")
Back to Journals » Drug Design, Development and Therapy » Volume 10
Fondaparinux vs warfarin for the treatment of unsuspected pulmonary embolism in cancer patients
Authors Amato B, Compagna R, Rocca A, Bianco T, Milone M, Sivero L, Vigliotti G, Amato M, Danzi M, Aprea G, GALLELLI L , de Franciscis S, Serra R
Received 10 February 2016
Accepted for publication 6 April 2016
Published 23 June 2016 Volume 2016:10 Pages 2041—2046
DOI https://doi.org/10.2147/DDDT.S106153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Wei Duan
Bruno Amato,1,2,* Rita Compagna,1,2,* Aldo Rocca,2 Tommaso Bianco,2 Marco Milone,2 Luigi Sivero,2 Gabriele Vigliotti,2 Maurizio Amato,2 Michele Danzi,2 Giovanni Aprea,2 Luca Gallelli,3,* Stefano de Franciscis,1,4,* Raffaele Serra1,4,*
1Interuniversity Center of Phlebolymphology, International Research and Educational Program in Clinical and Experimental Biotechnology, University Magna Graecia of Catanzaro, Viale Europa, Catanzaro, 2Department of Clinical Medicine and Surgery, University of Naples “Federico II”, Naples, 3Department of Health Sciences, 4Department of Medical and Surgical Sciences, University of Catanzaro, Catanzaro, Italy
*These authors contributed equally to this work
Introduction: In cancer patients, the chest computer tomography (CT) can be used to identify asymptomatic pulmonary embolism (APE). In most cases, these patients are treated with anticoagulant drugs for at least 3 months. The American College of Physicians recommend treatment of these patients as patients with symptomatic pulmonary embolism. In this study, we evaluated and compared the efficacy and safety of fondaparinux vs warfarin in the prevention of unsuspected pulmonary embolism in patients with active cancer.
Materials and methods: A prospective and parallel group study was performed on 64 cancer patients (29 males and 35 females) with APE. A multidetector CT angiography with high spatial and temporal resolution and quality of arterial opacification was used to make the diagnosis. Lung scintigraphy was reserved to selected patients only. Patients were randomized to either the warfarin (Group A) or the fondaparinux (Group B) for 90 days. The first end point of efficacy was the persistence, reduction, or disappearance of thrombosis after 90 days. The second end point was the reappearance of thrombosis after 1 year. The first end point of safety was the development of major bleeding.
Results: We enrolled 32 patients into each treatment group. We reached the first end point of efficacy and safety in Group B which showed that fondaparinux was able to induce the disappearance of thrombotic pulmonary with a lower incidence of major bleeding events compared with warfarin. No difference in the secondary end point was recorded.
Conclusion: We suggest that the treatment of cancer patients with APE can be oriented with the administration of a standard dose of fondaparinux until the next CT lung control (3 months). However, the lack of a randomized clinical trial, including a larger patient cohort, does not allow formulation of final recommendations in these patients. A broader study would be desirable, involving a larger number of patients and a longer follow-up period.
Keywords: cancer patients, asymptomatic pulmonary embolism, fondaparinux, warfarin
A Letter to the Editor has been received and published for this article.
Introduction
Cancer patients showed an increased risk of pulmonary embolism (PE) compared with the general population.1,2 These patients are subject, during the follow-ups, to imaging studies, including total body computer tomography (CT) with contrast and positron emission tomography–CT, to assess the extent of the malignancy and the response to the treatment. In these patients, the detection of unsuspected pulmonary embolism (UPE) related to asymptomatic pulmonary embolism (APE) has become increasingly common,3,4 with an increase in health cost.5,6
In most cases, these patients are treated with anticoagulant drugs (eg, warfarin) for at least 3 months, since the American College of Chest Physicians recommends to consider these patients as patients with symptomatic PE.7
Warfarin is commonly used prophylactically in patients with a high risk of thromboembolic events. However, it has several potential adverse effects (eg, bleeding) and drug interactions;8 therefore, it requires frequent monitoring and dose adjustments with a negative impact on the quality of life.9
In contrast, low-molecular-weight heparins (LMWHs) have a predictable pharmacokinetic profile, few drug interactions, and good safety.10 Fondaparinux, a synthesized pentasaccharide with antifactor Xa activity, is the newest agent with venous thromboembolism (VTE) prophylaxis activity.11
Here, we evaluated the efficacy and safety of fondaparinux vs warfarin in the prevention of UPE in patients with active cancer.
Materials and methods
Study design
A randomized, prospective, single-blind, and parallel group study was performed in the Department of Clinical Medicine and Surgery, “Federico II” University of Naples, between March 2013 and June 2015. The single-blind study was chosen in place of the double-blind due to the different methods of administration (eg, warfarin orally and fondaparinux subcutaneously). In order to exclude any risk for the patients, the physicians who evaluated the patients knew the protocol and the group that was being treated, whereas physicians who evaluated the data were not aware of the treatment.
The study was conducted according to the ethical principles of the Declaration of Helsinki, and the protocol was approved by the institutional review board – Independent Ethics Committee of Interuniversity Center of Phlebolymphology (CIFL). International Research and Educational Program in Clinical and Experimental Biotechnology with the following approval number: ER.NA.2013.34. Before beginning the study, all participants signed the written informed consent.
Patients
We enrolled 64 patients (29 males and 35 females) of both sexes who were diagnosed with active primary cancer and were in anticancer treatment, with occasional finding of APE (Table 1).
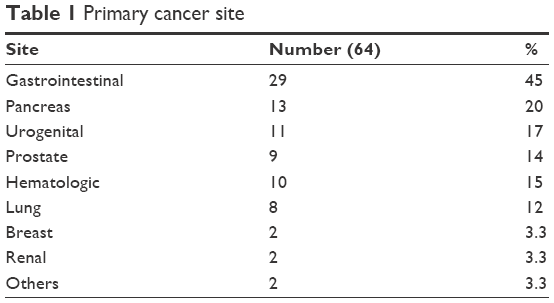 | Table 1 Primary cancer site |
Exclusion criteria consisted of the following: history of heart failure or stroke, drug allergies, psychiatric diseases, creatinine clearance <30 mL/min, or platelet count <100,000/mm3. Patients treated with dextran, thrombolytic agents, anticoagulants, or heparin or heparinoids for topical use were also excluded.
APE characteristic
APE was documented most commonly using chest CT during the follow-up for restaging after therapy (34 patients, 53%) and during the baseline cancer staging (21 patients, 33%), whereas in nine patients (14%) it was documented for the assessment of extrathoracic diseases.
Moreover, the CT scan detected thrombi in all tracts of the pulmonary artery (Table 2).
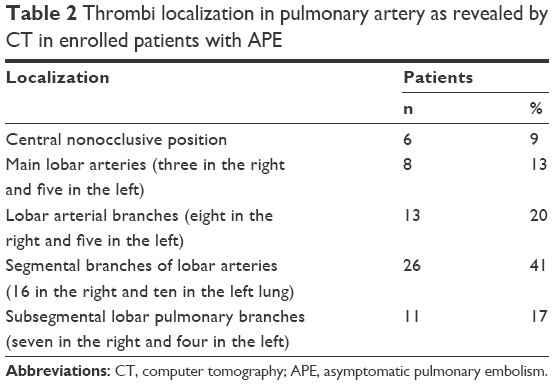 | Table 2 Thrombi localization in pulmonary artery as revealed by CT in enrolled patients with APE |
Experimental protocol
Patients with primary active cancer regardless of age, sex, or medical history were randomized to receive either warfarin (Coumadin®; dose-adjusted to achieve an international normalized ratio of 2.0–3.0) or fondaparinux (Arixtra®, 7.5 mg subcutaneously) once daily for 90 days (T1). The randomization was performed in agreement with our previous studies.12–16
We used a computer program to generate a sequence of treatment allocations by block randomization using a random number generator. Investigators were not aware of the block size to avoid selection bias.
At the time of admission (T0) and during the follow-ups (90 days = T1, end of the treatment; 1 year = T2, end of the observation), the patients underwent clinical evaluation, chemical blood findings (complete blood count with platelet count, activated partial thromboplastin time, and erythrocyte sedimentation rate), urine analysis, and a chest X-ray. Moreover, at the same time (T0–T2) in agreement with 2014 ESC guidelines, we used the multidetector CT (MDCT) angiography to determine the presence of UPE.
All the MDCT angiography examinations were performed with a 64-slice scanner MDCT (Toshiba Aquilion, Tokyo, Japan) using 50–70 mL of 350 mg nonionic iso-osmolar contrast (fonexal and omnipaque). A hypodense intraluminal filling defect causing partial or total obliteration of vascular lumen in segmental and subsegmental arteries with or without corresponding increase in the diameter of the affected vessel was taken as a positive result for PE on MDCT. Considering the high diagnostic power of this scan, lung scintigraphy was performed only in patients with contraindications to CT scanning (eg, critically ill patients or patients with multiorgan dysfunction) or with diagnostic doubts.
Clinical and safety assessment
During the follow-ups (T1 and T2), the persistence, reduction, or disappearance of the thrombotic pulmonary findings was evaluated.
The safety of the study medications was assessed by monitoring for any adverse drug reactions for severity and causality. The relationship between adverse drug reactions and drug treatment was evaluated using the Naranjo adverse probability scale in agreement with our previous studies.17–19 The bleeding related to the treatments was evaluated as previously described.20
Efficacy end points
The primary end point was defined as a statistically significant difference (P<0.01) in the thrombotic pulmonary CT findings between the two groups of treatment. The secondary end point was the recurrence/appearance of thrombotic events in other sites during the follow-ups (T1 and T2).
Safety end points
The primary end point was defined as a statistically significant difference (P<0.01) in the development of major bleeding between the two groups. Major bleeding was defined as hemorrhage occurring at a critical site (eg, intracranial hemorrhage), resulting in a major therapeutic intervention (eg, surgery), causing hemodynamic compromise, requiring at least one unit of red cell concentrates or resulting in death. Minor bleeding was defined as bleeding that did not fulfill the criteria for major bleeding. The secondary safety end point was the difference in overall mortality.
Statistical analysis
All data are expressed as mean ± standard deviation. The study analysis was based upon the intention to treat, therefore, all consented patients were included in the analysis. Data were checked for normality using the Kolmogorov–Smirnov test. The Student’s t-test and the χ2 test were used when appropriate to test the significance of the differences. The analysis of variance was used to evaluate the differences between multiple means. Once we determined that differences existed, a Bonferroni test was used to determine which means differed. The threshold of statistical significance was set at P<0.05. SPSS software Version 21 (IBM Corporation, Armonk, NY, USA) was used for statistical analyses.
Results
Patients
After a detailed clinical history and radiological examination, 64 patients (29 males and 35 females) were recruited and randomized into two groups:
Group A: 32 patients (13 males and 19 females) were treated with warfarin.
Group B: 32 patients (16 males and 16 females) were treated with fondaparinux.
All patients successfully completed the protocol, and all patients underwent follow-ups.
Efficacy outcomes
All the drugs were efficacious in the treatment of PE, even if the primary efficacy outcome was statistically significant (P<0.01) in Group B. In particular, persistence of thrombus occurred 14 times in Group A and four times in Group B; a reduction in thrombus was found in eight patients treated with warfarin (Group A) and in 12 treated with fondaparinux (Group B); and a complete disappearance of CT findings occurred in eleven Group A patients and in 16 Group B patients (Table 3).
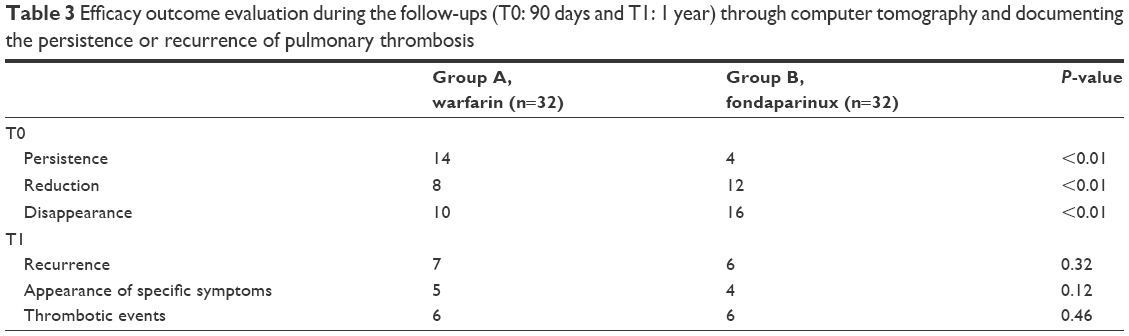 | Table 3 Efficacy outcome evaluation during the follow-ups (T0: 90 days and T1: 1 year) through computer tomography and documenting the persistence or recurrence of pulmonary thrombosis |
We did not find statistically significant differences in recurrence (Group A: 7; Group B: 6; P=0.32), appearance of symptoms (Group A: 5; Group B: 4; P=0.12), and thrombotic events in other locations (Group A: 6; Group B: 6; P=0.46; Table 3).
Safety outcomes
Patients treated with fondaparinux experienced a lower incidence of major bleeding (n=3) compared with patients treated with warfarin (n=6; P<0.01) and we did not find statistically significant differences in minor bleeding (Group A: 5; Group B: 4; P=0.12) and in overall mortality (Group A: 4; Group B: 3; P=0.47; Table 4).
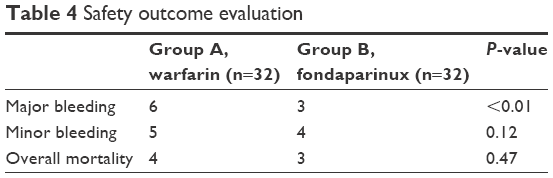 | Table 4 Safety outcome evaluation |
Discussion
In this study, we evaluated the effects of fondaparinux and of warfarin in the treatment of APE in cancer patients. A previous study documented that LMWH reduce the recurrent VTE in patients with active cancer in a similar manner to warfarin, but with low bleeding.21 Moreover, the Comparison of Low Molecular Weight Heparin Versus Oral Anticoagulant Therapy for Long Term Anticoagulation in Cancer Patients With Venous Thromboembolism (CLOT) study showed that dalteparin is the most effective therapy vs vitamin K antagonists (VKAs), and the current guidelines recommend the treatment with dalteparin, enoxaparin, or tinzaparin in cancer patients with symptomatic VTE.22 Unfortunately, these recommendations are based on a single study, and the patients enrolled in the CLOT study came mostly from North America and do not represent the global population.
The lack of diversity and the other bias in the CLOT study partly explain why the VKAs are still widely used in several countries in patients with thrombosis associated with cancer. A multinational, Phase III, open-label, randomized, controlled trial documented the efficacy and safety of long-term tinzaparin vs warfarin for the treatment of acute VTE in cancer patients.21 However, more recently Lee et al,23 in a randomized, open-label, multicenter study performed in patients with active cancer and acute symptomatic VTE, documented that the use of a daily full-dose tinzaparin (175 IU/kg) compared with warfarin for 6 months did not significantly reduce the composite measure of recurrent VTE and was not associated with reductions in overall mortality or major bleeding.
In our study, we documented that fondaparinux induced a significant decrease in the development of thrombosis in cancer patients. In our study, the overall mortality in the two groups was comparable and in our opinion acceptable, considering the disease. There was no difference between the two groups in the long-term outcome (1-year follow-up), but a better response in the primary efficacy outcome was found in patients treated with fondaparinux. Baseline characteristics between either groups (fondaparinux and warfarin) were not statistically significant, therefore, we can conclude that these could play a role in the difference in response to the drugs.
Moreover, it is widely known that several factors (genetic, food, and drugs) are able to modify clinical efficacy of warfarin. However, to date the clinical efficacy is reported for value of international normalized ratio between 2.0 and 3.0. In our study, chemical blood evaluation documented that international normalized ratio was in a normal range in all patients throughout the study.
Cho et al24 reported a patient with metastatic breast cancer, mobile right atrial thrombus, and PE who developed thrombocytopenia after heparin and warfarin treatment. Thrombocytopenia may represent a side effect during the treatment with heparin,25,26 and several authors have reported that fondaparinux can be used in patients who developed thrombocytopenia during heparin treatment.12,27,28
Shetty et al,29 in a single-arm observational cohort study of fondaparinux in 30 patients with intolerance to VKA therapy (16 had a history of recurrent VTE, eleven had idiopathic VTE, and three had cancer), did not record episodes of recurrent VTE or major bleeding.
Moreover, Pesavento et al,30 reviewing the experience of the RIETE investigators with subacute fondaparinux therapy for VTE (47,378 patients enrolled in the RIETE study, 263 treated for at least 3 months with fondaparinux, and 78 of these patients had cancer), documented that there was no difference in recurrent PE in patients taking fondaparinux and VKA or LMWH. Moreover, they also documented that major bleeding was similar between cancer patients taking fondaparinux and LMWH.
In agreement with these authors, in our study we did not record the development of thrombocytopenia, whereas we recorded a lower incidence of major bleeding in patients treated with fondaparinux compared with those treated with warfarin, without significant difference in minor bleeding.
Conclusion
Our data suggest that a standard dose of fondaparinux may be used in cancer patients with APE until the next CT lung control (3 months). However, the lack of randomized clinical trials that include a larger patient cohort does not allow formulation of final recommendations in these patients, but it is desirable to carry out a broader study, with the involvement of a larger number of patients and a longer follow-up.
Acknowledgments
BA and RC share the first authorship. LG, SdF, and RS share the senior authorship. The author Dr MA is the son of the author Prof BA. This work received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245–1248. | ||
Monreal M, Falgá C, Valdés M, et al. Fatal pulmonary embolism and fatal bleeding in cancer patients with venous thromboembolism: findings from the RIETE registry. J Thromb Haemost. 2006;4(9):1950–1956. | ||
Douma RA, Kok MG, Verberne LM, Kamphuisen PW, Büller HR. Incidental venous thromboembolism in cancer patients: prevalence and consequence. Thromb Res. 2010;125(6):e306–e309. | ||
Dentali F, Ageno W, Becattini C, et al. Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: a meta-analysis. Thromb Res. 2010;125(6):518–522. | ||
Boswell WD, Pierce J, Fahimi A, Parisky Y, Sheth P. Incidental pulmonary emboli detected by multi-detector row spiral CT in cancer patients. Cancer Imaging. 2005;5:25–26. | ||
Browne AM, Cronin CG, English C, NiMhuircheartaigh J, Murphy JM, Bruzzi JF. Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thorac Oncol. 2010;5(6):798–803. | ||
Kearon C, Akl EA, Comerota AJ, et al; American College of Chest Physicians. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(suppl 2):e419S–e494S. | ||
Palleria C, Di Paolo A, Giofrè C, et al. Pharmacokinetic drug-drug interaction and their implication in clinical management. J Res Med Sci. 2013;18(7):601–610. | ||
Noble SI, Finlay IG. Is long-term low-molecular-weight heparin acceptable to palliative care patients in the treatment of cancer related venous thromboembolism? A qualitative study. Palliat Med. 2005;19(3):197–201. | ||
Weitz JI. Low-molecular-weight heparins. N Engl J Med. 1997;337(10):688–698. | ||
Leporini C, Rende A, Sorrentino A, et al. Efficacy and safety of off-label use of fondaparinux in the management of heparin-induced thrombocytopenia with thrombosis in an elderly woman. J Clin Pharmacol. 2013;53(9):999–1002. | ||
Gallelli L, Colosimo M, Tolotta GA, et al. Prospective randomized double-blind trial of racecadotril compared with loperamide in elderly people with gastroenteritis living in nursing homes. Eur J Clin Pharmacol. 2010;66(2):137–144. | ||
Serra R, Gallelli L, Buffone G, et al. Doxycycline speeds up healing of chronic venous ulcers. Int Wound J. 2015;12(2):179–184. | ||
deFranciscis S, Gallelli L, Battaglia L, et al. Cilostazol prevents foot ulcers in diabetic patients with peripheral vascular disease. Int Wound J. 2015;12(3):250–253. | ||
Serra R, Gallelli L, Conti A, et al. The effects of sulodexide on both clinical and molecular parameters in patients with mixed arterial and venous ulcers of lower limbs. Drug Des Devel Ther. 2014;8:519–527. | ||
Amato B, Compagna R, Amato M, Gallelli L, de Franciscis S, Serra R. Aterofisiol® in carotid plaque evolution. Drug Des Devel Ther. 2015;9:3877–3884. | ||
Gallelli L, Ferreri G, Colosimo M, et al. Retrospective analysis of adverse drug reactions to bronchodilators observed in two pulmonary divisions of Catanzaro, Italy. Pharmacol Res. 2003;47(6):493–499. | ||
Gallelli L, Ferreri G, Colosimo M, et al. Adverse drug reactions to antibiotics observed in two pulmonology divisions of Catanzaro, Italy: a six-year retrospective study. Pharmacol Res. 2002;46(5):395–400. | ||
Gallelli L, Staltari O, Palleria C, De Sarro G, Ferraro M. Hepatotoxicity induced by methimazole in a previously healthy patient. Curr Drug Saf. 2009;4(3):204–206. | ||
Gallelli L, Galasso O, Falcone D, et al. The effects of nonsteroidal anti-inflammatory drugs on clinical outcomes, synovial fluid cytokine concentration and signal transduction pathways in knee osteoarthritis. A randomized open label trial. Osteoarthritis Cartilage. 2013;21(9):1400–1408. | ||
Lee AY, Bauersachs R, Janas MS, et al; CATCH Investigators. CATCH: a randomized clinical trial comparing long-term tinzaparin versus warfarin for treatment of acute venous thromboembolism in cancer patients. BMC Cancer. 2013;13:284. | ||
Lee AY, Levine MN, Baker RI. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003;349(2):146–153. | ||
Lee AY, Kamphuisen PW, Meyer G, et al; CATCH Investigators. Tinzaparin vs warfarin for treatment of acute venous thromboembolism in patients with active cancer: a randomized clinical trial. JAMA. 2015;314(7):677–686. | ||
Cho YK, Park BW, Lee MH, Hyon MS, Bang DW, Kim YJ. Fatal massive and recurring pulmonary embolism followed by thrombocytopenia developed after heparin and warfarin treatment in a patient with metastatic breast cancer with an incidental large right atrialthrombus. Blood Coagul Fibrinolysis. 2016;27(2):213–215. | ||
Warkentin TE. Heparin-induced thrombocytopenia. Curr Opin Crit Care. 2015;21(6):576–585. | ||
Tutwiler V, Madeeva D, Ahn HS, et al. Platelet transactivation by monocytes promotes the prothromboticstate in heparin-induced thrombocytopenia. Blood. 2016;127(4):464–472. | ||
Wei M, Wang CT, Li DM, Song XJ. Prolonged use of fondaparinux for perioperative bridging: a case report of a patient with mechanical heart valve and heparin-induced thrombocytopenia. J Clin Pharm Ther. 2015;40(6):702–705. | ||
Chaudhary RK, Nepal C, Khanal N, Pathak R, Giri S, Bhatt VR. Management and outcome of heparin-induced thrombocytopenia in pregnancy: a systematic review. Cardiovasc Hematol Agents Med Chem. 2015;13(2):92–97. | ||
Shetty R, Seddighzadeh A, Parasuraman S, Vallurupalli NG, Gerhard-Herman M, Goldhaber SZ. Once-daily fondaparinux monotherapy without warfarin for long-term treatment of venous thromboembolism. Thromb Haemost. 2007;98(6):1384–1386. | ||
Pesavento R, Amitrano M, Trujillo-Santos J, et al; RIETE Investigators. Fondaparinux in the initial and long-term treatment of venous thromboembolism. Thromb Res. 2015;135(2):311–317. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.