")
Back to Journals » Drug Design, Development and Therapy » Volume 9
A meta-analysis for CXCR4 as a prognostic marker and potential drug target in non-small cell lung cancer
Authors Zhang C, Li J, Han Y, Jiang J
Received 25 January 2015
Accepted for publication 14 April 2015
Published 24 June 2015 Volume 2015:9 Pages 3267—3278
DOI https://doi.org/10.2147/DDDT.S81564
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Shu-Feng Zhou
Changyuan Zhang,1,* Jie Li,2,* Yi Han,3 Jian Jiang4
1Department of Cardiothoracic Surgery, Inner Mongolia Autonomous Region People’s Hospital, Inner Mongolia; 2Department of Oncology, 3Department of Thoracic Surgery, Beijing Chest Hospital, 4Department of Thoracic Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Background: Recent reports have shown that C-X-C chemokine receptor type 4 (CXCR4) is a candidate oncogene in several types of human tumors, including non-small cell lung cancer (NSCLC). However, the correlation between CXCR4 expression and clinicopathological characteristics of NSCLC remains controversial and has not been emphasized. The aim of this study is to quantitatively evaluate the association of CXCR4 expression with the incidence of NSCLC and clinicopathological characteristics by performing a meta-analysis.
Methods: A detailed literature search was carried out for related research publications. Only articles in which CXCR4 expression was detected by immunohistochemical staining were included. Odds ratio (OR) and hazard ratio (HR) with 95% confidence intervals (CIs) were calculated and summarized.
Results: Final analysis of 1,872 NSCLC patients from 19 eligible studies was performed. We observed that CXCR4 expression was significantly higher in NSCLC than in normal lung tissue, based on the pooled OR from ten studies, including 678 NSCLCs and 189 normal lung tissues (OR =16.66, 95% CI =6.94–40.02, P<0.00001). CXCR4 expression was also significantly associated with clinical stages, metastatic status, and overall survival (OS) in NSCLC patients. In addition, CXCR4 mRNA high expression was found to correlate with worse OS of all NSCLC patients followed for 20 years, HR =1.24, P=0.0047.
Conclusion: The present meta-analysis indicated that CXCR4 protein expression is associated with an increased risk and worse survival in NSCLC patients. The aberrant CXCR4 protein and mRNA expression play an important role in the carcinogenesis and metastasis of NSCLC.
Keywords: prognosis, meta-analysis, odds ratio, hazard ratio
Introduction
Chemokines are a group of small proteins associated with cytoskeletal rearrangements, cell migration during development and physiology, and host immune response. Chemokines can interact with G-protein-coupled receptors, which play critical roles in the immune system and in the cellular proliferation, migration, invasion, angiogenesis, evasion of the immune response, and inflammatory microenvironment of tumors.1–3 C-X-C chemokine receptor type 4 (CXCR4), also known as fusin or CD184, is an alpha-chemokine receptor specific for stromal cell-derived factor 1 (SDF-1; also called CXCL12).4,5 CXCR4 belongs to the superfamily of seven-transmembrane domain, heterotrimeric G-protein-coupled receptors and is functionally expressed on the cell surface in a wide range of malignant tumors as well as implicated in the cell proliferation and migration of these cells.6–8 Recently, CXCR4 has been reported to be overexpressed and to play an important role in cell survival, proliferation, migration, and metastasis of several cancers, including breast,9–11 ovarian,12,13 cervical,14–16 colon or rectal,17,18 esophageal,18–20 stomach,21,22 liver,23–25 gall bladder,26,27 kidney,28–30 pancreatic,31,32 prostate,33–35 and uterine,36,37 as well as multiple myeloma38,39 and non-Hodgkin lymphoma.40 A number of studies showed that CXCR4 is also overexpressed in non-small cell lung cancer (NSCLC) and may account for its progression, metastasis, and prognosis.41–45 However, controversy still exists. CXCR4 has been identified by immunohistochemistry (IHC) in both the nucleus and cytoplasm of NSCLC cells, and the cellular localization of CXCR4 has been reported to correlate with the different biological behaviors of the tumor.46 Wagner et al found that positive cytomembranous staining for CXCR4 is an independent indicator of poor prognosis, while nuclear staining confers a survival benefit to patients with adenocarcinoma of the lung.47 In addition, the roles of CXCR4 in NSCLC and clinical significance have not been thoroughly investigated. Meta-analysis has great advantages in confirming prognostic and pathological factors in cancer patients by avoiding disadvantages of small sample size. Therefore, it is necessary to perform a pooled analysis using the results of published articles. In this study, we have analyzed and updated the published clinical investigations regarding the effects of CXCR4 on patients with NSCLC.
Material and methods
Search strategy and selection criteria
The following electronic databases were searched for relevant articles without any language restrictions: Web of Science (1945–2014), the Cochrane Library database (Issue 12, 2014), PubMed (1966–2014), Excerpta Medica dataBASE (EMBASE) (1980–2014), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (1982–2014), and the Chinese Biomedical Database (CBM) (1982–2014).
We searched articles using following terms: “lung,” “cancer or tumor or neoplasm or carcinoma,” “expression,” “CXCR4 or C-X-C chemokine receptor type 4,” and “prognosis or prognostic or outcome.” Criteria that an eligible study has to meet were as follows: 1) CXCR4 expression evaluated in the primary NSCLC tissues; 2) researches revealing the relationship between CXCR4 expression and NSCLC clinicopathological parameters and prognosis; and 3) studies providing sufficient information to estimate hazard ratio (HR) about overall survival (OS) and 95% confidence interval (CI). The exclusion criteria included the following: 1) letters, reviews, case reports, conference abstracts, editorials, expert opinion and 2) all publications regarding in vitro/ex vivo studies, cell lines, and human xenografts.
Data extraction and methodological assessment
The following information was recorded for each study: the first author name; year of publication; the authors’ nationality; sample source; number of cases; clinicopathological parameters; tumor, node, metastasis stage; immunohistochemical staining method; antibody source; percentage rate of expression; and follow-up. Data for study characteristics and clinical responses were summarized in a table format. Heterogeneity of investigation was evaluated to determine whether the data of the various studies could be analyzed for a meta-analysis.
For the methodological evaluation of the studies, three investigators read through each publication independently and assessed and scored them according to the Newcastle–Ottawa Quality Assessment Scale (NOQAS), for cohort and case–control studies.48 Studies are rated from one to nine stars in the NOQAS, with nine stars indicating a high-quality study. Any discrepancies or disagreements were discussed, and if consensus could not be achieved, a third reviewer resolved the issue.
Patient survival analysis
An online database49 was used to assess the relevance of CXCR4 mRNA expression to relapse free survival. The database was established using gene expression data and survival information of 1,405 NSCLC patients downloaded from Gene Expression Omnibus (GEO). Briefly, CXCR4 gene was entered into the database (http://kmplot.com/analysis/index.php?p=service&cancer=lung) to obtain Kaplan–Meier survival plots, where the number at risk is indicated below the main plot. HR (and 95% CIs) and logrank P were calculated and displayed on the webpage.
Statistical analysis
Analysis was conducted using the STATA 12 (StataCorp LP, College Station, TX, USA) and Review Manager 5.2 (Cochrane Collaboration, Oxford, UK). Heterogeneity among studies was evaluated with Cochran’s Q test50 and I2 statistic.51,52 When heterogeneity was not an issue (I2 values <50%), a fixed-effect model was used to calculate parameters. If there was substantial heterogeneity (I2 values ≥50%), a random-effects model was used to pool data and attempted to identify potential sources of heterogeneity based on subgroup analyses. The pooled odds ratio (OR) was estimated for the association between CXCR4 expression and clinicopathological features. P-values tailed <0.05 were considered statistically significant.
Publication bias was assessed by using a method reported by Egger et al.53 The analysis of meta-regression and publication bias was performed by using STATA version 10.
Results
Based on the above inclusion and exclusion criteria, 19 studies were finally identified for the final meta-analysis, as shown in Figure S1. A total of 1,872 NSCLC patients from People’s Republic of China, Japan, France, Germany, Canada, and USA were enrolled. Their basic characteristics are summarized in Table 1. Positive CXCR4 expression was defined by IHC. Most of the studies defined CXCR4 expression positive as a part of nucleus or cytoplasm was stained. There was difference in defining the cutoff value of positive CXCR4 expression. The quality of each study was assessed using NOQAS. Of the 19 studies, eleven scored 8 points, six scored 7 points, and two scored 6 points. Hence, the studies were of a relatively high quality (Table 2). In addition, among 19 studies, only two studies did not perform multivariate analysis.54,55
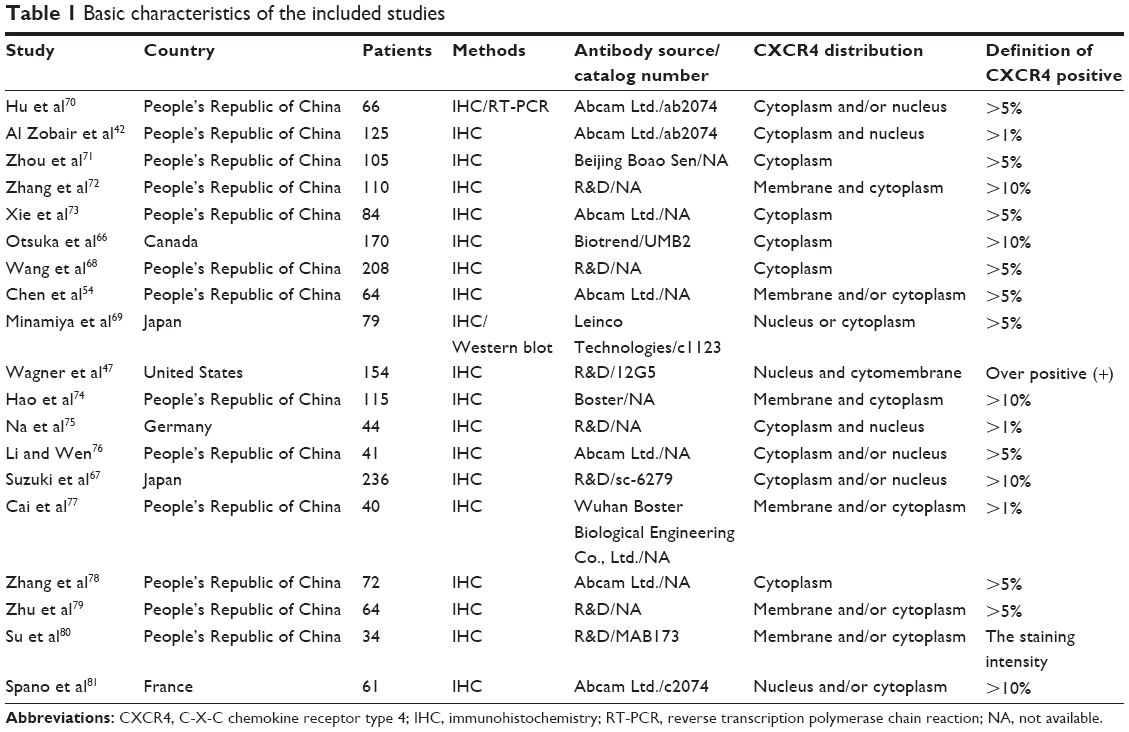 | Table 1 Basic characteristics of the included studies |
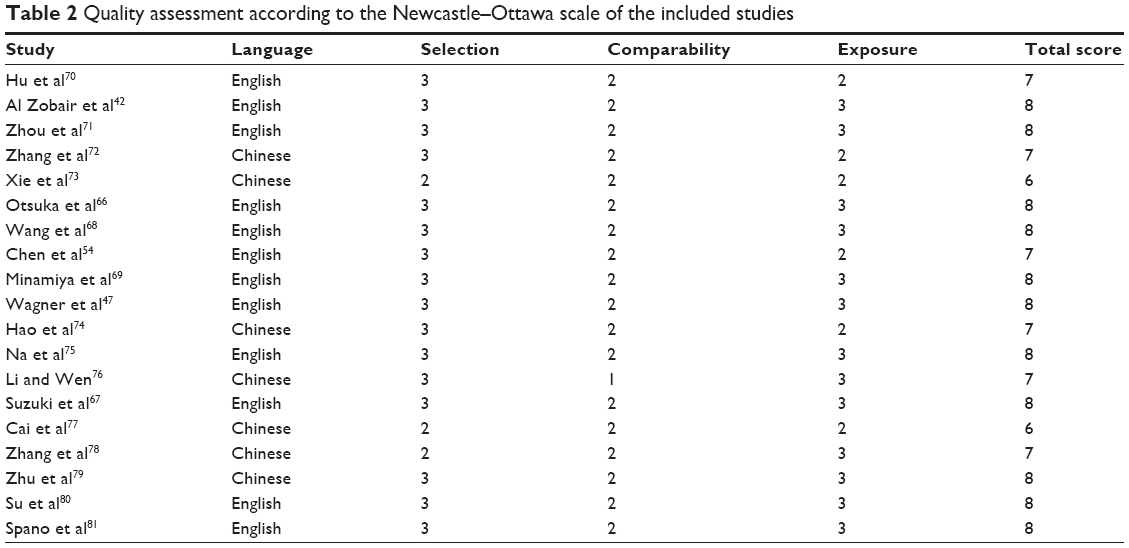 | Table 2 Quality assessment according to the Newcastle–Ottawa scale of the included studies |
We first determined whether CXCR4 expression is significantly higher in NSCLC than in normal lung tissue. The pooled OR from ten studies, including 678 NSCLCs and 189 normal lung tissues, is shown in Figure 1A. There was significant heterogeneity (I2=79%, P<0.0001), and the pooled OR was performed using a random model (OR =16.66, 95% CI =6.94–40.02, P<0.00001), which indicated that CXCR4 expression is significantly higher in NSCLC than in the normal lung tissue. We then analyzed 942 NSCLC patients pooled from ten studies to assess whether CXCR4 expression in NSCLC was associated with advanced stage. As shown in Figure 1B, aberrant CXCR4 expression was significantly higher in advanced staged NSCLC (III and IV) than that in early staged NSCLC (I and II), OR =2.75, 95% CI =1.52–4.99, P=0.0008. However, as shown in Figure S2, aberrant CXCR4 expression was not significantly higher in poorly differentiated NSCLC than that in moderately and highly differentiated NSCLC, OR =1.63, 95% CI =0.87–3.05, P=0.13. These results suggest that CXCR4 expression may not associate with tumor’s differentiated status, but it may play an important role in NSCLC progression and metastasis. We further analyzed 1,395 NSCLC patients pooled from 14 studies to assess whether CXCR4 expression in NSCLC was associated with metastatic status. As shown in Figure 2A, aberrant CXCR4 expression was significantly higher in metastatic NSCLC than in nonmetastatic NSCLC, OR =4.31, 95% CI =2.27–8.20, P<0.00001. These results suggest that CXCR4 expression is strongly correlated with metastatic status in NSCLC patients. For studies evaluating OS, we identified five studies that estimated the relationship between CXCR4 expression and OS in NSCLC. Since the heterogeneity between studies for CXCR4 (I2=22%, P=0.27) was not significant, a fixed model was applied to calculate a pooled HR and its 95% CI. The pooled HR for OS showed that CXCR4 expression was significantly associated with worse survival in NSCLC patients as shown in Figure 2B (HR =3.63, 95% CI =2.57–5.13, P<0.00001).
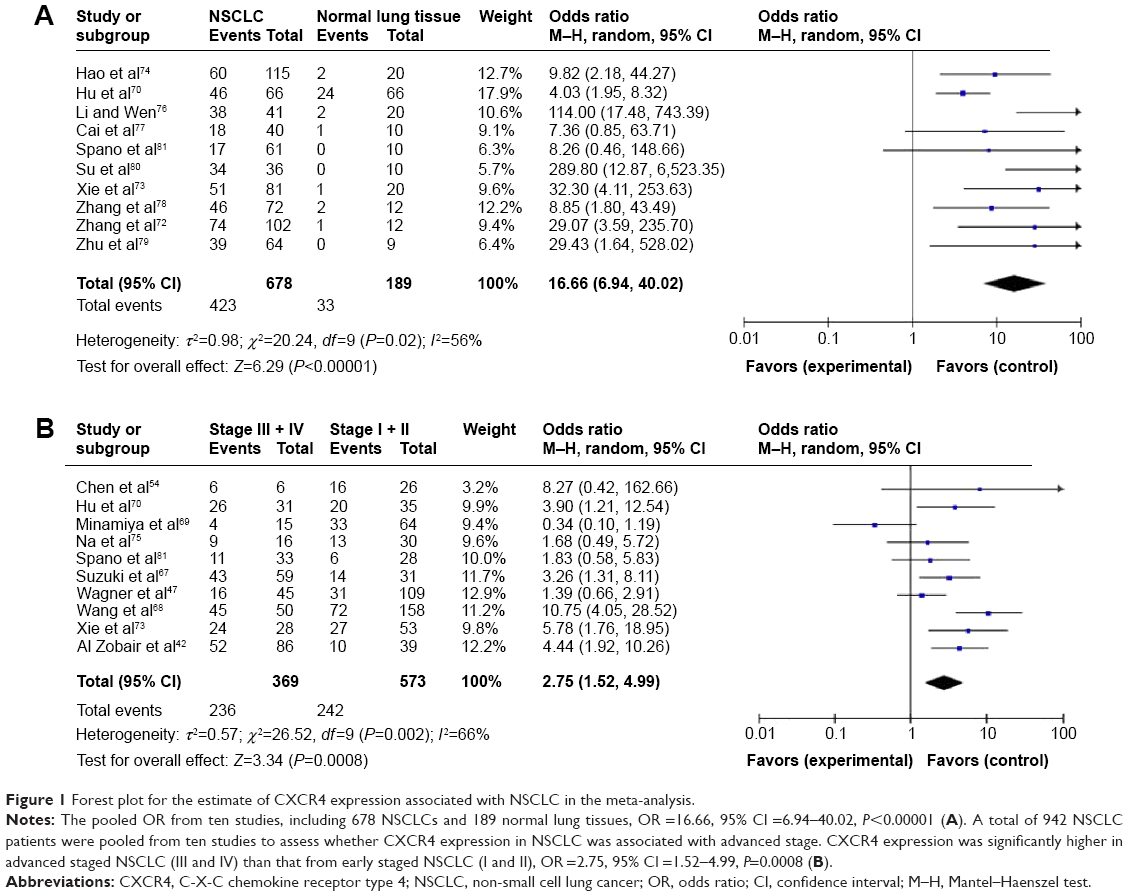 | Figure 1 Forest plot for the estimate of CXCR4 expression associated with NSCLC in the meta-analysis. |
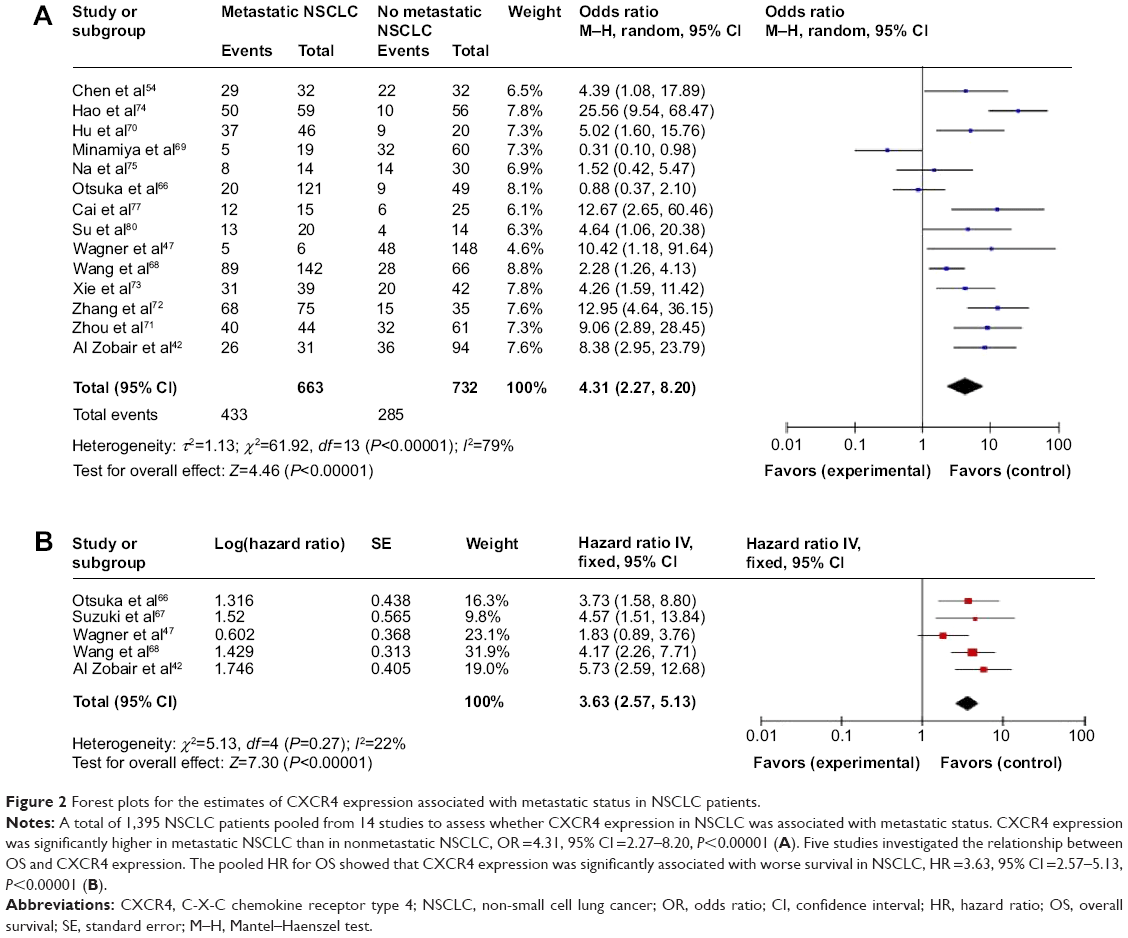 | Figure 2 Forest plots for the estimates of CXCR4 expression associated with metastatic status in NSCLC patients. |
A sensitivity analysis, in which one study was removed at a time, was conducted to assess the result stability. The pooled ORs and HRs were not significantly changed, indicating the stability of our analyses. In the case of relationship between CXCR4 expression in NSCLC and in the normal lung tissue, the overall OR is in the range from 14.39 (95% CI =12.21–18.71) to 23.5 (95% CI =10.9–50.71). The funnel plots were largely symmetric (Figure 3) suggesting that there were no publication biases in the meta-analysis.
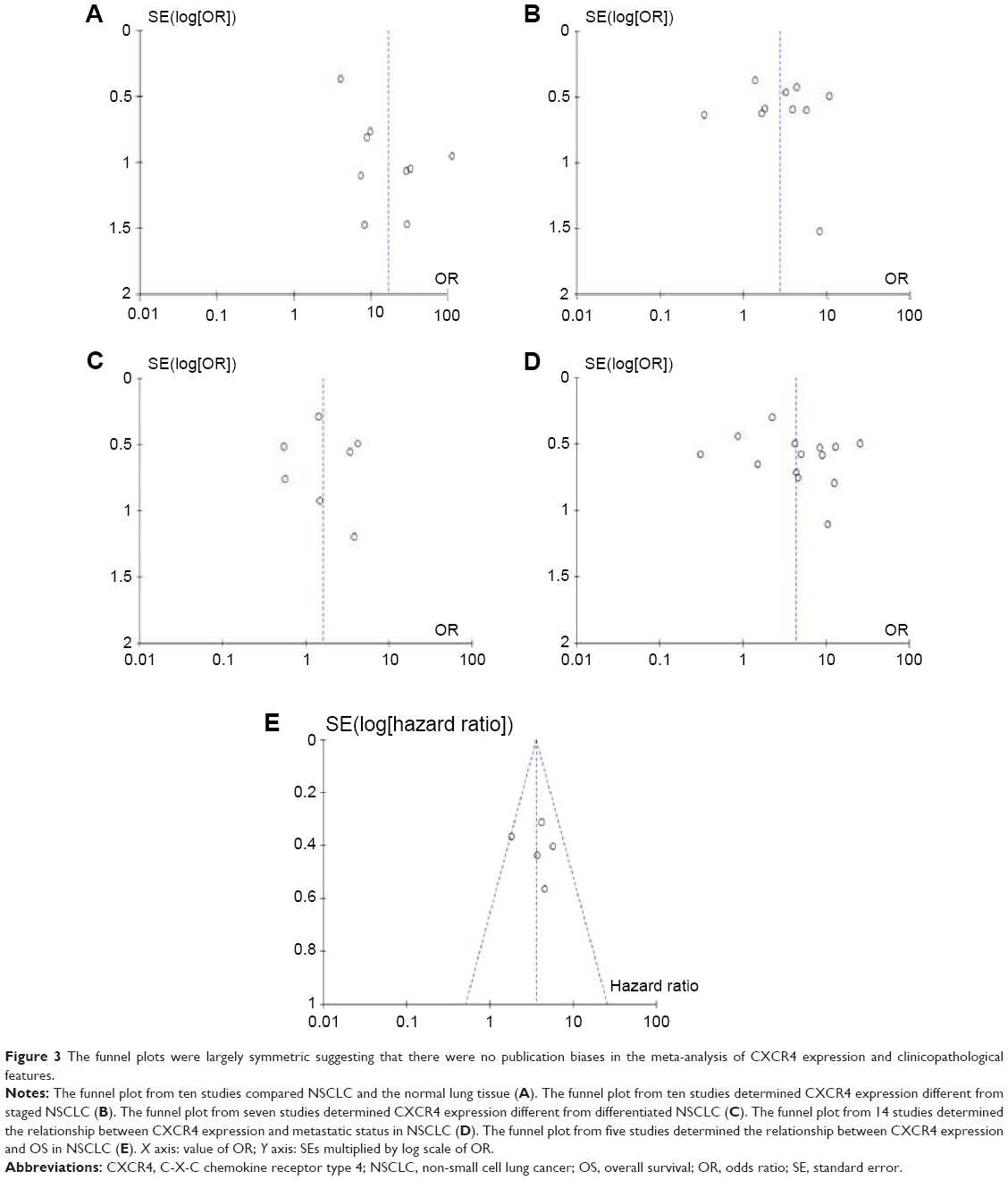 | Figure 3 The funnel plots were largely symmetric suggesting that there were no publication biases in the meta-analysis of CXCR4 expression and clinicopathological features. |
The clinical relevance of CXCR4 was further corroborated in a patient survival analysis using an online database containing the expression of 22,277 genes and 20-year survival information of 1,809 patients.49 The database has recently been updated to include survival information of 1,432 NSCLC patients (http://www.kmplot.com/analysis/). CXCR4 mRNA high expression was found to correlate with better OS of all NSCLC patients followed for 20 years (Figure 4; HR =1.24, P=0.0047).
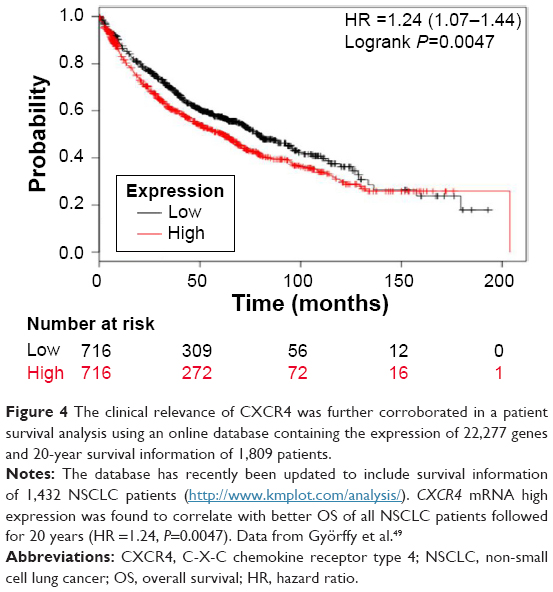 | Figure 4 The clinical relevance of CXCR4 was further corroborated in a patient survival analysis using an online database containing the expression of 22,277 genes and 20-year survival information of 1,809 patients. |
Discussion
NSCLC accounts for approximately 85% of all lung cancers and is the leading cause of cancer-related deaths worldwide.56,57 Despite the advances in early detection, radical cure operation, and multimodal therapeutic modalities, at diagnosis, there are about 80% of NSCLC cases in advanced stage, and systemic chemotherapy that remains in the standard care provides marginal improvement in survival.58 More effective and well-tolerated treatment options are needed for patients with advanced staged NSCLC. Therefore, investigation on the mechanism of initiation and progression, as well as the identification of novel drug target and prognostic marker, is still needed and will help to select the patients with high chance of lung cancer recurrence and provide better prognosis and individualized treatment. The presence of CXCR4 on lymphocytes and/or cancer cells can active chemotaxis and signify proliferation, invasion, metastasis, and angiogenesis in several cancers, including NSCLC.6,10,43,59,60 To date, there have been some studies describing the precise expression and prognostic impact of CXCR4 in NSCLC; however, the roles of CXCR4 expression in NSCLC and clinical significance have not been thoroughly investigated. We conducted the meta-analysis to determine the correlation between CXCR4 expression and clinicopathological characteristics in NSCLC. Analyses of the pooled data showed that: 1) NSCLC had a higher expression than the normal lung tissue; 2) aberrant CXCR4 expression was significantly higher in advanced staged NSCLC (III and IV) than that in early staged NSCLC (I and II); however, aberrant CXCR4 expression was not significantly higher in poorly differentiated NSCLC than in moderately and highly differentiated NSCLC; 3) aberrant CXCR4 expression was significantly higher in metastatic NSCLC than in nonmetastatic NSCLC; and 4) NSCLC patients with CXCR4 expression had a low survival rate than those without CXCR4 expression. The results from the current study demonstrated that the expression rate of CXCR4 in NSCLC was significantly higher than that in the normal lung tissue, indicating that CXCR4 expression was common in NSCLC. CXCR4 expression may not associate with tumor’s differentiated status, but it may play an important role in NSCLC progression and development. In addition, CXCR4 expression is strongly correlated with metastatic status and prognostic outcome in NSCLC patients. Information about the prognostic and predictive values of CXCR4 in NSCLC is limited. To our knowledge, the present meta-analysis is the first study to systematically evaluate the association between CXCR4 expression and clinicopathological features and prognostic factors in NSCLC.
CXCR4 exerts pleiotropic effects during tumor progression. CXCR4 mediates actin polymerization and pseudopodia formation, as well as induces chemotactic and invasive responses.8 Hence, CXCR4 plays an important role within tumor cells and the tumor microenvironment, in which the interaction influences the adhesion, migration, and invasion of tumor cells, reflecting the strong association of CXCR4 with cancer metastasis. CXCR4 expression on tumor cells is upregulated by hypoxia and angiogenic factors, such as vascular endothelial growth factor (VEGF) and hypoxia-inducible factor 1 (HIF-1); thus, CXCR4 could be a novel target of VEGF, HIF-1, and hypoxia-mediated angiogenesis.61–63 In addition, CXCR4 also appears to play a critical role in the self-renewal of cancer stem cells in NSCLC.64,65 Therefore, CXCR4 can be considered as an oncogene, and its activation could contribute to tumor progression and poor prognosis. There were five studies that evaluated the relationship between CXCR4 expression and OS in NSCLC and showed very similar results.42,47,66–68 Based on this meta-analysis, we may consider that CXCR4 expression in NSCLC tends to indicate a poor prognosis. We further determined the clinical relevance of CXCR4 mRNA expression in a patient survival analysis using an online database containing the expression of 22,277 genes and 20-year survival information of 1,405 patients.49 As expected, CXCR4 mRNA high expression was found to correlate with OS of all NSCLC patients followed for 20 years.
This meta-analysis also met heterogeneity issues. We found notable heterogeneity among the 19 studies. The heterogeneity among the studies may be due to the differences in the baseline characteristics of patients, source of samples, technical platforms, different sources of antibodies, normalization controls, cutoff values, the time of follow-up, and other technical issues. Considerable degree of heterogeneity was noticed, especially in the comparisons of metastatic vs nonmetastatic NSCLC (I2=79%). There are two studies from Japan; both of them showed that CXCR4 expression rate in metastatic NSCLC was less than nonmetastatic NSCLC (26.3% vs 53.3%; 16.5% vs 18.4%).66,69 When these two studies were removed from the meta-analysis, I2 was reduced to 60% from 79%. In the comparisons of stages III and IV vs I and II (I2=66%), I2 was significantly reduced to 47%, when one study69 from Japan was removed from meta-analysis. These results indicate that the heterogeneity may come from the different region selection biases. We also checked the heterogeneity from the comparisons of NSCLC and normal lung tissue. There is one study from People’s Republic of China, which showed that CXCR4 expression rate in the normal lung tissue is 24.6% (24/66) significantly higher than others.70 When this study was removed from the meta-analysis, I2 was dramatically reduced to 17% from 56%. This result indicates that the heterogeneity may come from the individual study. Consistent results were shown in sensitivity analyses, and no evidence of publication bias was found. This study has several potential limitations. First, the possibility of information and selection biases and unidentified confounders could not be completely excluded because all of the included studies were observational. Second, the searching strategy was restricted to articles published in English and Chinese. Articles with potentially high-quality data that were published in other languages were not included because of anticipated difficulties in obtaining accurate medical translation. Third, the samples and studies were limited by the presence of heterogeneity between the studies. In addition, in our selected 19 studies, immunohistochemical staining of CXCR4 is mixed and the definition of CXCR4 positive by IHC, as well as the cutoff value of positive CXCR4 expression, has not reached a consensus yet. This situation will make more difficult to interpret the data, and the readers should take precautions of data interpretation and hopefully get the attentions from the future clinical trail designers to consider more about the protein localization and the cutoff value. Hence, cautions should be taken when our findings are interpreted among the general population.
In conclusion, our meta-analysis showed that high CXCR4 expression was associated with an increased risk and worse survival in NSCLC patients. The aberrant CXCR4 expression plays an important role in the carcinogenesis and metastasis of NSCLC. Thus, it is safe to say that the remarkable potential of CXCR4 could serve as a prognostic biomarker for patients with NSCLC. Further large-scale studies, especially multicenter, could serve well-matched cohort. Research will provide more insight into the role of CXCR4 in the prognosis and clinical implementation of NSCLC patients.
Funding
The authors have no financial involvement with any organization or entity or financial interest in the subject matter or materials discussed in the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Sarvaiya PJ, Guo D, Ulasov I, Gabikian P, Lesniak MS. Chemokines in tumor progression and metastasis. Oncotarget. 2013;4:2171–2185. | ||
Vinader V, Afarinkia K. The emerging role of CXC chemokines and their receptors in cancer. Future Med Chem. 2012;4:853–867. | ||
Ghanem I, Riveiro ME, Paradis V, Faivre S, de Parga PM, Raymond E. Insights on the CXCL12-CXCR4 axis in hepatocellular carcinoma carcinogenesis. Am J Transl Res. 2014;6:340–352. | ||
Moriuchi M, Moriuchi H, Turner W, Fauci AS. Cloning and analysis of the promoter region of CXCR4, a coreceptor for HIV-1 entry. J Immunol. 1997;159:4322–4329. | ||
Caruz A, Samsom M, Alonso JM, et al. Genomic organization and promoter characterization of human CXCR4 gene. FEBS Lett. 1998;426:271–278. | ||
Cojoc M, Peitzsch C, Trautmann F, Polishchuk L, Telegeev GD, Dubrovska A. Emerging targets in cancer management: role of the CXCL12/CXCR4 axis. Onco Targets Ther. 2013;6:1347–1361. | ||
Domanska UM, Kruizinga RC, Nagengast WB, et al. A review on CXCR4/CXCL12 axis in oncology: no place to hide. Eur J Cancer. 2013;49:219–230. | ||
Sun X, Cheng G, Hao M, et al. CXCL12/CXCR4/CXCR7 chemokine axis and cancer progression. Cancer Metastasis Rev. 2010;29:709–722. | ||
Zhang Z, Ni C, Chen W, et al. Expression of CXCR4 and breast cancer prognosis: a systematic review and meta-analysis. BMC Cancer. 2014;14:49. | ||
Mukherjee D, Zhao J. The role of chemokine receptor CXCR4 in breast cancer metastasis. Am J Cancer Res. 2013;3:46–57. | ||
Hiller D, Chu QD. CXCR4 and axillary lymph nodes: review of a potential biomarker for breast cancer metastasis. Int J Breast Cancer. 2011;2011:420981. | ||
Wang J, Cai J, Han F, et al. Silencing of CXCR4 blocks progression of ovarian cancer and depresses canonical Wnt signaling pathway. Int J Gynecol Cancer. 2011;21:981–987. | ||
Miyanishi N, Suzuki Y, Simizu S, Kuwabara Y, Banno K, Umezawa K. Involvement of autocrine CXCL12/CXCR4 system in the regulation of ovarian carcinoma cell invasion. Biochem Biophys Res Commun. 2010;403:154–159. | ||
Yang YC, Lee ZY, Wu CC, Chen TC, Chang CL, Chen CP. CXCR4 expression is associated with pelvic lymph node metastasis in cervical adenocarcinoma. Int J Gynecol Cancer. 2007;17:676–686. | ||
Kodama J, Hasengaowa, Kusumoto T, et al. Association of CXCR4 and CCR7 chemokine receptor expression and lymph node metastasis in human cervical cancer. Ann Oncol. 2007;18:70–76. | ||
Chang YW, Chen MW, Chiu CF, et al. Arsenic trioxide inhibits CXCR4-mediated metastasis by interfering miR-520h/PP2A/NF-kappaB signaling in cervical cancer. Ann Surg Oncol. 2014;22:22. | ||
Murakami T, Kawada K, Iwamoto M, et al. The role of CXCR3 and CXCR4 in colorectal cancer metastasis. Int J Cancer. 2013;132:276–287. | ||
Zeelenberg IS, Ruuls-Van Stalle L, Roos E. The chemokine receptor CXCR4 is required for outgrowth of colon carcinoma micrometastases. Cancer Res. 2003;63:3833–3839. | ||
Gros SJ, Graeff H, Drenckhan A, et al. CXCR4/SDF-1alpha-mediated chemotaxis in an in vivo model of metastatic esophageal carcinoma. In Vivo. 2012;26:711–718. | ||
Gros SJ, Kurschat N, Drenckhan A, et al. Involvement of CXCR4 chemokine receptor in metastastic HER2-positive esophageal cancer. PLoS One. 2012;7:e47287. | ||
Hashimoto I, Koizumi K, Tatematsu M, et al. Blocking on the CXCR4/mTOR signalling pathway induces the anti-metastatic properties and autophagic cell death in peritoneal disseminated gastric cancer cells. Eur J Cancer. 2008;44:1022–1029. | ||
Yasumoto K, Koizumi K, Kawashima A, et al. Role of the CXCL12/CXCR4 axis in peritoneal carcinomatosis of gastric cancer. Cancer Res. 2006;66:2181–2187. | ||
Xiang Z, Zeng Z, Tang Z, et al. Increased expression of vascular endothelial growth factor-C and nuclear CXCR4 in hepatocellular carcinoma is correlated with lymph node metastasis and poor outcome. Cancer J. 2009;15:519–525. | ||
Schimanski CC, Bahre R, Gockel I, et al. Dissemination of hepatocellular carcinoma is mediated via chemokine receptor CXCR4. Br J Cancer. 2006;95:210–217. | ||
Li N, Guo W, Shi J, et al. Expression of the chemokine receptor CXCR4 in human hepatocellular carcinoma and its role in portal vein tumor thrombus. J Exp Clin Cancer Res. 2010;29:156. | ||
Yao X, Zhou L, Han S, Chen Y. High expression of CXCR4 and CXCR7 predicts poor survival in gallbladder cancer. J Int Med Res. 2011;39:1253–1264. | ||
Lee HJ, Lee K, Lee DG, et al. Chemokine (C-X-C motif) ligand 12 is associated with gallbladder carcinoma progression and is a novel independent poor prognostic factor. Clin Cancer Res. 2012;18:3270–3280. | ||
Huang CS, Tang SJ, Chung LY, et al. Galectin-1 upregulates CXCR4 to promote tumor progression and poor outcome in kidney cancer. J Am Soc Nephrol. 2014;25(7):1486–1495. | ||
Wang L, Huang T, Chen W, et al. Silencing of CXCR4 by RNA interference inhibits cell growth and metastasis in human renal cancer cells. Oncol Rep. 2012;28:2043–2048. | ||
Pan J, Mestas J, Burdick MD, et al. Stromal derived factor-1 (SDF-1/CXCL12) and CXCR4 in renal cell carcinoma metastasis. Mol Cancer. 2006;5:56. | ||
Park HD, Lee Y, Oh YK, et al. Pancreatic adenocarcinoma upregulated factor promotes metastasis by regulating TLR/CXCR4 activation. Oncogene. 2011;30:201–211. | ||
Jiang YM, Li G, Sun BC, Zhao XL, Zhou ZK. Study on the relationship between CXCR4 expression and perineural invasion in pancreatic cancer. Asian Pac J Cancer Prev. 2014;15:4893–4896. | ||
Wong D, Kandagatla P, Korz W, Chinni SR. Targeting CXCR4 with CTCE-9908 inhibits prostate tumor metastasis. BMC Urol. 2014;14:12. | ||
Cho KS, Yoon SJ, Lee JY, et al. Inhibition of tumor growth and histopathological changes following treatment with a chemokine receptor CXCR4 antagonist in a prostate cancer xenograft model. Oncol Lett. 2013;6:933–938. | ||
Conley-LaComb MK, Saliganan A, Kandagatla P, Chen YQ, Cher ML, Chinni SR. PTEN loss mediated Akt activation promotes prostate tumor growth and metastasis via CXCL12/CXCR4 signaling. Mol Cancer. 2013;12:85. | ||
Gelmini S, Mangoni M, Castiglione F, et al. The CXCR4/CXCL12 axis in endometrial cancer. Clin Exp Metastasis. 2009;26:261–268. | ||
Luczak MW, Roszak A, Pawlik P, et al. Transcriptional analysis of CXCR4, DNMT3A, DNMT3B and DNMT1 gene expression in primary advanced uterine cervical carcinoma. Int J Oncol. 2012;40:860–866. | ||
Beider K, Begin M, Abraham M, et al. CXCR4 antagonist 4F-benzoyl-TN14003 inhibits leukemia and multiple myeloma tumor growth. Exp Hematol. 2011;39:282–292. | ||
Azab AK, Runnels JM, Pitsillides C, et al. CXCR4 inhibitor AMD3100 disrupts the interaction of multiple myeloma cells with the bone marrow microenvironment and enhances their sensitivity to therapy. Blood. 2009;113:4341–4351. | ||
Bertolini F, Dell’Agnola C, Mancuso P, et al. CXCR4 neutralization, a novel therapeutic approach for non-Hodgkin’s lymphoma. Cancer Res. 2002;62:3106–3112. | ||
Choi YH, Burdick MD, Strieter BA, Mehrad B, Strieter RM. CXCR4, but not CXCR7, discriminates metastatic behavior in non-small cell lung cancer cells. Mol Cancer Res. 2014;12:38–47. | ||
Al Zobair AA, Al Obeidy BF, Yang L, et al. Concomitant overexpression of EGFR and CXCR4 is associated with worse prognosis in a new molecular subtype of non-small cell lung cancer. Oncol Rep. 2013;29:1524–1532. | ||
Wald O, Shapira OM, Izhar U. CXCR4/CXCL12 axis in non small cell lung cancer (NSCLC) pathologic roles and therapeutic potential. Theranostics. 2013;3:26–33. | ||
Fahham D, Weiss ID, Abraham M, et al. In vitro and in vivo therapeutic efficacy of CXCR4 antagonist BKT140 against human non-small cell lung cancer. J Thorac Cardiovasc Surg. 2012;144(1167–1175):e1. | ||
Reckamp KL, Figlin RA, Burdick MD, Dubinett SM, Elashoff RM, Strieter RM. CXCR4 expression on circulating pan-cytokeratin positive cells is associated with survival in patients with advanced non-small cell lung cancer. BMC Cancer. 2009;9:213. | ||
Rodriguez-Lara V, Peña-Mirabal E, Baez-Saldaña R, et al. Estrogen receptor beta and CXCR4/CXCL12 expression: differences by sex and hormonal status in lung adenocarcinoma. Arch Med Res. 2014;45:158–169. | ||
Wagner PL, Hyjek E, Vazquez MF, et al. CXCL12 and CXCR4 in adenocarcinoma of the lung: association with metastasis and survival. J Thorac Cardiovasc Surg. 2009;137:615–621. | ||
Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Health Research Institute, Ottowa; 2010. Available from: http://wwwohrica/programs/clinical_epidemiology/oxford.htm. Accessed July 20, 2010. | ||
Györffy B, Lanczky A, Eklund AC, et al. An online survival analysis tool to rapidly assess the effect of 22,277 genes on breast cancer prognosis using microarray data of 1,809 patients. Breast Cancer Res Treat. 2010;123:725–731. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. | ||
DerSimonian R. Meta-analysis in the design and monitoring of clinical trials. Stat Med. 1996;15:1237–1248. [discussion 49–52]. | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. | ||
Chen G, Wang Z, Liu XY, Liu FY. High-level CXCR4 expression correlates with brain-specific metastasis of non-small cell lung cancer. World J Surg. 2011;35:56–61. | ||
Zhang Y, Li H, Qi Y, Haofeng C, Shinan F, Chenkun W. Expression of CXCR4 in lung cancer tissue array and clinical significance. Guide Chin Med. 2012;10(36):448–450. | ||
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. | ||
Guo P, Huang ZL, Yu P, Li K. Trends in cancer mortality in China: an update. Ann Oncol. 2012;23:2755–2762. | ||
Ramalingam S, Belani C. Systemic chemotherapy for advanced non-small cell lung cancer: recent advances and future directions. Oncologist. 2008;13(Suppl 1):5–13. | ||
Nayak TR, Hong H, Zhang Y, Cai W. Multimodality imaging of CXCR4 in cancer: current status towards clinical translation. Curr Mol Med. 2013;13:1538–1548. | ||
Lombardi L, Tavano F, Morelli F, Latiano TP, Di Sebastiano P, Maiello E. Chemokine receptor CXCR4: role in gastrointestinal cancer. Crit Rev Oncol Hematol. 2013;88:696–705. | ||
Liekens S, Schols D, Hatse S. CXCL12-CXCR4 axis in angiogenesis, metastasis and stem cell mobilization. Curr Pharm Des. 2010;16:3903–3920. | ||
Liu YL, Yu JM, Song XR, Wang XW, Xing LG, Gao BB. Regulation of the chemokine receptor CXCR4 and metastasis by hypoxia-inducible factor in non small cell lung cancer cell lines. Cancer Biol Ther. 2006;5:1320–1326. | ||
Zagzag D, Lukyanov Y, Lan L, et al. Hypoxia-inducible factor 1 and VEGF upregulate CXCR4 in glioblastoma: implications for angiogenesis and glioma cell invasion. Lab Invest. 2006;86:1221–1232. | ||
Jung MJ, Rho JK, Kim YM, et al. Upregulation of CXCR4 is functionally crucial for maintenance of stemness in drug-resistant non-small cell lung cancer cells. Oncogene. 2013;32:209–221. | ||
Murakami A, Takahashi F, Nurwidya F, et al. Hypoxia increases gefitinib-resistant lung cancer stem cells through the activation of insulin-like growth factor 1 receptor. PLoS One. 2014;9:e86459. | ||
Otsuka S, Klimowicz AC, Kopciuk K, et al. CXCR4 overexpression is associated with poor outcome in females diagnosed with stage IV non-small cell lung cancer. J Thorac Oncol. 2011;6:1169–1178. | ||
Suzuki M, Mohamed S, Nakajima T, et al. Aberrant methylation of CXCL12 in non-small cell lung cancer is associated with an unfavorable prognosis. Int J Oncol. 2008;33:113–119. | ||
Wang M, Chen GY, Song HT, Hong X, Yang ZY, Sui GJ. Significance of CXCR4, phosphorylated STAT3 and VEGF-A expression in resected non-small cell lung cancer. Exp Ther Med. 2011;2:517–522. | ||
Minamiya Y, Saito H, Takahashi N, et al. Expression of the chemokine receptor CXCR4 correlates with a favorable prognosis in patients with adenocarcinoma of the lung. Lung Cancer. 2010;68:466–471. | ||
Hu T, Yao Y, Yu S, et al. [CXCR4 and Nrf2 expressions in non-small cell lung cancer and their clinical implications]. Nan Fang Yi Ke Da Xue Xue Bao. 2014;34:153–158. Chinese. | ||
Zhou Z, Chen ZW, Yang XH, et al. Establishment of a biomarker model for predicting bone metastasis in resected stage III non-small cell lung cancer. J Exp Clin Cancer Res. 2012;31:34. | ||
Zhang Y, Li H, Qi Y, Haofeng C, Shinan F, Chenkun W. Expression of CXCR4 in lung cancer tissue array and clinical significance. Chin Med. 2012;36(2):78–82. | ||
Xie S, Zeng W, Zuo T, et al. Expression and significance of CXCR4 chemokine receptor in non small cell lung cancer. Chin J Gen Pract. 2012;10(9):234–236. | ||
Hao X, Ren Y, Chen X, Wei L, Li W. Expression and clinical significance of chemokine receptor CXCR4 in lung cancer and its corresponding lymph node metastasis. Clin Chin Army Med. 2009;37(3):56–61. | ||
Na IK, Scheibenbogen C, Adam C, et al. Nuclear expression of CXCR4 in tumor cells of non-small cell lung cancer is correlated with lymph node metastasis. Hum Pathol. 2008;39:1751–1755. | ||
Li X, Wen J. The significance of CXCR4 expression in non small cell lung cancer. Journal of Chongqing Med Univ. 2008;4:407–410. | ||
Cai Y, Xin J, Shi X, Tian S. The expressions of stromal-cell derived factor 1(SDF-1), CXC chemokin receptor 4(CXCR4) and their clinical significances in human non-small cell lung cancer. Chin J Cancer Res. 2006;33(8):578–580. | ||
Zhang M, Yu S, Xia S. Chemokine receptor CXCR4 expression with invasion and metastasis of lung cancer. J Huazhong Univ Sci Technol Med Sci. 2006;6:801–803. | ||
Zhu D, Ma Y, Thang X. The clinical significance of chemokine receptor CCR7, CXCR4 expression in non-small cell lung cancer. Shandong Pharm. 2006;11:176–178. | ||
Su L, Zhang J, Xu H, et al. Differential expression of CXCR4 is associated with the metastatic potential of human non-small cell lung cancer cells. Clin Cancer Res. 2005;11:8273–8280. | ||
Spano JP, Andre F, Morat L, et al. Chemokine receptor CXCR4 and early-stage non-small cell lung cancer: pattern of expression and correlation with outcome. Ann Oncol. 2004;15:613–617. |
Supplementary materials
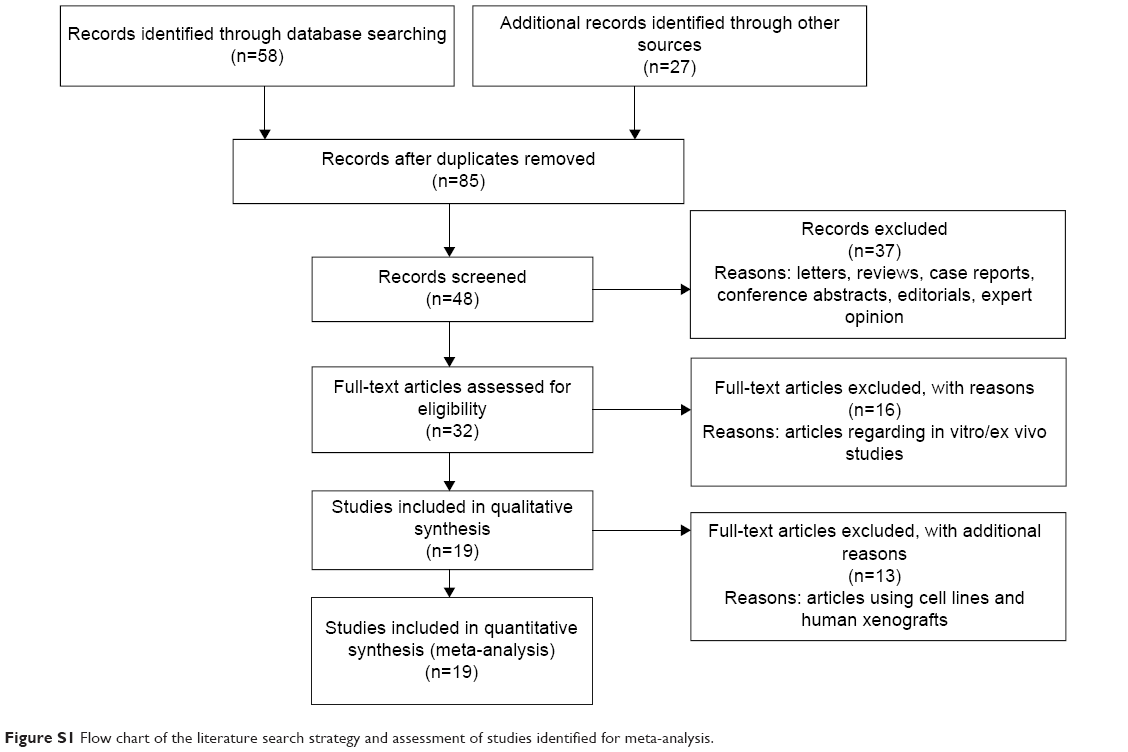 | Figure S1 Flow chart of the literature search strategy and assessment of studies identified for meta-analysis. |
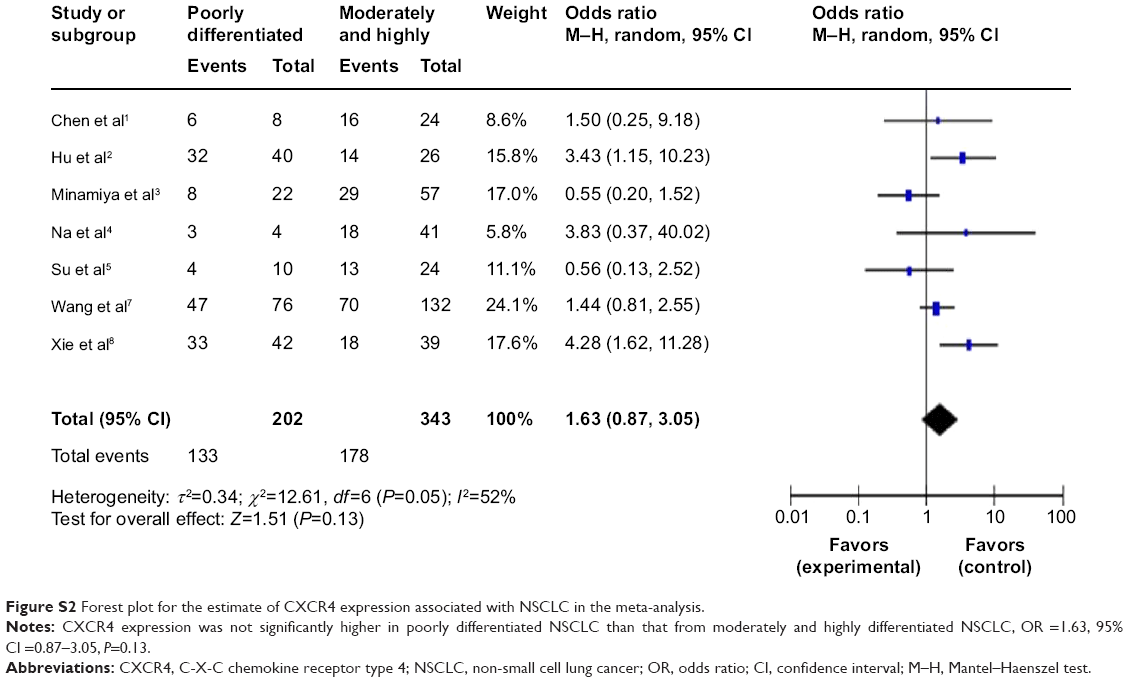 | Figure S2 Forest plot for the estimate of CXCR4 expression associated with NSCLC in the meta-analysis. |
References
Chen G, Wang Z, Liu XY, Liu FY. High-level CXCR4 expression correlates with brain-specific metastasis of non-small cell lung cancer. World J Surg. 2011;35:56–61. | ||
Hu T, Yao Y, Yu S, et al. [CXCR4 and Nrf2 expressions in non-small cell lung cancer and their clinical implications]. Nan Fang Yi Ke Da Xue Xue Bao. 2014;34:153–158. | ||
Minamiya Y, Saito H, Takahashi N, et al. Expression of the chemokine receptor CXCR4 correlates with a favorable prognosis in patients with adenocarcinoma of the lung. Lung Cancer. 2010;68:466–471. | ||
Na IK, Scheibenbogen C, Adam C, et al. Nuclear expression of CXCR4 in tumor cells of non-small cell lung cancer is correlated with lymph node metastasis. Hum Pathol. 2008;39:1751–1755. | ||
Su L, Zhang J, Xu H, et al. Differential expression of CXCR4 is associated with the metastatic potential of human non-small cell lung cancer cells. Clin Cancer Res. 2005;11:8273–8280. | ||
Wang J, Cai J, Han F, et al. Silencing of CXCR4 blocks progression of ovarian cancer and depresses canonical Wnt signaling pathway. Int J Gynecol Cancer. 2011;21:981–987. | ||
Wang M, Chen GY, Song HT, Hong X, Yang ZY, Sui GJ. Significance of CXCR4, phosphorylated STAT3 and VEGF-A expression in resected non-small cell lung cancer. Exp Ther Med. 2011;2:517–522. | ||
Xie S, Zeng W, Zuo T, et al. Expression and significance of CXCR4 chemokine receptor in non small cell lung cancer. Chin J Gen Pract. 2012;10(9):234–236. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.