")
Back to Journals » Drug Design, Development and Therapy » Volume 9
A prospective treatment for sepsis
Authors Shahidi Bonjar MR, Shahidi Bonjar L
Received 12 February 2015
Accepted for publication 16 March 2015
Published 6 May 2015 Volume 2015:9 Pages 2537—2543
DOI https://doi.org/10.2147/DDDT.S82755
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Shu-Feng Zhou
Mohammad Rashid Shahidi Bonjar,1 Leyla Shahidi Bonjar2
1School of Dentistry, 2College of Pharmacy, Kerman University of Medical Sciences, Kerman, Iran
Abstract: The present paper proposes a prospective auxiliary treatment for sepsis. There exists no record in the published media on the subject. As an auxiliary therapy, efficacious extracorporeal removal of sepsis-causing bacterial antigens and their toxins (BATs) from the blood of septic patients is discussed. The principal component to this approach is a bacterial polyvalent antibody-column (BPVAC), which selectively traps wide spectrum of BATs from blood in an extracorporeal circuit, and detoxified blood returns back to the patient’s body. BPVAC treatment would be a device of targeted medicine. Detoxification is performed under supervision of trained personnel using simple blood-circulating machines in which blood circulates from the patient to BPVAC and back to the patient aseptically. BPVACs’ reactive sites consist of carbon nanotubes on which a vast spectra of polyvalent BATs-antibodies are bond to. The devise acts as a biological filter that selectively immobilizes harmful BATs from intoxicated blood; however, no dialysis is involved. For effective neutralization, BPVAC provides large contact surface area with blood. BPVAC approach would have advantages of: 1) urgent neutralization of notorious BATs from blood of septic patients; 2) applicability in parallel with conventional treatments; 3) potential to minimize side effects of the malady; 4) applicability for a vast range of BATs; 5) potential to eliminate contact of BATs with internal tissues and organs; 6) tolerability by patients sensitive to antiserum injections; 7) capability for universal application; 8) affectivity when antibiotic-resistant bacteria are involved and the physician has no or limited access to appropriate antibiotics; and 10) being a single-use, disposable, and stand-alone device. Before using it for clinical trials in human beings, it should pass animal evaluations accurately; however, research works should optimize its implementation in human beings. For optimization, it needs appropriate investments, collaboration of scientists in many fields of research, and development through several interdisciplinary sciences such as medical engineering, nanotechnology, immunology, biochemistry, emergency medicine, internal, and infectious diseases.
Keywords: antibiotic, blood, infection, targeted medicine, detoxification, polyvalent antibody
Introduction
Severe sepsis and septic shock are the biggest causes of mortality in critically ill patients.1,2 For every three heartbeats, someone dies of sepsis. In the developing world, sepsis accounts for 60%–80% of childhood deaths. Those who survive, both adults and children, often struggle with life.3 Sepsis ranks in the top 10 causes of death.4 It encompasses a spectrum of illness that ranges from minor signs and symptoms to organ dysfunction and shock.5–8 According to the University of Maryland Medical Center, the sepsis mortality rate is higher than 50% in some cases.9
Sepsis is a serious life-threatening bacterial infection of blood. It happens when bloodstream is infected with bacteria. It can result from something as seemingly harmless as a scraped elbow or from a more serious medical problem such as appendicitis, pneumonia, meningitis, or a urinary tract infection.10 In hospitalized patients, common sites of initial infection include intravenous (IV) lines, surgical incisions, urinary catheters, and bed sores.10,11 Anomalies in the pathways of immune, inflammation, coagulation, oxygen delivery, and utilization play a role in organ dysfunction and death. If not treated, it is a serious convolution, an infection characterized by complication throughout the body. It may progress and get severely worse very quickly. Systemic inflammatory response syndrome is called sepsis if accompanied by any confirmed source of infection.12,13 It occurs in 1%–2% of all hospitalizations in the US, and it affects at least 750,000 people each year.10 Sepsis can cause blood clots and block oxygen from reaching vital organs, resulting in organ failure.12,14 In many instances, it arises from infections throughout the body, including infections in the lungs, abdomen, and urinary tract. It may come before or at the same time as infections of the bone (osteomyelitis), central nervous system (meningitis), heart (endocarditis), and other tissues.14 Symptoms of septicemia can begin with chills, high fever, rapid breathing, and rapid heart rate in which the person looks very ill or even experiences a coma. The symptoms quickly progress to confusion or other changes in mental status, red spots on the skin (petechia and ecchymosis), adult respiratory distress syndrome, adrenal collapse (Waterhouse–Friderichsen syndrome), multiple organ dysfunction syndrome, and serious drop in blood pressure.15,16 Death rate of septic shock is more than 50% for some infections.3 Sepsis prognosis depends on the bacteria involved and how quickly the patient is hospitalized and treated.17
Conventional treatments for sepses
Sepsis is a medical emergency that requires hospitalization of the patient admitted to an intensive care unit (ICU). Early identification of septic patients allows for evidence-based interventions. Several tests that can confirm sepsis include blood culture, blood gases, CBC, clotting studies (PT, PTT, and fibrinogen levels), CSF culture, culture of skin sore, platelet count, and urine culture.5,6,14
In 2013, Dellinger et al18 issued the iteration of clinical guidelines for the management of severe sepsis and septic shock. Common treatments include antibiotics to treat the infection, fluids and medicines by IV to maintain the blood pressure and stabilize blood circulation, and oxygen and plasma or other blood products to correct any clotting problems. In antibiotic therapies, patients’ survival depends to a large extent on receiving successful treatment for the infection that led to sepsis, including broad-range antibiotics.3,19 Furthermore, death in the clinical setting often occurs despite the use of antibiotics, resuscitation, and intensive life support.19,20
Plasmapheresis or plasma filtration21,22 has also been evaluated in sepsis, however, having controversial results. Busund et al tried to determine the therapeutic efficacy and safety of plasmapheresis in the treatment of patients with severe sepsis and septic shock.23 In their evaluation, 106 patients were randomized and received either standard therapy or an add-on treatment with plasmapheresis. They observed that at the end of day 28, all-cause mortality rate was 33.3% (18/54) in the plasmapheresis group and 53.8% (28/52) in the control group; they concluded that risk reduction was 20.5% in the treated group. In a similar study, Long et al used plasmapheresis to determine whether plasma filtration improves 28-day survival in infants and children with severe sepsis.24 They observed that ten (40%) children died in the plasma filtration group and four (17%) died in the control group. Such controversial results indicate that further research is needed if plasmapheresis is to be used in sepses treatment.
Difficulties in conventional treatments of sepses
In patient with sepsis, it is clear that the faster the diagnosis and treatment, the better the prognosis. There exist several difficulties and consequences in conventional therapies as: 1) time is crucial in resuscitation of septic patients; in delayed treatments, patients may experience permanent organ failure; for example, in lung infection (pneumonia) with sepsis, patients may need respiratory support or septic shock related to a limb infection patient may end up to limb amputation;25 2) in improper antibiotic therapies, each patient is likely to have the potential for complications related to invasion of bacterial antigens and their toxins (BATs) to internal organs, which may lead to organ dysfunction, damage, or death; however, death is usually due to multiorgan dysfunction (liver, kidney, or lung failure);17,26,27 3) patients are with overwhelmed immune response to infection;28 4) there exist complications in patients who are at greater risk for infection such as people with diabetes,29 cancer, suppressed immune systems, and elderly patients;14,30 and 5) there is spread of antibiotic resistance and the appearance of multiple antibiotic-resistant pathogenic bacteria, such as MRSA, which is an increasingly prevalent problem that complicates the care of many patients.30,31 However, several more can be added to the above.
Proposed prospective treatment
The proposed auxiliary therapy is based on the application of bacterial polyvalent antibody-column (BPVAC) for neutralization of wide spectra of blood BATs known as causal agents of prevalent types of bacterial sepses. As indicated in Figure 1, in the course of resuscitation of septic patients, BPVAC behaves as the key unit. It would trap bacteria and remove their toxins from the blood out of the body. BPVACs perform as out of body detoxification for trapping of BATs from septic blood and check them from returning back to the patient’s body.
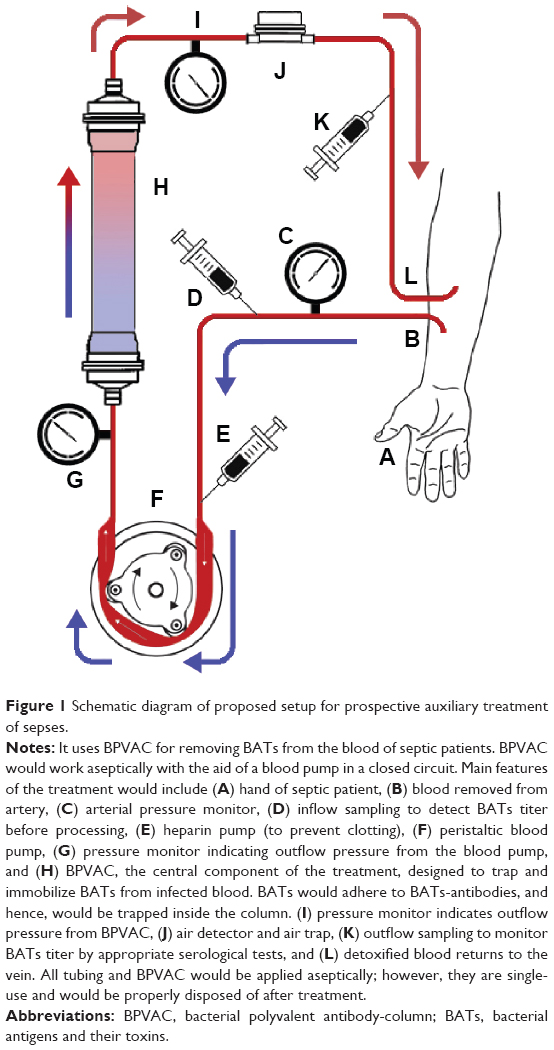 | Figure 1 Schematic diagram of proposed setup for prospective auxiliary treatment of sepses. |
In this treatment, the blood of a septic patient is processed while passing through the trapping device, BPVAC. The procedure set in BPVAC approach is similar to that in devices designed and reported by Shahidi Bonjar32–35 or in renal dialysis machine36 used for patients with renal failure; however, instead of dialysis membrane, the machine is equipped with BPVAC. BPVAC involves no dialysis. BPVACs have vast internal surface areas for direct contact with blood to trap and immobilize BATs. BATs-polyvalent-antibodies would adhere on contact surfaces of the reaction platforms inside the column. BATs-polyvalent-antibodies would be specifically manufactured against BATs of prevalent sepses.
Passage of blood through BPVAC immobilizes BATs on stationary BPVAs. Similar to renal dialysis machine, blood circulates from the patient to BPVAC and from there back to the patient in a closed circuit till BATs are depleted enough from the blood. The BATs level in blood returning to the body would be monitored by appropriate serological tests. Use of BPVAC as an auxiliary therapy along with conventional treatments would improve the therapy outcome since: 1) BPVAC diminishes BATs in blood and minimizes the duration of their contact with internal vital organs and 2) when BPVAC is used, the major titer of BATs in blood would be depleted rapidly, and hence, the efficacy of conventional treatments, especially antibiotic therapies, would enhance. Such a dual therapy may decrease sepsis side effects. Considering that time is a key factor in resuscitation of intoxicated patient, BPVAC may act as a lifesaving device in infectious blood diseases when the physician has limited choice of antibiotic therapy due to microbial resistance and/or lack of appropriate antibiotics.
When sufficient research in animal evaluations proved positive, BPVAC would be evaluated in human cases under meticulous supervision of appropriate specialists. BPVAC may serve as an emergency resuscitation device in emergency ambulances to treat septic shock patient in situ, and it may also be implemented in ICUs of hospitals. The period needed for BPVAC treatment depends on BATs’ titers in blood before it returns back to the body; however, optimization studies should set the procedure details. BPVAC is a single-use and stand-alone device that would be appropriately disposed of after each detoxification therapy.
Proposed structural specifications of BPVAC
BPVACs would be manufactured as single-use, disposable, and stand-alone devices. They would be biotechnologically engineered for BATs involved in prevalent sepses. As a polyvalent column, BPVAC harbors wide spectra and sufficient amounts of BATs-antibodies to trap BATs internally. As indicated in Figure 2, a BPVAC would be aseptically manufactured to have the following main features. It has an inlet and an outlet for blood and a column cylinder that confines a stack of thousands of monovalent antibody plates (MAPs) around its center axis. Each MAP consists of an extensive lattice of biocompatible organic polymers. MAPs harbor millions of nano carbon-rods on their entire surfaces. Nano carbon-rods, which act as antibody-BATs reaction platforms, are coated with monovalent antibodies via supportive intermediate moieties. Stacking of BPVACs with MAPs takes place in the manufacturing factory. Each type of MAP harbors one specific kind of antibody that has been immunologically prepared against one specific kind of antigen present in BATs. Types and number of each of various MAPs to stack in the column depend upon factors determined through immunological investigations. While column is in action, each nocent antigen coagulates with its specific antibody on the relevant MAPs and would be immobilized and trapped from blood thereafter.
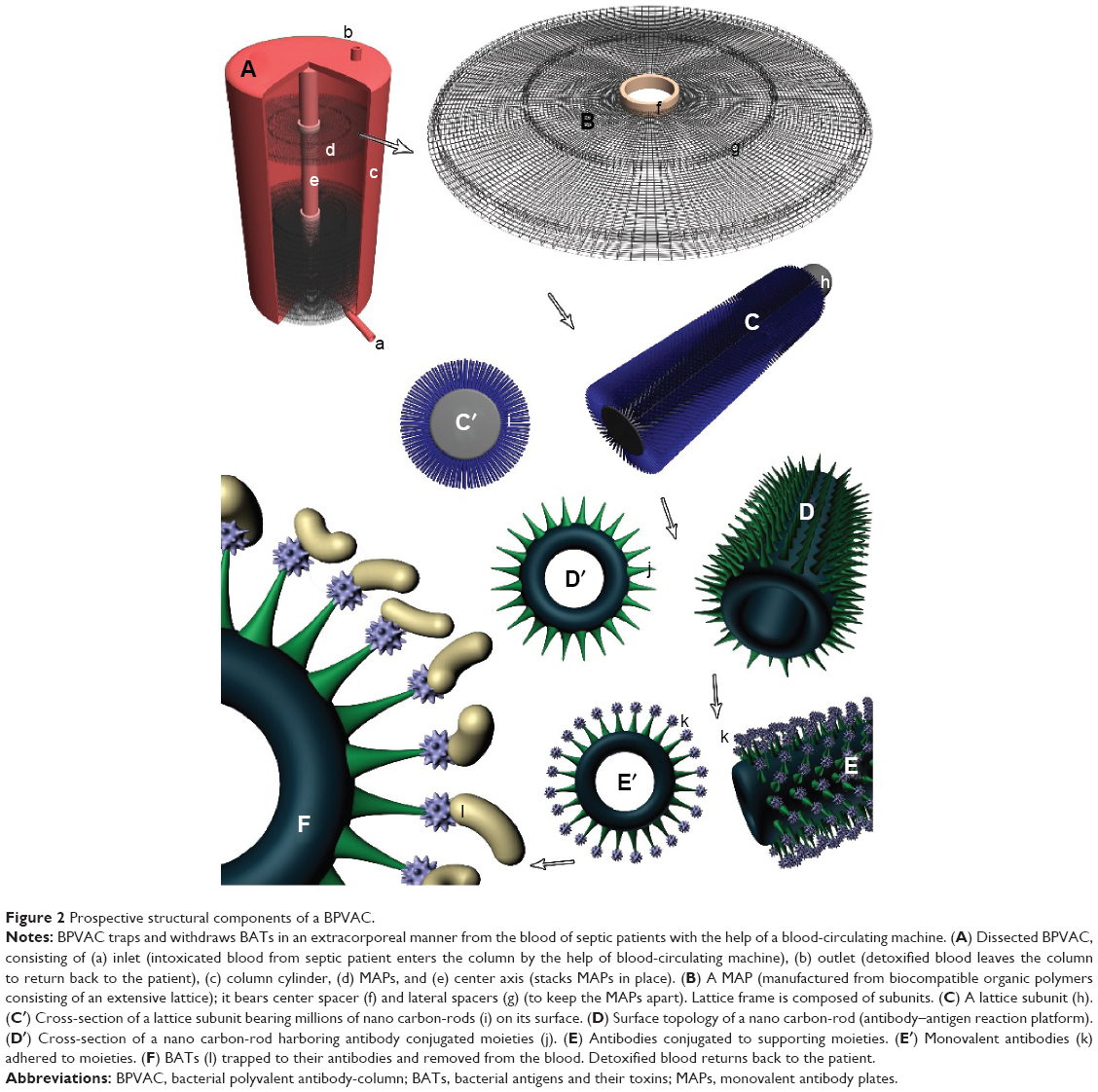 | Figure 2 Prospective structural components of a BPVAC. |
BPVAC approximations in action
Each MAP is engineered for a specific antigen it has to trap. The number of MAPs per each BPVAC depends on the maximum titer of relevant antigens to trap; however, such information would be provided through appropriate toxicological and immunological investigations. Just as an approximation, the number of specific MAPs per each BPVAC may exceed hundreds and the total number of all MAPs per each BPVAC may exceed several thousands. Assuming 50 μm thickness (including spacers) and 5 cm diameter for each MAP, and 10,000 MAPs per BPVAC, the maximum height and volume of the column would be about 50 cm and 400 cm3, respectively. With such approximations, the column may have an internal volume to hold 500 mL of blood. The volume of involved connection silicone-tubes may not exceed 100 mL. Thence, for an average-sized septic adult, the total volume of blood being processed at a given point of time would be about 600 mL. The flow rate may be 300–500 mL/min in which about 18–30 L of blood would pass through BPVAC/h. Considering a duration of 3 hours per treatment, approximate volume of blood passing through BPVAC would be ~54–90 L. Under such circumstances, if circulating machine and BPVAC perform as defined, there exists a high chance of convenient extracorporeal detoxification of the majority of the BATs; however, the settings would be adjusted according to the optimization studies.
Clinical significance
Effective removal of BATs from the blood of patients with sepsis may be a lifesaving therapy. Any delay or failure in such a vital treatment may make the patient disabled or lead to death. The major clinical significances of BPVAC, which may justify its application as an auxiliary therapy, are: 1) its capability for parallel application along with conventional treatments; 2) it may minimize sepsis side effects; 3) the procedure may be administrable for a vast range of BATs; 4) it may minimize the period of contact of notorious antigens with internal tissues and organs; 5) it may be well tolerated by patients sensitive to antiserum injections; 6) it may have a high chance of effectiveness because there is no need to identify the BATs prior to administration, since it would be designed to contain almost all antibodies for almost all sepses-known antigens; 7) it would be a disposable stand-alone device, which would be biotechnologically engineered for prevalent BATs involved in known sepses maladies; 8) it is expected that BPVAC in dual therapy may shorten recovery periods (In other words, in conventional therapies, BATs remain internal even when deactivated by antibiotics, while in BPVAC therapy, they are immobilized out of the patients body.); 9) it may lower the chance of many amputations and permanent disabilities, which are the result of delayed detoxification; 10) while optimized, it would be a ready-to-use device; in other words, no preliminary preparation is needed for its immediate implementation and while needed; 11) it would have the potential to become an emergency medical device for emergency ambulances and emergency care units in hospitals; 12) since aseptically made for a single-use, it reduces the chance of further infections; and 13) removal of the major content of toxic antigens from blood in a relatively short period of time may make it indispensable in sepses therapy. While optimized, BPVAC detoxification treatment may attain capability for universal application in remediation of septic patients. The authors believe that BPVAC approach holds great promise to reduce the time, effort, and expense in sepses research and therapy. They also believe that it would save more septic lives than conventional remedies do.
Disadvantages and probable side effects
While BPVAC treatment can be efficient at removal of sepsis-causing BATs from blood, patients may suffer from some side effects. Although not every septic patient may confront diverse side effects, treatment team can help the patients to avoid some of the discomforts. Similar to kidney dialysis,37–39 the side effects are usually contributed to the amount and speed of blood removal. In this regard, BPVAC patients may face with two major side effects and their consequences. These side effects include a) hypotension: drop in blood pressure may go along with abdominal cramps, muscle cramps, shortness of breath, or vomiting; such symptoms can be eased by adjusting the treatment prescription and b) new infections: aseptic management of the treatment and proper care should be taken to prevent such further complications.
Period of treatment
In BPVAC procedure, the treatment duration depends on the concentration of BATs in blood. The blood leaving the column should be sampled and examined for titer of BATs by the use of serological tests. The treatment duration will last till the patient’s overall health is improved or set by the physician; however, standardization procedures should be developed through appropriate investigations.
Optimization protocol
Appropriate research works would be needed to gain optimized performance from the application of BPVAC procedure along with conventional treatments such as antibiotic therapies. Before human application, optimized protocols should be revealed in animal investigations. The optimization studies in animals would pave the path for optimization in human cases. At present, any prediction about an optimized protocol may have no validity for real treatments.
Sanitation concerns
BPVAC setup would be single-use. All the components in contact with the blood, including the column, vein sets, and silicone connection-tubes, are to be single-use and would be properly disposed of after each treatment. However, the ready-to-use BPVAC pack would be presterilized by gamma or electron-beam radiation during manufacturing process.
Further prospective
Application of PVAC holds promise to effectively improve patients whose health is threatened by the invasion of deleterious agents in their blood. PVAC methodology may serve similarly in other blood maladies in which prompt removal of detoxification of systemic antigens and notorious molecules (as in poison intoxication) has high priority. Such columns would have stationary antibodies or trapping molecules for removal of the target agents. Application of PVAC as an auxiliary treatment along with conventional therapies may lead to enhanced improvement of patients’ health; however, in such a concomitant therapy, conventional treatments may work more efficiently.
Evaluation of the hypothesis
It is clear that before implementation of BPVAC in human beings, it should be evaluated in animals; however, research works would pave the route of its use in human beings. Animal experiments under appropriate ethical obedience should mimic human sepses cases to the best possible. For clear deductions, statistical evaluations would have five treatments, including: 1) healthy, untreated; 2) septic, treated with conventional therapies; 3) septic, treated with BPVAC alone; 4) septic, treated with dual therapy (conventional plus BPVAC); and 5) septic, untreated. Treated animals should go through lifetime for investigating side effects on internal vital organs such as liver, muscles, spleen, kidneys, lungs, heart, and brain. Special attention should be placed on investigating nephrotoxicity (kidney), hepatotoxicity (liver), and hematological toxicity (blood) responses. The effectiveness of BPVAC in animal investigations would then allow the use of BPVAC on volunteer human beings. When proved effective, BPVAC could be used as a procedure to assist many septic patients. It is anticipated that since BPVAC encompasses the widest spectrum of sepses antibodies, it may act as a suitable choice for physicians in treating sepses.
Conclusion
Bacterial sepsis is a serious medical emergency, and delays in treatment can become life threatening. The authors believe that if meticulous investigation of BPVAC proves positive, application of BPVAC will reduce human casualties due to septic shocks. BPVAC may become an important adjuvant to conventional treatment for reducing mortality in such patients. It may set a new therapeutic protocol in treating similar systemic diseases. BPVAC in combination therapy may improve therapeutic efficacies of conventional therapies and so the well-being of treated patients. BPVAC would shorten recovery periods since it selectively traps notorious antigens from patient’s blood in a short period of time as low as 2–3 hours. BPVAC may justify its presence as a necessary device in emergency and ICUs in hospitals. BPVAC is anticipated to reduce time, effort, and expense in blood detoxification therapies. The authors believe that controlled application of BPVAC prevents many human casualties, which conventional methods alone may not.
BPVAC approach is different from plasmapheresis (removal of blood plasma, including antibodies and proteins). As described, BPVAC selectively removes sepses antigens and toxins for which it has been manufactured; it has no interference with normal blood-proteins and antibodies.
To minimize probable side effects of BPVAC approach, appropriate treatment prescription, aseptic management of the treatment, and proper care should be taken to check further complications. Before human application, optimized protocols should be deduced from animal investigations. In the process of manufacturing the BPVAC pack, it would be sterilized by the use of gamma or electron-beam radiation. With the hope to lower human casualties and serve sepsis patients, BPVAC pack may be considered a lifesaving device in emergency ambulances, departments of infectious diseases, and ICUs of hospitals.
The authors hope that BPVAC will set smile to the face of remediated patients and physicians and personnel who thrive to bring health back to their patients.
Dedication
We dedicate this paper to patients who would be resuscitated with BPVAC and get back to their families and healthy normal lives, and also, we dedicate it to the physicians and scientists whose attempts bring this desire to reality.
Disclosure
The authors declare that they have no financial and personal relationships with other people or organizations that can inappropriately influence their work. There is no professional or other personal interest of any nature or kind in any product, service, and/or company that could be construed as influencing the position presented in this article.
References
Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41(5):1167–1174. | ||
Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA. 2014;311(13): 1308–1316. | ||
World-sepsis-day.org. World sepsis declaration. Available from: http://www.world-sepsis-day.org/?MET=SHOWCONTAINER&vCONTAINERID=489. Accessed October 1, 2014; 2015. | ||
U.S. National Library of Medicine. Acute respiratory distress syndrome. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001164/. Accessed October 1, 2014; 2015. | ||
Johns Hopkins Medicine, Health Library. Septicemia. Available from: http://www.hopkinsmedicine.org/healthlibrary/conditions/adult/nervous_system_disorders/septicemia_85,P00802/. Accessed October 1, 2014. | ||
Healthline.com. Septicemia. Available from: http://www.healthline.com/health/septicemia#Overview. Accessed October 1, 2014. | ||
U.S. National Library of Medicine. Septic shock. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001689/. Accessed October 1, 2014. | ||
Bone R, Balk R, Cerra F, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992; 101(6):1644–1655. | ||
University of Maryland Medical Center. Septicemia. Available from: http://umm.edu/health/medical/ency/articles/septicemia. Accessed October 1, 2014. | ||
US National Library of Medicine. Septicemia. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002331/. Accessed October 1, 2014. | ||
Derek C, van der Poll A, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369(9):840–851. | ||
Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369(9):840–851. | ||
Bone RC, Fisher CJ Jr, Clemmer TP, Slotman GJ, Metz CA, Balk RA. Sepsis syndrome: a valid clinical entity. Crit Care Med. 1989;17:389–393. | ||
NIH, US National Library of Medicine. Septicemia. Bethesda, MD; 2015. Available from: http://www.nlm.nih.gov/medlineplus/ency/article/001355.htm. Accessed October 1, 2014. | ||
Matsuda N, Hattori Y. Systemic inflammatory response syndrome (SIRS): molecular pathophysiology and gene therapy. J Pharmacol Sci. 2006;101(3):189–198. | ||
Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet. 2015; 365(9453):63–78. | ||
Cunha BA. Bacterial Sepsis. Medscape.com; 2014. Available from: http://emedicine.medscape.com/article/234587-overview. Accessed October 1, 2014. | ||
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign guidelines: international guidelines for management of severe sepsis and septic shock. Crit Care Med. 2012;41(2):580–637. | ||
Rivers E, Nguyen B, Havstad S, et al; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. New Engl J Med. 2001;345(19): 1368–1377. | ||
Marshall JC. Sepsis: rethinking the approach to clinical research. J Leukocyte Biol. 2013;94(1):471–482. | ||
Plasmapheresis. Johns Hopkins Comprehensive Transplant Center. Available from: http://www.hopkinsmedicine.org/transplant/programs/kidney/incompatible/plasmapheresis.htm. Accessed October 1, 2014. | ||
Nguyen TC, Kiss JE, Goldman JR, Carcillo JA. The role of plasmapheresis in critical illness. Crit Care Clinician. 2012;28(3):453–468. | ||
Busund R, Koukline V, Utrobin U, Nedashkovsky E. Plasmapheresis in severe sepsis and septic shock: a prospective, randomized, controlled trial. Intensive Care Med. 2002;28(10):1434–1439. | ||
Long EJ, Shann F, Pearson G, Buckley D, Butt W. A randomised controlled trial of plasma filtration in severe paediatric sepsis. Crit Care Resusc. 2013;15(3):198–204. | ||
MedicineNet.com. Sepsis; what is the prognosis (outcome) with sepsis? 2015. Available from: http://www.medicinenet.com/sepsis/page7.htm#what_are_the_complications_of_sepsis. Accessed October 1, 2014. | ||
Wheeler A, Carmichael L, Christman B, et al. Renal function abnormalities in sepsis. Am J Respir Crit Care Med. 1995;151(Suppl):A317. | ||
Pastor CM, Billiar TR, Losser MR, Payen DM. Liver injury during sepsis. J Crit Care. 1995;10:183–197. | ||
Webmed.com. Information and resources; sepsis (blood infection) and septic shock. Available from: http://www.webmd.com/a-to-z-guides/sepsis-septicemia-blood-infection. Accessed October 1, 2014. | ||
Hirasawa H, Oda S, Nakamura M. Blood glucose control in patients with severe sepsis and septic shock. World J Gastroenterol. 2009; 15(33):4132–4136. | ||
Weber B, Saliken J, Jadavji T, Gray RR, Moore R. A near-fatal case of sepsis with an antibiotic-resistant organism complicating a routine transrectal prostate biopsy in a health care worker. Can Urol Assoc J. 2008;2(5):543–545. | ||
Turnidge J. Impact of antibiotic resistance on the treatment of sepsis. Scand J Infect Dis. 2003;35(9):677–682. | ||
Shahidi Bonjar L. “Nanogold detoxifying machine” to remove idle nanogold particles from blood stream of cancer patients treated with antibody-nanogold therapeutics. Med Hypotheses. 2013;80(5):601–605. | ||
Shahidi Bonjar L. Design of a new therapy to treat snake envenomation. Drug Des Dev Ther. 2014;8:820–824. | ||
Shahidi Bonjar MR, Shahidi Bonjar L. Antiaging therapy: a prospective hypothesis. Drug Des Dev Ther. 2015;9:663–667. | ||
Shahidi Bonjar MR, Shahidi Bonjar L. Design of a new therapy for patients with chronic kidney disease: use of microarrays for selective hemoadsorption of uremic wastes and toxins to improve homeostasis. Drug Des Dev Ther. 2015;9:625–629. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4307649/ | ||
DaVita HealthCare Partners Inc; Joe S. How does a dialysis machine work? Available from: http://www.davita.com/treatment-options/hemodialysis/in-center-hemodialysis/how-does-a-dialysis-machine-work?/t/5596. Accessed October 1, 2014. | ||
Mayo Clinic Staff. Risks – Tests and Procedures, Hemodialysis. Available from: http://www.mayoclinic.org/tests-procedures/hemodialysis/basics/risks/prc-20015015. Accessed March 14, 2015. | ||
National Kidney Foundation. Coping with the top five side effects of dialysis. Available from: https://www.kidney.org/news/ekidney/january12/top5. Accessed March 14, 2015. | ||
Kidney Dialysis Information Centre. Risks and side effects during kidney dialysis. Available from: http://www.kidneydialysis.org.uk/risks.htm. Accessed March 14, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.