")
Back to Journals » Journal of Pain Research » Volume 12
Fremanezumab in the treatment of migraines: evidence to date
Authors Robblee J , VanderPluym J
Received 5 April 2019
Accepted for publication 6 August 2019
Published 22 August 2019 Volume 2019:12 Pages 2589—2595
DOI https://doi.org/10.2147/JPR.S166427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Jennifer Robblee, Juliana VanderPluym
Department of Neurology, Mayo Clinic, Scottsdale, AZ, USA
Correspondence: Juliana VanderPluym
Department of Neurology, Mayo Clinic, 13400 E Shea Blvd, Scottsdale, AZ 85259, USA
Email [email protected]
Abstract: Calcitonin gene-related peptide (CGRP) is a major player in migraine pathophysiology, and CGRP monoclonal antibodies including fremanezumab may be a safe effective preventive therapy. Phase IIb studies in episodic migraine (EM) and chronic migraine (CM) demonstrated efficacy at both the monthly 225 mg and quarterly 675 mg doses. The Phase III trials for EM and CM both showed a reduction in the primary endpoint of monthly migraine days (MMD). In the EM trial, the baseline MMD of 8.9 days was reduced to 5.3 at 12 weeks and to 4.0 days in the 6-month open-label extension (OLE) for monthly dosing. In the quarterly dosing, the baseline was 9.2 days reduced to 5.3 at 12 weeks and to 4.2 days in the OLE. In the CM data for monthly dosing, the baseline was 16.2 days decreased to 11.4 at 12 weeks then to 8.3 in the OLE. In the CM quarterly dosing, the baseline of 16.4 days was reduced to 11.9 at 12 weeks and 9.9 days in the OLE. Randomized controlled trials of fremanezumab in both episodic cluster and post-traumatic headache are underway, but the trial for chronic cluster headache was stopped for futility. The most common adverse events are injection site pain (24% vs 22% for placebo), induration (17% vs 13% for placebo), and erythema (16% vs 12% for placebo). Severe adverse events were reported in 3.9% of the fremanezumab vs 3.7% of the placebo. No changes in vitals or ECG were reported. The long-term effects are not known, but the American Headache Society recommends that CGRP monoclonal antibodies be considered in EM or CM depending on previous medication trials and headache disability/frequency. Further, post-market studies are required, but for EM and CM fremanezumab is a new option for migraine preventive treatment.
Keywords: fremanezumab, migraine, headache, calcitonin gene-related peptide, CGRP, treatment, monoclonal antibody
Introduction
Calcitonin gene-related peptide (CGRP) is believed to play a major role in migraine pathophysiology. Evidence to date suggests that inhibition of CGRP via monoclonal antibodies including fremanezumab may be a safe and effective preventive therapy for migraine. This review will examine in more detail the CGRP monoclonal antibody fremanezumab.
Fremanezumab: a CGRP monoclonal antibody
Fremanezumab is a fully human immunoglobulin G2 (IgG2) delta a/kappa antibody made in Chinese hamster ovary cells.1,2 It is 95% humanized and 5% murine.1 It binds to both isoforms of CGRP and prevents intracellular signaling through cAMP.3 One study demonstrated that fremanezumab selectively prevents activation of A-delta but not C-fibers peripherally leading to the prevention of high threshold trigeminovascular neurons being activated and/or sensitized hence preventing the migraine pain phase.4 The half-life has been reported in the range of 32–48 days, and bioavailability is reported to be 40–74%.1,5,6 Fremanezumab is metabolized into small peptides and amino acids via enzymatic proteolysis like other monoclonal antibodies; it is not metabolized by the liver or kidney.7 It was originally developed as LBR-101 with translational work done in monkeys, and then was renamed as TEV-48125 before being released as fremanezumab.3 Fremanezumab has been extensively studied now for migraine, but studies are also underway for cluster headache and post-traumatic headache. Animal studies, as well as the inclusion of patients with chronic migraine (CM) and medication overuse (MO), also raise the question of whether this category of medication may also have MOH as a potential indication.8 While a loading dose in intravenous form has been studied, fremanezumab is currently available as a subcutaneous injection used monthly at a dose of 225 mg or quarterly at a dose of 675 mg. It is the only monoclonal antibody with the quarterly dosing option. An auto-injector is not yet available. The current pre-filled syringe comes as 1.5 mL of 150 mg/mL. Fremanezumab, marketed as Ajovy by Teva Pharmaceutical, was officially approved by the FDA on September 14, 2018 with the indication of preventive treatment for migraine in adults.
Fremanezumab in clinical trials
A Phase IIb study of high-frequency episodic migraine (HFEM) in 297 patients looked at both 225 and 675 mg subcutaneous injections every 28 days for 12 weeks. Both doses showed efficacy compared to placebo for primary and secondary endpoints of change in monthly migraine days (MMD) and in headache days from baseline at weeks 9–12, respectively.9 A Phase IIb study was similarly done for CM, including those with daily headaches and/or MO per ICHD-3 criteria, in 264 patients with different dosing. One group received 900 mg every 28 days while the low dose group received a loading dose of 675 mg followed by 225 mg every 28 days for a total of 12 weeks. Patients who had been on more than three prophylactic agents were excluded, and patients could not have been on onabotulinumtoxinA within the 6 months prior to a 28-day run-in time period. Adverse events were not significantly different from placebo, with the main one being injection site reaction.9 Post-hoc analyses of the Phase II studies showed that treatment affects started within 7 days for the 225 or 675 mg doses, and within 3 days for the higher dose studied of 900 mg when looking at number of headache hours.10 Post-hoc analyses also showed benefit in the number of MMD, headache days, and abortive medication use when fremanezumab was used as an add-on treatment for prophylaxis of episodic or CM.11 Post-hoc analysis further showed that patients with response at 1 month appeared to have sustained responses at months 2 and 3.12 Furthermore, CM and particularly EM have post-hoc evidence of functional improvement on non-headache days on fremanezumab (Table 1).13
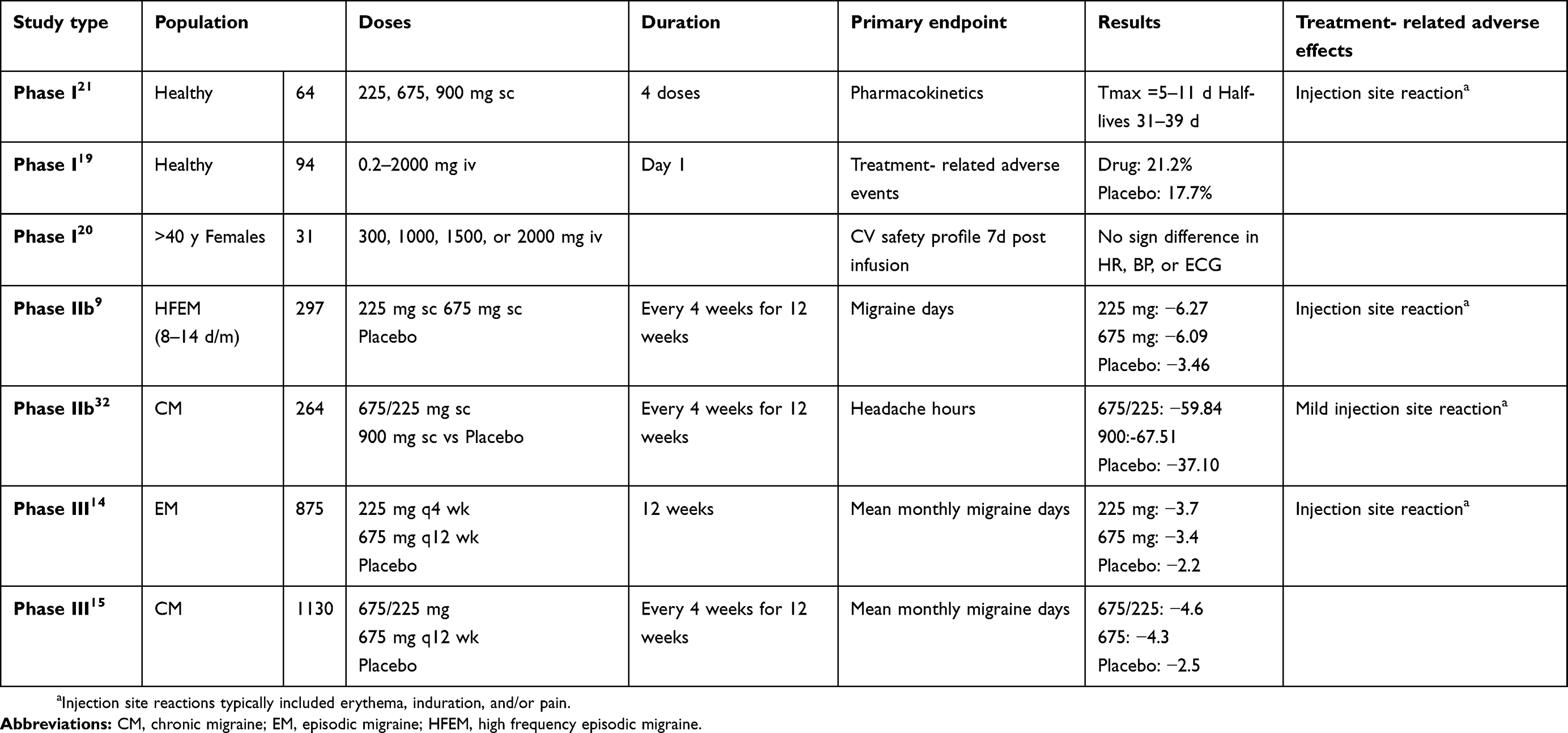 |
Table 1 Overview of Phase I to Phase III trials for fremanezumab |
The Phase III trial (HALO) for fremanezumab was done for EM patients with high frequency and less than two treatment failures. This study enrolled 875 patients from 9 countries. The primary endpoint was a decrease in MMD at the 9–12-week time point. Both the monthly 225 mg subcutaneous dose and the quarterly 675 mg subcutaneous dose showed a significant reduction in MMD relative to placebo.14 They reported a mean change compared to baseline of −3.7 days for monthly fremanezumab and −3.4 days for quarterly fremanezumab with both endpoints showing significance (p-value of <0.0001) as compared to placebo of −2.2 days. A reduction in acute migraine medication (all types) was also assessed with a 3-day reduction from 7.7 to 4.7 days in the monthly arm and a 2.9-day reduction from 7.9 to 5 days in the quarterly arm as compared to a 1.6-day reduction from 6.1 days in the placebo arm with statistical significance (p<0.001). MIDAS was decreased by 24.6 for the monthly dose and 23 for the quarterly dose as compared to 17.5 for placebo (p<0.001 and p=0.002, respectively). This reduction took the scores which on average were all in the severe range to being in the moderate range. Reported reasons for discontinuation were injection site reaction (erythema or induration), diarrhea, anxiety, or depression. Three patients were found to have liver abnormalities in treatment groups. Nasopharyngitis and upper respiratory infection were also slightly more common in the treatment groups.
The Phase III (HALO) CM study randomized 1130 patients from 132 sites to monthly fremanezumab 225 mg with a 675 mg loading dose or quarterly fremanezumab 675 mg compared to a monthly placebo.15 The primary endpoint was also mean change in MMDs at 12 weeks. They reported −4.6 days for the monthly fremanezumab with loading dose and −4.3 days for the quarterly fremanezumab as compared to placebo of −2.5 days. Both dosing schedules were found to be significant (p-value of <0.0001). The ≥50% responder rate was 41% for monthly fremanezumab, 38% for quarterly fremanezumab, and 18% for placebo (both p<0.001). The use of acute migraine treatment was reduced by 4.2 days in monthly fremanezumab, 3.7 days in quarterly fremanezumab, and 1.9 days for placebo (both p<0.001). HIT-6 was reduced by 6.8 for monthly fremanezumab, 6.4 for quarterly fremanezumab, and 4.5 for placebo (both p<0.001). Injection site reactions were reported in 47% of the treatment compared to 40% of the placebo (p=0.03). Post-hoc data also showed benefit in CM in patients with concurrent topiramate or onabotulinumtoxinA.16
The first 6 months of data for the 1-year open-label extension (OLE) of the Phase III trials for both EM and CM were presented at the American Headache Society 61st meeting in 2018. They reported on 312 new patients assigned to monthly or quarterly dosing. They reviewed the reduction in MMD as compared to the 12-week randomized controlled data. In the EM trial, monthly dosing had a baseline MMD of 8.9 that reduced to 5.3 days at 12 weeks within the randomized controlled trial, and at 6 months in the OLE the MMD was reported as 4.0 days. In the quarterly dosing, the baseline and 12 weeks MMDs were 9.2 days and 5.3 days, respectively with the 6-month OLE data showing a further reduction to 4.2 days. In the CM data, the baseline and 12 weeks randomized controlled data for the monthly dosing were 16.2 days decreased to 11.4 days. At 6 months the CM monthly dosing was further reduced to 8.3 days. In the CM quarterly dosing, the baseline and 12 week MMD were 16.4 days reduced to 11.9 days, while the 6-month OLE data were 9.9 days. The >50% responder rates did not change between 12 weeks and 6 months. Days of acute medication use were further reduced at 6 months compared to baseline and 12 weeks in the EM OLE as well. MIDAS was also reduced for the monthly dosing, but not the quarterly, at 6 months though all numbers decreased from the severe range. Injection site reactions were the main reported adverse event.17
Fremanezumab and other headache conditions
A 13-week multicenter, double-blind randomized placebo-controlled trial of fremanezumab efficacy in episodic cluster headache is underway with completion expected for end of February 2019. Unfortunately, the chronic cluster headache trial was stopped in June 2018 due to futility. There is also a Phase II, multicenter, randomized, double-blind, placebo-controlled study comparing one subcutaneous dose of fremanezumab vs placebo for persistent post-traumatic headache prophylaxis. The estimated study completion date is December 11, 2019.
Safety of fremanezumab
Based on pooled data between the Phase II and Phase III studies, there were 1702 patients exposed to fremanezumab as compared to 861 placebo.17 In total, at least 2773 patients have been exposed to at least one dose of fremanezumab including 262 healthy volunteers. Overall the rates of adverse events were similar between fremanezumab (1.2%) and placebo (1.6%) in controlled trials.18 Fremanezumab had no treatment-related safety events that differed from placebo. After intravenous infusion with doses up to 2000 mg in women over 40 years of age, no significant changes were found in heart rate, blood pressure, or ECG.19,20 Only two major safety events were reported in the Phase I study, and neither had treatment-related causality. One was a thoracic abdominal aneurysm in a patient with previously unreported Ehlers-Danlos syndrome and another was glaucoma with increased intra-ocular pressure 84 days after treatment.21 In data already presented from the OLE, no deaths occurred, and only 4% of the patients withdrew.17 In the Phase II and III trials, the most common adverse effect was injection site reaction. There were three patients with drug hypersensitivity of which two were on placebo. Respiratory events were no different between drug and placebo groups.17 While anti-drug antibodies were reported, none had clinically significant events. Of 1888 tested, only 30 had antibodies identified against fremanezumab.18,21
According to data from the FDA, two patients, both receiving the quarterly 675 mg dose, died in the clinical trials. They were both felt to be unrelated to treatment. One death was 110 days after last drug exposure, and was determined to be due to intentional drug overdose from diphenhydramine. This patient withdrew from the study. Another patient died 69 days after drug exposure, and cause of death was determined to be chronic obstructive pulmonary disease.18
The most common adverse events reports were injection site pain (24% fremanezumab, 22% placebo), injection site induration (17% fremanezumab, 13% placebo), and injection site erythema (16% fremanezumab, 12% placebo). There were reports of upper respiratory tract infections (4%) and nasopharyngitis (4%). Unlike erenumab, constipation has not been reported as a common adverse effect despite the fact that fremanezumab does block the beta form of CGRP which is found in the enteric nervous system. Severe adverse events were reported in 3.9% of the patients receiving fremanezumab vs with 3.7% of the placebo. Importantly, no changes in vitals or ECG were reported in these studies including when studied in CM with concurrent use of triptans.22 While there was no increased risk of cardiovascular events, documented cases have included sudden death in a patient with significant vascular risk factors, two episodes of hypertensive crises, one episode of angina with new hypertension, one stroke, one transient ischemic attack, three deep vein thromboses, and one new onset atrial fibrillation. Safety with fremanezumab in cardiac patients has not been studied directly, but there was a study with erenumab that demonstrated no significant effect on exercise time in a high-risk cardiovascular population with the conclusion that myocardial ischemia was not worsened.23 Adverse events related to ophthalmologic conditions were also looked at due to a concern raised from animal studies, though these findings were not reproduced. Safety data demonstrated <1% ophthalmologic disorders. Specific cases described included bilateral retinal detachment after fremanezumab 675 mg and vitreous detachment after 2 doses of fremanezumab 675 mg (taken monthly). Two cases of retina tears were also reported as well as individual cases of unilateral retinal detachment, vitreous detachment, vitreous prolapse, and unilateral vision loss. The direct correlation of these events to fremanezumab is currently unclear.
One concern raised with the CGRP monoclonal antibodies is whether it is safe during pregnancy and lactation as the effects in humans are unknown at this time. When given to rats or rabbits at high doses during organogenesis no adverse developmental effects were seen.24 It is known that CGRP is elevated during pregnancy, and it has been hypothesized that the elevation causes increased plasma volume through vasodilation.25,26 It is unknown what effect not having CGRP elevation during pregnancy would have, but one theory is that it may increase the risk of hypertension during pregnancy.25 If true, then it also raises the question whether long-term CGRP blockade may also increase the risk of hypertension in general. Pregnancy elevations in CGRP fall back done to normal within 5–7 days following the postpartum period. Safety during breastfeeding is also unknown. Fremanezumab is a large molecule protein with a molecular weight of 148,000 so it is unlikely that much is excreted in breast milk. A risk to the breast-fed infant cannot be excluded during the first 3 days postpartum due to the wider gaps between breast alveolar cells that allow these large immunoglobulins to pass; however, in humans, the primary immunoglobulins in milk are IgA with IgG only comprising 2%.27,28 The amount in breastmilk is likely destroyed in the gastrointestinal tract. While fremanezumab has not been studied specifically, it is known that pasteurization of IgG2 reduces activity by 50%.2
Outside of pregnancy, other patient populations for which CGRP antagonism may be worrisome have been considered. The occurrence of subarachnoid hemorrhage (SAH) in a patient on fremanezumab or similar could lead to a higher rate of vasospasm as it has been shown that CGRP is elevated in patients with SAH, and those without vasospasm tended to have higher levels.29 This protective effect also raises the question of safety in the setting of stroke – could a transient ischemic attack or minor stroke be converted to a larger more debilitating stroke with these agents? The same question is raised for those with unstable angina and the risk of myocardial infarction. The long-term effects are also not known. In a mouse model with CGRP gene deletion, renal failure was seen though clinically there has been no signal of renal dysfunction in those receiving fremanezumab. Other observations in mice lacking CGRP were high core temperature, decreased daytime respiration, and increased energy expenditure. The concern raised is that both cardiac and renal failure could be a result of loss of CGRP in part due to hypertension.30 Another unknown at this time is whether increased access to the central nervous system by fremanezumab and similar medications in the setting of disruption of the blood-brain barrier as seen in infection, trauma, or seizures, will lead to centrally mediated adverse effects. Additionally, safety and effectiveness in pediatric and geriatric patients have not been established.
Conclusion
Fremanezumab is one of the three new CGRP monoclonal antibodies. It acts against the calcitonin-gene-related peptide (CGRP) ligand directly affecting this neuropeptide that has been shown to be integral to migraine pathophysiology. At this time, the prophylactic effects in EM and CM have been shown to be likely comparable across this class of medications, and may be comparable to our current prophylactic options but with better tolerability as well as no need for titration, good compliance, short latency of action, presence of super-responders and effect in patients with multiple previous ineffective treatment trials including those with MO. Benefits for other conditions like cluster headache and post-traumatic headache have yet to be determined though early reports do suggest benefit in episodic cluster headache. The long-term effects are still not known, but per the American Headache Society, CGRP monoclonal antibodies may be considered in patients of at least 18 years of age with a diagnosis of migraine with or without aura. In those with a low headache frequency of 4–7 days per month, it is recommended that they have a moderate disability, and have an ineffective trial or intolerance to topiramate, divalproex sodium, beta blocker, tricyclic antidepressant, SNRI, or other level A-B prophylactic therapy. In those with high-frequency EM, level of disability is not a requirement. In CM, an ineffective trial of onabotulinumtoxinA for 2 cycles is sufficient.31 However, there is limited evidence to guide patient selection between each of the antibodies. Benefit is likely to be seen in the setting of multiple medication failures and MO headache however this medication has benefit for not only complex patients but the entire migraine population with indication for prophylaxis. Further post-market studies are required at this time for fremanezumab to better understand its clinical efficacy and safety and to learn the long-term effects of this new exciting class of medication.
Disclosure
Dr. Juliana VanderPluym reports grants from Amgen, personal fees from Healint, personal fees from Teva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tepper SJ. History and review of anti-calcitonin Gene-Related Peptide (CGRP) therapies: from translational research to treatment. Headache. 2018;58 Suppl 3:238–275.
2. Fremanezumab. Drugs and Lactation Database (lactmed). Bethesda (MD): National Library of Medicine (US); 2006.
3. Walter S, Bigal ME. TEV-48125: a review of a monoclonal CGRP antibody in development for the preventive treatment of migraine. Curr Pain Headache Rep. 2015;19(3):6.
4. Melo-Carrillo A, Strassman AM, Nir RR, et al. Fremanezumab-A humanized monoclonal anti-CGRP antibody-inhibits thinly myelinated (Adelta) but not unmyelinated (C) meningeal nociceptors. J Neurosci. 2017;37(44):10587–10596.
5. Hong P, Wu X, Liu Y. Calcitonin gene-related peptide monoclonal antibody for preventive treatment of episodic migraine: a meta analysis. Clin Neurol Neurosurg. 2017;154:74–78.
6. Bigal ME, Rapoport AM, Silberstein SD, Walter S, Hargreaves RJ, Aycardi E. From LBR-101 to fremanezumab for migraine. CNS Drugs. 2018;32(11):1025–1037. doi:10.1007/s40263-018-0579-4
7. Hussar DA, Moyer MR. Baloxavir marboxil, Fremanezumab-vfrm, Galcanezumab-gnlm, and Lofexidine hydrochloride. J Am Pharm Assoc. 2019;59(1):141–144. doi:10.1016/j.japh.2018.12.002
8. Kopruszinski CM, Xie JY, Eyde NM, et al. Prevention of stress- or nitric oxide donor-induced medication overuse headache by a calcitonin gene-related peptide antibody in rodents. Cephalalgia. 2017;37(6):560–570. doi:10.1177/0333102416650702
9. Bigal ME, Dodick DW, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of high-frequency episodic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. 2015;14(11):1081–1090. doi:10.1016/S1474-4422(15)00249-5
10. Bigal ME, Dodick DW, Krymchantowski AV, et al. TEV-48125 for the preventive treatment of chronic migraine: efficacy at early time points. Neurology. 2016;87(1):41–48. doi:10.1212/WNL.0000000000002801
11. Cohen JM, Dodick DW, Yang R, et al. Fremanezumab as add-on treatment for patients treated with other migraine preventive medicines. Headache. 2017;57(9):1375–1384. doi:10.1111/head.13156
12. Halker Singh RB, Aycardi E, Bigal ME, Loupe PS, McDonald M, Dodick DW. Sustained reductions in migraine days, moderate-to-severe headache days and days with acute medication use for HFEM and CM patients taking fremanezumab: post-hoc analyses from phase 2 trials. Cephalalgia. 2019;39:52–60.
13. VanderPluym J, Dodick DW, Lipton RB, Ma Y, Loupe PS, Bigal ME. Fremanezumab for preventive treatment of migraine: functional status on headache-free days. Neurology. 2018;91(12):e1152–e65. doi:10.1212/01.wnl.0000544321.19316.40
14. Dodick DW, Silberstein SD, Bigal ME, et al. Effect of fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. Jama. 2018;319(19):1999–2008. doi:10.1001/jama.2018.4853
15. Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113–2122. doi:10.1056/NEJMoa1709038
16. Yeung PP, Spierings ELH, Blankenbiller T, et al. Efficacy of fremanezumab in patients with chronic migraine who had prior use of topiramate or onabotulinumtoxinA (P4.104). Neurology. 2018;90(15 Supplement):
17. Tepper SJ. Anti-Calcitonin Gene-Related Peptide (CGRP) therapies: update on a previous review after the American Headache Society 60th Scientific Meeting, San Francisco, June 2018. Headache. 2018;58 Suppl 3:276–290. doi:10.1111/head.13417
18. U.S. Food and Drug Administration. Drug approval package: Ajovy (fremanezumab-vfrm). Teva Pharmaceuticals USA, Inc.; 2018.
19. Bigal ME, Escandon R, Bronson M, et al. Safety and tolerability of LBR-101, a humanized monoclonal antibody that blocks the binding of CGRP to its receptor: Results of the Phase 1 program. Cephalalgia. 2014;34(7):483–492. doi:10.1177/0333102413517775
20. Bigal ME, Walter S, Bronson M, Alibhoy A, Escandon R. Cardiovascular and hemodynamic parameters in women following prolonged CGRP inhibition using LBR-101, a monoclonal antibody against CGRP. Cephalalgia. 2014;34(12):968–976. doi:10.1177/0333102414527646
21. Cohen-Barak O, Weiss S, Rasamoelisolo M, et al. A phase 1 study to assess the pharmacokinetics, safety, and tolerability of fremanezumab doses (225 mg, 675 mg and 900 mg) in Japanese and Caucasian healthy subjects. Cephalalgia. 2018;38(13):1960–1971. doi:10.1177/0333102418771376
22. VanderPluym J, Dodick D, Bigal M. Effect of CGRP Inhibition with TEV-48125 on cardiovascular parameters as a function of triptan use among individuals with chronic migraine (P2.205). Neurology. 2016;86(16 Supplement):
23. Depre C, Antalik L, Starling A, et al. A randomized, double-blind, Placebo-Controlled Study to evaluate the effect of erenumab on exercise time during a treadmill test in patients with stable angina. Headache. 2018;58(5):715–723. doi:10.1111/head.13316
24. Teva Pharmaceuticals USA, Inc. Ajovy (fremanezumab-vfrm) [package Insert]. North Wales, PA: Teva Pharmaceuticals USA Inc.; 2019.
25. Stevenson JC, Macdonald DW, Warren RC, Booker MW, Whitehead MI. Increased concentration of circulating calcitonin gene related peptide during normal human pregnancy. BMJ. 1986;293(6558):1329–1330. doi:10.1136/bmj.293.6558.1329
26. Saggese G, Bertelloni S, Baroncelli GI, Pelletti A, Benedetti U. Evaluation of a peptide family encoded by the calcitonin gene in selected healthy pregnant women. A longitudinal study. Horm Res. 1990;34(5–6):240–244.
27. Witzel SJ. Lactation and the use of biologic immunosuppressive medications. Breastfeeding Med. 2014;9(10):543–546. doi:10.1089/bfm.2014.0107
28. Hurley WL, Theil PK. Perspectives on immunoglobulins in colostrum and milk. Nutrients. 2011;3(4):442–474. doi:10.3390/nu3040442
29. Schebesch KM, Herbst A, Bele S, et al. Calcitonin-gene related peptide and cerebral vasospasm. J Clin Neurosci. 2013;20(4):584–586. doi:10.1016/j.jocn.2012.07.006
30. Peroutka SJ. Not all CGRP antagonists are created equal. Headache. 2013;53(6):1004–1006. doi:10.1111/head.12107
31. American Headache S. The American Headache Society position statement on integrating new migraine treatments into clinical practice. Headache. 2019;59(1):1–18.
32. Bigal ME, Edvinsson L, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of chronic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Nuerol. 2015;14(11):1091–1100.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.