genotype and activity on thiopurine-induced leukopenia in Korean patients with inflammatory bowel disease: a retrospective cohort study. J Clin Gastroenterol. 2010;44:e242–e248. doi:10.1097/MCG.0b013e3181d6baf5
15. Moriyama T, Nishii R, Perez-Andreu V, et al. NUDT15 polymorphisms alter thiopurine metabolism and hematopoietic toxicity. Nat Genet. 2016;48:367–373. doi:10.1038/ng.3508
16. Yang JJ, Landier W, Yang W, et al. Inherited NUDT15 variant is a genetic determinant of mercaptopurine intolerance in children with acute lymphoblastic leukemia. J Clin Oncol. 2015;33:1235–1242. doi:10.1200/JCO.2014.59.4671
17. Yang SK, Hong M, Baek J, et al. A common missense variant in NUDT15 confers susceptibility to thiopurine-induced leukopenia. Nat Genet. 2014;46:1017–1020. doi:10.1038/ng.3060
18. Zhang AL, Yang J, Wang H, Lu JL, Tang S, Zhang XJ. Association of NUDT15 c.415C>T allele and thiopurine-induced leukocytopenia in Asians: a systematic review and meta-analysis. Ir J Med Sci. 2017;187:145–153. doi:10.1007/s11845-017-1608-x
19. Yin DD, Xia X, Zhang J, et al. Impact of NUDT15 polymorphisms on thiopurines-induced myelotoxicity and thiopurines tolerance dose. Oncotarget. 2017;8:13575–13585. doi:10.18632/oncotarget.14594
20. Tanaka Y, Kato M, Hasegawa D, et al. Susceptibility to 6-MP toxicity conferred by a NUDT15 variant in Japanese children with acute lymphoblastic leukaemia. Br J Haematol. 2015;171:109–115. doi:10.1111/bjh.13518
21. Suzuki H, Fukushima H, Suzuki R, et al. Genotyping NUDT15 can predict the dose reduction of 6-MP for children with acute lymphoblastic leukemia especially at a preschool age. J Hum Genet. 2016;61:797–801. doi:10.1038/jhg.2016.55
22. Liang DC, Yang CP, Liu HC, et al. NUDT15 gene polymorphism related to mercaptopurine intolerance in Taiwan Chinese children with acute lymphoblastic leukemia. Pharmacogenomics J. 2015;16:536–539. doi:10.1038/tpj.2015.75
23. Tanaka Y, Nakadate H, Kondoh K, et al. Interaction between NUDT15 and ABCC4 variants enhances intolerability of 6-mercaptopurine in Japanese patients with childhood acute lymphoblastic leukemia. Pharmacogenomics J. 2017;2:275–280. doi:10.1038/tpj.2017.12
24. Lee JH, Kim TJ, Kim ER, et al. Measurements of 6-thioguanine nucleotide levels with TPMT and NUDT15 genotyping in patients with Crohn’s disease. PLoS One. 2017;12:e188925. doi:10.1371/journal.pone.0188925
25. Asada A, Nishida A, Shioya M, et al. NUDT15 R139C-related thiopurine leukocytopenia is mediated by 6-thioguanine nucleotide-independent mechanism in Japanese patients with inflammatory bowel disease. J Gastroenterol. 2016;51:22–29. doi:10.1007/s00535-015-1142-4
26. Kakuta Y, Naito T, Onodera M, et al. NUDT15 R139C causes thiopurine-induced early severe hair loss and leukopenia in Japanese patients with IBD. Pharmacogenomics J. 2015;16:280–285. doi:10.1038/tpj.2015.43
27. Wang HH, He Y, Wang HX, et al. Comparison of TPMT and NUDT15 polymorphisms in Chinese patients with inflammatory bowel disease. World J Gastroenterol. 2018;24:941–948. doi:10.3748/wjg.v24.i8.941
28. Sutiman N, Chen S, KL L, et al. Predictive role of NUDT15 variants on thiopurine-induced myelotoxicity in Asian inflammatory bowel disease patients. Pharmacogenomics. 2018;19:31–43. doi:10.2217/pgs-2017-0147
29. Sato T, Takagawa T, Kakuta Y, et al. NUDT15, FTO, and RUNX1 genetic variants and thiopurine intolerance among Japanese patients with inflammatory bowel diseases. Intest Res. 2017;15:328–337. doi:10.5217/ir.2017.15.3.328
30. Chao K, Wang X, Cao Q, et al. Combined detection of NUDT15 variants could highly predict thiopurine-induced leukopenia in Chinese patients with inflammatory bowel disease: a multicenter analysis. Inflamm Bowel Dis. 2017;23:1592–1599. doi:10.1097/MIB.0000000000001148
31. Shah SA, Paradkar M, Desai D, Ashavaid TF. Nucleoside diphosphate-linked moiety X-type motif 15 C415T variant as a predictor for thiopurine-induced toxicity in Indian patients. J Gastroenterol Hepatol. 2017;32:620–624. doi:10.1111/jgh.13494
32. Tsuchiya A, Aomori T, Sakamoto M, et al. Effect of genetic polymorphisms of azathioprine-metabolizing enzymes on response to rheumatoid arthritis treatment. Pharmazie. 2017;72:22–28. doi:10.1691/ph.2017.6799
33. Zhu X, Wang XD, Chao K, et al. NUDT15 polymorphisms are better than thiopurine S-methyltransferase as predictor of risk for thiopurine-induced leukopenia in Chinese patients with Crohn’s disease. Aliment Pharmacol Ther. 2016;44:967–975. doi:10.1111/apt.13796
34. Kim SY, Shin JH, Park JS, et al. NUDT15 p.R139C variant is common and strongly associated with azathioprine-induced early leukopenia and severe alopecia in Korean patients with various neurological diseases. J Neurol Sci. 2017;378:64–68. doi:10.1016/j.jns.2017.04.041
35. Yi ES, Choi YB, Choi R, et al. NUDT15 variants cause hematopoietic toxicity with low 6-TGN levels in children with acute lymphoblastic leukemia. Cancer Res Treat. 2017;3:872–882. doi:10.4143/crt.2017.283
36. Moriyama T, Nishii R, Lin TN, et al. The effects of inherited NUDT15 polymorphisms on thiopurine active metabolites in Japanese children with acute lymphoblastic leukemia. Pharmacogenet Genomics. 2017;27:236–239. doi:10.1097/FPC.0000000000000282
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.