")
Back to Journals » Patient Preference and Adherence » Volume 13
Fixed Versus Free Combinations Of Antihypertensive Drugs: Analyses Of Real-World Data Of Persistence With Therapy In Italy
Authors Putignano D , Orlando V , Monetti VM , Piccinocchi G, Musazzi UM , Piccinocchi R, Minghetti P , Menditto E
Received 31 July 2019
Accepted for publication 15 October 2019
Published 11 November 2019 Volume 2019:13 Pages 1961—1969
DOI https://doi.org/10.2147/PPA.S225444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Daria Putignano,1 Valentina Orlando,1 Valeria Marina Monetti,1 Gaetano Piccinocchi,2 Umberto Maria Musazzi,3 Roberto Piccinocchi,4 Paola Minghetti,3 Enrica Menditto1
1CIRFF, Center of Pharmacoeconomics, University of Naples Federico II, Naples, Italy; 2SIMG, Società Italiana di Medicina Generale, Florence, Italy; 3Dipartimento di Scienze Farmaceutiche, Università degli Studi di Milano, Milan, Italy; 4University of Naples Federico II, Naples, Italy
Correspondence: Valentina Orlando
CIRFF, Center of Pharmacoeconomics, University of Naples Federico II, Via Domenico Montesano 49, Naples 80131, Italy
Tel +39 081 678657
Fax +39 081 678303
Email [email protected]
Purpose: To analyse the pattern of use and cost of antihypertensive drugs in new users in an Italian population, and explore the patient/treatment factors associated with the risk of therapy discontinuation.
Patients and methods: In this retrospective study, information was collected from a population-based electronic primary-care database. Persistence with medication use 1 year from therapy initiation was evaluated for each user using the gap method. Each new user was classified according to his/her pattern of use as: “continuer”, “discontinuer” “switching” or “add-on”. A Cox regression model was used to analyse the factors influencing therapy discontinuation. Primary-care costs comprised specialists’ visits, diagnostic procedures and pharmacologic therapies.
Results: Among 14,999 subjects included in persistence analyses, 55.1% of cases initially started on monotherapy were classified as discontinuers vs 36.5% of cases taking combination therapy (42.3% vs 32.7%, respectively, for free and fixed combinations, P < 0.01). Old age, high cardiovascular risk and being in receipt of fixed-combination therapy were associated with greater persistence. Overall, the primary-care cost/person/year of hypertension management was ∼€95.3 (IQR, 144.9). The monotherapy cost was €88 per patient (IQR, 132.9), and that for combination therapy was €151±148.3. The median cost/patient with a fixed combination was lower than that for a free combination (€98.4 (IQR, 155.3) and €154.9 (IQR, 182.6), respectively).
Conclusion: The initial type of therapy prescribed influences persistence. Prescribing fixed combinations might be a good choice as initial therapy.
Keywords: drug-utilization, adherence, fixed combination, hypertension
Introduction
Hypertension affects 31.1% of the global population (1.4 billion people) and results in 9.4 million deaths every year.1,2 Pharmacologic treatment can be very successful with the potential to reduce blood pressure (BP) to recommended levels in almost all patients (<140/90 mmHg or <130/80 mmHg for patients with diabetes mellitus or chronic kidney disease). Monotherapy fails to control BP in ~50% of patients. Hence, national and international guidelines suggest starting therapy with combinations of more than one antihypertensive drug, which increases the complexity of the therapeutic regimen.3
Therapy using a combination of antihypertensive drugs offers an advantage over monotherapy (at least in part) due to the: (i) different sites of action of each drug; (ii) lower risk of adverse events. It is important for patients to take their medications appropriately and continue to take them long term.4 However, poor adherence and persistence in taking medications are common problems in hypertensive patients, partly because of complex treatment regimens and high pill burdens. These factors result in sustained periods of uncontrolled hypertension, leading to disease progression and the associated economic consequences.
Various strategies have been implemented to improve compliance with drug regimens. A combination of two pharmacologic agents in a single medicinal product has been available for hypertension therapy since the mid-1960s. Nowadays, numerous fixed-dose combinations (hereafter termed “fixed combinations”) are available for the treatment of hypertension and other chronic diseases with high risks for morbidity and mortality.5,6
In recent years, fixed combinations have acquired an important role in hypertension management.7–9 Guidelines set in 2018 by the European Society of Hypertension (ESH)/European Society of Cardiology (ESC) stated that fixed combinations can be used as first as well as second-line therapies to achieve the recommended BP target.3 More than 27 fixed combinations are available for daily use in Italy. Of these, 18 consist of an angiotensin-converting enzyme inhibitor (ACEI) and a diuretic or calcium-channel blocker (CCB); 9 consist of an angiotensin-receptor blocker (ARB) and a diuretic or a CCB.
Data on pharmacy claims have been suggested to be powerful tools to analyze compliance with antihypertensive therapy.10,11 However, studies that evaluate the therapeutic approach to hypertension in primary care in Italy are lacking.
We investigated the prescription patterns for hypertensive patients in a real-world practice and whether drug combinations improve persistence with drug therapy. Furthermore, we discussed some aspects related to legal authorization of fixed combinations.
Materials And Methods
Study Design And Data Sources
This was a retrospective cohort study on the pattern of use of antihypertensive drugs in primary-care settings in the Campania region of southern Italy. The study was carried out according to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Data were retrieved from a population-based database for general practitioners (COMEGEN Social Cooperative Society) which oversees ~190,000 subjects.12 All participating general practitioners use the same software to record data during their daily practice, and receive formal and periodic training for data entry (Millewin; Millenium Dedalus, Florence Italy). For the present study, data were retrieved using an encrypted patient code linking demographic details with medical diagnoses, drug prescriptions, diagnostic tests (with their relevant values) and date of death. All diagnoses were coded according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Drugs were coded according to the Anatomical Therapeutic Chemical (ATC) Classification System (ATC/Defined Daily Doses methodology). The influence of dosage forms was not the focus of our study. The term “pill”, even though it is not a standard term employed by the European Directorate for the Quality of Medicines, was used to identify the solid oral dosage forms used by patients regardless the type of pharmaceutical dosage form (e.g., tablets, capsules) or release profile (e.g., immediate, prolonged).13
The quality characteristics of this data source have been described.14 COMEGEN has been used to provide drug-utilization information and to undertake studies.15–19 This automated system is anonymous so, according to the Italian Data Protection Authority, neither Ethical Committee approval nor informed consent were required for our study.20 Our research protocol adhered to the tenets of the Declaration of Helsinki and its amendments.
Case Definitions
All patients with at least one prescription of an antihypertensive drug were defined as “users” or “cases”. Antihypertensive drugs were classified as belonging to C03 (diuretics), C07 (beta-blockers), C08 (CCBs), C09 (agents acting on the renin–angiotensin system) groups of the ATC Classification System.
The target population was classified into two groups: “prevalent” cases and “incident” cases (cases with no antihypertensive prescriptions during the 365 previous days). The index date was the date of the first prescription.
The study period was from 1 January 2010 to 31 December 2015. The year 2010 was the reference for selecting incident cases with an index prescription in 2011. 2011–2014 was the “recruitment” period of the study population (identification of prevalent cases and incident cases). The year 2015 was used to follow-up incident cases with an index prescription in 2014.
Outcomes
The first prescriptions for incident cases were analyzed. To identify the first-line therapeutic approach, the number and type of antihypertensive drugs were recorded, and incident cases in monotherapy and combination therapy were identified. That is: cases in monotherapy receiving a prescription of only one drug, including diuretics (ATC: C03), beta-blockers (ATC: C07), CCBs (ATC: C08), ACEIs (ATC: C09AA), angiotensin II receptor antagonists (ATC: C09CA); cases in fixed-combination therapy receiving products belonging to C07BB, C07CB, C07FB, C09BA, C09BB, C09DA, or C09DB ATC subgroups (Appendix); cases in free-combination therapy receiving two drugs belonging to C03 and/or C07 and/or C08 and/or C09AA and/or C09CA ATC groups; cases in “multiple mix” combinations receiving two or more fixed combinations belonging to C09BA, C09BB, C09DA or C09DB ATC subgroups and/or and free combinations of two or more drugs belonging to C03 and/or C07 and/or C08 and/or C09AA and/or C09CA ATC groups.
Concomitant therapy with anti-diabetes agents (ATC: A10), lipid‐lowering drugs (ATC: C10), antiplatelets (ATC: B01AC) and hospitalizations for the diagnosis of acute myocardial infarction (ICD 9 CM: 410–414), congestive heart failure (ICD 9CM: 428) and cerebrovascular disease (ICD 9 CM: 430–438) were analyzed.
Medication Persistence 1 year after therapy initiation was evaluated according to the International Society of Pharmacoeconomics and Outcome Research definition21 Recently, the European Society of Patient Adherence and Compliance developed a Taxonomy of Adherence. This defines medication adherence “as the process by which patients take their medication as prescribed” and subdivides adherence into three essential elements to capture the sequence of events that must occur for a patient to experience the optimal benefit from his/her prescribed treatment regimen: initiation, implementation, and discontinuation. The present study focused on the discontinuation phase (medication persistence)22 Medication persistence was assessed using the gap method. A gap was defined as the period during which no medication is available to the patient. A user of antihypertensive drugs was considered to be a “discontinuer” if a gap of >60 days between two prescriptions was recorded. The number of days of available medication (days of therapy) was estimated based on the pill number. These assumptions are based on studies undertaken on antihypertensive drugs in an identical setting.23,24 Only the number of days of therapy from the prescription dispensed most recently was used to evaluate the gap. Subjects were censored if the gap allowed was exceeded without purchasing a new prescription or upon reaching the end of the follow-up period (365 days after the index date). As described by Halpern and colleagues25 persistence in the separated-drugs cohort was assessed as “therapy persistence” (i.e., continuation with any antihypertensive medication was sufficient to be considered as persistent).
Each incident user was classified according to his/her pattern of use as: “continuer”, “discontinuer”, “switching” or “add-on”. A “spot user” (only one prescription during the study period) and multiple mix (due to the complexity of the regimen) were excluded from the analysis of persistence.
Cost Analyses
Cost analyses were carried out on incident cases. The methodology used for cost assessment was bottom–up because this methodology values each cost component for an individual patient. This approach enabled statistical analyses aimed at the detection of cost differences among patients and among cost components. For each type of therapy, primary-care costs were expressed as the cost of hypertension management per person year of follow-up. They included specialists’ visits, diagnostic procedures, laboratory costs, and pharmacologic therapies quantified according to the Italian National Health Service (NHS) by means of charges pertaining in 2015.
Cost analyses were conducted from the perspective of the third-party payer, the NHS which, in Italy is in charge of financing and providing healthcare services.
Costs are expressed in terms of median patient cost/year, and interquartile range (IQR), stratified by the first-line approach (monotherapy; free combination; fixed combination). The total cost was computed as the sum of the different cost items (drugs, visits, procedures). Values were expressed in Euros at the time of the analyses.
Statistical Analyses
Data are the mean ± standard deviation for continuous variables or as absolute and relative frequencies for categorical variables. The chi-square test and analysis of variance were undertaken to determine the difference between categorical and continuous variables. Cox regression models estimated the likelihood of non-persistence over 1 year after therapy initiation, and evaluated the factors influencing the probability of discontinuation. Hazard ratios (HRs) and 95% confidence intervals (95%CIs) were calculated to assess crude and adjusted associations for all covariates.
Cost data were skewed, and the nonparametric Kruskal–Wallis test was used to examine significant differences in median values across different therapy categories.
Data management was undertaken with SQL server v2018 (Microsoft, Redmond, WA, USA). Analyses were carried out using SPSS v17.1 (IBM, Armonk, NY USA). P < 0.05 was considered significant.
Results
During the study period, 46,482 subjects were identified as chronic users of antihypertensive drugs (prevalent cases). Overall, 18,504 (44.8% male) were incident cases. Appendix Table 1 shows the main characteristics of the cohort. For the overall cohort, the mean BP was 143±18.7/87±11.1 mmHg. Also, 4474 subjects (24.2% of incident cases) were also taking lipid‐lowering drugs and 4027 (21.8% of incident cases) were also taking antiplatelets. The most used first-line therapeutic approach was monotherapy (67.0% of subjects): 31.4% of cases in monotherapy began with an ACEI, 25.8% with beta-blockers, 18.1% with diuretics and 24.7% with ARBs or CCBs. Among subjects starting combination therapy, fixed combinations were the most used (60.0%).
During the 12 months after the index prescription, 51.8% of incident cases, of the total cohort, discontinued the initial treatment, 19.3% remained with the same antihypertensive drug, 20.2% switched to another antihypertensive drug, and 8.6% received prescriptions for a new drug in addition to the initial therapy (Appendix Table 1).
We found that 14,999 subjects (excluding spot therapy and multiple-mix therapy) were included in the persistence analysis. Overall, 55.1% of cases with initial monotherapy were classified as discontinuers vs 36.5% of cases in combination therapy (p < 0.001).
Among subjects starting with combination therapy, the highest percentage of discontinuers was for free combinations (42.3%) compared with fixed combinations (32.7%) (p < 0.01) (Figure 1).
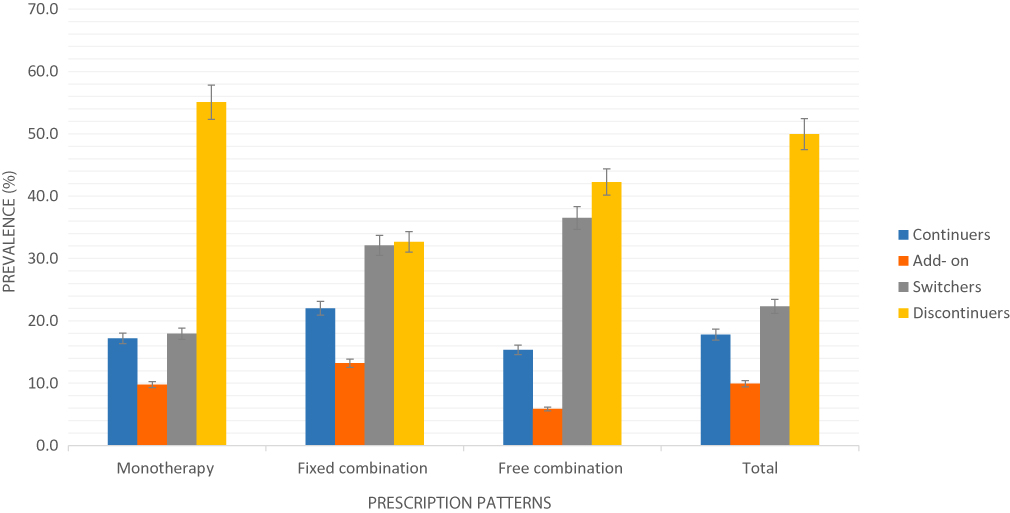 |
Figure 1 Pattern of persistence with monotherapy, fixed dose and free combination (prevalence, 95%CI). |
Cox regression analysis (Appendix Table 2) shows that subjects in combination therapy were less likely to be non-persistent compared with those in monotherapy. In particular, subjects in free-combination therapy were ~17% less likely to have a period of discontinuation, and subjects in fixed-combination therapy were ~43% less likely to be non-persistent (free combination: HR, 0.83 [95%CI 0.77–0.90]; fixed combination: 0.57, 0.54–0.61). With increasing age, the risk of non-persistent therapies increased (40–49 years: HR, 0.74 [95%CI 0.69–0.80]; 50–59 years: 0.71, 0.66–0.76; 60–69 years: 0.64, 0.59–0.69; 70–79 years: 0.62, 0.57–0.67; 80 years: 0.68, 0.62–0.75); concomitant treatment with lipid‐lowering drugs and/or antiplatelet therapy decreased the risk of non-persistence with therapy (0.83, 0.78–0.88; 0.75, 0.71–0.80) (Appendix Table 2).
Overall, the primary-care costs per person per year of hypertension management were estimated to be €95.3 (IQR, 144.9). On average, monotherapy cost €88 per patient (IQR, 132.9), whereas combination therapy cost €151±148.3. The median cost per patient with a fixed combination was lower than that of a patient with a free combination, €98.4 (IQR, 155.3) and €154.9 (IQR, 182.6), respectively. Figure 2 shows median costs stratified by persistence patterns. Stratification of total costs, according to the pattern of persistence and the prescribed combination (fixed vs free), showed that patients changing therapy in the follow-up period (add-on and switchers) had the highest direct costs for both combinations, followed by the continuers for the fixed combination and discontinuers for the free combination.
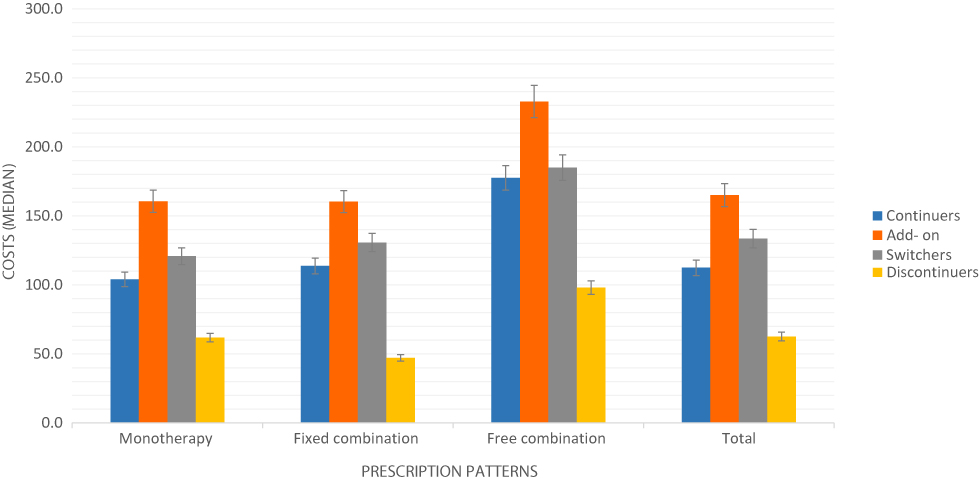 |
Figure 2 Annual primary-care costs (median and IQR) by drug cohort and persistence category. |
Discussion
This retrospective cohort study elicited several important findings. ESH/ESC 2018 guidelines emphasize that monotherapy can reduce BP values efficaciously in a limited number of patients, and that most of them require the association of at least two drugs to achieve BP control.3 Our results showed that monotherapy was the most used first-line therapeutic approach (72.5% of incident cases). We found that 27.5% of incident cases were in combination therapy, and this was probably due to excessive confidence in the efficacy of monotherapy, with consequent scarce and insufficient use of combination therapy in the hypertensive population.26
In the present study, ACEIs were the most used drugs in monotherapy, a finding that is consistent with the literature.27 Indeed, studies have suggested that patients initiated on ACEIs and beta-blockers have slightly better BP control.28
We showed that 50.0% of the study population discontinued their initial treatment within 1 year, whereas 22% of patients switched to another drug class during the same period. Suboptimal adherence to medication-taking is frequent in real-world practices: usually, ~50% of all prescribed medications for chronic diseases are not taken as prescribed.29,30
Focusing research on adherence to treatment is very much a research focus currently.31,32 The factors underlying the lack of adherence to therapy are many and varied.33,34 They are related to physicians’ behavior or to the willingness of the patients to follow the prescriptions or to the characteristics of the drugs (which are sometimes impediments to correct long-term treatment).35,36
With regard to factors related to patients, concerns about medications and their adverse effects should be noted, as well as a lack of knowledge of their own disease and the presence of comorbidities, which are accentuated in the presence of socio-economic and psychological/cognitive limitations.37–41 Moreover, factors related to therapy, such as complexity and multiple medications, must be taken into account.
We showed that patients taking combination therapy were less likely to be non-persistent compared with those in monotherapy. These results are in accordance with data from other studies carried out with the same methodology in Italian settings.42,43 Interestingly, among subjects taking combination therapy, a higher percentage of subjects in free combination were discontinuers (42.3%) compared with those in fixed combination (32.7%) (P < 0.01). The persistence of patients with regard to antihypertensive therapy may decrease with an increasing number of drugs in multiple pill regimens. Furthermore, better persistence has been associated with old age and greater cardiovascular risk. The most persistent subjects were those who received antiplatelets and/or lipid‐lowering drugs together with antihypertensive agents. That is, greater persistence seems to be associated with greater awareness of the risks related to the disease.
Fixed combinations have been developed to reduce the pill burden for hypertensive patients. According to the European regulatory framework, a fixed combination is a medicinal product which contains at least two active substances combined to improve the therapeutic efficacy or safety profiles in comparison with monotherapy44 In this context, fixed combinations can be classified according to three therapeutic goals: (a) add-on treatment of patients whose disease is not controlled by existing therapies; (b) substitution therapies in monitored patients to simplify the multiple-drug daily regimen; (c) initial combination therapies for treatment-naïve patients.
If the drug substances contained in a fixed combination are not new, an abridged (or hybrid) application can be followed to achieve the marketing authorization. In this light, the authorization dossier is simplified. A full characterization of physicochemical and technologic properties must be provided to support the quality of the fixed combination.
However, the preclinical and clinical data required by regulatory agencies vary based on the complexity of assessment of the efficacy–safety balance of the new drug product (in addition to the established scientific and clinical knowledge). Indeed, according to article 10b of Directive 2001/83/EC, in the case of a fixed combination for add-on treatments or treatments containing drug substances already present in authorized medicinal products but not hitherto used in combination for therapeutic purposes (e.g., initial combination therapies), the applicant must include in the dossier the results of preclinical or clinical studies to support the pharmacologic and medical rationale of the combination and to determine the benefit–risk balance on the basis of the desired therapeutic effect. In the case of add-on treatment, the superiority of fixed combinations compared with monotherapies should be demonstrated. However, preclinical and clinical studies on individual drug substances should not be provided because data can be derived from already authorized medicinal products. Conversely, if the drug substances are already being used in clinical practice as free-combination or fixed-combination products (e.g., substitution therapies), the preclinical and clinical studies required may be simplified significantly and based on demonstration of therapeutic equivalence. Indeed, bioequivalence studies vs the free-combination or fixed-combination originator can be accepted. Such studies are fundamental to support substitution of monotherapies with fixed combinations.
Comparative efficacy studies of treatment strategies using antihypertensive therapeutic classes in hypertension control in primary care showed that patients beginning antihypertensive therapy with a fixed combination had significantly greater reductions in BP than patients initiated on a free combination or monotherapy.34 By reducing the overall pill burden and simplifying medication regimens, fixed combinations have been shown to improve medication compliance and medication persistence in several studies.45–51 A recent retrospective cohort study carried out in Canada showed that patients taking a fixed combination had greater rates of medication adherence than the free-combination group (70% vs 42%, P < 0.01) and a significantly lower risk of composite clinical outcomes, which may have been related to better adherence to therapy.44
We also evaluated the primary-care costs of fixed and free combinations. After 12-month follow-up, the fixed-combination group had an annual mean cost per patient lower than free combinations. Furthermore, for both drug combinations, patient-changing therapy was the most expensive. This reduction in healthcare costs is consistent with the results observed in other reports. In a meta-analysis comparing annual healthcare costs of fixed vs free equivalent combination regimens for hypertension treatment, Sherrill et al estimated a $2039 reduction in all-cause total costs and a $709 reduction in hypertension- and cardiovascular-related costs in the fixed-combination group.52
Combination therapy with a fixed combination may be less costly than if the drugs are administered separately. Furthermore, recently many fixed combinations have become available as generic formulations in Italy, and this may encourage the use of the drugs used in fixed combinations.
Strengths And Limitations Of Our Study
Our study was conducted in >170,000 subjects and covered a 5-year period. Only subjects living in the Campania region and receiving prescriptions from general practitioners belonging to the COMEGEN Medical Association were included in analyses, so prescribing patterns may not be fully representative of those in Italy. For assessment of persistence, patients with at least one discontinuation episode were considered to be non-persistent. However, an intrinsic limitation of retrospective analyses of databases (such as COMEGEN) is that tracking the reason for the discontinuation is not possible, such as whether discontinuation was recommended by the clinician (e.g., a temporary suspension due to an adverse reaction). Also, pharmacy-refill records provide details only on whether patients were dispensed their medication, and do not provide details on whether patients ingested their medications.
Healthcare databases can be used to support evaluation of the use of drugs in real-world practice allowing tracing (over time) of their type, mode and use. In particular, through pharmaceutical prescriptions, it was possible to trace the profiles of persistence to pharmacologic therapies.
Some factors not included in our analyses, such as governmental regulation of prescribing, as well as monitoring the drug-expenditure budget of general practitioners and the pharmaceutical industry, could influence the prescriber’s choice of therapeutic regimen. In addition, it was not possible to assess the costs of hospital admission or indirect costs because such information was scarce or not available.
Conclusions
Our retrospective study presented the real-world results of different regimens for hypertension treatment. We found that use of a fixed combination improved persistence and decreased healthcare costs compared with use of free combinations. Use of a fixed combination provided an important opportunity to improve the quality of hypertension treatment. Therefore, it is reasonable for physicians, pharmacists and regulatory agencies to facilitate use of fixed combinations for patients who need to take two or more antihypertensive drugs. Nevertheless, the improvement of persistence is a complex problem requiring a multifactorial strategy, and simplification of therapy with fixed formulations is a crucial aspect.
Acknowledgement
The authors thank the editors of Charlesworth Author Services for English-language editing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. A Global Brief on Hypertension. Geneva: World Health Organization; 2013.
2. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e92. doi:10.1161/01.cir.0000441139.02102.80
3. Williams B, Mancia G, Spiering W, et al. ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104.
4. Jamerson K, Weber MA, Bakris GL, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008;359(23):2417–2428. doi:10.1056/NEJMoa0806182
5. Burnier M. Antihypertensive combination treatment: state of the art. Curr Hypertens Rep. 2015;17(7):51. doi:10.1007/s11906-015-0562-0
6. Blonde L, San Juan ZT, Bolton P. Fixed-dose combination therapy in type 2 diabetes mellitus. Endocr Pract. 2014;20(12):1322–1332. doi:10.4158/EP14259.RA
7. Bramlage P, Schmidt S, Sims H. Fixed-dose vs free-dose combinations for the management of hypertension - an analysis of 81 958 patients. J Clin Hypertens. 2018;20(4):705–715. doi:10.1111/jch.2018.20.issue-4
8. Corrao G, Nicotra F, Parodi A, et al. Cardiovascular protection by initial and subsequent combination of antihypertensive drugs in daily life practice. Hypertension. 2011;58(4):566–572. doi:10.1161/HYPERTENSIONAHA.111.177592
9. Gradman AH, Parise´ H, Lefebvre P, et al. Initial combination therapy reduces the risk of cardiovascular events in hypertensive patients: a matched cohort study. Hypertension. 2013;61:309–318. doi:10.1161/HYPERTENSIONAHA.112.201566
10. Qvarnström M, Kahan T, Kieler H, et al. Persistence to antihypertensive drug classes: a cohort study using the Swedish Primary Care Cardiovascular Database (SPCCD). Costa E, Giardini A, Monaco A, editors. Medicine (Baltimore). 2016;95(40):e4908. doi:10.1097/MD.0000000000004908
11. Menditto E, Orlando V, Malo S, et al. Measuring medication adherence in health-related databases. In: Adherence to Medical Plans for Active and Healthy Ageing. NY, USA: Nova Science Publisher, Inc.; 2017:189–206.
12. Cammarota S, Bruzzese D, Sarnelli G, et al. Proton pump inhibitors prescribing following the introduction of generic drugs. Eur J Clin Invest. 2012;42(10):1068–1078. doi:10.1111/eci.2012.42.issue-10
13. EDQM. Standard terms. Available from: https://standardterms.edqm.eu/.
14. Carey IM, Cook DG, De Wilde S, Bremner SA, Richards N, Caine S. Developing a large electronic primary care database (Doctors’ Independent Network) for research. Int J Med Inform. 2004;73:443–453. doi:10.1016/j.ijmedinf.2004.02.002
15. Iolascon G, Gimigliano F, Moretti A, et al. Rates and reasons for lack of persistence with anti-osteoporotic drugs: analysis of the Campania region database. Clin Cases Min Bone Metab. 2016;13(2):127.
16. Orlando V, Guerriero F, Putignano D, et al. Prescription patterns of antidiabetic treatment in the elderly. Results from Southern Italy. Curr Diabetes Rev. 2016;12(2):100–106. doi:10.2174/1573399811666150701120408
17. Casula M, Catapano AL, Piccinelli R, et al. Assessment and potential determinants of compliance and persistence to antiosteoporosis therapy in Italy. Am J Man Care. 2014;20(5):e138–e145.
18. Putignano D, Bruzzese D, Orlando V, et al. Differences in drug use between men and women: an Italian cross sectional study. BMC Women’s Health. 2017;17(1):73. doi:10.1186/s12905-017-0424-9
19. Iolascon G, Gimigliano F, Orlando V, et al. Osteoporosis drugs in real-world clinical practice: an analysis of persistence. Aging Clin Exp Res. 2013;25(1):137–141. doi:10.1007/s40520-013-0127-5
20. Italian Data Protection Authority. General authorisation to process personal data for scientific research purposes - 1 March 2012 [1884019].
21. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
22. De Geest S, Zullig L, Dunbar-Jacob J. Adherence Reporting Guideline EMERGE. ESPACOMP medication adherence reporting guideline (EMERGE). Ann Intern Med. 2018;169:30–35. doi:10.7326/M18-0543
23. Malo S, Aguilar-Palacio I, Feja C, et al. Different approaches to the assessment of adherence and persistence with cardiovascular-disease preventive medications. Curr Med Res Opin. 2017;33(7):1329–1336. doi:10.1080/03007995.2017.1321534
24. Menditto E, Cahir C, Aza-Pascual-Salcedo M, et al. Adherence to chronic medication in older populations: application of a common protocol among three European cohorts. Patient Pref Adhere. 2018;12:1975. doi:10.2147/PPA.S164819
25. Halpern MT, Khan ZM, Schmier JK, et al. Recommendations for evaluating compliance and persistence with hypertension therapy using retrospective data. Hypertension. 2006;47(6):1039–1048. doi:10.1161/01.HYP.0000222373.59104.3d
26. Ruzicka M, Leenen FH. Monotherapy versus combination therapy as first line treatment of uncomplicated arterial hypertension. Drugs. 2001;61(7):943–954. doi:10.2165/00003495-200161070-00004
27. Elliott WJ, Plauschinat CA, Skrepnek GH, et al. Persistence, adherence, and risk of discontinuation associated with commonly prescribed antihypertensive drug monotherapies. J Am Board Fam Med. 2007;20(1):72–80. doi:10.3122/jabfm.2007.01.060094
28. Bronsert MR, Henderson WG, Valuck R, et al. Comparative effectiveness of antihypertensive therapeutic classes and treatment strategies in the initiation of therapy in primary care patients: a Distributed Ambulatory Research in Therapeutics Network (DARTNet) study. J Am Board Fam Med. 2013;26(5):529–538. doi:10.3122/jabfm.2013.05.130048
29. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;20(11):CD000011.
30. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125(9):882–887. doi:10.1016/j.amjmed.2011.12.013
31. Illario M, Vollenbroek-Hutten M, Molloy DW, et al. Active and healthy ageing and independent living. J Aging Res. 2015;2015:542183. doi:10.1155/2015/542183
32. Illario M, Vollenbroek-Hutten MM, Molloy DW, et al. Active and healthy ageing and independent living 2016. J Aging Res. 2016;2016:8062079. doi:10.1155/2016/8062079
33. Giardini A, Martin MT, Cahir C, et al. Toward appropriate criteria in medication adherence assessment in older persons: position paper. Aging Clin Exp Res. 2016;28(3):371–381. doi:10.1007/s40520-015-0435-z
34. Costa E, Giardini A, Savin M, et al. Interventional tools to improve medication adherence: review of literature. Patient Pref Adhere. 2015;9:1303–1314. doi:10.2147/PPA.S87551
35. Sokol MC, McGuigan KA, Verbrugge RR, et al. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43(6):521–530. doi:10.1097/01.mlr.0000163641.86870.af
36. Cilurzo F, Musazzi UM, Franzè S, Selmin F, Minghetti P. Orodispersible dosage forms: biopharmaceutical improvements and regulatory requirements. Drug Disc Today. 2018;23(2):251–259. doi:10.1016/j.drudis.2017.10.003
37. Kronish IM, Ye S. Adherence to cardiovascular medications: lessons learned and future directions. Prog Cardiovasc Dis. 2013;55(6):590–600. doi:10.1016/j.pcad.2013.02.001
38. Newby LK, LaPointe NM, Chen AY, et al. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation. 2006;113(2):203–212. doi:10.1161/CIRCULATIONAHA.105.505636
39. Menditto E, Guerriero F, Orlando V, et al. Self-assessment of adherence to medication: a case study in Campania region community-dwelling population. J Aging Res. 2015;2015:682503. doi:10.1155/2015/682503
40. Scala D, Menditto E, Armellino MF, et al. Italian translation and cultural adaptation of the communication assessment tool in an outpatient surgical clinic. BMC Health Serv Res. 2016;16(1):163. doi:10.1186/s12913-016-1411-9
41. Sultana J, Musazzi UM, Ingrasciotta Y, et al. Medication is an additional source of phosphate intake in chronic kidney diseases patients. Nutr Metab Cardiovasc Dis. 2015;25:959–967. doi:10.1016/j.numecd.2015.06.001
42. Perrone V, Veronesi C, Gambera M, et al. Treatment with free triple combination therapy of atorvastatin, perindopril, amlodipine in hypertensive patients: a real- world population study in Italy. High Blood Press Cardiovasc Prev. 2019. doi:10.1007/s40292-019-00336-2
43. Degli Esposti E, Sturani A, Di Martino M, et al. Long-term persistence with antihypertensive drugs in new patients. J Hum Hypertens. 2002;16(6):439–444. doi:10.1038/sj.jhh.1001418
44. EMA. Guideline on clinical development of fixed combination medicinal products. London, 23 March 2017. EMA/CHMP/158268/2017 Committee for Human Medicinal Products (CHMP).
45. Gupta AK, Arshad S, Poulter NR. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: a meta-analysis. Hypertension. 2010;55(2):399–407. doi:10.1161/HYPERTENSIONAHA.109.139816
46. Verma AA, Khuu W, Tadrous M, et al. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: a population-based retrospective cohort study. PLoS Med. 2018;15(6):e1002584. doi:10.1371/journal.pmed.1002584
47. Webster R. Fixed-dose combination medications for non-communicable diseases. Heart. 2019;105(3):176–177. doi:10.1136/heartjnl-2018-313859
48. Reinhold K, Jurgen S, Antonios D. Single-pill triple fixed dose combination therapy with single component drug monitoring in treatment-resistant hypertension: a pilot study. Curr Vasc Pharmacol. 2018;16(2):197–203. doi:10.2174/1570161115666170821155555
49. Du LP, Cheng ZW, Zhang YX, et al. The impact of fixed-dose combination versus free-equivalent combination therapies on adherence for hypertension: a meta-analysis. J Clin Hypertens. 2018;20(5):902–907. doi:10.1111/jch.13272
50. Schulz M, Krueger K, Schuessel K, et al. Medication adherence and persistence according to different antihypertensive drug classes: a retrospective cohort study of 255,500 patients. Int J Cardiol. 2016;220:668–676. doi:10.1016/j.ijcard.2016.06.263
51. Grimmsmann T, Himmel W. Comparison of therapy persistence for fixed versus free combination antihypertensives: a retrospective cohort study. BMJ Open. 2016;6:e011650. doi:10.1136/bmjopen-2016-011650
52. Sherrill B, Halpern M, Khan S, et al. Single-pill vs free‐equivalent combination therapies for hypertension: a meta‐analysis of health care costs and adherence. J Clin Hypertens. 2011;13(12):898–909. doi:10.1111/jch.2011.13.issue-12
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.