")
Back to Journals » Clinical Interventions in Aging » Volume 15
Age-Dependent Disparities in the Prevalence of Single and Clustering Cardiovascular Risk Factors: A Cross-Sectional Cohort Study in Middle-Aged and Older Adults
Authors Macek P , Zak M , Terek-Derszniak M , Biskup M , Ciepiela P , Krol H , Smok-Kalwat J, Gozdz S
Received 16 November 2019
Accepted for publication 15 January 2020
Published 5 February 2020 Volume 2020:15 Pages 161—169
DOI https://doi.org/10.2147/CIA.S238930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Pawel Macek,1,2 Marek Zak,2 Malgorzata Terek-Derszniak,3 Malgorzata Biskup,2,3 Przemyslaw Ciepiela,4 Halina Krol,2,5 Jolanta Smok-Kalwat,6 Stanislaw Gozdz2,6
1Department of Epidemiology and Cancer Control, Holycross Cancer Centre, Kielce, Poland; 2Faculty of Medicine and Health Sciences, The Jan Kochanowski University, Kielce, Poland; 3Department of Rehabilitation, Holycross Cancer Centre, Kielce, Poland; 4Clinic of Oncological Surgery, Holycross Cancer Centre, Kielce, Poland; 5Research and Education Department, Holycross Cancer Centre, Kielce, Poland; 6Clinic of Clinical Oncology, Holycross Cancer Centre, Kielce, Poland
Correspondence: Marek Zak
Faculty of Medicine and Health Sciences, The Jan Kochanowski University, Al. IX Wiekow Kielc 19, Kielce 25-317, Poland
Tel +48 41 349 6909
Fax +48 41 349 6916
Email [email protected]
Background: Cardiovascular diseases (CVDs) are the leading cause of mortality worldwide; with age acknowledged as an independent cardiovascular risk factor (CRF) in adults. Appreciating the association between age and classic CRFs is believed to boost all potential benefits of prevention.
Purpose: Assessment of the prevalence of single and clustered CRFs and their association with age.
Patients and Methods: The survey involved 4735 people (33.6% men) who were PONS project attendees aged 45– 64. The study protocol comprised the Health Status Questionnaire, general medical examination, anthropometric measurements, and blood and urine sampling. The prevalence of single and clustered CRFs (hypertension, dyslipidemia, diabetes mellitus, and obesity) in the incrementally split age groups was calculated. The incidence rate of CRFs, against their absence, was determined by Poisson regression models with robust standard errors.
Results: The prevalence of CRFs was established in 90% of the respondents. Except dyslipidemia and ≥ 1 CRFs, prevalence of risk factors increased with age, although this trend was the weakest in men. In the total group, and in women, prevalence of dyslipidemia and ≥ 1 CRFs was unrelated to age, whereas in men, it was on the rise in the younger age groups. The incidence rate of CRFs was strongly related to age, and, with the exception of dyslipidemia, was higher in the older age groups.
Conclusion: Cardiovascular risk factors are common in the adult population, while their prevalence and clustering are more prevalent in seniors. Apart from dyslipidemia, the risk of CRFs is appreciably age-related, and higher in seniors.
Keywords: age, cardiovascular disease, risk factors, prevalence, public health
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death worldwide in the developed and developing countries alike.1 According to the WHO, 17 million people die of CVDs every year. By 2030, nearly 23.6 million people are expected to die of CVDs.2 CVDs are deemed a serious hazard to public health, as well as a commonly acknowledged factor in overall health-care expenditure across the world.2,3 The increasing burden of CVDs is a major public health issue in most developing regions.3 Recent years have borne witness to a decline in the number of CVDs deaths in Poland, even though mortality is still higher than the European average.4
Hypertension, dyslipidemia, diabetes mellitus, obesity, and nicotinism are presently deemed major cardiovascular risk factors (CRFs).5,6 Originally, obesity was considered a predisposing risk factor, although nowadays, according to the American Heart Association, it has been upgraded to the principal factor.7–9 The key risk factors are additive, due to their predictive power. Consequently, total risk of CVD is the sum of respective risks arising from the incidence of major CRFs.10–14 The estimated risk of a CVD increases with the emergence of an additional CRF.15 Age is also frequently allocated into the same category.16,17 The risk of developing CVDs increases with age. It is estimated that by 2030, approx. 20% of the world’s population over 65 will have contracted CVDs.18,19
Commonly acknowledged strategy for preventing CVDs consists in reducing CRFs. Quitting a smoking habit, boosting one’s physical activity, especially in leisure time, dietary intake rich in vegetables, BMI optimization, reduction of total cholesterol concentration, increase of high-density lipoprotein cholesterol concentration, and ensuring normal blood pressure, remain the key-building blocks of both primary and secondary prevention strategy. The above-referenced CRFs have been the focus of numerous studies, the results of which, following subsequent validation, make the officially endorsed body of pertinent recommendations for the prevention of CVDs.
The present study aimed to assess the differences in the prevalence of major CRFs (hypertension, dyslipidemia, diabetes mellitus, obesity) in the 60–64 years, 55–59 years, 50–54 years, 45–49 years, 40–44 years age groups, based on quantitative determination of the proportion of subjects who had 1, ≥1, ≥2, and ≥3 CRFs, as well as the association of age with the prevalence of single, and clustered CRFs under study.
Materials and Methods
The Polish–Norwegian Study (PONS)
The PONS Project, i.e. “Establishment of infrastructure for population health research in Poland”, pursued in collaboration with Norwegian researchers, aimed at collecting population data, with a view to assessing the main determinants of individual health, and generally addressing the causes of morbidity and mortality in Poland. The PONS Project was a continuation of the International Health Monitoring (HEM) – Closing the Gap project carried out in the Oncology Centre in Warsaw. The recruitment for the PONS study, supported by a wide ranging media campaign, was entirely voluntary. Within the period spanning Sept. 2010 - Dec. 2011, all men and women aged 45–64 (n=110,000), residents of two geographically separate regions, were invited to attend the PONS study. Permanent local residents were recruited from one urban district (the city of Kielce) – 60,000 residents aged 45–64 years of whom 13% were included in the PONS sample, and from one rural district (the district of Kielce)– 50,000 residents aged 45–64 years of whom 10% were included in the PONS sample. Consequently, within 16 months, 12% (n=13,172) of the target population were recruited to the PONS study, including 4799 Kielce residents. The choice of study location was made in due consideration of acknowledged hazard patterns for major non-communicable diseases (NCDs), exposure to risk factors, level of economic development, predictability of migration flows, adequate infrastructure, and long-term commitment to Project objectives. The study protocol comprised an individual Health Status Questionnaire, medical examination, basic anthropometric measurements, and biological blood and urine sampling. The Health Status Questionnaire was applied in a direct study, collecting information on the psycho-social determinants of individual health status on interactive, structural, and behavioural levels.
Data Verification
In line with the right of access to data, the present study made use of pertinent data on PONS participants, i.e. permanent Kielce residents. The verification covered the data of 4.799 (33.7% of men) survey participants. Based on the assessment of the data completeness, all cases (n=64) of missing information necessary to define the established study endpoints (Figure 1A) were removed from the database. Finally, 4.735 (33.6% of men) participants, mean age 55.1 years, were declared eligible for a detailed analysis.
Anthropometric Measurements
Bodyweight was measured using the Tanita SC.-240 MA body composition analyzer with an accuracy of 0.1 kg. Height in an upright position was measured with a Seca height measure, in an accuracy of 0.1 cm. Body mass index (BMI) was calculated as the quotient of body weight in kg divided by the height in meters squared. Systolic (SBP) and diastolic (DBP) blood pressure was measured with blood pressure monitor Omron (Model M3 Intellisense), and subsequently calculated as an average of two consecutive measurements.
Laboratory Measurements
Fasting venous blood was sampled. Serum measurements were taken in a laboratory, in compliance with pertinent reference standards. The concentration of fasting blood glucose (FBG) in the blood serum was determined by means of the enzyme method with hexokinase. The total cholesterol (TC) was obtained by means of the cholesterol oxidase and cholesterol esterase method. The concentration of high-density lipoprotein cholesterol (HDL-C) was obtained using the direct method with TOOS and surfactant. The triglycerides (TG) concentration was determined by means of the phosphoglyceride oxidase-peroxidase method. Laboratory tests were performed with CB 350i Wiener Lab. The estimation of low-density lipoprotein cholesterol (LDL-C) level was performed using Friedewald’s equation for TG level less than 400 mg/dl.
Outcomes Definitions
Hypertension was defined as SBP≥140 mm/Hg and DBP≥90 mm/Hg, or currently self-reported hypertension under treatment with antihypertensive drugs. Diabetes mellitus was defined as fasting glucose levels above 126 mg/dl, or currently self-reported treatment for diabetes mellitus. Dyslipidemia was defined as TC≥190 mg/dl and/or HDL-C<40 mg/dl for men (HDL-C<45 mg/dl for women) and/or LDL-C≥115 mg/dl and/or TG≥150 mg/dl, or currently self-reported treatment for dyslipidemia with the cholesterol-lowering drugs. In accordance with the WHO guidelines obesity was defined as BMI≥30 kg/m2. Clustered CRF’s ≥1, ≥2, ≥3 were defined as at least one, two or three risk factors, respectively.
The Individual Health Status Questionnaire
Self-reported CRFs related to individual lifestyle (tobacco smoking status, alcohol consumption, and physical activity) were established on the basis of an individual Health Status questionnaire. Moderate to vigorous physical activity in leisure (MVPA) was calculated against the long version of the International Physical Activity Questionnaire based on the number of days and duration of physical activity in leisure time. Tobacco smoking status and alcohol consumption were categorised similarly as never (never and former), and current smoker or drinker.
Statistical Analysis
Distributions of the variables under study in the 5-year age groups were analyzed using the Kruskal–Wallis one-way analysis of variance by ranks and chi-square test. The significance of differences in the variables between respective age groups were investigated by pairwise comparison test with the Benjamini and Hochberg, or FDR (false discovery rate) P value adjustment methods. The prevalence of analysed CRFs was calculated as a quotient of the number of persons in whom the occurrence of a given CRF was found divided by the number of persons in whom the occurrence of a given CRF might have pertained to. The prevalence of single and clustered CRFs was presented as a percentage for the total group in the 5-year age groups, and by age and gender groups. Adjusted incident rate ratios (IRRs) and 95% confidence intervals (CIs) of the occurrence of analysed CRFs in comparison with the absence of CRFs were determined on the basis of Poisson regression models with robust standard errors. Covariates for adjusted IRRs included sex, smoking history, alcohol drinking, and MVPA status. P values <0.05 were considered to be statistically significant. All statistical analyses were pursued in R version 3.5.3.
Sensitivity Analysis
We carried out sensitivity analysis for the associations of analysed CRFs with age. From the database, we excluded all subjects (n=679) with self-reported: stroke or/and ischemic heart disease or/and coronary artery disease (Figure 1B) and then we fitted adjusted Poisson regression models with robust standard errors with the same set of CRFs and covariates as in the main analyses.
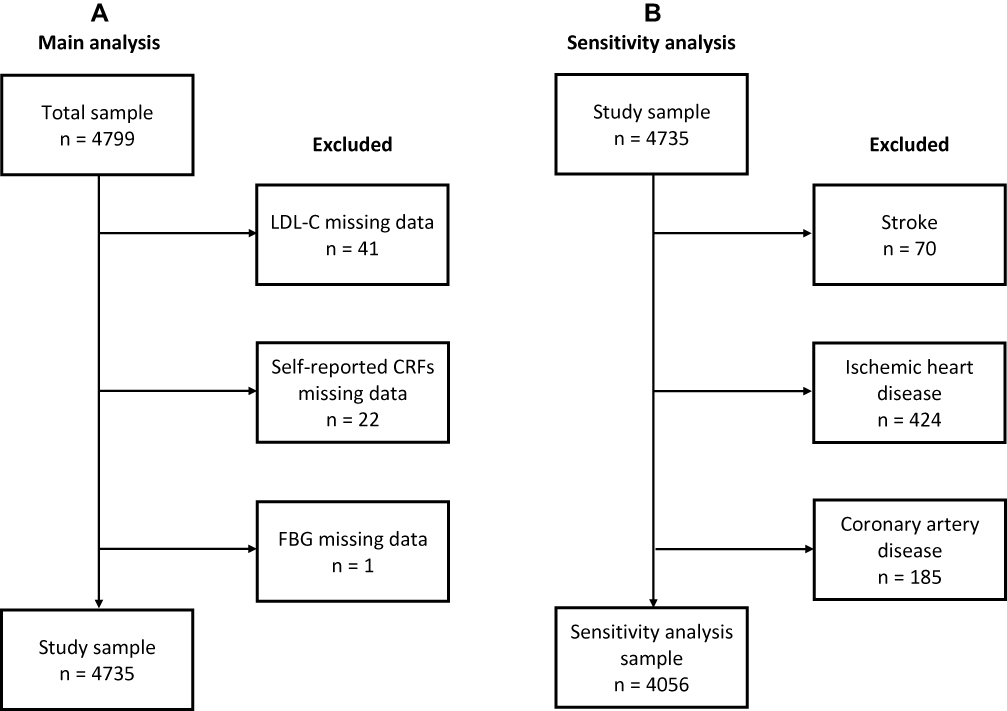 |
Figure 1 Flow diagram of data selection process in main (A) and sensitivity analysis (B). |
Results
The study was conducted on 4735 persons aged 45–64 years (mean age 55.1 years). Men constituted 33.6% of the surveyed cohort (Table 1). Starting from the age of 40, the subjects were divided into five 5-year age groups. The most numerous cohorts were represented by persons aged 55–59 years (30.8%) and 50–54 years (25.9%), and the least numerous by the ones aged 45–49 years (14.5%) and 40–44 years (3.0%). The oldest persons, aged 60–64, constituted 25.7% of the group. Average values of BMI, SBP, FBG, and frequency (Table 2) of ≥2, ≥3 CRFs in the 60–64 years age group were higher than in the younger ones. The mean values of DBP, TC, and HDL-C were significantly lower in the oldest group, as compared to the younger ones. Persons aged 60-64y were also lower in height than younger people. The differences in the variables under study were most often observed between people aged 60–64 years and 40–44 years. The differences between the oldest age group and all other groups were observed with regard to the mean values of height, BMI, SBP, FBG, and HDL-C.
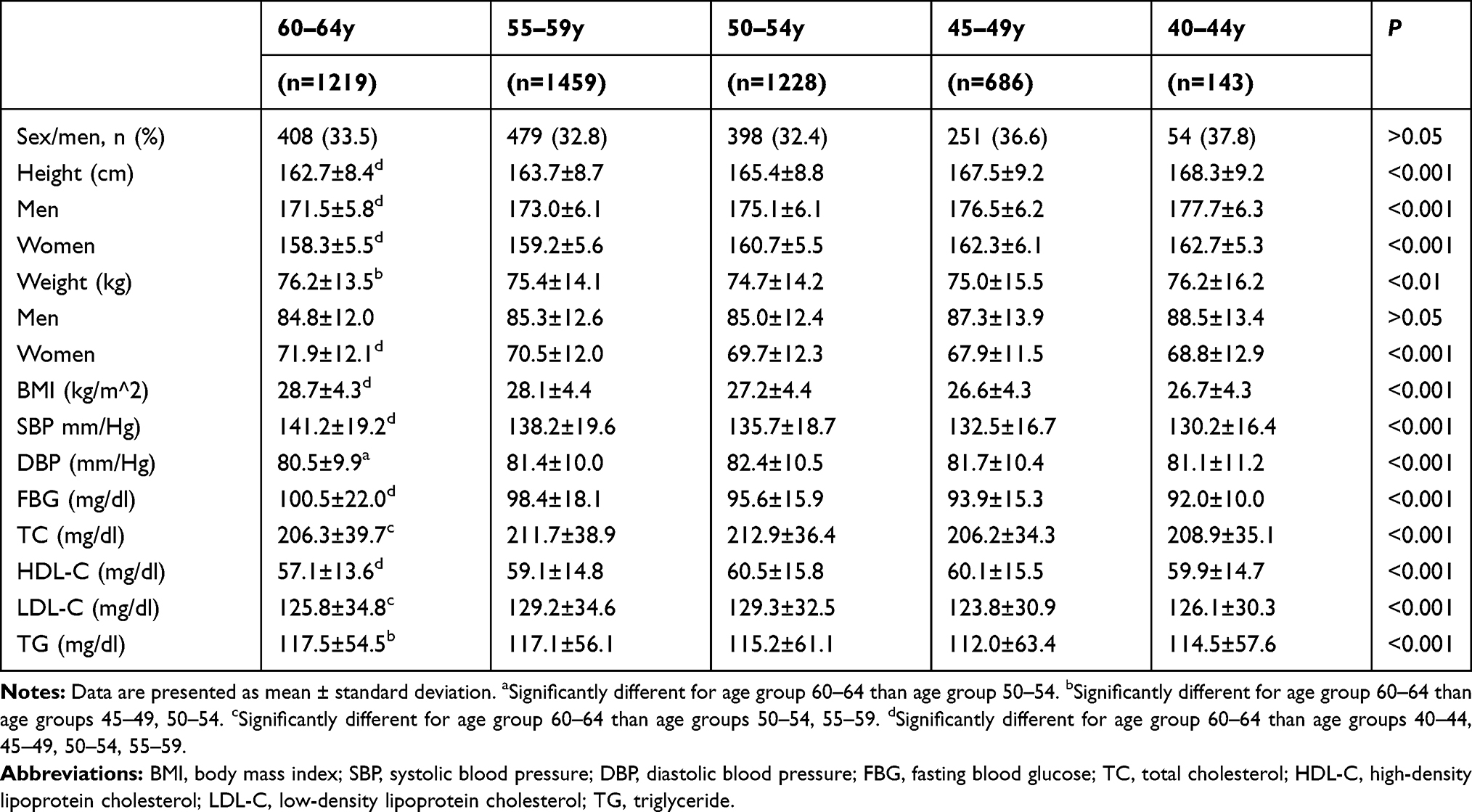 |
Table 1 Basic Characteristics of Study Group Stratified by Age Groups |
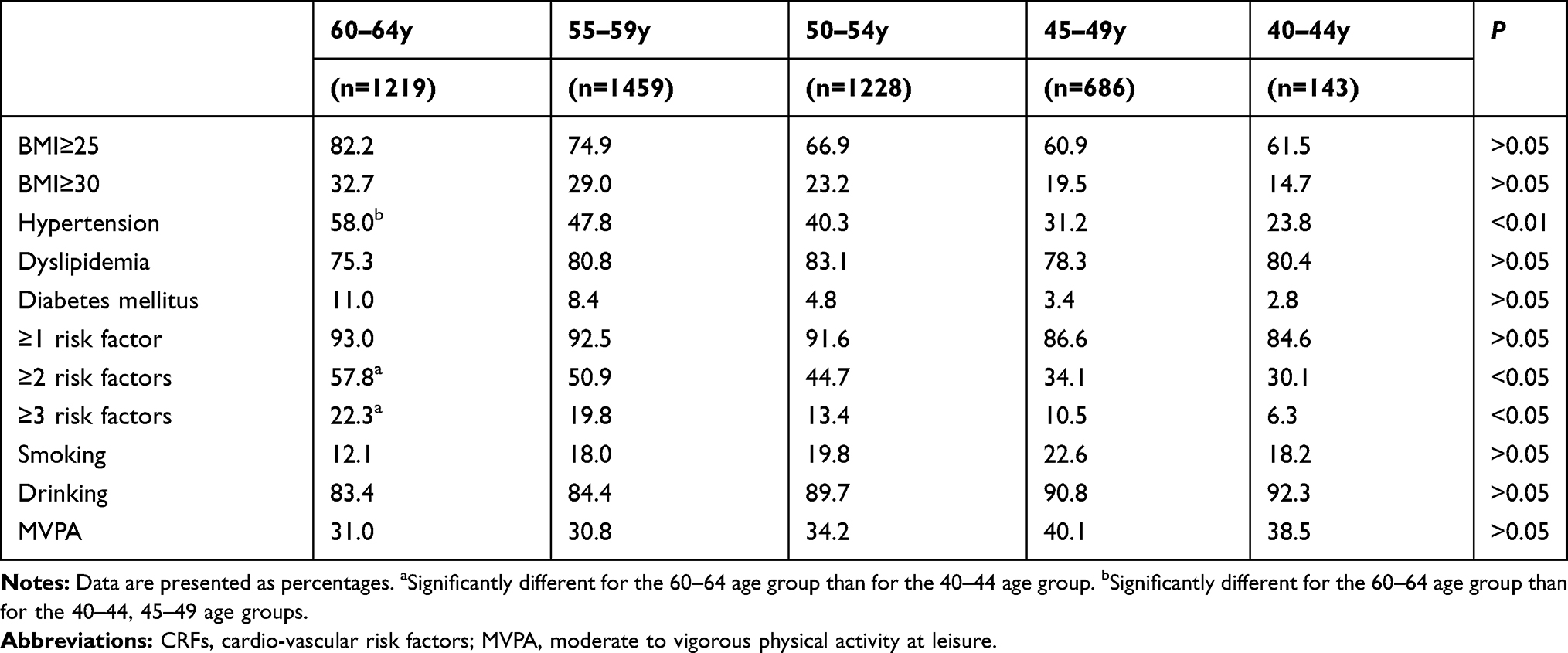 |
Table 2 Distribution Frequency of Single and Clustered CRFs, Stratified by Age Groups |
Data from 4735 participants were used to evaluate the distribution of single and clustered CRFs (Figure 2 and Table S1). Absence of risk factors was observed in 8.7% of cases (2.7% of men and 6.0% of women). In the remaining proportion of subjects, 1 or 2 CRFs were observed most frequently, i.e. 43.3% and 31.0%, respectively, whereas the most seldom – 3 or 4 CRFs, i.e. 14.5% and 2.5%, respectively. Prevalence of hypertension, diabetes mellitus, and obesity was age-related, while the prevalence of these CRFs decreased in younger age groups. Only the distribution of obesity in men, stratified by age, indicated a slightly abnormal prevalence pattern. Even though prevalence of obesity in the youngest men was the lowest, the differences between the oldest and the middle-aged men were not as pronounced as in women, nor indeed within the entire group of subjects. Prevalence of dyslipidemia in women and within the entire group had very similar, not age-related patterns. In men, unlike in the case of other CRFs, the prevalence of dyslipidemia was reported on the rise in the younger age groups. The prevalence of ≥1 CRF within the entire group and in both genders indicated very similar patterns, although with regard to men, in contrast to other groups, the highest prevalence was observed in the youngest age group. The prevalence of ≥2 and ≥3 CRFs was clearly age-related, indicating a decreasing trend in the younger age groups. The least regular associations relationship between these CRFs and age were observed in men, although in this case the highest prevalence was observed in older men, whereas the lowest one was observed in the younger age groups.
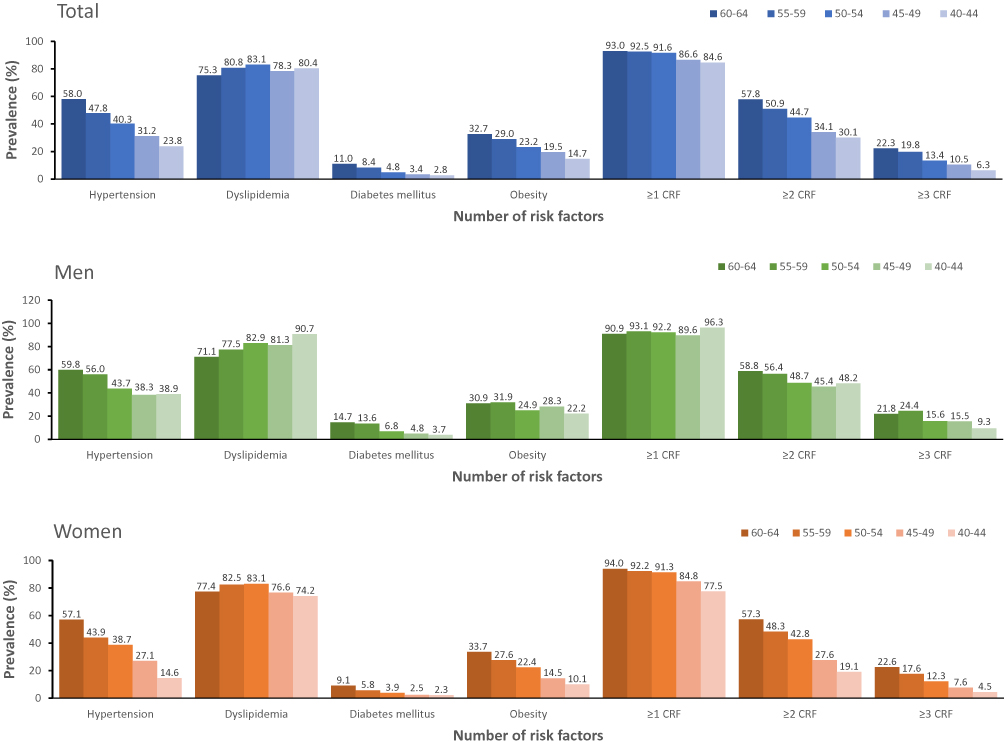 |
Figure 2 Prevalence of single and clustered CRFs by age groups in total and sex-specific groups. |
Based on the unadjusted and adjusted Poisson regression models the incident rate of CRFs was strongly related to age (Figure 3 and Table S2). With the exception of dyslipidemia and ≥1 CRF, younger persons had significantly lower IRRs for developing single and clustered risk factors. The strongest associations of age and CVDs risk factors were observed with regard to diabetes mellitus, hypertension, and ≥3 CRFs. The incident rate for dyslipidemia increased in the younger age groups (excluding the 45–49 years age group), but the differences between the oldest and the youngest groups were not deemed significant. The sensitivity analysis (Table S3) did not deviate considerably from the primary results. Although the IRRs values were generally lower, they never differed more than 0.05 from the main models.
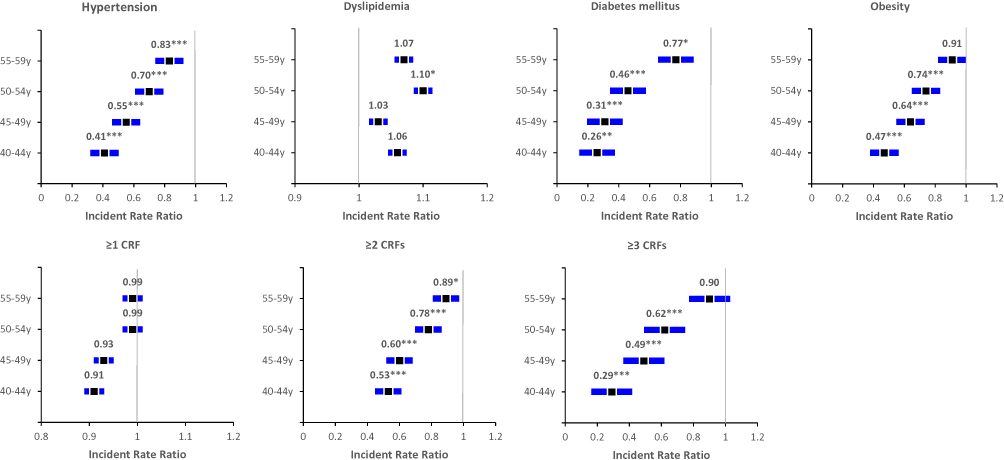 |
Figure 3 Adjusted IRRs (95% CIs) of CVD risk factors vs non CVD risk factors associated with age groups. Note: For visible presentation of confidence intervals, the beginning of the x-axis for dyslipidemia and ≥1 CRFs starts from 0.9 and 0.8 values, respectively. Gender; smoking status categorised as non-smoker (never smoker and former smoker) or smoker (current smoker); drinking status categorised as (never drinker and former drinker) or drinker (current drinker); moderate to vigorous physical activity at leisure categorised as yes or no. *P < 0.05; **P < 0.01; ***P < 0.001 vs 60–64 years age group. |
Discussion
Prevalence of major CRFs and their association with the subjects’ age was assessed. It was established in 90% of the respondents. Apart from dyslipidemia and ≥1 CRFs, prevalence of the risk factors under study increased with age, although slight deviations from the above-referenced pattern were observed in men. Prevalence of the single and clustered CRFs was less differentiated in the respective age groups, whereas in the case of the youngest and middle-aged males it proved similar. Prevalence of dyslipidemia and ≥1 CRF in the total study group, as well as in women, was unrelated to age, whereas in men it was on the rise in the younger age groups. The incident rate of CRFs was strongly associated with age, and, with the exception of dyslipidemia and ≥1 CRF, were higher in the older age groups.
CVDs are multifactorial by nature. The main modifiable CRFs are hypertension, dyslipidemia, diabetes mellitus, and obesity, although the age factor is deemed by far the strongest of them all.20 Similar results were reported in the WOBASZ study.21 All currently available prediction scores for individual risk assessment of CVDs make due allowances for age in their calculation formula. Even though metabolic and vascular disorders are age-related, there is no consensus on whether the age itself is a risk factor, or merely a measure of the intensity and duration of exposure to other CRFs.22 The importance of age as a measure of exposure to other risk factors is corroborated by potential benefits of controlling the existing CRFs, with a view to reducing overall of fatal and non-fatal CVDs events. This particular effect is also observed in seniors.
Prevalence of major CRFs and their modification are generally similar in their significance in persons of different ages, but in seniors, the risk of CVDs and the attendant benefits of prevention are slightly different than in the younger people.23 In a general population, reducing SBP by 20 mm/Hg halves the risk of cardiovascular disorders, whereas in seniors this risk drops by approx. 30%. Furthermore, overall risk of fatal and non-fatal CVDs in seniors is associated both with high and low blood pressure.24 The association of high LDL-C level with CVDs risk in seniors is not as strong as in the younger people, but very much like in the case of blood pressure, high and low TC levels are strongly associated with CDs risk.25,26 Diabetes mellitus increases the risk of CVDs, although this association is not age-dependent.27
The assumption that the effect of age on CVDs risk is modifiable was supported by several studies.22,28–31 It should be borne in mind, though, that potential for increasing life expectancy is associated with an increased control, or even with an altogether elimination of modifiable CRFs in persons of all ages, especially in the young ones. This is owed to the fact that while the relative risk of CVDs is rather constant throughout an individual lifespan, the absolute risk increases with age.22 Consequently, younger persons with specific CRFs are going to have a lower absolute risk of CVDs than the older ones, even though this risk is bound to increase with age.22,32
Appreciating the interrelationship between age and classical risk factors in CVDs enhances overall benefits of prevention.28 Long-term risk assessment of CVDs is particularly valuable for the young persons, as a low, short-term risk may not have them motivated sufficiently to alter their health-promoting behavioural paradigm.33 Assessment of global risk throughout an individual lifespan is therefore essential, as an extended exposure to an uncontrollable, single risk factor may result in a high risk of CVDs, or death.34 Consequently, preventive action should be taken as early as possible, before adverse health consequences associated with an occurrence of even a single CRF can occur.35 Owing to the causal link between CRFs, adequate dietary habits, and physical activity at an early age, are acknowledged to reduce the risk of obesity, hypertension, diabetes mellitus, as well as the clustering of these factors in older age.36,37
In our study, the distribution of CRFs was presented, aided by the example of a cohort undergoing systemic changes in the former Eastern Bloc countries in the 1990s. The cohort under study reflects a specific health behavioural paradigm (or lack of it, as the case might be), characteristic of both the post-communist, and EU countries. On the one hand, a drop in CVDs mortality in Poland after 1990 bears witness to a positive effect induced by the above-referenced systemic transformations, while on the other, high prevalence of some CRFs is probably owed partly to the traditional health behavioural paradigm, and partly to the negative impact of the said political transformation. We subscribe to the view that evaluation of overall effectiveness in the struggle against CVDs targeted exclusively on the reduction of mortality only is structurally flawed. The rise in the incidence of CVDs is mainly due to the rise in DALYs, and an appreciable burdening of the state resources resulting from the requirement to finance modern invasive cardiology techniques. In accordance with currently available epidemiological data for Poland, the number of patients is 40% higher than in the countries benefiting from much higher statutory expenditure in the health-care sector.
Admittedly, the present study is not free from a burden of certain limitations, though. Firstly, its cross-sectional nature did not provide for establishing the causal associations between the distribution and grouping of CRFs, and the incidence of CVDs. Secondly, behavioural CRFs (cigarette smoking, alcohol consumption, physical activity) were excluded from the analysis, as they indicate a causal association with the CRFs under study, while their presence, especially in the case of physical activity, might ostensibly have increased the prevalence of grouped CRFs. Thirdly, relative paucity of the participants from the 40–44 age group could affect the outcomes bias.
Conclusion
Cardiovascular risk factors are common in the adult population and their prevalence and clustering are generally higher in seniors. The age-induced effect is more significant in women than in men, especially in CRFs clustering. Apart from dyslipidemia, the risk of CRFs is also strongly age-related and higher in seniors. Considering potential significance of age as a measure of the intensity and duration of exposure to the risk factors, testing for the presence of CRFs, and interventions aimed at their modification should be initiated at an early age. The differences in the burden of cardiovascular risk factors depending on age hold a certain utilitarian potential which might well be tapped in mapping out public health-care policies in the countries where demographic changes indicate a dynamic aging of their populations.
Ethical Approval
The PONS study was approved by the ethics committee within the Cancer Center and by the Institute of Oncology in Warsaw, Poland. The present study was duly approved by a local Ethics Review Committee, Faculty of Health Sciences (Approval Ref. No. 25/2015), The Jan Kochanowski University (JKU) in Kielce, Poland.
Acknowledgments
The authors are most grateful to all participants for their committed involvement in the study protocol, despite numerous inconveniences.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
2. WHO. Cardiovascular Diseases (Cvds). WHO. Available from: http://www.who.int/cardiovascular_diseases/en/.
3. Gersh BJ, Sliwa K, Mayosi BM, Yusuf S. Novel therapeutic concepts * The epidemic of cardiovascular disease in the developing world: global implications. Eur Heart J. 2010;31(6):642–648. doi:10.1093/eurheartj/ehq030
4. Doryńska A, Polak M, Kozela M. Cardiovascular disease risk factors in Kraków and in the whole Poland adult population results from the WOBASZ study and Polish arm of the HAPIEE project. Epidemiol Rev. 2015;69:175–180.
5. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet Lond Engl. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
6. O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112–123. doi:10.1016/S0140-6736(10)60834-3
7. Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–1847. doi:10.1161/01.CIR.97.18.1837
8. Tao M, Pi X, Ma X, et al. Relationship between serum uric acid and clustering of cardiovascular disease risk factors and renal disorders among Shanghai population: a multicentre and cross-sectional study. BMJ Open. 2019;9(3):e025453. doi:10.1136/bmjopen-2018-025453
9. Grundy SM, Pasternak R, Greenland P, Smith S, Fuster V. Assessment of cardiovascular risk by use of multiple-risk-factor assessment equations. J Am Coll Cardiol. 1999;34(4):1348–1359. doi:10.1016/S0735-1097(99)00387-3
10. Kong X-L, Ma X-J, Zhang C-Y, Xu D-M. Clustering of major cardiovascular risk factors is associated with arterial stiffness in adults. Chronic Dis Transl Med. 2018;4(4):254–259. doi:10.1016/j.cdtm.2018.02.005
11. Wu J, Cheng X, Qiu L, et al. Prevalence and clustering of major cardiovascular risk factors in China. Medicine (Baltimore). 2016;95(10). doi:10.1097/MD.0000000000002712
12. Hong X, Ye Q, He J, et al. Prevalence and clustering of cardiovascular risk factors: a cross-sectional survey among Nanjing adults in China. BMJ Open. 2018;8(6). doi:10.1136/bmjopen-2017-020530
13. Gao B, Zhang L, Wang H. Clustering of major cardiovascular risk factors and the association with unhealthy lifestyles in the Chinese adult population. PLoS One. 2013;8:6. doi:10.1371/journal.pone.0066780
14. Birch J, Petty R, Hooper L, Bauld L, Rosenberg G, Vohra J. Clustering of behavioural risk factors for health in UK adults in 2016: a cross-sectional survey. J Public Health. 2018. doi:10.1093/pubmed/fdy144
15. Yu J, Ma Y, Yang S, et al. Risk factors for cardiovascular disease and their clustering among adults in Jilin (China). Int J Environ Res Public Health. 2016;13(1). doi:10.3390/ijerph13010070
16. Tadayon S, Wickramasinghe K, Townsend N. Examining trends in cardiovascular disease mortality across Europe: how does the introduction of a new European Standard Population affect the description of the relative burden of cardiovascular disease? Popul Health Metr. 2019;17. doi:10.1186/s12963-019-0187-7
17. Lloyd-Sherlock P, Ebrahim S, Martinez R, McKee M, Ordunez P. Reducing the cardiovascular disease burden for people of all ages in the Americas region: analysis of mortality data, 2000–15. Lancet Glob Health. 2019;7(5):e604–e612. doi:10.1016/S2214-109X(19)30069-5
18. Costantino S, Paneni F, Cosentino F. Ageing, metabolism and cardiovascular disease. J Physiol. 2016;594(8):2061–2073. doi:10.1113/JP270538
19. Akgöz A, Gözüm S. Cardiovascular disease risk in Turkish family health centers. J Vasc Nurs off Publ Soc Peripher Vasc Nurs. 2019;37(2):117–124. doi:10.1016/j.jvn.2019.02.002
20. Yusuf S, Hawken S, Ôunpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:16.
21. Piotrowski W, Waśkiewicz A, Cicha-Mikołajczyk A. Global cardiovascular mortality risk in the adult Polish population: prospective assessment of the cohorts studied in multicentre national WOBASZ and WOBASZ Senior studies. Kardiol Pol. 2016;74(3):262–273. doi:10.5603/KP.a2015.0175
22. Dhingra R, Vasan RS. Age as a cardiovascular risk factor. Med Clin North Am. 2012;96(1):87–91. doi:10.1016/j.mcna.2011.11.003
23. Tuomilehto J. Impact of age on cardiovascular risk: implications for cardiovascular disease management. Atheroscler Suppl. 2004;5(2):9–17. doi:10.1016/j.atherosclerosissup.2004.03.006
24. Lewington S, Clarke R, Qizilbash N. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi:10.1016/S0140-6736(02)11911-8
25. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360(9346):1623–1630. doi:10.1016/S0140-6736(02)11600-X
26. Casiglia E, Mazza A, Tikhonoff V, Scarpa R, Schiavon L, Pessina AC. Total cholesterol and mortality in the elderly. J Intern Med. 2003;254(4):353–362. doi:10.1046/j.1365-2796.2003.01200.x
27. Yakaryılmaz FD, Öztürk ZA. Treatment of type 2 diabetes mellitus in the elderly. World J Diabetes. 2017;8(6):278–285. doi:10.4239/wjd.v8.i6.278
28. Sniderman AD, Furberg CD. Age as a modifiable risk factor for cardiovascular disease. Lancet. 2008;371(9623):1547–1549. doi:10.1016/S0140-6736(08)60313-X
29. Lloyd-Jones DM, Leip EP, Larson MG, et al. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation. 2006;113(6):791–798. doi:10.1161/CIRCULATIONAHA.105.548206
30. Terry DF, Pencina MJ, Vasan RS, et al. Cardiovascular risk factors predictive for survival and morbidity-free survival in the oldest-old Framingham Heart Study participants. J Am Geriatr Soc. 2005;53(11):1944–1950. doi:10.1111/j.1532-5415.2005.00465.x
31. Ungar A, Galizia G, Morrione A, et al. Two-year morbidity and mortality in elderly patients with syncope. Age Ageing. 2011;40(6):696–702. doi:10.1093/ageing/afr109
32. Cochrane T, Davey R, Gidlow C, et al. Contribution of individual risk factor changes to reductions in population absolute cardiovascular risk. Biomed Res Int. 2014;2014:1–6. doi:10.1155/2014/626205
33. Quispe R, Bazo‐Alvarez JC, Burroughs Peña MS, et al. Distribution of short‐term and lifetime predicted risks of cardiovascular diseases in peruvian adults. J Am Heart Assoc. 2015;4(8). doi:10.1161/JAHA.115.002112
34. Loria CM, Liu K, Lewis CE, et al. Early adult risk factor levels and subsequent coronary artery calcification. J Am Coll Cardiol. 2007;49(20):2013–2020. doi:10.1016/j.jacc.2007.03.009
35. Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18(3):109. doi:10.4103/HEARTVIEWS.HEARTVIEWS_106_17
36. Berry JD, Dyer A, Cai X, et al. Lifetime risks of cardiovascular disease. N Engl J Med. 2012;366(4):321–329. doi:10.1056/NEJMoa1012848
37. Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the american heart association’s strategic impact goal through 2020 and beyond. Circulation. 2010;121(4):586–613. doi:10.1161/CIRCULATIONAHA.109.192703
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.