")
Back to Journals » Cancer Management and Research » Volume 14
Free Ferrous Protoporphyrin and Reactive Oxygen Species Status of Voided Urine Predicts Higher Stage in Urothelial Carcinoma
Authors Zhao F , Qi N , Shen X, Xiong Z, Xue N , Xu Y, Wang J, Zhu H
Received 23 December 2021
Accepted for publication 3 February 2022
Published 15 February 2022 Volume 2022:14 Pages 615—621
DOI https://doi.org/10.2147/CMAR.S352127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Fangzheng Zhao,1 Nienie Qi,1 Xihao Shen,2 Zhuang Xiong,1 Ning Xue,1 Yang Xu,1 Junqi Wang,1 Haitao Zhu1
1Department of Urology, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China; 2The First Clinical Medical College of Nanjing Medical University, NanJing, People’s Republic of China
Correspondence: Junqi Wang; Haitao Zhu, Department of Urology, the Affiliated Hospital of Xuzhou Medical University, No. 99 Huaihai West Road, Quanshan District, Xuzhou, 221100, People’s Republic of China, Tel +86-18761389113, Fax +86051685609999, Email [email protected]; [email protected]
Purpose: This study was conducted to evaluate the correlation between the free ferrous protoporphyrin and reactive oxygen species (FH and ROS) combined test and the tumor grade and stage in a pathologically confirmed uroepithelial carcinoma (UC) patient population.
Patients and Methods: In this retrospective study, we enrolled patients newly diagnosed with UC between May 2020 and June 2021. All patients were classified as FH(+) and ROS(+), FH(+) and ROS(-), or FH(-) and ROS(-), based on the FH and ROS combined test of voided urine. Demographic information, pathological results, and status of the FH and ROS combined test were reviewed retrospectively. The relationship between FH and ROS combined test status and tumor stage and grade was evaluated using logistic regression.
Results: This study included 120 UC patients with a median age of 69 years (interquartile range [IQR] 62– 77 years). Eighteen patients (15%) were diagnosed with upper tract urothelial carcinoma, and the others (85%) were diagnosed with bladder cancer. The pathological stages for those with FH(+) and ROS(+) at diagnosis were 25.0% Ta, 45.8% T1, and 29.2% ≥T2. The pathological stages for those with FH(+) and ROS(-) at diagnosis were 23.5% Ta, 35.3% T1, and 41.2% ≥T2. The pathological stages for those with FH(-) and ROS(-) at diagnosis were 52.6% Ta, 26.3% T1, and 21.1% ≥T2. After adjusting for clinical factors, including age, sex, and smoking history, FH(+) and ROS(-) were independent risk factors for muscle-invasive UC (≥T2 stage) at diagnosis (odds ratio [OR] 3.379; 95% confidence interval [CI] 1.103– 10.355; P=0.033) in the univariate and multivariate logistic regression analyses.
Conclusion: Among patients with newly diagnosed UC, FH(+) and ROS(-) might have an association with a more advanced pathological stage. This finding may help differentiate between patients with aggressive diseases and those who may benefit from organ-sparing surgery.
Keywords: urothelial carcinoma, free ferrous protoporphyrin, reactive oxygen species, stage, grade
Introduction
Urothelial carcinomas (UCs) are the fourth most common type of tumors which can develop in the lower (bladder and urethra) or upper (pyelocaliceal cavities and ureter) urinary tract.1 Bladder cancer (BC) accounts for 90–95% of UCs.2 Compared to BC, upper tract urothelial carcinomas (UTUCs) are relatively rare, comprising 5–10% of UCs.3 UTUCs consist of renal pelvic carcinomas and ureteral carcinomas, with the former being approximately twice as common as the latter. Approximately 60% of the newly diagnosed UTUCs are muscle-invasive, whereas it is 15–25% for BC.4 Regardless of tumor location, radical nephroureterectomy (RNU) with bladder cuff excision is the current standard treatment for high-risk UTUCs.5 However, due to a post-surgery substantial decline in the estimated glomerular filtration rate, chronic kidney disease is prevalent.6,7 Hence, conservative management for small, non-invasive, and low-grade UTUCs may help preserve renal function in selected patients.8 A strict risk stratification should be performed for patients with UTUC. Similarly, radical cystectomy is currently considered the standard treatment for patients with muscle-invasive bladder cancer (MIBC). Compared to those diagnosed with a non-invasive disease, patients with MIBC were associated with higher mortality risk. However, for patients with BC, it is difficult for surgeons to identify the stage and grade of the tumor through urine cytology or preoperative imaging. To improve the survival of MIBC patients, earlier detection is required. Although cystoscopy and ureteroscopy are more sensitive and specific than urine cytology and radiography for diagnosing UTUC and BC, both are invasive procedures, and complications such as perforation and bleeding may occur during the examination. Recent studies indicated that patients with UTUC who underwent ureteroscopy before RNU were associated with significantly higher intravesical recurrence rates.7,9 Thus, a novel and more reliable method is required to identify low-and high-risk patients before surgery.
In China, researchers have developed free ferrous protoporphyrin and reactive oxygen species (FH and ROS) combined detection kits based on the characteristics of ROS and FH. It has been used as a new detection method for cervical cancer screening and diagnosis. A previous study confirmed that this method is highly sensitive and specific.10 In this study, we investigated the ability of FH and ROS to predict the tumor stage and grade of UCs.
Patients and Methods
In this single-center retrospective study, we enrolled patients with UCs diagnosed between May 2020 and June 2021. This study included 120 UC patients with a median age of 69 years (Interquartile range [IQR] 62–77 years). Informed consent was obtained from all the patients. Clinicopathological factors were gathered from the medical records (including age, sex, smoking history, and status of the FH and ROS combined test at initial diagnosis) to assess their influence on the tumor stage and grade. All procedures involving human participants in this study were performed following the ethical standards of the institutional and/or national research committee and complied with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the institutional review board of the Affiliated Hospital of Xuzhou Medical University.
Intracellular FH and ROS levels increased after the malignant transformation of urinary tract epithelial cells. The kit produced color changes by combining the dye solution with FH and ROS in the sample for a specific reaction, and the result was obtained through a colorimetric card. In this study, patients were divided into three groups according to the test results: FH(+) and ROS(+), FH(+) and ROS(-), and FH(-) and ROS(-). As the sensitivity of FH was higher than that of ROS, no patient presented with FH(-) and ROS(+). The original diagnoses of all pathological specimens were reexamined by a highly experienced urological pathologist. The tumor stage and grade were evaluated based on the UICC 2009 TNM classification of malignant tumors and the 2004 WHO classification grading system, respectively.
Statistical Analysis
The median (IQR) was used to evaluate continuous variables. Frequencies and proportions were categorized as categorical variables. Independent samples t-test and Kruskal–Wallis test were used to compare continuous variables. Categorical variables were evaluated using the χ2 test. Univariate and multivariate logistic regression analyses were used to examine the association between the variables and tumor stage or grade. The stages were divided into dichotomous variables according to the presence of muscle invasion (≥T2 vs T1+Ta). All reported P-values were two-sided. Statistical significance was set at P<0.05. SPSS version 26.0 (IBM Corporation, Armonk, NY, USA) was used for all statistical analyses.
Results
In this study, 120 patients diagnosed with UC were enrolled, of whom 90 were male and 30 were female. Their clinicopathological features are shown in Table 1. The median age was 69 years (IQR 62–77 years). Eighteen patients (15%) were diagnosed with UTUC, and 102 patients (85%) were diagnosed with BC. Eighty-four patients had non-muscle-invasive tumors (≤pT1) and 36 had muscle-invasive tumors (≥pT2), whereas 36 patients had low-grade tumors and 84 had high-grade tumors. FH(+) and ROS(+), FH(+) and ROS(-), and FH(-) and ROS(-) were present in 48 (40.0%), 34 (28.3%), and 38 patients (31.7%), respectively. The median body mass index was 24.3 (kg/m2) (IQR 23.1–26.3) (kg/m2). The median tumor size was 2.5 cm (IQR 1.6–4.0 cm). Most patients with UC had no smoking history. No significant difference was observed in the distribution of patients with a smoking history among the three groups (P=0.730).
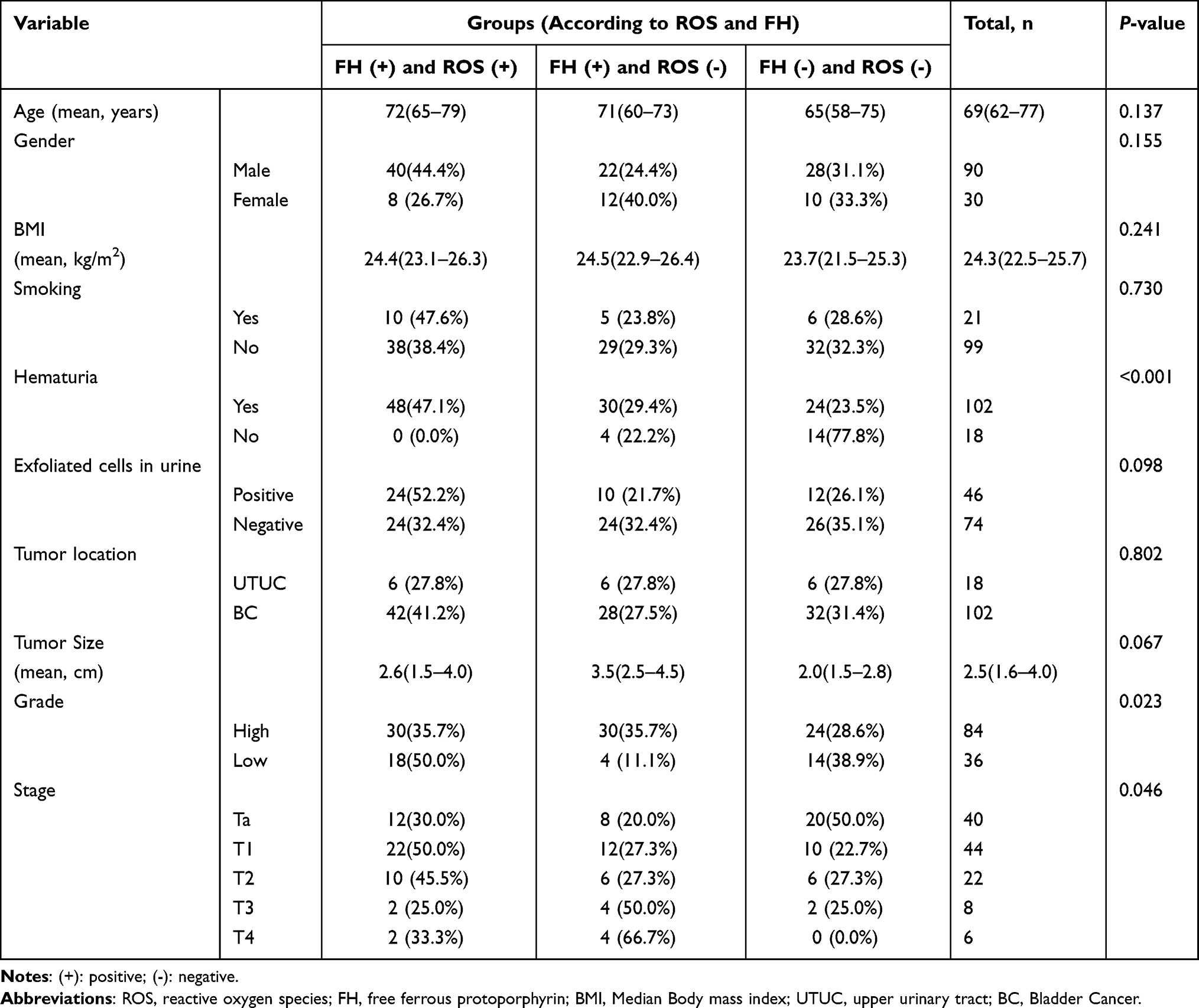 |
Table 1 Clinical and Pathological Characteristics of UC Patients According to the Type of FH and ROS |
The pathological stages for FH(+) and ROS(+) cases were ≤pT1 and ≥pT2 in 34 (70.8%) and 14 (29.2%) patients at diagnosis, respectively. For FH(+) and ROS(-) cases, 20 (58.8%) and 14 (41.2%) patients were diagnosed as stage ≤pT1 and ≥pT2, respectively, whereas for FH(-) and ROS(-) cases, 30 (78.9%) and 8 (21.2%) patients were diagnosed with stages ≤ pT1 and ≥pT2, respectively.
Multivariate logistic regression analyses demonstrated that FH(+) and ROS(-) were independent risk factors for muscle-invasive UCs (≥T2 disease) at diagnosis after adjustment for clinical parameters such as age, sex, and history of smoking (Odds ratio [OR] 3.379; 95% confidence interval [CI] 1.103–10.355; P=0.033, Table 2). A total of 62.5% patients with FH(+) and ROS(+), 88.2% with FH(-) and ROS(-), and 63.2% with FH(-) and ROS(-) presented with high-grade tumors. The status of the FH and ROS test did not correlate with the tumor grade.
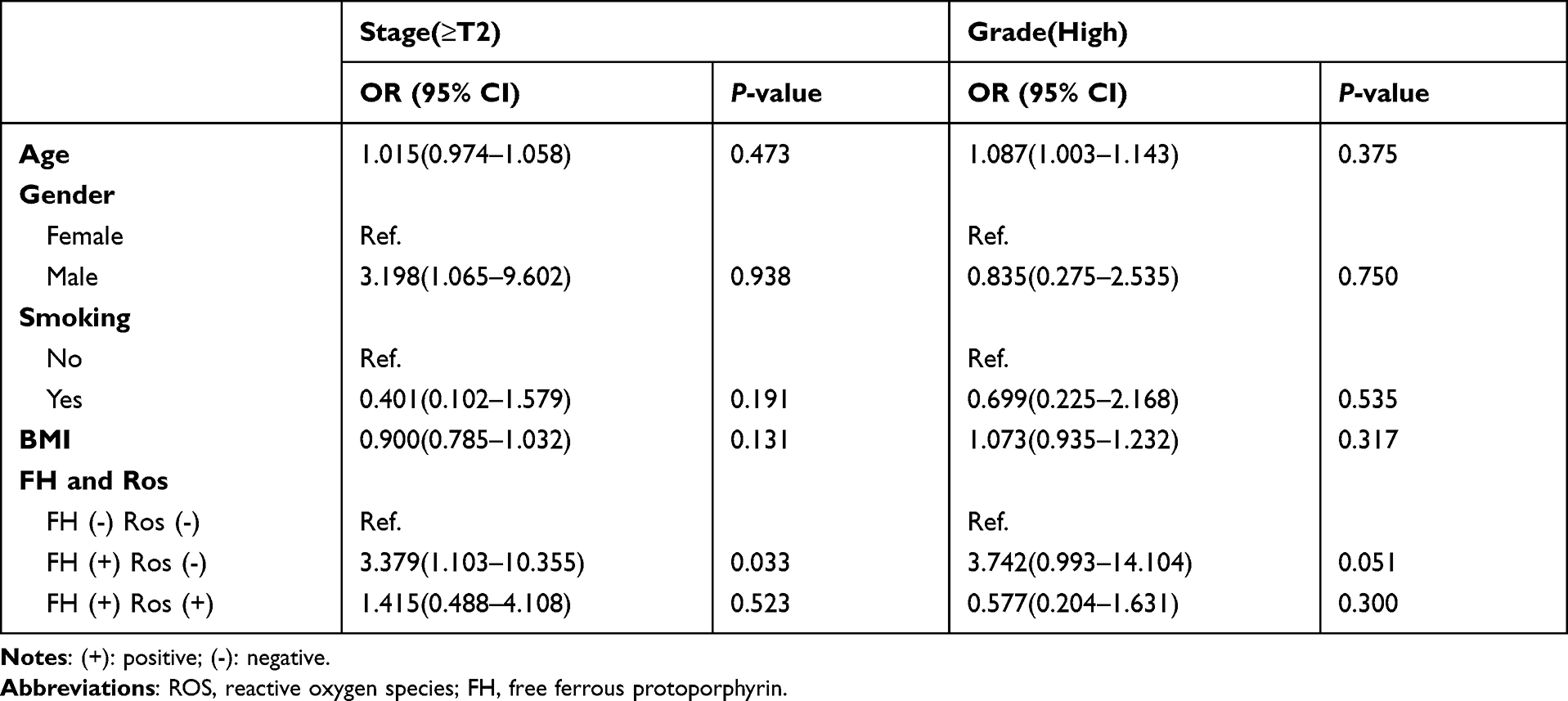 |
Table 2 Multivariate Logistic Regression Analysis of Factors Predicting High Grade or Stage (≥T2) |
After excluding patients with FH(-) and ROS(-), Table 3 shows the types of testing results (FH(+) and ROS(+) or FH(+) and ROS(-)) after stratification according to the pathological stage and grade. The positive predictive value (PPV) and negative predictive value (NPV) of FH(+) and ROS(-) for high-grade UCs were 88.2% and 37.5%, respectively. FH(+) and ROS(-) had a PPV of 41.2% and NPV of 70.8% for muscle-invasive UCs.
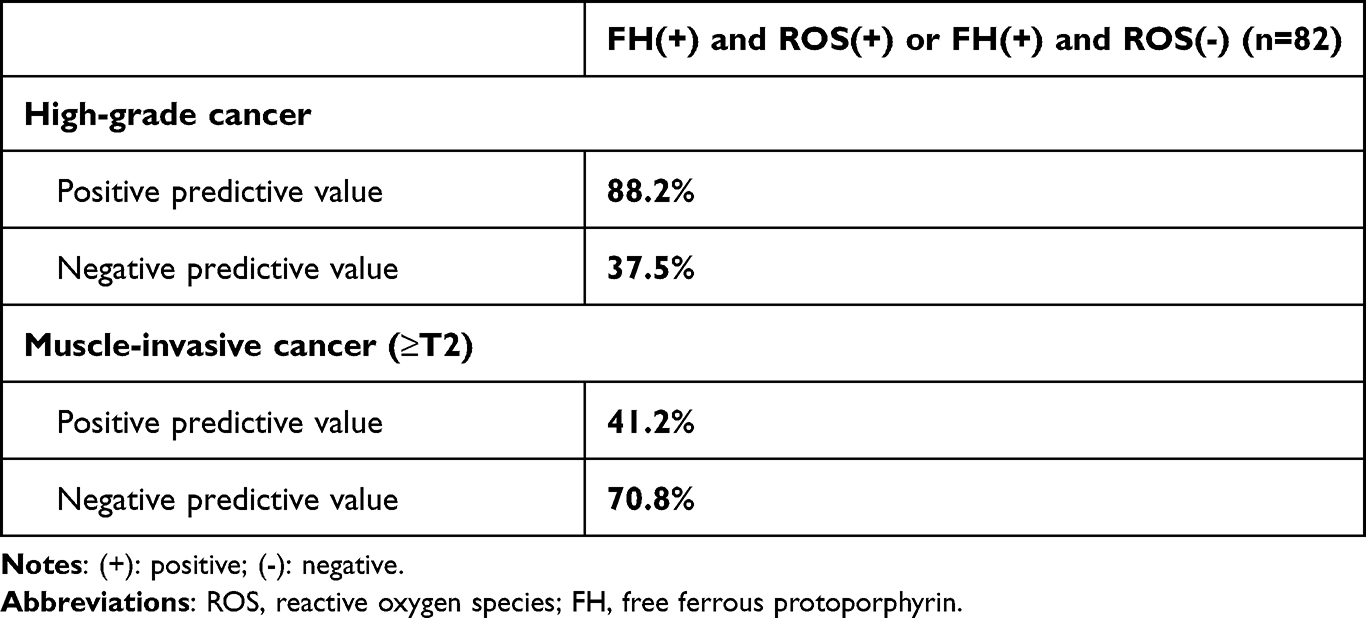 |
Table 3 Positive and Negative Predictive Values of FH (+) and Ros (-) for Predicting High-Grade and Muscle-Invasive UC |
Discussion
The management and survival of UCs are affected by the tumor stage. Patients diagnosed with muscle-invasive diseases have a significantly worse prognosis than those with non-muscle-invasive diseases.11 Therefore, urologists have a general consensus that surgery should be performed in UC patients at the earliest possible time after diagnosis.12 Research revealed that most patients with microscopic hematuria (MH) are not referred to a urologist for evaluation by undergoing imaging or cystoscopy.13–15 Delays in diagnosis of BC can lead to a worse prognosis due to a more advanced stage at diagnosis. In addition, previous studies have reported that among patients who underwent radical cystectomy (RC) for urothelial carcinoma of the urinary bladder (UCB), patients in the old-age (≥75–84 years) group had a better overall and cancer-specific survival than those in the oldest-age (≥85 years) group, highlighting the benefit that easier and earlier diagnosis through FH and ROS may benefit older patients by providing potentially curative therapy.16 The same problem also exists in UTUC. Furthermore, many RNUs are performed unnecessarily because of inaccurate preoperative staging of patients with UTUC. For patients with low-risk UTUC (described as unifocal, sizes <1 cm, low-grade, and no evidence of infiltrative lesions on computed tomography urography), conservative treatment can avoid complications related to radical surgery to a certain extent.8 Previous studies have suggested that for patients with localized renal cell carcinoma (T1-2N0M0), partial nephrectomy can reduce the risk of new-onset chronic kidney disease after surgery.17 Therefore, conservative management of small, non-invasive, and low-grade UTUCs might be useful in preserving renal function in low-risk patients.
The number and size of tumors can be easily determined using preoperative imaging. Nevertheless, it is challenging to precisely determine the stage and grade of UCs using currently available methods. In a multi-institutional study of 326 patients, Messer et al demonstrated that muscle invasiveness or high-grade malignant disease could not be precisely predicted using urine cytology alone in UTUC patients. Positive urine cytology had a PPV and sensitivity of 54% and 56%, and 44% and 62% for the high-grade UTUC and muscle-invasive UTUC, respectively.18 Although ureteroscopy is more sensitive and specific than urine cytology and radiography for diagnosing UTUC, it may not be as accurate in predicting the tumor stage. Straub et al reported that preoperative ureteroscopy was only 58% accurate in predicting the tumor grade in UTUC patients, and when urinary cytology was considered, the accuracy improved to only 68%.19 In addition, as an invasive procedure, ureteroscopy involves general anesthesia and entails concomitant surgical complications. A recent study demonstrated that the risk of postoperative intravesical recurrence was higher when ureteroscopy was conducted before RNU.20
There is an urgent need for a diagnostic tool or combined tools to effectively determine the stage and grade of UCs to clarify the diagnosis and specify a reasonable treatment plan. Formulated by the partial reduction of molecular oxygen, ROS is generally considered the by-product of cellular metabolism and oxygen consumption.21,22 Cancers have been associated with ROS due to its excessive production by various types of tumor cells compared to their normal counterparts.23 Increased ROS levels are considered oncogenic. FH exists widely in every cell, especially in the mitochondria. FH performs different physiological functions by binding with various types of proteins.24 FH is released from the protein of tumor cells under pathological conditions, including the destruction of gene expression regulation, abnormal DNA transcription, and changes in protein conformation, which leads to the loss of homeostasis through a series of electronic reactions, eventually resulting in cancer. As cell damage aggravates cell autolysis caused by the proteolytic enzymes, it leads to the exudation of FH substances. Based on these characteristics, Chinese researchers have developed ROS and FH combined detection kits. They are employed as a new detection method for cervical cancer screening and deliver good results. In this study, we examined the ability of the combined FH and ROS test to predict tumor staging and grading in UCs. Integrated with additional diagnostic techniques, the FH and ROS status may help distinguish between high-risk and low-risk UCs.
In this study, 68.3% of UC patients tested positive for FH or ROS. Among them, FH(+) and ROS(+), and FH(+) and ROS(-) accounted for 58.5% and 41.5%, respectively. FH(+) and ROS(-) had a PPV and NPV of 88.2% and 37.5% for high-grade UCs, respectively. FH(+) and ROS(-) had a PPV and NPV of 41.2% and 70.8% for muscle-invasive UCs, respectively. FH(+) and ROS(-) were independent risk factors for advanced UCs. With a higher accuracy in predicting advanced characteristics, the FH and ROS test may help surgeons choose a better treatment.
Some studies observed that routine laboratory parameters and diagnostics may aid in detecting the tumor stage and outcomes. Su et al retrospectively evaluated the diagnostic accuracy for detecting aggressive UTUC using fluorescence in situ hybridization (FISH). They discovered that FISH had an overall sensitivity of 62.4% for detecting aggressive UTUC.7 Therefore, positive results of voided urine FISH may suggest advanced UTUC. Qi et al reported that in newly diagnosed UTUC patients, a lower pathological stage can be predicted accurately by observing the microscopic hematuria at the onset. Detecting the disease before the presence of GH may affect therapeutic decisions and survival. The type of hematuria did not affect the tumor grade.25 Similarly, Ramirez et al assessed the association between hematuria and the grade and stage of BC. They noted that gross hematuria was related to more advanced pathological stages. The type of hematuria did not affect the tumor grade.26 Tamalunas et al observed elevated preoperative C-reactive protein (CRP) levels and decreased hemoglobin levels as independent prognostic factors, indicating an unfavorable outcome in patients undergoing RC for UCB. They also believed that the primary tumor stage, the presence of regional lymph node and distant metastases were also significantly associated with CRP and hemoglobin levels in UCB patients.27
In interpreting the results, a few disadvantages of this study should be considered. First, this retrospective study encountered a few unavoidable data losses during the collection process. Second, the sample size was relatively small, with only 120 patients. Among them, there were only 18 patients with UTUC. Finally, as the sensitivity of ROS is weaker than that of FH, no patient presented with FH(-) and ROS(+). Our results are preliminary and require further validation in larger populations.
Conclusion
This is the first study to assess the relationship between FH and ROS status and the stage and grade of UCs. Our results suggested that FH(+) and ROS(-) at diagnosis predict a higher pathological stage in patients with UC. The status of the FH and ROS test was not associated with the tumor grade. The FH and ROS combined test may help guide treatment decisions for patients with UC.
Acknowledgments
This work was supported by the Xuzhou Medical Leading Talents Training Project (XWRCHT20210027).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. doi:10.3322/caac.21551
2. Babjuk M, Bohle A, Burger M, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol. 2017;71:447–461. doi:10.1016/j.eururo.2016.05.041
3. Munoz JJ, Ellison LM. Upper tract urothelial neoplasms: incidence and survival during the last 2 decades. J Urol. 2000;164(5):1523–1525. doi:10.1016/S0022-5347(05)67019-X
4. Margulis V, Shariat SF, Matin SF, et al. Outcomes of radical nephroureterectomy: a series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer. 2009;115(6):1224–1233. doi:10.1002/cncr.24135
5. Rouprêt M, Babjuk M, Burger M, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2020 update. Eur Urol. 2021;79(1):62–79. doi:10.1016/j.eururo.2020.05.042
6. Lane BR, Smith AK, Larson BT, et al. Chronic kidney disease after nephroureterectomy for upper tract urothelial carcinoma and implications for the administration of perioperative chemotherapy. Cancer. 2010;116(12):2967–2973. doi:10.1002/cncr.25043
7. Su X, Han H, Li X, et al. Fluorescence in situ hybridization status of voided urine predicts invasive and high-grade upper tract urothelial carcinoma. Oncotarget. 2017;8(16):26106–26111. doi:10.18632/oncotarget.15344
8. Rouprêt M, Babjuk M, Compérat E, et al. European Association of Urology guidelines on upper urinary tract urothelial cell carcinoma: 2015 update. Eur Urol. 2015;68(5):868–879. doi:10.1016/j.eururo.2015.06.044
9. Liu Z, Zheng S, Li X, et al. Oncologic outcomes of patients undergoing diagnostic ureteroscopy before radical nephroureterectomy for upper urinary tract urothelial carcinomas: a systematic review and meta-analysis. J Laparoendosc Adv Surg Tech A. 2018;28:1316–1325. doi:10.1089/lap.2018.0015
10. You M, Li H, Gao Y, et al. Clinical application value of FH/ROS combined test in cervical cancer screening. Hans J Biomed. 2019;9(4):5. doi:10.12677/HJBM.2019.94022
11. Mbeutcha A, Rouprêt M, Kamat AM, et al. Prognostic factors and predictive tools for upper tract urothelial carcinoma: a systematic review. World J Urol. 2017;35(3):337–353. doi:10.1007/s00345-016-1826-2
12. Bourgade V, Drouin SJ, Yates DR, et al. Impact of the length of time between diagnosis and surgical removal of urologic neoplasms on survival. World J Urol. 2014;32(2):475–479. doi:10.1007/s00345-013-1045-z
13. Buteau A, Seideman CA, Svatek RS. What is evaluation of hematuria by primary care physicians? Use of electronic medical records to assess practice patterns with intermediate follow-up. Urol Oncol. 2014;32(2):128–134. doi:10.1016/j.urolonc.2012.07.001
14. Nieder AM, Lotan Y, Nuss GR, et al. Are patients with hematuria appropriately referred to urology? A multi-institutional questionnaire based survey. Urol Oncol Semin Original Investig. 2010;28(5):500–503. doi:10.1016/j.urolonc.2008.10.018
15. Johnson EK, Daignault S, Zhang Y, et al. Patterns of hematuria referral to urologists: does a gender disparity exist? Urology. 2008;72(3):
16. Tamalunas A, Volz Y, Schlenker BA, et al. Is it safe to offer radical cystectomy to patients above 85 years of age? A long-term follow-up in a single-center institution. Urol Int. 2020;104(11–12):975–981. doi:10.1159/000510137
17. Wang Z, Wang G, Xia Q, et al. Partial nephrectomy vs. radical nephrectomy for renal tumors: a meta-analysis of renal function and cardiovascular outcomes. Urol Oncol. 2016;34(12):
18. Messer J, Shariat SF, Brien JC, et al. Urinary cytology has a poor performance for predicting invasive or high-grade upper-tract urothelial carcinoma. BJU Int. 2011;108:701–705. doi:10.1111/j.1464-410X.2010.09899.x
19. Straub J, Strittmatter F, Karl A, Stief CG, Tritschler S. Ureterorenoscopic biopsy and urinary cytology according to the 2004 WHO classification underestimate tumor grading in upper urinary tract urothelial carcinoma. Urol Oncol. 2013;31(7):1166–1170. doi:10.1016/j.urolonc.2011.12.021
20. Guo RQ, Hong P, Xiong GY, et al. Impact of ureteroscopy before radical nephroureterectomy for upper tract urothelial carcinomas on oncological outcomes: a meta-analysis. BJU Int. 2018;121(2):184–193. doi:10.1111/bju.14053
21. Giorgio M, Trinei M, Migliaccio E, Pelicci PG. Hydrogen peroxide: a metabolic by-product or a common mediator of ageing signals? Nat Rev Mol Cell Biol. 2007;8(9):722–728. doi:10.1038/nrm2240
22. Zorov DB, Juhaszova M, Sollott SJ. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol Rev. 2014;94(3):909–950. doi:10.1152/physrev.00026.2013
23. Panieri E, Santoro MM. ROS homeostasis and metabolism: a dangerous Liason in cancer cells. Cell Death Dis. 2016;7:e2253. doi:10.1038/cddis.2016.105
24. O’Quinn RL, Fishbein M. Isolation, characterization and cross-species amplification of polymorphic microsatellite loci in Asclepias (Apocynaceae). Conservat Genet. 2009;10(5):1437–1440. doi:10.1007/s10592-008-9755-2
25. Qi N, Zhang J, Chen Y, Wen R, Li H. Microscopic hematuria predicts lower stage in patients with upper tract urothelial carcinoma. Cancer Manag Res. 2018;10:4929–4933. doi:10.2147/CMAR.S180606
26. Ramirez D, Gupta A, Canter D, et al. Microscopic haematuria at time of diagnosis is associated with lower disease stage in patients with newly diagnosed bladder cancer. BJU Int. 2016;117(5):783–786. doi:10.1111/bju.13345
27. Tamalunas A, Buchner A, Kretschmer A, et al. Impact of routine laboratory parameters in patients undergoing radical cystectomy for urothelial carcinoma of the bladder: a long-term follow-up. Urol Int. 2020;104(7–8):551–558. doi:10.1159/000506263
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.