")
Back to Journals » Clinical Ophthalmology » Volume 11
Flap motility as a sign of posterior capsule rupture in peripherally extended anterior capsular tears
Authors Om Parkash R, Mahajan S, Biala V, Om Parkash T, Tasneem AF
Received 11 March 2017
Accepted for publication 14 July 2017
Published 8 August 2017 Volume 2017:11 Pages 1445—1451
DOI https://doi.org/10.2147/OPTH.S136532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Rohit Om Parkash.
Views: 3010
Rohit Om Parkash,1 Shruti Mahajan,2 Vinod Biala,3 Tushya Om Parkash,4 Alhaj F Tasneem5
1Department of Cataract Surgery, 2Department of Cataract and Refractive Surgery, Dr Om Parkash Eye Institute, Amritsar, 3Department of Cataract Surgery, Eye Care Centre, Ghaziabad, 4Department of Cataract and Refractive Surgery, 5Department of Ophthalmology, Vydehi Institute of Medical Sciences and Research Centre, Bangalore, India
Purpose: To describe various types of anterior capsular tears and an early diagnostic, flap motility, as a sign of posterior capsular rupture following posterior extension of radial tears.
Design: This was a prospective study carried out in 4,331 eyes that underwent phacoemulsification in a private practice setting from April 2015 to February 2016. Twenty six consecutive cases of anterior capsular tears were included. Morphological features of anterior capsular tears and resultant complications were evaluated. Parameters studied were surgical step during which the tear occurred, shape of tear, its extension in relation to the equator, and flap nature and motility in tear extending up to equator.
Main outcome measures: The main outcome measures were motility and nature of flaps in anterior capsular radial tears and the relation to posterior capsule rupture.
Results: Based on shape, extent, and angulation, anterior capsular tears were categorized into 5 types: Type I, pre-equatorial radial tear (26.92%); Type II, post-equatorial radial tear (3.85%); Type III, Argentinean flag sign pre-equatorial tear (57.69%); Type IV, Argentinean flag sign post-equatorial tear (7.69%), and Type V, mini punch (3.85%). Flaps were either seen to be everted and fluttering or inverted and non-fluttering. In all cases with everted fluttering flaps no posterior capsular rupture (PCR) was observed, while in cases with inverted non-fluttering flaps a PCR was observed (p<0.05).
Conclusion: Everted and fluttering flaps of the anterior capsular tears indicate pre-equatorial tear, while inverted and non-fluttering flaps indicate posterior capsule rupture following tear extension beyond the equator.
Keywords: anterior capsule tear, posterior capsule rupture, flap motility sign, earliest sign
Introduction
Radial tears in capsulorhexis margin are not an uncommon complication and can occur during any stage of phacoemulsification surgery.1 Once a tear occurs in the capsulorhexis margin, it can easily extend to the equator and sometimes beyond it due to the irrigating fluid and the inter-capsular pressure created by lens material. If it extends to the posterior capsule causing a posterior capsule rent (PCR), then the surgery can get complicated by vitreous loss or nucleus drop.2 At present, there is no known intraoperative clue that can ascertain the extent of intraoperative radial tear of the capsulorhexis margin. Consequently, the surgeon remains in a dilemma whether to continue or abort phacoemulsification.
In the present study, we describe various types of anterior capsular tears and for the first time an intraoperative sign, flap motility, that can help to ascertain the extent of the anterior capsular tear in relation to lens equator.
Materials and methods
This prospective study comprised 4,331 eyes with a clinical diagnosis of cataract that underwent phacoemulsification in a private practice setting from April 2015 to February 2016. The study analyzed anterior capsular tears in 26 consecutive cases, which occurred while performing phacoemulsification. The protocol adhered to the tenets of the Declaration of Helsinki and received approval from the ethics committee of Dr Om Parkash Eye Hospital. Prior to the surgical procedure all of the patients provided a written informed consent for the surgery and for inclusion in this study. The anterior capsular tears in patients with subluxated cataracts and maculo-leucomatous corneal opacities were excluded from the study. Patients aged 20–70 years (mean 56.40±8.63 years) with variable grades of cataract were included in the study. Morphological features of anterior capsular tears and the resultant complications, if any, were studied. The parameters studied were anterior chamber depth (ACD), type and density of cataract, step of surgery during which tear occurred, shape of tear, and its extension in relation to the equator of lens. Additionally, the nature and motility of the flaps of the capsular tears were closely observed in relation to the extension of the tear up to the equator or beyond it. The nature of the flap was noted as everted or inverted/flat. The motility of the flap was noted as fluttering or non-fluttering.
The hypothesis was that the everted and fluttering flaps do not extend beyond the equator and the inverted and non-fluttering flaps indicate the extension of the flap beyond the equator onto the posterior capsule with associated complications. This is explained as follows:
- Fluttering and everted flap in the pre-equatorial anterior capsular tear: When the edge of the anterior capsular tear does not extend beyond the equator, the capsular flap traverses a short distance prior to the equator. The flap thus formed remains everted and free. The end point of the extension of the flap functions as the pivotal point for the flap. The flap, being short, is responsive to the pressure gradient dynamics of the anterior chamber and thus flutters freely.
- Non-fluttering and inverted flap in the post equatorial tear: During phacoemulsification, the intact posterior capsule compartmentalizes the eye into the highly pressurized anterior segment and relatively less-pressurized posterior segment. The inflated bag in the anterior compartment has the weight of the lenticular content and a high pressure due to the fluidics involved in the procedure. When the extension of the flap goes beyond the equator, there is no more division into the anterior and posterior compartments. The weight of the lenticular content, the fluid dynamics in the bag, and the high intraocular pressure in the anterior chamber cause the bag contents to move posteriorly. Simultaneously, there is extension of the tear (Figure 1). Furthermore, the negative pressure in the posterior segment makes the bag contents to move posteriorly. The posterior displacement of the tear moves the corresponding anterior part of the tear along with it posteriorly. The continuous posterior pulling of the whole flap makes it flat and eventually inverted. Subsequently, the taut flap becomes totally non-responsive to the pressure gradient dynamics of the anterior chamber and stops fluttering.
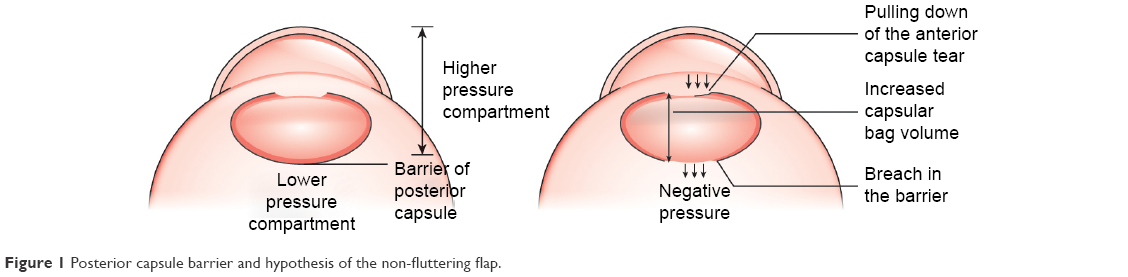 | Figure 1 Posterior capsule barrier and hypothesis of the non-fluttering flap. |
Statistical analysis
Statistical analysis was performed by STATA 11.2 (College Station, TX, USA). Fisher exact test was used to measure the association between the posterior capsule rupture with everted flap, inverted flap, fluttering flap, and non-fluttering flap, respectively. These parameters were expressed as frequency and percentage. p<0.05 was considered as statistically significant.
Results
In this study, of the 26 cases, 14 were males and 12 were females with an age range of 29–67 years (56.4±8.63 years). Of the 26 cases, 17 (65.38%) had white mature cataract. Mean ACD was 2.92±0.34 mm. Based on the shape, extent, and angulation, the anterior capsular tears were categorized into five types (Figure 2):
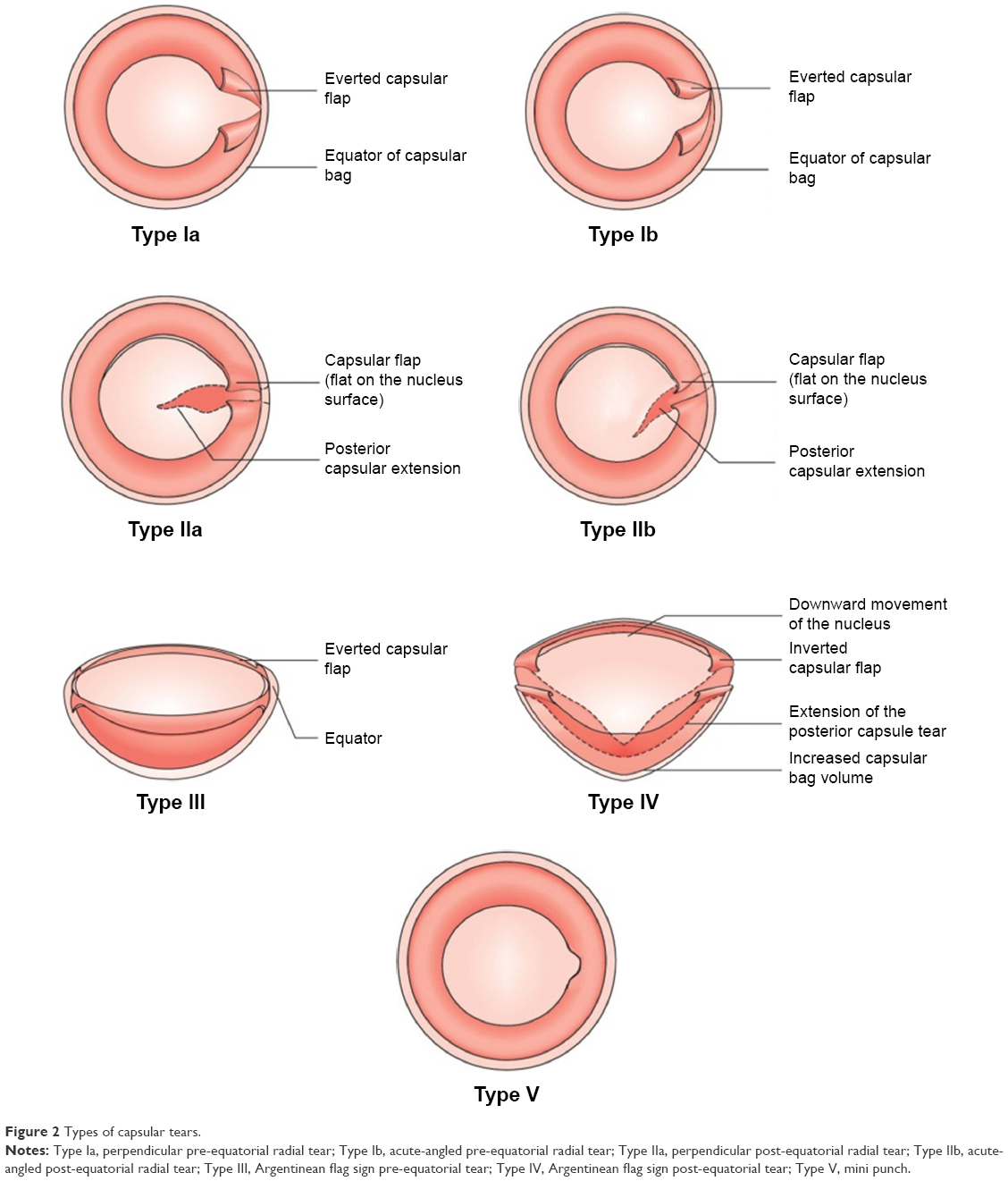 | Figure 2 Types of capsular tears. |
- Type I – pre-equatorial radial tear
Type Ia – perpendicular pre-equatorial radial tear (11.54%)
Type Ib – acute-angled pre-equatorial radial tear (15.38%) - Type II – post-equatorial radial tear
Type IIa – perpendicular post-equatorial radial tear (3.85%)
Type IIb – acute angled post-equatorial radial tear (0%) - Type III – Argentinean flag sign pre-equatorial tear (57.69%)
- Type IV – Argentinean flag sign post-equatorial tear (7.69%)
- Type V – mini punch (3.85%)
The most common radial tears were the perpendicular tears not extending beyond the equator. The acute-angled tears were caused in cases of zonulopathy associated with pseudoexfoliation. Type V (mini punch) in the capsulorhexis was observed during phacoemulsification in one case by the phaco probe. Since the Type V (mini punch) did not extend to the periphery, it was excluded from the study for statistical analysis. Most of the anterior capsular tears (84%) occurred during the step of capsulorhexis (Table 1).
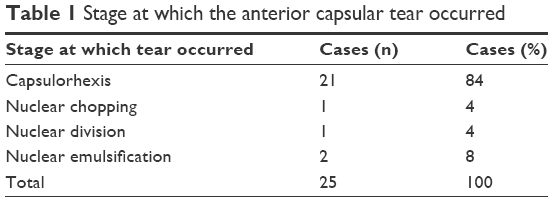 | Table 1 Stage at which the anterior capsular tear occurred |
In 21 out of 25 cases the flap was seen to be everted, while in 4 out of 25 cases the flap was inverted. Flaps of the tear in all the cases that had everted flaps were seen to be fluttering during phacoemulsification procedure. In these cases, no PCR was observed to occur (p-value <0.05; Tables 2 and 3). The cases that had inverted flaps, no flap fluttering was observed and all these cases developed a PCR (p-value <0.05; Tables 4 and 5).
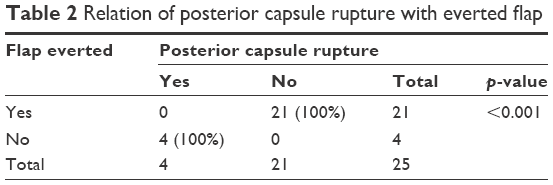 | Table 2 Relation of posterior capsule rupture with everted flap |
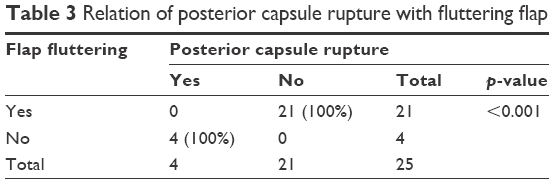 | Table 3 Relation of posterior capsule rupture with fluttering flap |
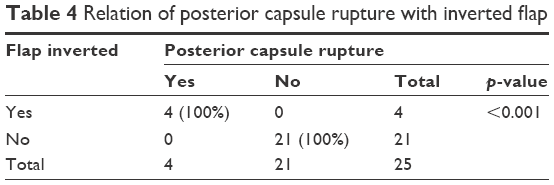 | Table 4 Relation of posterior capsule rupture with inverted flap |
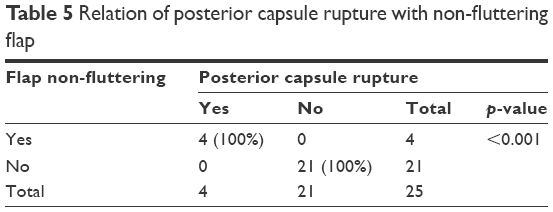 | Table 5 Relation of posterior capsule rupture with non-fluttering flap |
In all 4 cases with posterior extension of the tear with associated posterior capsule rupture, there is a correlation with the non-fluttering and everted nature of the flaps. Additionally, in all 21 cases of pre-equatorial tears with intact posterior capsule, the flaps are everted and fluttering. Nevertheless, the absence of inverted and non-fluttering flaps in these 21 cases indirectly validates the clinical correlation between the flap motility and posterior capsule rupture.
We provide videos of 3 cases of extended anterior capsular tears and the flap motility sign to ascertain its relationship to the extent of equatorial anterior capsular tears (Video S1).
Case 1
Capsulorhexis was completed with forceps. The nucleus was phacoemulsified by direct vertical chop technique. The nuclear core was separated and emulsified to debulk the nucleus. During the emulsification of the nuclear core, an extension in the rhexis was seen in the sub-incisional area. On careful evaluation, the flaps thus created by the tear in the anterior capsule were seen to be everted and fluttering with the fluidics in the anterior chamber. Phacoemulsification was continued taking care that the tear does not extend further. Maneuvers like nucleus rotation and chopping were carried out gently to avoid tear extension. During the procedure, a close vigil was kept on the nature of the flap. Nucleus emulsification was completed using safe phacoemulsification technique by dividing nuclear pieces into fully separated small pieces. The remaining cortex was removed with coaxial irrigation and aspiration handpiece. The flap continued to flutter and remained everted during the entire procedure. No extension of the tear to the posterior capsule was observed. A foldable intraocular lens (IOL) was implanted in the bag.
Case 2
This was a case of white intumescent cataract, and the presence of Argentinian flag sign was noted as soon as capsulorhexis was initiated. The capsulorhexis forceps was used to fashion a hemi-rhexis on both sides of capsular tears. The motility of flaps of tear in the anterior capsule was carefully observed and they were seen to be everted and fluttering with the fluidics in the anterior chamber. Phacoemulsification was continued and a close vigil was kept on the nature of the flap. Nucleus emulsification was completed using safe phacoemulsification technique by dividing nuclear pieces into completely separated small pieces with minimal force of separation. The cortex was removed with coaxial irrigation and aspiration handpiece. The flap continued to flutter and remained everted during the entire procedure. No extension of the tear onto the posterior capsule was observed.
Case 3
This was a case in which anterior capsular tear extended in to the posterior capsule resulting in posterior capsular rent. A difficulty was faced by the surgeon during capsulorhexis, and Vanna’s scissors and forceps were used for its completion. This caused an irregularity in the capsulorhexis margin at one place. During nuclear trenching, a radial anterior capsular tear occurred and soon it extended reaching close to equatorial area. The flaps created by the tear in the anterior capsule were seen to be everted and fluttering with the fluidics in the anterior chamber. However, fluttering of the flaps stopped as the nucleus was being divided into quadrants. Also, they had become inverted. At this stage, according to our hypothesis, a conversion to extracapsular extraction should have been done since the flap had extended beyond equator. However, phacoemulsification was continued. Further maneuvers led to the nucleus quadrant dropping into the vitreous. The PCR was visible at this stage suggestive of an extension onto the posterior capsule.
Discussion
Radial tears in the anterior capsular tears can occur during any stage of surgery such as during viscoelastic injection by the cannula, capsulorhexis, hydrodissection, phacoemulsification, irrigation/aspiration, movement of the second instrument, and IOL/iris prosthesis implantation.1 Marques et al observed capsulorhexis as the most frequent step during a surgery to have radial anterior capsular tears.1 The capsular tears occurred during capsulorhexis in 84% of our cases making it the most common step during surgery in our study.
Radial tears in capsulorhexis can be predisposed by various factors including shallow anterior chamber, weak zonules such as in coexisting pseudoexfoliation, previous inflammatory conditions, positive vitreous pressure, squeezing of eye intraoperatively, requirement of local anesthesia, intumescent cataracts, cataracts in pediatric age group with highly elastic anterior capsules, and handling of capsulorhexis by novice surgeons.3–14 In our study, majority of the cases with capsulorhexis tears had an ACD of <3 mm and were mature intumescent cataracts.
Peripheral extension of the radial tear in anterior capsulorhexis margin can cause serious complications if it travels beyond lens equator and into the posterior capsule. Although there are measures to rescue the tear extension including Little’s rescue technique, cystitome retrieval technique, rhexis restarting from the other side, tangential flap creation, and anterior localized zonulysis with flap rescue, the radial tear may still extend to the peripheral part of lens mostly due to an increase in intracapsular pressure.15–19
Radial tears do not cross the equator immediately in a significant number of cases because of the thickened mid periphery of anterior capsule and the barrier created by the zonular attachment to the anterior capsule.20 Nevertheless, radial tears can breach the barrier of equator during the course of emulsification or thereafter, and subsequently have complications such as posterior capsular tear, vitreous loss, insufficient capsular support for IOL implantation, and nuclear drop. Phaco-surgeons employ different maneuvers such as creating additional radial tears, performing supra-capsular phacoemulsification, using stable chamber settings, avoiding deep or shallow anterior chamber, and employing techniques that put minimal stress to the extended capsular flaps21–25 to prevent the extension of the tear beyond the equator onto the posterior capsule.26 Subsequently, the posterior capsular rupture rate varies depending upon the experience and the technique of the surgeon. In a Moorfields Eye Hospital study of anterior capsular tear extension, a high rate (24%) of posterior capsular rupture, with 5% nuclear drop and 11% requiring a secondary procedure, was reported.27 In a study by Marques et al, the incidence of extension of the anterior capsule to the posterior capsule through the equator was noted as ~52%.1
The intraoperative signs of posterior capsular rupture are the sudden deepening of the anterior chamber, pupillary snap sign, increased red glow, decreased followability, and nuclear tilt.28 However, these signs of posterior capsular rupture do not appear instantly after the extension of the tear onto the posterior capsule. Additionally, the time lag for appreciating the posterior capsular rupture may vary regardless of the experience of the surgeon. These deficiencies in recognizing the signs of radial tear of anterior capsule traveling beyond lens equator and causing a rent in the posterior capsule can lead to nucleus drop and its sequels.
We describe for the first time a surgical sign – flap motility sign – which clearly helps to ascertain the extent of a flap extension.
While performing phacoemulsification, if the extended flap of the capsulorhexis is everted and fluttering, it indicates that the flap has not extended beyond the equator. In such cases, phacoemulsification can be safely continued without a dilemma. Nevertheless, safe phacoemulsification techniques should be employed, as described earlier, and a close vigil has to be kept on the nature and motility of the flap as the tear can extend to the posterior capsule. If the extended flap becomes inverted on the nucleus and stops fluttering, it indicates the end point of safe phacoemulsification and denotes the extension of the flap beyond the equator onto the posterior capsule. In such situations, an instant decision to abort phacoemulsification and adopt extra-capsular cataract surgery or small incision cataract surgery helps to decrease the incidence of posterior capsular rupture.
The flap motility sign helps in deciding whether an IOL implantation is required. If the flaps are fluttering at the end of phacoemulsification surgery, IOL implantation can be done safely in the bag over the intact posterior capsule.
Conclusion
Based on our definite results, peripherally extended everted and fluttering flaps of the tears indicate that the radial tears have not extended beyond equator. Additionally, inverted and non-fluttering tears symbolize the extension of tear beyond equator.
Acknowledgments
This paper was presented as an abstract at the 74th Annual Conference (AIOC) of All India Ophthalmological Society, Kolkata, India; February 25–28, 2016. Dr Tushya Om Parkash now has a degree in MS Ophthalmology and is currently affiliated with Dr Om Parkash Eye Institute, Amritsar, India (as of July 11, 2017).
Disclosure
The authors report no conflicts of interest in this work.
References
Marques FF, Marques DMV, Osher RH, Osher JM. Fate of anterior capsule tears during cataract surgery. J Cataract Refract Surg. 2006;32(10):1638–1642. | ||
Mohammadpour M, Erfanian R, Karimi N. Capsulorhexis: pearls and pitfalls. Saudi J Ophthalmol. 2012;26(1):33–40. | ||
Corey RP, Olson RJ. Surgical outcomes of cataract extractions performed by residents using phacoemulsification. J Cataract Refract Surg. 1998;24(1):66–72. | ||
Saber H, Butler TJ, Cottrell DG. Resistance of the human posterior lens capsule and zonules to disruption. J Cataract Refract Surg. 1998;24(4):536–541. | ||
Assia EI, Apple DJ, Tsai JC, Lim ES. The elastic properties of the lens capsule in capsulorrhexis. Am J Ophthalmol. 1991;111(5):628–632. | ||
Prasad S. Phacoemulsification learning curve: experience of two junior trainer ophthalmologists. J Cataract Refract Surg. 1998(1);20:73–77. | ||
Seward HC, Dalton R, Davis A. Phacoemulsification during learning curve: risk/benefit analysis. Eye (Lond). 1993;7(Pt 1):164–168. | ||
Pingree MF, Crandall AS, Olson RJ. Cataract surgery complication in 1 year at an academic institution. J Cataract Refract Surg. 1999;25(5):705–708. | ||
Browining OJ, Cobo LM. Early experience in extracapsular cataract surgery by residents. Ophthalmology. 1985;92(12):1647–1653. | ||
Bianchi E, Scarinci F, Ripandelli G, et al. Retinal pigment epithelium, age-related macular degeneration and neurotrophic keratouveitis. Int J Mol Med. 2013;31(1):232–242. | ||
Taurone S, Ripandelli G, Pacella E, et al. Potential regulatory molecules in the human trabecular meshwork of patients with glaucoma: immunohistochemical profile of a number of inflammatory cytokines. Mol Med Rep. 2014;11(12):1384–1390. | ||
Fehér J, Kovács I, Pacella E, Radák Z. A mikrofl óra és a bélnyálkahártya kölcsönhatása az irritábilis bél, irritábilis szem és irritábilis elme szindróma kórtanában és kezelésében [Correlation of the microbiota and intestinal mucosa in the pathophysiology and treatment of irritable bowel, irritable eye, and irritable mind syndrome]. Orv Hetil. 2014;155(37):1454–1460. Hungarian. | ||
Pacella E, Collini S, Pacella F, Piraino DC, Santamaria V, De Blasi RA. Levobupivacaine vs racemic bupivacaine in peribulbar anaesthesia: a randomized double blind study in ophthalmic surgery. Eur Rev Med Pharmacol Sci. 2010;14(6):539–544. | ||
Pacella E, Pacella F, Troisi F, et al. Efficacy and safety of 0.5% levobupivacaine versus 0.5% bupivacaine for peribulbar anesthesia. Clin Ophthalmol. 2013;7:927–932. | ||
Little BC, Smith JH, Packer M. Little capsulorhexis tear-out rescue. J Cataract Refract Surg. 2006;32(9):1420–1422. | ||
Karim SMR, Ong CT, Miah MR, Sleep T, Hanifudin A. A novel technique of rescuing capsulorhexis radial tear-out using a cystotome. J Vis Exp. 2011;47:2317. | ||
Franchini A. The rhexis: errant, compromised, or smaller or larger than planned. Cataract & Refractive Surgery Today. 2012;3:35–38. | ||
Mohammadpour M. Rescue of an extending capsulorrhexis by creating a midway tangential anterior capsular flap: a novel technique in 22 eyes. Can J Ophthalmol. 2010;45(3):256–258. | ||
Page TP. Anterior zonulotomy: rescue technique for capsulorhexis tear-out. J Cataract Refract Surg. 2015;41(10):2036–2039. | ||
Assia EI, Apple DJ, Tsai JC, Morgan RC. Mechanism of radial tear formation and extension after anterior capsulectomy. Ophthalmology. 1991;98(4):432–437. | ||
Colvard DM. Radial anterior capsular tear causes and management. Cataract & Refractive Surgery Today. 2009;10:83–84. | ||
Alio JL, Mulet ME, Shalaby AM, Attia WH. Phacoemulsification in the anterior chamber. J Cataract Refract Surg. 2002;28(1):67–75. | ||
Osher RH, Barros MG, Marques DM, Marques FF, Osher JM. Early uncorrected visual acuity as a measurement of the visual outcomes of contemporary cataract surgery. J Cataract Refract Surg. 2004;30(9):1917–1920. | ||
Ocular Surgery News U.S Edition. Complications from anterior capsule tears may require secondary intervention. Available from: http://www.healio.com/ophthalmology/cataract-surgery/news/print/ocular-surgery-news/%7B13f27d61-f984-4a1e-a4de-a917065a208b%7D/complications-from-anterior-capsule-tears-may-require-secondary-intervention. Accessed January 21, 2017. | ||
Reus NJ. Management of anterior and posterior capsular tears. Cataract & Refractive Surgery Today.2011;7:38–40. | ||
Vajpayee RB, Sharma N, Dada T, Gupta V, Kumar A, Dada VK. Management of posterior capsule tears. Surv Ophthalmol. 2001;45(6):473–488. | ||
Carifi G, Miller MH, Pitsas C, et al. Complications and outcomes of phacoemulsification cataract surgery complicated by anterior capsule tear. Am J Ophthalmol. 2015;159(3):463–469. | ||
Rani N, Gupta P. Posterior capsular rent: risk factors, diagnosis and management. Surg Sci. 2014;5(5):224–226. |
Supplementary material
|
Video S1 Flap motility sign. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.