")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 11
Focus on the use of antidepressants to treat pediatric functional abdominal pain: current perspectives
Received 18 April 2018
Accepted for publication 28 July 2018
Published 28 September 2018 Volume 2018:11 Pages 365—372
DOI https://doi.org/10.2147/CEG.S146646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Silvana Bonilla, Samuel Nurko
Division of Pediatric Gastroenterology, Hepatology and Nutrition, Boston Children’s Hospital. Boston, MA, USA
Abstract: Chronic abdominal pain is frequently encountered in pediatric practice. A large proportion of cases meet Rome criteria for abdominal pain-functional gastrointestinal disorders (AP-FGIDs). These disorders are costly and, in some cases, lead to impairment of daily functioning and overall quality of life. Pathophysiologic mechanisms include early stressful events, visceral hypersensitivity, dysmotility, changes in intestinal microbiota, and altered central nervous system processing. They are considered disorders of the brain–gut interaction. The diagnosis is made on clinical grounds using symptom-based criteria (Rome criteria). Anxiety and depressive symptoms are more prevalent in patients with AP-FGIDs. Therefore, attention has been directed to the use of neuromodulators as potential interventions for AP-FGIDs. Antidepressants are one type of neuromodulators, and one of the most studied drugs for the management of AP-FGIDs in adult and pediatric population. Data available in pediatric population have significant limitations including nonuniform methodology with different study designs and primary endpoints. Evidence of the efficacy of antidepressants in the management of pediatric AP-FGIDs is not consistent. There is an urgent need for well-designed randomized clinical trials using age-appropriate validated outcome measures. Careful consideration must be given to adverse effects, particularly increased suicidal ideation.
Keywords: tricyclic antidepressants, SSRI, functional gastrointestinal disorders, children
Introduction
Chronic abdominal pain is a common problem encountered in childhood.1 A significant percentage of pediatric chronic abdominal pain cases meet criteria for abdominal pain-functional gastrointestinal disorders (AP-FGIDs). AP-FGIDs are a group of disorders characterized by the presence of chronic abdominal pain without evidence of biochemical or structural abnormalities that may account for the symptoms. The diagnosis relies mainly on clinical evaluation and the use of symptom-based criteria known as Rome criteria. These criteria have been recently revised and are currently in its fourth iteration.2,3 AP-FGIDs are a global problem with a pooled prevalence of 13.5%. A recent cross-sectional study based on the Rome IV criteria in US children aged 0–18 years found that 24.7% of infants and toddlers aged 0–3 years and 25.0% of children and adolescents aged 4–18 years fulfilled symptom-based criteria for a functional gastrointestinal disorder (FGID).4 This group of disorders are costly and have a significant impact in the child daily activities and quality of life (QoL).1,4
The pathophysiology of FGIDs is thought to be multifactorial. There is significant evidence of the role of predisposing factors including genetic makeup, stressful events during childhood, and pathophysiologic mechanisms such as visceral hypersensitivity, altered gastrointestinal motility, intestinal dysbiosis, and altered central nervous system processing.5 Accordingly, the association between pediatric recurrent abdominal pain (RAP), anxiety, and depression is well established.6 Anxiety and depressive symptoms are more prevalent in patients with AP-FGIDs.7,8 Higher rates of AP-FGIDs have also been reported in adolescents with anxiety or depressive symptoms.9 These disorders are considered problems of the brain–gut interaction, and usually require multidisciplinary treatments. Nonpharmacologic strategies such as cognitive-behavioral therapy (CBT) and hypnotherapy have consistently demonstrated superior efficacy in improving pain in children with AP-FGIDs.10–12 When available, these are excellent tools that constitute the first line of treatment of pediatric patients with AP-FGIDs. However, these interventions involve significant amount of time and require qualified professionals, consequently not realistic in most settings in our current environment. Emerging evidence on new ways to provide these techniques in a cost-effective and accessible manner including telephone-delivered CBT and exposure-based Internet-CBT are promising.13,14 Central neuromodulators have also been used as a therapy, and the antidepressants are the central modulators that have been more extensively used and studied for the management of AP-FGIDs in adult and pediatric population (Tables 1 and 2).15–19
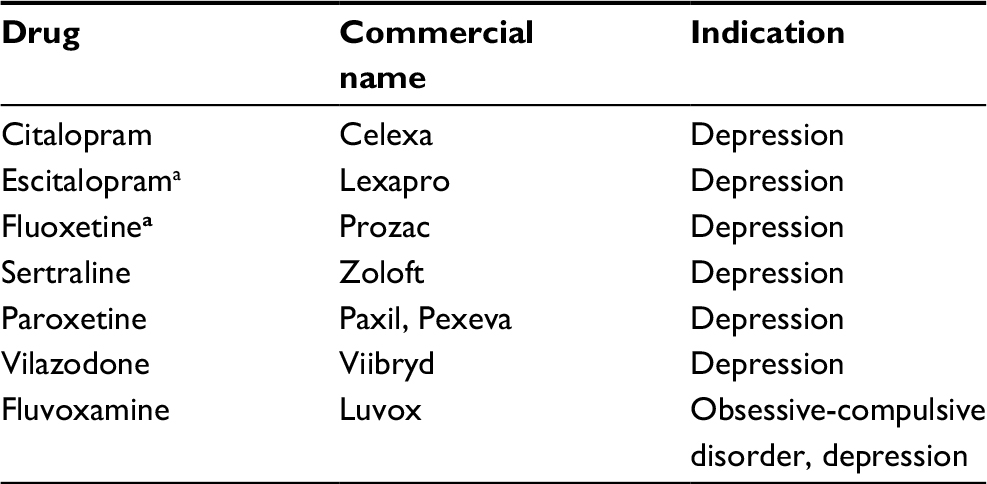 | Table 1 Selective serotonin reuptake inhibitors Note: aUS Food and Drug Administration approved for the treatment of pediatric depression. |
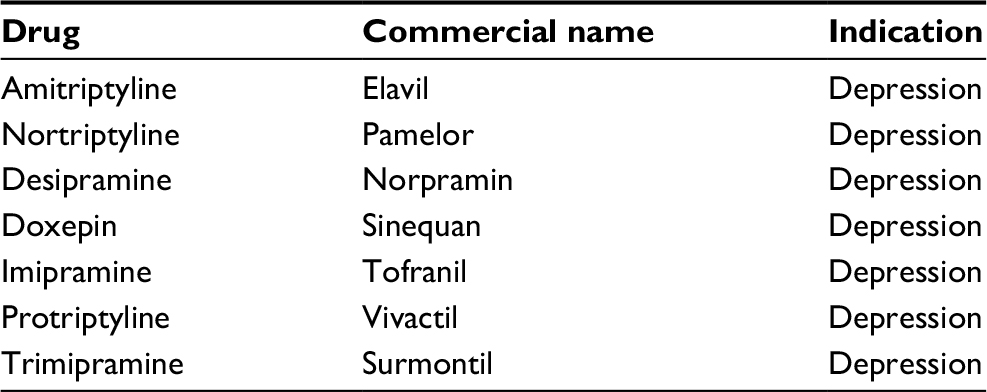 | Table 2 Tricyclic antidepressants |
Data available in pediatric population have significant limitations with lack of multicenter, randomized controlled trials (RCTs)18 (Table 3). Among the few RCTs investigating pharmacologic interventions in AP-FGIDs, there is a lack of uniform methodologies such as study design and primary endpoints, which constitute significant barriers in interpreting and extrapolating findings to the patient population.15,18,20 Adverse effects and outcomes such as definitive suicidal behavior and suicidal ideation also call for careful consideration when contemplating its use. A systematic review including more than 3,000 children and adolescents found an increased risk (58%) of suicide-related outcome for those on antidepressant compared to placebo, which equals to an increase from baseline risk from 25 in 1,00040 in 1,000.21
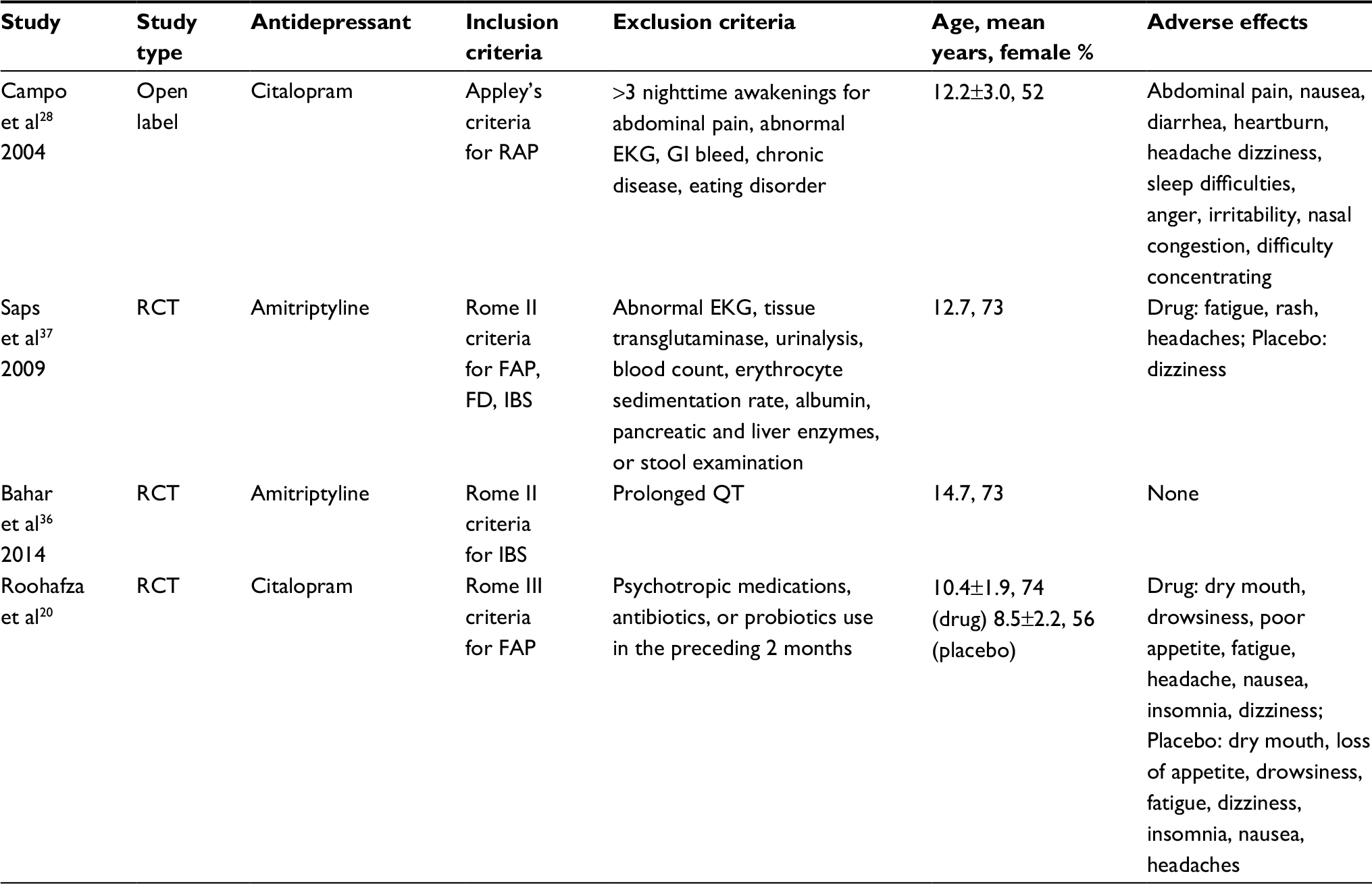 | Table 3 Summary of antidepressant studies in children Abbreviations: EKG, electrocardiography; FAP, functional abdominal pain; FD, funtional dyspepsia; GI, gastrointestinal; IBS, irritable bowel syndrome; RAP, recurrent abdominal pain; RCT, randomized, placebo-controlled trial. |
The main types of antidepressants that have been used in AP-FGID fall into the following categories19:
- Tricyclic antidepressants (TCAs). Their main antidepressant (and analgesic) properties are a variable combination of 5-HT and noradrenaline reuptake inhibition properties (Table 2).
- Selective serotonin reuptake inhibitors (SSRIs). SSRIs are characterized by selective blockade of the presynaptic 5-HT transporter, thereby boosting 5-HT neurotransmission (Table 1).
- Serotonin noradrenaline reuptake inhibitors. Like the TCAs, they primarily block both 5-HT and noradrenaline reuptake thereby boosting their neurotransmission. These include medications like duloxetine and venlafaxine.
- Noradrenergic and specific serotoninergic (tetracyclic) antidepressants. They boost both 5-HT and noradrenaline neurotransmission, not by blocking their reuptake pumps, but by blocking presynaptic A2 noradrenergic auto- and heteroreceptors on noradrenaline and 5-HT neurons, respectively, which act as brakes on both noradrenaline and 5-HT release from these respective neurons. These include medications like mirtazapine.
Given that most of the experience in pediatric AP-FGIDs is with the use of TCAs and SSRIs, they will be the focus of the present review.
SSRIs
SSRIs are the most commonly prescribed antidepressants.18 Approved by the US Food and Drug Administration (FDA) for the treatment of depression (escitalopram and fluoxetine are the only agents approved in pediatrics), they are relatively safe and typically cause fewer side effects than other types of antidepressants22 (Table 1). There are several possible mechanisms that might explain their beneficial effect in AP-FGIDs independent of mood changes that do benefit patients with psychological comorbidities such as depression. Among these mechanisms are a possible effect on visceral hypersensitivity, acceleration of transit time (beneficial in patients with additional constipation), and analgesic effects.23–25 In addition, some SSRIs may reduce the reporting of multiple bodily symptoms or somatization as well as reduce negative biases in information processing leading to reduce attention to gastrointestinal sensations.26,27
Citalopram has been the most studied SSRI in AP-FGIDs. A small, single-center open-label study that included 25 children and adolescents aged 7–18 years with RAP found a significant response (84%) using a maximum dose of 40 mg daily for a total of 12 weeks.28 Primary and secondary outcomes were patient-reported outcomes including improvement of abdominal pain, anxiety, depression, other somatic symptoms, functional impairment, and overall improvement. No major side effects were reported. A single-tertiary-care-center RCT from Iran published almost a decade later also found the effectiveness of citalopram.29 One hundred fifteen children who met Rome III criteria for functional abdominal pain (FAP) were included. The dose was 10 mg/day for the first week and 20 mg/day subsequently for a total duration of 4 weeks. The primary outcome was 50% improvement in the pain scale compared to baseline.30 Per-protocol analysis of response rate in the citalopram and placebo groups was 55.8% and 39.5% at week 4 (P=0.097) and 72% and 53.4% at week 12 (P=0.059), respectively. The intention to treat (ITT) revealed no difference in treatment response rate between the groups at 4 or 12 weeks. The citalopram group experienced more drowsiness and dry mouth than the placebo group. Side effects were mild and did not lead to discontinuation of the medication. The effect on pain was independent of the patient’s psychological status, which has also been the case in adult studies.17 This observation highlights the importance of SSRI mechanisms other than psychotropic effects such as analgesia at central and peripheral levels.31 As in many of the adult and pediatric trials, the placebo effect is exceedingly high, which underscores the need of well-powered studies of longer duration.
A recent retrospective, single-tertiary-care-center study that investigated treatment efficacy of antidepressant use in pediatric FAP found a significantly greater response to SSRIs than TCAs even after controlling for psychiatric factors (univariate analysis P=0.03).32 Eighty-five patients were on SSRIs (mostly citalopram). Most patients were started on low doses of 5–10 mg, which were titrated up to 60–200 mg depending on the specific SSRI. Half of the patients on SSRI had psychological comorbidity of anxiety and required psychiatric or psychological interventions. Interestingly, most of the SSRIs were prescribed by psychiatrists (59%), followed by gastroenterologist (39%) and a small percentage by pediatricians. Conversely, TCAs were largely prescribed by gastroenterologists (88%). The latter is not surprising as TCAs are typically used for the treatment of pain, in contrast to SSRIs, whose use is more focused on the treatment of underlying anxiety and depression. An interesting finding was the minimal consideration of associated gastrointestinal symptoms such as diarrhea or constipation in the decision to prescribe TCAs or SSRIs, which resulted in adverse effects and in many instances in termination of the medication. As such, TCAs should be used carefully in patients with constipation, while SSRIs should be avoided in patients with diarrhea.
TCAs
TCAs are among the initial antidepressants developed (Table 2). Their effectiveness has been demonstrated, being FDA-approved for the treatment of depression. The mechanism of action of these first-generation medications involves serotonergic and/or noradrenergic pathways.33 They block the reuptake of serotonin and norepinephrine increasing their levels in the brain. Unfortunately, TCAs also blocked histaminic, cholinergic, and alpha1-adrenergic receptor sites causing subsequent undesirable side effects. Among the most common side effects are weight gain, dry mouth, constipation, drowsiness, and dizziness.33 Increased risk of adverse cardiac events, and an FDA black box warning on suicidality risk have led to their replacement by the newer generation of antidepressants that are linked with fewer side effects.34,35 TCA overdose produces conduction delays and prolonged corrected QT (QTc) in children.36 However, low doses of TCAs such as amitriptyline in children do not appear to be associated with clinically significant changes in cardiac conduction.37
TCAs’ analgesic effects have been studied in several chronic pain syndromes including irritable bowel syndrome (IBS), low back pain, migraine, tension-type, and mixed headaches, and neuropathic pain.38–40 Possible mechanisms that explain the beneficial effects of antidepressants specifically in IBS include improvement on key pathophysiologic mechanism including visceral hypersensitivity and dysregulation of central pain perception.41 Improvement of the sensory threshold to colonic and rectal balloon distention and electrical stimulation has been observed with TCAs.42,43 Other potential mechanisms include anticholinergic effects, changes in gastrointestinal transit, and peripheral antineuropathic effects.43
An updated systematic review and meta-analysis of RCT in adults with IBS published in 2014 found that antidepressants are effective treatments for IBS.17 Forty-eight RCTs were eligible for inclusion, of which 16 compared antidepressants with placebo, and one compared both psychological therapy and antidepressants with placebo. The relative risk (RR) of IBS symptom not improving with antidepressants vs placebo was 0.67 (95% CI =0.58–0.77), with no difference between TCAs and SSRIs. A recent systematic review of a working group of the Rome Foundation provided the following recommendations for the use of antidepressants in adults: 1) low to modest dosages of TCAs provide the most convincing evidence of benefit for treating chronic gastrointestinal pain and AP-FGIDs and serotonin noradrenergic reuptake inhibitors can also be recommended, though further studies are needed; 2) augmentation, that is, adding a second treatment (adding quetiapine, aripiprazole, buspirone, and ligand agents) is recommended when a single medication is unsuccessful or produces side effects at higher dosages; 3) treatment should be continued for 6–12 months to potentially prevent relapse; and 4) implementation of successful treatment requires effective communication skills to improve patient acceptance and adherence and to optimize the patient–provider relationship.19
The information in children is limited. A systematic review in children and adolescents published in 2011, and a follow-up in 201618 found no evidence that supports the use of antidepressants for the treatment of AP-FGIDs, cautioning clinicians to consider potential benefits as well as risks of this group of medications in pediatric patients.15
Among the TCAs, amitriptyline is the agent that has been studied the most in the treatment of AP-FGIDs in children. From the few randomized clinical trials of pharmacologic agents available in pediatrics, two studies assessed the efficacy of amitriptyline.44,45 Bahar et al conducted a single-center double-blind placebo-controlled trial in 23 newly diagnosed adolescent patients (12–18 years of age) with IBS.44 The investigators used a symptom checklist, pain rating scale, visual analog scale, and IBS QoL questionnaire. Subjects were randomized in a double-blinded fashion to receive amitriptyline or placebo and were evaluated at 2, 6, 10, and 13 weeks. There was improvement in the overall QoL score from baseline at 6, 10, and 13 weeks (P=0.019, 0.004, and 0.013, respectively). Patients in the amitriptyline group also experienced improvement in right lower quadrant pain at 6, 10, and 13 weeks (P=0.014, 0.039, and 0.004). There was no consistent improvement in pain in other areas. In addition, the investigators reported improvement of diarrhea symptoms at 6 and 10 weeks (P=0.029 for both). Pain relief after defecation, constipation, or pain exacerbation with defecation was not improved. There were no significant differences in the rate of interference with daily activities, and extraintestinal manifestations such as headache, back pain, dizziness, and fatigue between the amitriptyline and placebo groups.
Saps et al conducted a multicenter trial assessing the efficacy of amitriptyline in pediatric IBS, FAP, and functional dyspepsia.45 Ninety patients were randomized to 4 weeks of placebo or amitriptyline (10 mg/d<35 kg; 20 mg/d>35 kg). Eighty-three patients completed the study. The investigators assessed gastrointestinal symptoms, psychological traits, and daily activities before and after intervention. Pain was assessed daily with self-report diaries. Child’s assessment of pain relief and sense of improvement was the primary outcome. Effect on psychosocial traits and daily functioning were the secondary outcomes. Patients reported feeling better 63%, worse 5% in amitriptyline group vs better 57.5%, worse 2.5% in placebo group (P=0.63). There was no significant difference in pain relief in ITT or per-protocol (PP) analysis between amitriptyline and placebo groups at 4 weeks of treatment. Patients who reported severe pain at baseline in both groups (P=0.0065) fared worse. Patients with pain of mild-to-moderate intensity reacted better to treatment. Possible reasons for the failure of significant improvement in the amitriptyline group in regard to pain included the overwhelming placebo effect coupled with the relatively small population size.
In addition, the Saps trial found that amitriptyline significantly reduced anxiety scores (P<0.0001). In this regard, there is evidence from animal models that TCAs significantly prevent the anxiety-related behaviors induced by chronic neuropathic pain in mice.46 Human studies have also shown that amitriptyline reduced the activation of brain areas associated with pain, and emotional and cognitive function during mental stress in patients with IBS.47
Long-term efficacy of amitriptyline has not been established. A retrospective study in 98 pediatric patients with AP-FGIDs meeting the Rome III criteria for functional dyspepsia, IBS, and FAP found low-dose TCAs (amitriptyline or Imipramine) effective for a long duration.48 Seventy-eight percent of patients responded to the treatment for an average of 10.73 (range 1–45) months. In the subgroup of 27 patients with FAP, 85% responded well. Only five patients reported adverse effects that lead to stopping the medication and overall it was well tolerated for the study period. However, we need larger and long-term studies to fully establish TCAs’ long-term efficacy.
Other interventions to produce brain neuromodulation in AP-FGIDS
Psychological interventions
When discussing antidepressant medications, it is also imperative to discuss evidence available on psychological interventions in the management of AP-FGIDs particularly since there is compelling evidence in pediatrics. The latest systematic review and meta-analysis of antidepressants and psychological therapies in adults with IBS included 31 RCTs comparing psychological therapies with control therapy or “usual management”.49 Both the RR of IBS symptom not improving with antidepressants (TCAs and SSRIs) vs placebo, and psychological therapies were virtually similar (0.67 [95% CI =0.58–0.77] vs 0.68 [95% CI =0.61–0.76]). CBT, hypnotherapy, multicomponent psychological therapy, and dynamic psychotherapy were found to be valuable in the management of IBS.
Despite methodologic limitations, the consistency and magnitude of the effects reported provide some evidence that psychological interventions are useful for children with RAP.50 Cognitive-behavioral approaches such as guided imagery and progressive relaxation effectively reduced chronic abdominal pain and improved social functioning and school attendance in children with FGIDs.49 A combination of standard medical care and short-term cognitive-behavioral family treatment was more effective than standard medical care alone in children with RAP.51 CBT aimed at reducing protective parental responses and improving child coping skills was superior in reducing children’s pain and symptom levels compared to an educational control condition with apparent long-term efficacy.52,53 Clinical response was at least partially mediated by reducing maladaptive parent and child cognitions.54 Exposure-based CBT weekly for 10 weeks was feasible, acceptable, and potentially efficacious in 20 children with AP-FGIDs at posttreatment and at 6-month follow-up.55 In contrast, a randomized controlled trial found no difference in the effectiveness of a six-session CBT compared with six visits to a pediatrician (intense medical care) for the treatment of pediatric FAP underlying importance of further research on specific working mechanisms of CBT for pediatric AP-FGIDs.56 Treatment approaches that are more accessible such as internet-delivered family CBT intervention, telephone-delivered CBT, and exposure-based Internet-CBT have also demonstrated greater improvement in pain than a wait-list control group.13,14,57
Gut-directed hypnotherapy is highly effective in the treatment of children with long-standing FAP or IBS as found in a randomized controlled trial that compared the clinical effectiveness of hypnotherapy with standard medical therapy.10 Patients received either six sessions of hypnotherapy over a 3-month period or standard medical care and six sessions of supportive therapy. Pain intensity, pain frequency, and associated symptoms were scored at baseline, during therapy, and 6 and 12 months after therapy. Hypnotherapy was highly superior, with a significantly greater reduction in pain scores compared to standard medical treatment (P<0.001) with similar rates at 12 months follow-up. Sustained response was observed as well at 5 years follow-up.11 Furthermore, home-based hypnotherapy utilizing CDs has been shown to be almost as effective as hypnotherapy administered by a therapist with proven long-term effectiveness, offering a less costly and practical alternative.58,59 The investigators conducted a study hypothesizing that hypnotherapy improvement of clinical symptoms was driven by an improvement in rectal sensitivity; however, no association was found.60 A recent Cochrane review regarding the effectiveness of psychosocial interventions for school-aged children with RAP or AP-FGIDs found some evidence for beneficial effects of CBT and hypnotherapy in short-term reduction of pain.61
In light of the current accumulated evidence, the way we communicate with our patients and their parents is of utmost importance. Centering the discussion in the biopsychosocial model of care and providing a thoughtful explanation of the different factors that can trigger chronic abdominal pain including psychosocial contributors are paramount. The implementation of these changes, in turn, will boost the acceptance of psychosocial interventions for children with AP-FGIDs.62 Integrating these therapies into our conventionally medically oriented model of care can be challenging. Considering various models and adapting them to individual needs seems to be the best approach.63
Probiotics
Probiotics have been widely studied in animal models and patients with IBS. It has been suggested that probiotics have a neuromodulatory potential, although the underlying molecular mechanisms are unclear. IBS patients exhibit altered intestinal microbiota composition64,65 and lower microbial intestinal diversity.66 Fecal microbiota from IBS patients resulted in increased abdominal contractions in germ-free mice.67 A recent meta-analysis reported that probiotics reduced pain and symptom severity scores in IBS patients in comparison with placebo.68 Thus, several studies have targeted intestinal microbiota to regulate visceral pain.69,70 Bifidobacterium and lactobacillus species have been shown to reduce visceral pain in IBS animal models via regulation of the neural function and normalization of the hypothalamic pituitary adrenal (HPA) function.71–73 A recent study found that the combination of Lactobacillus helveticus and Bifidobacterium longum is more effective than probiotic alone in treating stress-induced visceral pain via HPA axis.74 In light of this evidence, probiotics appear to be an attractive alternative in terms of both efficacy and safety; however, larger studies are needed.
In conclusion, there is no consistent evidence of the efficacy of antidepressants in the management of pediatric AP-FGIDs. The majority of the studies have methodologic limitations and small sample size. There is an urgent need for well-designed randomized clinical trials using age-appropriate validated outcome measures. Careful consideration must be given to adverse effects, particularly increased suicidal ideation. Psychological interventions such as CBT and hypnotherapy have shown both short- and long-term efficacy in pain relief in children with AP-FGIDs; however. higher-quality, longer-term outcome studies are needed to fully investigate their effectiveness and potential mechanism of action.
Disclosure
The authors report no conflicts of interest in this work.
References
Saps M, Seshadri R, Sztainberg M, Schaffer G, Marshall BM, Di Lorenzo C. A prospective school-based study of abdominal pain and other common somatic complaints in children. J Pediatr. 2009;154(3):322–326. | ||
Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology. 2016:S0016-5085(16)00182-7. | ||
Hyams JS, di Lorenzo C, Saps M, et al. Functional disorders: children and adolescents. Gastroenterology. 2016:S0016-5085(16)00181-5. | ||
Robin SG, Keller C, Zwiener R, et al. Prevalence of pediatric functional gastrointestinal disorders utilizing the Rome IV criteria. J Pediatr. 2018;195:134–139. | ||
Korterink J, Devanarayana NM, Rajindrajith S, Vlieger A, Benninga MA. Childhood functional abdominal pain: mechanisms and management. Nat Rev Gastroenterol Hepatol. 2015;12(3):159–171. | ||
Campo JV, Bridge J, Ehmann M, et al. Recurrent abdominal pain, anxiety, and depression in primary care. Pediatrics. 2004;113(4):817–824. | ||
Rutten JM, Benninga MA, Vlieger AM. IBS and FAPS in children: a comparison of psychological and clinical characteristics. J Pediatr Gastroenterol Nutr. 2014;59(4):493–499. | ||
Dorn LD, Campo JC, Thato S, et al. Psychological comorbidity and stress reactivity in children and adolescents with recurrent abdominal pain and anxiety disorders. J Am Acad Child Adolesc Psychiatry. 2003;42(1):66–75. | ||
Yacob D, Di Lorenzo C, Bridge JA, et al. Prevalence of pain-predominant functional gastrointestinal disorders and somatic symptoms in patients with anxiety or depressive disorders. J Pediatr. 2013;163(3):767–770. | ||
Vlieger AM, Menko-Frankenhuis C, Wolfkamp SC, Tromp E, Benninga MA. Hypnotherapy for children with functional abdominal pain or irritable bowel syndrome: a randomized controlled trial. Gastroenterology. 2007;133(5):1430–1436. | ||
Vlieger AM, Rutten JM, Govers AM, Frankenhuis C, Benninga MA. Long-term follow-up of gut-directed hypnotherapy vs. standard care in children with functional abdominal pain or irritable bowel syndrome. Am J Gastroenterol. 2012;107(4):627–631. | ||
Rutten JM, Korterink JJ, Venmans LM, Benninga MA, Tabbers MM. Nonpharmacologic treatment of functional abdominal pain disorders: a systematic review. Pediatrics. 2015;135(3):522–535. | ||
Levy RL, Langer SL, van Tilburg MA, et al. Brief telephone-delivered cognitive behavioral therapy targeted to parents of children with functional abdominal pain: a randomized controlled trial. Pain. 2017;158(4):618–628. | ||
Lalouni M, Ljótsson B, Bonnert M, et al. Internet-delivered cognitive behavioral therapy for children with pain-related functional gastrointestinal disorders: feasibility study. JMIR Ment Health. 2017;4(3):e32. | ||
Kaminski A, Kamper A, Thaler K, Chapman A, Gartlehner G. Antidepressants for the treatment of abdominal pain-related functional gastrointestinal disorders in children and adolescents. Cochrane Database Syst Rev. 2011;7(7):CD008013. | ||
Ruepert L, Quartero AO, de Wit NJ, et al. Bulking agents, antispasmodics and antidepressants for the treatment of irritable bowel syndrome. Cochrane Database Syst Rev. 2011;(8):CD003460. | ||
Ford AC, Quigley EM, Lacy BE, van der Heijden GJ, Rubin G, Muris JW. Effect of antidepressants and psychological therapies, including hypnotherapy, in irritable bowel syndrome: systematic review and meta-analysis. Am J Gastroenterol. 2014;1091366(9):1350–1365quiz. | ||
Cooper TE, Heathcote LC, Clinch J, et al. Antidepressants for chronic non-cancer pain in children and adolescents. Cochrane Database Syst Rev. 2017;8:CD012535. | ||
Drossman DA, Tack J, Ford AC, Szigethy E, Törnblom H, Van Oudenhove L. Neuromodulators for functional gastrointestinal disorders (disorders of gut-brain interaction): a Rome Foundation Working Team Report. Gastroenterology. 2018;154(4):1140–1171.e1. | ||
Saps M, Biring HS, Pusatcioglu CK, Mintjens S, Rzeznikiewiz D. A comprehensive review of randomized placebo-controlled pharmacological clinical trials in children with functional abdominal pain disorders. J Pediatr Gastroenterol Nutr. 2015;60(5):645–653. | ||
Hetrick SE, McKenzie JE, Cox GR, Simmons MB, Merry SN. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851. | ||
Wagner KD, Robb AS, Findling RL, Jin J, Gutierrez MM, Heydorn WE. A randomized, placebo-controlled trial of citalopram for the treatment of major depression in children and adolescents. Am J Psychiatry. 2004;161(6):1079–1083. | ||
Tack J, Broekaert D, Corsetti M, Fischler B, Janssens J. Influence of acute serotonin reuptake inhibition on colonic sensorimotor function in man. Aliment Pharmacol Ther. 2006;23(2):265–274. | ||
Gorard DA, Libby GW, Farthing MJ. Influence of antidepressants on whole gut and orocaecal transit times in health and irritable bowel syndrome. Aliment Pharmacol Ther. 1994;8(2):159–166. | ||
Aragona M, Bancheri L, Perinelli D, et al. Randomized double-blind comparison of serotonergic (Citalopram) versus noradrenergic (Reboxetine) reuptake inhibitors in outpatients with somatoform, DSM-IV-TR pain disorder. Eur J Pain. 2005;9(1):33–38. | ||
Clouse RE, Lustman PJ. Use of psychopharmacological agents for functional gastrointestinal disorders. Gut. 2005;54(9):1332–1341. | ||
Kilkens TO, Honig A, Fekkes D, Brummer RJ. The effects of an acute serotonergic challenge on brain-gut responses in irritable bowel syndrome patients and controls. Aliment Pharmacol Ther. 2005;22(9):865–874. | ||
Campo JV, Perel J, Lucas A, et al. Citalopram treatment of pediatric recurrent abdominal pain and comorbid internalizing disorders: an exploratory study. J Am Acad Child Adolesc Psychiatry. 2004;43(10):1234–1242. | ||
Roohafza H, Pourmoghaddas Z, Saneian H, Gholamrezaei A. Citalopram for pediatric functional abdominal pain: a randomized, placebo-controlled trial. Neurogastroenterol Motil. 2014;26(11):1642–1650. | ||
Corsetti M, Tack J. FDA and EMA end points: which outcome end points should we use in clinical trials in patients with irritable bowel syndrome? Neurogastroenterol Motil. 2013;25(6):453–457. | ||
Kuiken SD, Tytgat GN, Boeckxstaens GE. Review article: drugs interfering with visceral sensitivity for the treatment of functional gastrointestinal disorders--the clinical evidence. Aliment Pharmacol Ther. 2005;21(6):633–651. | ||
Zar-Kessler CAM, Belkind-Gerson J, Bender S, Kuo BM. Treatment of functional abdominal pain with antidepressants: benefits, adverse effects, and the gastroenterologist’s role. J Pediatr Gastroenterol Nutr. 2017;65(1):16–21. | ||
Feighner JP. Mechanism of action of antidepressant medications. J Clin Psychiatry. 1999;60 (Suppl 4):4–11; discussion 12–13. | ||
Ray WA, Meredith S, Thapa PB, Hall K, Murray KT. Cyclic antidepressants and the risk of sudden cardiac death. Clin Pharmacol Ther. 2004;75(3):234–241. | ||
Olfson M, Marcus SC, Druss BG. Effects of Food and Drug Administration warnings on antidepressant use in a national sample. Arch Gen Psychiatry. 2008;65(1):94–101. | ||
James LP, Kearns GL. Cyclic antidepressant toxicity in children and adolescents. J Clin Pharmacol. 1995;35(4):343–350. | ||
Chogle A, Saps M. Electrocardiograms changes in children with functional gastrointestinal disorders on low dose amitriptyline. World J Gastroenterol. 2014;20(32):11321–11325. | ||
Jackson JL, O’Malley PG, Tomkins G, Balden E, Santoro J, Kroenke K. Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis. Am J Med. 2000;108(1):65–72. | ||
Atkinson JH, Slater MA, Wahlgren DR, et al. Effects of noradrenergic and serotonergic antidepressants on chronic low back pain intensity. Pain. 1999;83(2):137–145. | ||
Jackson JL, Shimeall W, Sessums L, et al. Tricyclic antidepressants and headaches: systematic review and meta-analysis. BMJ. 2010;341: c5222. | ||
Saarto T, Wiffen PJ. Antidepressants for neuropathic pain. Cochrane Database Syst Rev. 2005;(3):CD005454. | ||
Truong TT, Naliboff BD, Chang L. Novel techniques to study visceral hypersensitivity in irritable bowel syndrome. Curr Gastroenterol Rep. 2008;10(4):369–378. | ||
Gorelick AB, Koshy SS, Hooper FG, Bennett TC, Chey WD, Hasler WL. Differential effects of amitriptyline on perception of somatic and visceral stimulation in healthy humans. Am J Physiol. 1998;275(3 Pt 1):G460–G466. | ||
Bahar RJ, Collins BS, Steinmetz B, Ament ME. Double-blind placebo-controlled trial of amitriptyline for the treatment of irritable bowel syndrome in adolescents. J Pediatr. 2008;152(5):685–689. | ||
Saps M, Youssef N, Miranda A, et al. Multicenter, randomized, placebo-controlled trial of amitriptyline in children with functional gastrointestinal disorders. Gastroenterology. 2009;137(4):1261–1269. | ||
Matsuzawa-Yanagida K, Narita M, Nakajima M, et al. Usefulness of antidepressants for improving the neuropathic pain-like state and pain-induced anxiety through actions at different brain sites. Neuropsychopharmacology. 2008;33(8):1952–1965. | ||
Morgan V, Pickens D, Gautam S, Kessler R, Mertz H. Amitriptyline reduces rectal pain related activation of the anterior cingulate cortex in patients with irritable bowel syndrome. Gut. 2005;54(5):601–607. | ||
Teitelbaum JE, Arora R. Long-term efficacy of low-dose tricyclic antidepressants for children with functional gastrointestinal disorders. J Pediatr Gastroenterol Nutr. 2011;53(3):260–264. | ||
Youssef NN, Rosh JR, Loughran M, et al. Treatment of functional abdominal pain in childhood with cognitive behavioral strategies. J Pediatr Gastroenterol Nutr. 2004;39(2):192–196. | ||
Huertas-Ceballos A, Logan S, Bennett C, Macarthur C. Psychosocial interventions for recurrent abdominal pain (RAP) and irritable bowel syndrome (IBS) in childhood. Cochrane Database Syst Rev. 2008;(1):CD003014. | ||
Robins PM, Smith SM, Glutting JJ, Bishop CT. A randomized controlled trial of a cognitive-behavioral family intervention for pediatric recurrent abdominal pain. J Pediatr Psychol. 2005;30(5):397–408. | ||
Levy RL, Langer SL, Walker LS, et al. Cognitive-behavioral therapy for children with functional abdominal pain and their parents decreases pain and other symptoms. Am J Gastroenterol. 2010;105(4):946–956. | ||
Levy RL, Langer SL, Walker LS, et al. Twelve-month follow-up of cognitive behavioral therapy for children with functional abdominal pain. JAMA Pediatr. 2013;167(2):178–184. | ||
Levy RL, Langer SL, Romano JM, et al. Cognitive mediators of treatment outcomes in pediatric functional abdominal pain. Clin J Pain. 2014;30(12):1033–1043. | ||
Lalouni M, Olén O, Bonnert M, Hedman E, Serlachius E, Ljótsson B. Exposure-based cognitive behavior therapy for children with abdominal pain: a pilot trial. PLoS One. 2016;11(10):e0164647. | ||
van der Veek SM, Derkx BH, Benninga MA, Boer F, de Haan E. Cognitive behavior therapy for pediatric functional abdominal pain: a randomized controlled trial. Pediatrics. 2013;132(5):e1163–e1172. | ||
Palermo TM, Wilson AC, Peters M, Lewandowski A, Somhegyi H. Randomized controlled trial of an Internet-delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain. Pain. 2009;146(1–2):205–213. | ||
Rutten JM, Vlieger AM, Frankenhuis C, et al. Gut-directed hypnotherapy in children with irritable bowel syndrome or functional abdominal pain (syndrome): a randomized controlled trial on self exercises at home using CD versus individual therapy by qualified therapists. BMC Pediatr. 2014;14:140. | ||
Rutten J, Vlieger AM, Frankenhuis C, et al. Home-based hypnotherapy self-exercises vs individual hypnotherapy with a therapist for treatment of pediatric irritable bowel syndrome, functional abdominal pain, or functional abdominal pain syndrome: a randomized clinical trial. JAMA Pediatr. 2017;171(5):470–477. | ||
Vlieger AM, van den Berg MM, Menko-Frankenhuis C, Bongers ME, Tromp E, Benninga MA. No change in rectal sensitivity after gut-directed hypnotherapy in children with functional abdominal pain or irritable bowel syndrome. Am J Gastroenterol. 2010;105(1):213–218. | ||
Abbott RA, Martin AE, Newlove-Delgado TV, et al. Psychosocial interventions for recurrent abdominal pain in childhood. Cochrane Database Syst Rev. 2017;1:CD010971. | ||
Sood E, Pinder W, Pendley JS, Fisher AO, Wali PD, del Rosario F. Provider communication regarding psychosocial factors predicts pain beliefs in parent and child. J Dev Behav Pediatr. 2016;37(3):205–212. | ||
Reed-Knight B, Claar RL, Schurman JV, van Tilburg MA. Implementing psychological therapies for functional GI disorders in children and adults. Expert Rev Gastroenterol Hepatol. 2016;10(9):981–984. | ||
Jeffery IB, O’Toole PW, Öhman L, et al. An irritable bowel syndrome subtype defined by species-specific alterations in faecal microbiota. Gut. 2012;61(7):997–1006. | ||
Rajilić-Stojanović M, Biagi E, Heilig HG, et al. Global and deep molecular analysis of microbiota signatures in fecal samples from patients with irritable bowel syndrome. Gastroenterology. 2011;141(5):1792–1801. | ||
Tap J, Derrien M, Törnblom H, et al. Identification of an intestinal microbiota signature associated with severity of irritable bowel syndrome. Gastroenterology. 2017;152(1):111–123.e8. | ||
Crouzet L, Gaultier E, Del’Homme C, et al. The hypersensitivity to colonic distension of IBS patients can be transferred to rats through their fecal microbiota. Neurogastroenterol Motil. 2013;25(4): e272–e282. | ||
Didari T, Mozaffari S, Nikfar S, Abdollahi M. Effectiveness of probiotics in irritable bowel syndrome: Updated systematic review with meta-analysis. World J Gastroenterol. 2015;21(10):3072–3084. | ||
Mazurak N, Broelz E, Storr M, Enck P. Probiotic therapy of the irritable bowel syndrome: why is the evidence still poor and what can be done about it? J Neurogastroenterol Motil. 2015;21(4):471–485. | ||
Sisson G, Ayis S, Sherwood RA, Bjarnason I, et al. Randomised clinical trial: a liquid multi-strain probiotic vs. placebo in the irritable bowel syndrome - a 12week double-blind study. Aliment Pharmacol Ther. 2014;40(1):51–62. | ||
Kamiya T, Wang L, Forsythe P, et al. Inhibitory effects of Lactobacillus reuteri on visceral pain induced by colorectal distension in Sprague-Dawley rats. Gut. 2006;55(2):191–196. | ||
Ma X, Mao YK, Wang B, Huizinga JD, Bienenstock J, Kunze W. Lactobacillus reuteri ingestion prevents hyperexcitability of colonic DRG neurons induced by noxious stimuli. Am J Physiol Gastrointest Liver Physiol. 2009;296(4):G868–G875. | ||
Gareau MG, Jury J, MacQueen G, Sherman PM, Perdue MH. Probiotic treatment of rat pups normalises corticosterone release and ameliorates colonic dysfunction induced by maternal separation. Gut. 2007;56(11):1522–1528. | ||
Ait-Belgnaoui A, Payard I, Rolland C, et al. Bifidobacterium longum and Lactobacillus helveticus synergistically suppress stress-related visceral hypersensitivity through hypothalamic-pituitary-adrenal axis modulation. J Neurogastroenterol Motil. 2018;24(1):138–146. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.