")
Back to Journals » OncoTargets and Therapy » Volume 12
First-line treatment of women with advanced ovarian cancer: focus on bevacizumab
Authors Marchetti C, Muzii L, Romito A, Benedetti Panici P
Received 12 September 2018
Accepted for publication 27 December 2018
Published 8 February 2019 Volume 2019:12 Pages 1095—1103
DOI https://doi.org/10.2147/OTT.S155425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Claudia Marchetti, Ludovico Muzii, Alessia Romito, Pierluigi Benedetti Panici
Department of Gynecological-Obstetrical and Urological Sciences, Sapienza University of Rome, Rome, Italy
Abstract: Ovarian cancer is the fifth most common cause of cancer death in women in Europe. Despite the progress, almost 70% of the patients relapse. The standard treatment is cytoreductive surgery followed by platinum-taxane chemotherapy; in patients with a disseminated disease, one option is neoadjuvant chemotherapy with delayed surgery (ie, interval debulking surgery). The most important change in the last decades involved the schedule treatment and the addition of new drugs to first-line therapy. Because of the pathogenetic role of angiogenesis in solid-tumor growth and metastasis, research has been concentrated on anti-angiogenetic drug. Bevacizumab, the most promising anti-angiogenetic drug, is a humanized monoclonal IgG antibody that targets vascular endothelial growth factor receptor. It was approved on December 23, 2011 by the European Medicines Agency and on June 13, 2018 by the Food and Drug administration as first-line treatment in epithelial ovarian, fallopian tube, or primary peritoneal cancer stage III or IV in combination with carboplatin and paclitaxel. There are still some doubts, regarding the schedule, dosage, duration of the treatment, safety, and tolerability, both in first-line and in neoadjuvant chemotherapy treatments. This review tries to answer clinical practice questions and summarizes the evidence from Phase III studies, emerging data, and ongoing trials.
Keywords: ovarian cancer, first-line treatment, bevacizumab, anti-angiogenesis
Introduction
Ovarian cancer (OC) is the most lethal gynecologic cancer; it is responsible for ~14,070 deaths and 22,240 new cases in the United States annually.1 Primary debulking surgery (PDS) followed by a combination of platinum-paclitaxel-based chemotherapy is currently considered as the standard of care for advanced epithelial ovarian cancer (AOC).2,3
In patients with wide and aggressive tumor dissemination, an alternative treatment strategy is neoadjuvant chemotherapy (NACT) with delayed surgery (ie, interval debulking surgery, IDS). Despite the progress achieved in the last decades, almost 70% of the patients relapse, thus a lot of effort in the scientific community is being done for ameliorating the prognosis of these patients. The most important change in the last decades involved the schedule treatment and the addition of new drugs.
As the target therapy should be less toxic than cytotoxic drug, and because of the pathogenetic role of angiogenesis in solid-tumor growth and metastasis, research has been concentrated on antiangiogenetic medication. The rationale to use an antiangiogenetic treatment in cancer is related to the presence of hypoxia in cancer tissue; the reduction of oxygen induces the transcription of vascular endothelial growth factor receptor (VEGF-R) on the endothelial cells; subsequently, the binding of circulating vascular endothelial growth factor (VEGF) with the receptor leads to proliferation of new vessels, promoting tumor growth.
Bevacizumab, a humanized monoclonal IgG antibody that targets VEGF-R, has been one of the first and most investigated antiangiogenetic drugs, and several evidences demonstrated its efficacy also in OC.4
This inhibition leads to a reduction of neo-angiogenesis and an increase of vascular permeability; consequently, a higher dose of chemotherapeutic agents is released, finally resulting in the apoptosis of tumor endothelial cells.5
Bevacizumab is approved for the first-line treatment of AOC, fallopian tube, and primary peritoneal cancers due to the results of two randomized controlled Phase III trials.6,7
The International Collaborative Ovarian Neoplasm Trial 7 (ICON-7) and the Gynecologic Oncology Group protocol (GOG-0218) demonstrated an improvement of progression-free survival (PFS), mainly in the high-risk OC population; the “higher risk” was defined as patient with a FIGO stage III tumor, suboptimally debulked (residual disease [RT] after IDS >1 cm) or stage IV.
This review summarizes the evidence for the use of bevacizumab in first-line AOC with attention on the ongoing trials.
First-line treatment
Phase III randomized controlled trials
Bevacizumab was approved on December 23, 2011 by the European Medicines Agency (EMA)8 and on June 13, 2018 by the Food and Drug Administration (FDA)9 as the first-line treatment in patients with epithelial ovarian, fallopian tube, or primary peritoneal cancer stage III or IV in combination with carboplatin and paclitaxel. The dosage suggested is 15 mg/kg every 3 weeks with carboplatin and paclitaxel for up to six cycles, followed by 15 mg/kg every 3 weeks as a single agent, for a total of up to 22 cycles.10
The approval is based on the results of a multicenter, Phase III trial. In the GOG-0218 trial, 1,873 women with stage III/IV OC were involved. Patients, after PDS, were randomized to receive the standard treatment (carboplatin [AUC 6] and paclitaxel [175 mg/m2] from cycles 1–6 [group A=625], or adding bevacizumab from cycles 2 through 6, followed by placebo in cycles 7 through 22 [group B=625], or bevacizumab from cycles 2 through 22 [group C=623]). Bevacizumab was administered at the dosage of 15 mg/kg every 3 weeks.
The primary endpoint of the study was PFS, with overall survival (OS) as a secondary endpoint. The median PFS was 10.3, 11.2, and 14.1 months in the group A, group B, and group C, respectively (the hazard ratio for progression or death for group C compared with control group was 0.717 [95% CI, 0.625–0.824; P<0.001]).7 The final OS presented recently at the 2018 American Society of Clinical Oncology (ASCO) did not demonstrate a difference among the groups in terms of OS (the hazard ratio for group B vs group A was 1.06 [95% CI, 0.94–1.20, P=0.34], and for group C vs group A was 0.96 [95% CI, 0.85–1.09, P=0.53]).11
ICON-7 was another, Phase III randomized trial enrolling 1,528 patients with FIGO stage I–IIA clear-cell/grade 3 or FIGO stage III/IV epithelial AOC, primary peritoneal or fallopian tube cancer, to receive six cycles of 3-weekly carboplatin (AUC 5 or 6) and paclitaxel (175 mg/m2) with or without bevacizumab (7.5 mg/kg) for 12 months. The primary endpoint was PFS; the median PFS was 17.4 months for the control group vs 19.8 months for the bevacizumab group (P=0.004).6 Similar to the GOG-0218 study, no differences in the OS rate were reported after 49 months of follow-up (44.6 vs 45.5 months for the control and bevacizumab groups, respectively, P=0.85).12 Details of the studies about first-line therapy are summarized in Table 1.
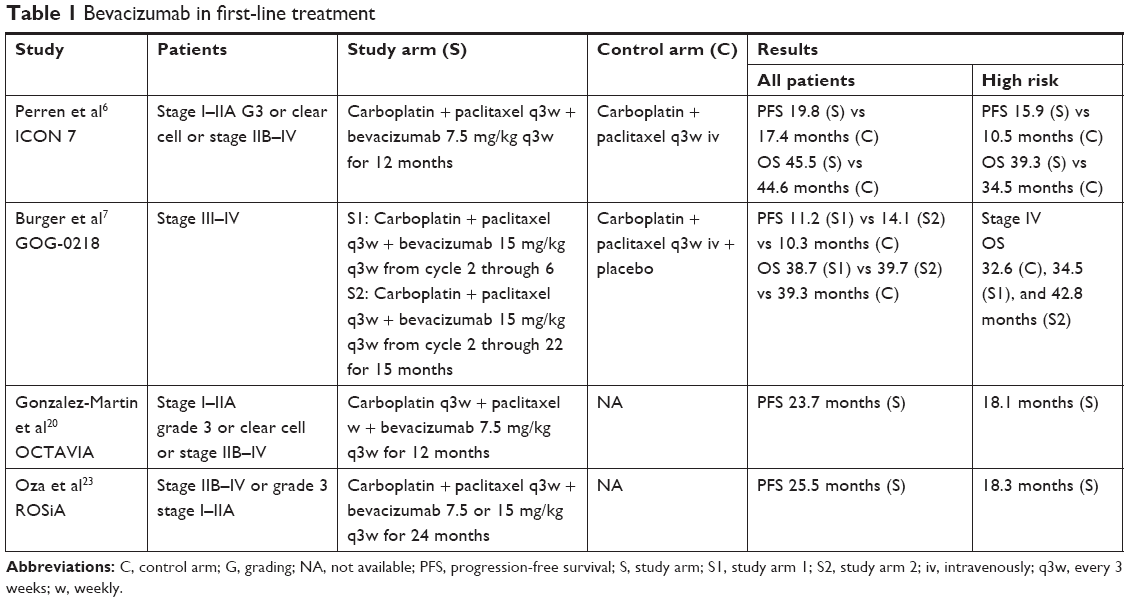 | Table 1 Bevacizumab in first-line treatment |
In which category of patients is adding bevacizumab better?
In both the studies, ICON-7 and GOG-0218, high-risk patients seem to have a greater benefit from bevacizumab.
In GOG-0218 trial, the study population included only patients with FIGO stage III–IV; the majority had a stage III tumor with optimal debulking (33% [n=205] RT after PDS <1 cm), or suboptimal debulking surgery (41% [n=256] RT after PDS >1 cm) and 26% (n=164) were stage IV.
For the primary outcome, which was PFS, a benefit was achieved for the entire population independently from risk stratification (the hazard ratio for group C compared with control group was 0.618, 0.763, and 0.698 for stage III optimally or suboptimally debulked and for stage IV, respectively).7
However, regarding the OS, a better prognosis was shown for FIGO stage IV (the relative hazard ratio for stage IV patients for group C compared to the control group was 0.774 with a median OS times of 32.6, 34.5, and 42.8 months in group A, group B, and group C, respectively) rather than FIGO stage III (control group, 44.3 months; group B, 42.9 months; group C, 44.2 months).11
In the ICON-7 study, the population included patients from early to advanced stage (FIGO stage I–IV); in particular, 9% had an early stage, 21% had a FIGO stage IIIA–B, and 70% had a FIGO stage IIIC–IV. In the overall population, PFS improved by 2.4 months while in the high-risk patients, PFS was higher of 5.4 months in the bevacizumab group (hazard ratio, 0.68; 95% CI, 0.55–0.85, P<0.001). Equally, the results in terms of OS were better in the high-risk patients (39.7 vs 30.3 months in the experimental vs control group, respectively, P=0.002).6
Which dosage should we use?
The dosage suggested according to the EMA and FDA approval is 15 mg/kg every 3 weeks.
The incidence of the main adverse events was lower in the ICON-7 trial, in which the dosage was 7.5 mg/kg, compared to GOG-0218, in which the dosage was 15 mg/kg; in particular, hypertension grade ≥2 occurred in 18% vs 22.9%, proteinuria grade ≥3 in 1% vs 1.6%, and gastrointestinal (GI) events 1% vs 2.6% in the ICON-7 and GOG-0218, respectively.
However, the two dosages were not directly compared, so, other studies are necessary to address this topic.
Associated with which schedule?
In both GOG-0218 and ICON-7 trials, bevacizumab was associated with the traditional 3-weekly carboplatin/paclitaxel.
This schedule was considered the standard for many decades;13 however, after the publication of the Japanese Gynecologic Oncology Group (JGOG), demonstrating a better prognosis in patient treated with a dose-dense strategy (carboplatin [AUC 6] 3-weekly and paclitaxel [80 mg/m2] weekly vs carboplatin [AUC 6] and paclitaxel [175 mg/m2] 3-weekly), there was a doubt about which schedule was more favorable. It is important to point out that JGOG was performed in an Asian population, which could have a different metabolism compared to European population.14,15 Subsequently, the Multicentre Italian Trials in Ovarian Cancer (MITO) studied another schedule of treatment; in MITO-7 carboplatin (AUC 2) plus paclitaxel (60 mg/m2) administrated both weekly was compared with the standard treatment; comparable results in term of PFS with less adverse events were found in the weekly schedule (PFS was 18.8 vs 16.5 months, in the weekly vs 3-weekly treatment, respectively, P=0.18).16 To investigate the three schedule in the European population, a Phase III randomized controlled trial was conducted. All three regimens were equally useful (PFS was 17.9 months for carboplatin 3 weeks/paclitaxel 3 weeks, 20.6 months for carboplatin 3 weeks/paclitaxel 1 week and 21.1 months for carboplatin 1 week/paclitaxel 1 week, P=NS),17 a result confirmed by a recent metanalysis.18
Therefore, could bevacizumab be associated with another schedule? As weekly paclitaxel seems to have antiangiogenetic effects,19 in the OCTAVIA trial, the efficacy and safety of bevacizumab (7.5 mg/kg 3-weekly) administrated with carboplatin (AUC 6) 3-weekly and paclitaxel (80 mg/m2) weekly was explored. The population was comparable to the ICON-7 study; the main characteristics were similar unless for a higher proportion of patients with measurable disease in OCTAVIA trial (48% vs 34%) and a lower proportion of patients optimally debulked (59% vs 79%). Interestingly, there were no treatment-related deaths, with 4.2% of patients having hypertension grade ≥3% and 0.4% of patients having GI perforation.20
The median PFS in the entire population was 23.7 months compared to a median of 19.8 months in the ICON-7 population, meanwhile, in the high-risk subgroup, the median PFS was 18.1 months compared to 15.9 months of the ICON-7. An update of the study which confirms these results was recently published.21
Data about safety of bevacizumab also emerged from another Phase III study. In GOG 262 trial, weekly vs 3-weekly paclitaxel and carboplatin was compared. Bevacizumab was administered to the 84% of the patients. In the weekly group, there was no difference in terms of therapy discontinuation owing to adverse events with or without bevacizumab (12% vs 11% of discontinuation in the group with or without bevacizumab, respectively).
To note, the adverse events that could be related to the administration of bevacizumab were comparable in the weekly vs 3-weekly administration (hypertension grade ≥3 was 44% vs 51%, proteinuria was 7% vs 13%, in the weekly and 3-weekly group, respectively), with a slightly higher GI events (GI wall disruption was 11% vs 4% in the weekly and 3-weekly group, respectively). Finally, in the weekly group, one death was registered for GI hemorrhage and one for ventricular fibrillation, while in the 3-weekly group, one death for stroke and one for myocardial infarction.22
For how long?
The current administration of bevacizumab according to the EMA and FDA approval is up to 22 cycles (15 months).8,9
In the GOG-0218, bevacizumab was administrated for 15 months, in the ICON-7 for 12 months; as the benefit peak in the PFS was achieved exactly at the end of bevacizumab in the GOG-0218, the ROSiA study, a single-arm Phase 3B study was designed, within the aim to evaluate the efficacy and safety of prolonging bevacizumab beyond 15 months.23
The population included was similar to the ICON-7; treatment discontinuation was principally due to disease progression (33%); only 17% patients discontinued because of the toxicity. Compared to the safety profile of the ICON-7, an increased incidence of proteinuria and hypertension was registered; it is not possible to know if this increased toxicity is due to the higher dose of bevacizumab (15 mg/kg in ROSiA vs 7.5 mg/kg in ICON-7) or to the prolongation of the treatment. However, the toxicity profile seems to be acceptable, and no increase of major adverse events as GI perforation was registered (1.3% vs 1% G3-4 in ROSiA and ICON-7, respectively). Moreover in terms of efficacy, the PFS was the longest reported for frontline bevacizumab-containing therapy (25.5 months in the overall population and 18.3 months in the high-risk subgroup).
According to these results, treatment prolongation with bevacizumab seems to be feasible, but final conclusion could be drawn only when the final results of AGO-OVAR17, a Phase III randomized controlled trial comparing 15 vs 30 months of bevacizumab therapy, will be available.24
Does age of the patient matter?
Fragility is typical of elderly people. In a clinical trial on solid tumor, addressing the safety of bevacizumab in older patients, the adverse events appeared higher.25 Otherwise, in the setting of OC, even if the toxicity is slightly increased, fatal events are comparable.24
A post hoc analysis of ROSiA study explored the safety and efficacy according to the age. A population of 121 women older than 70 years experienced higher incidences of anemia (44% vs 32%), diarrhea (35% vs 25%), asthenia (22% vs 12%), grade 3 hypertension (41% vs 22%), and thromboembolic events (7% vs 2%) compared with younger patients but only 1 (0.8%) fatal bevacizumab-related adverse events occurred in older vs 5 (0.6%) in younger patients (P=NS). The efficacy was comparable between older and younger women (median PFS was 23.7 vs 25.6 months, respectively).26 Moreover, in GOG-0218, the hazard ratio for group C vs control group demonstrated a benefit independently to the age (the hazard ratio for women <60 years was 0.680, for women from 60 to 69 years was 0.763, and for women ≥70 years was 0.678).
Can we predict the response?
Angiogenesis plays an important role in OC, even if it is still not clear in which category of patient the addition of anti-angiogenic therapy could improve the prognosis. A few studies started to analyze the angiogenetic gene profile of patients.
In the ICON-7 study, a molecular analysis was done, extracting the mRNA from 265 high-grade serous OC. Three subgroups were identified, two with an upregulation and one with a suppression (the immune group) of the angiogenic genes.
The OS was better for the immune subgroup (hazard ratio, 0.66; 95% CI, 0.46–0.94). Moreover, in the immune group, the addition of bevacizumab has worsened the PFS (hazard ratio, 1.73; 95% CI, 1.12–2.68) and the OS (hazard ratio, 2.00; 95% CI, 1.11–3.61). Conversely, in the pro-angiogenic group, there was a non-significant trend to improved PFS adding bevacizumab to chemotherapy (median 17.4 vs 12.3 months in controls).27
Another analysis was done on 359 patients included in ICON-7; four molecular subtypes were found: 73 differentiated (20%), 122 immunoreactive (34%), 68 mesenchymal (19%), and 96 proliferative (27%).
According to previous reports, patients with mesenchymal and proliferative tumors had a worse prognosis compared to the differentiated and immunoreactive subgroups; the greatest benefit from bevacizumab was obtained in the proliferative group, with a median PFS improvement of 10.1 months. This improvement in PFS remained statistically significant even after adjusting for age, grade, histology, and high risk of progression (hazard ratio, 0.45; 95% CI, 0.27–0.74, P=0.0015).28
Recently, attention was focused on the inflammation; release of proinflammatory cytokines has a pro-angiogenetic effect, thus, patients with a systemic inflammation could benefit more of the treatment with bevacizumab. Neutrophil-to-lymphocyte ratio (NLR) is an inflammatory marker increased in different solid tumor, including OC. The NLR and other markers were combined to calculate different score, and in a small series of patients shown to predict prognosis and response to the treatment.29
In this context, MITO-24 was a retrospective study analysis aimed to analyze different inflammatory index in AOC. Thirty hundred and seventy-five patients were recruited, 301 (81%) received chemotherapy alone and 74 (19%) received chemotherapy plus bevacizumab. Patients with higher NLR were older (median age was 60 vs 64 years in low and high NLR group, respectively), presented a more diffuse disease (26% vs 34% of patients presented FIGO stage 4 in low and high NLR group, respectively), and had a worse prognosis (hazard ratio for the PFS was 1.45; 95% CI, 1.16–1.82, P=0.001, hazard ratio for the OS was 1.88; 95% CI, 1.42–2.47, P<0.0001). Interestingly, in patients with higher NLR, the PFS and OS were higher in those receiving chemotherapy with bevacizumab than in those receiving chemotherapy alone (P=0.026 and P=0.029, respectively).30
Neoadjuvant setting
PDS followed by adjuvant platinum-taxane-based chemotherapy is the standard of care in AOC.31,32 In patients with non-optimally resectable disease, IDS is the best strategy.33–35 The doubt about adding bevacizumab in the NACT setting is related to the risk of complications, primarily, GI or thromboembolic events;36 with this regard, it has been suggested to postpone the surgery at least 28 days after the last bevacizumab administration.37
These topics were addressed in the ANTHALYA trial, a Phase II multicenter randomized trial aimed to evaluate the safety and efficacy of bevacizumab in a neoadjuvant setting. Patients initially received four cycles of neoadjuvant 3-weekly carboplatin-paclitaxel chemotherapy with (BCP group) or without (CP group) three cycles of bevacizumab 15 mg/kg followed by IDS; after surgery, adjuvant chemotherapy was administrated, reintroducing bevacizumab at cycle 6 and maintained for at least 26 cycles. The first objective was the complete resection rate (CRR). Thirty-seven (39%) patients were included in the CP group and 58 (61%) in the BCP group. The CRR was higher in the BCP group (85.5%) with an acceptable toxicity profile. Grade 3 adverse event occurred in a similarly proportion of patients (28% in CP and 29% in BCP group). Postoperative complication occurred in eight patients (36%) in CP and in eleven patients (28%) in BCP group.38
These data were confirmed in a more recent Phase IV study, the MITO16A-Mango OV2A, a trial designed to find prognostic factor to individualize the therapy with bevacizumab. An unplanned analysis showed the surgical details of 79 patients receiving NACT with bevacizumab followed by IDS. Interestingly, 63.5% of patients had no RT after IDS, 86.5% were optimally debulked (RT ≤1 cm) and only 13.5% were suboptimally debulked (RT >1 cm). No postoperative deaths were reported. Twenty-seven patients (38%) had at least one postoperative adverse event, especially mild (fever [4%], transfusion [4%]), with only 3 (3.9%) GI events registered.39
Regarding the schedule to associate with, bevacizumab was investigated in a few studies. Salani et al analyzed nine advanced high-grade serous epithelial OC patients in a Phase I study treated with weekly paclitaxel (80 mg/m2) plus carboplatin (AUC 5) and bevacizumab (15 mg/kg) every 3 weeks. No intraoperative complications were registered and 78% of patients had no gross RT. Only one patient was re-operated because of an anastomotic leakage 10 days after the IDS.40
Another case–control study analyzed 25 patients with high-grade serous AOC treated with or without bevacizumab-based NACT in the 3-weekly schedule. The experimental group was compared with 50 patients in the control group. The IDS was generally performed 4 weeks after the end of chemotherapy in both groups (P=0.547). Optimal cytoreduction was achieved equally in the investigational arm (80%) and in the control group (72.3%) (P=0.26). No differences in terms of surgical complications were observed.
The prognosis was better in the bevacizumab group with a PFS of 18 vs 10 months in the control group, respectively (P=0.001).41
The characteristics of the studies are summarized in Table 2.
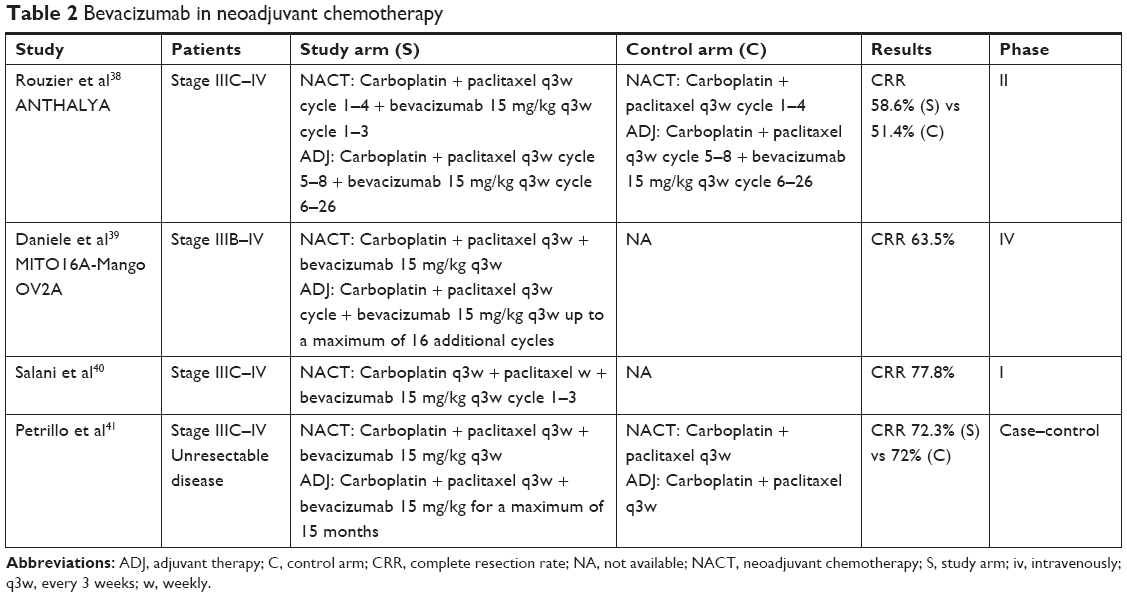 | Table 2 Bevacizumab in neoadjuvant chemotherapy |
In conclusion, interesting results have been shown also with the use of bevacizumab in the NACT setting, but further studies are necessary to draw definitive conclusions.
Ongoing trials
Few ongoing studies are currently under way, investigating the combination of bevacizumab with other drugs, such as poly adenosine diphosphate ribose polymerase-inhibitors (PARP-i) or immune checkpoint inhibitor, in both the neoadjuvant and the adjuvant settings. Neopembrov is a Phase II study that involves patients not amenable of PDS stage IV, evaluating the efficacy of associating bevacizumab with pembrolizumab, an anti-programmed cell death 1 (PD1) receptor blocking both PD-L1 and PD-L2, from interacting with PD-1 to help restore T-cell response and immune response. The first objective is the CRR.
Patients will be randomized to receive carboplatin (AUC5-6) and paclitaxel (175 mg/m²) with or without bevacizumab (15 mg/kg) and pembrolizumab (200 mg) 3-weekly.42 Imagyn050 is a Phase III, randomized controlled trial, aimed to evaluate the association of bevacizumab and atezolizumab. Participants in the NACT group will receive paclitaxel, carboplatin, and atezolizumab for six cycles and bevacizumab for four cycles. Interval surgery will occur between cycles 3 and 4. Each cycle is 21 days long. After six cycles, participants will start maintenance therapy of bevacizumab and atezolizumab for additional 16 cycles.43
In addition to a study on new drugs in NACT, other associations are also on study in the adjuvant setting. NCT00520013 is a Phase II study aimed to evaluate the combination of bevacizumab and erlotinib. Patients will receive carboplatin (AUC 5) plus paclitaxel (175 mg/m2) plus bevacizumab (15 mg/kg) 3-weekly for six cycles and a consolidation with bevacizumab (15 mg/kg) on day 1 of the cycle plus oral erlotinib (150 mg) daily for 1 year.44
MITO-25 is a Phase I–II study evaluating the addition of a PARP inhibitor to the standard treatment. Experimental group will receive carboplatin (AUC 5) plus paclitaxel (175 mg/m2) 3-weekly for six cycles plus bevacizumab 15 mg/kg 3-weekly for 22 cycles (in combination and maintenance) plus rucaparib at the dose defined by the Phase I study continuously for 2 years (rucaparib only in maintenance).45 The trial details are shown in Table 3.
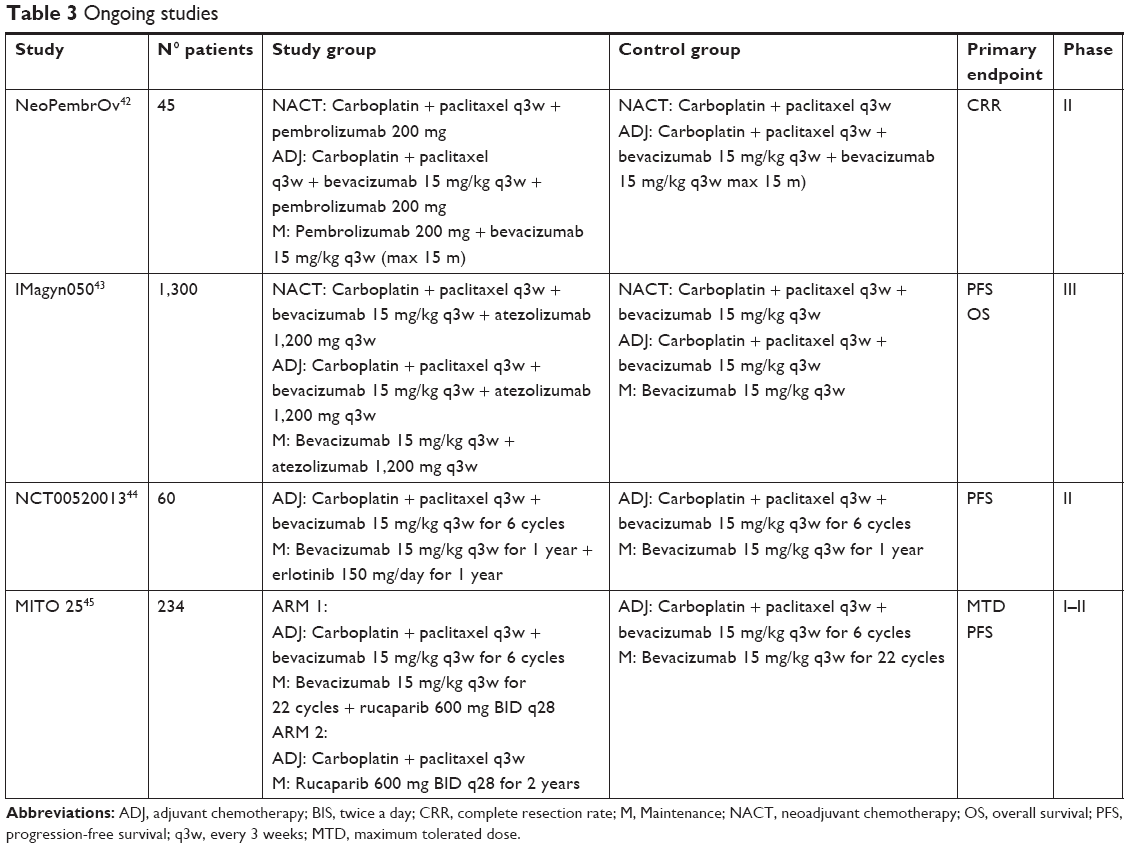 | Table 3 Ongoing studies |
Conclusion
Bevacizumab combined with standard chemotherapy drugs has led to a significant improvement in the PFS in first-line approach, mainly in high-risk patients (stage III–IV) affected by OC; the results seem to be comparable between older and younger women. Nevertheless, there are still pending issues. The dosage suggested is 15 mg/kg every 3 weeks, but it is not already known if a lower dosage has a comparable efficacy with lower toxicity. Other schedules and other combination drugs are under investigation, trying favorable effects of bevacizumab. The duration of the treatment is not universally shared; data from randomized trials are still awaited, and researchers are looking for biologic factors to identify women who could most benefit from bevacizumab therapy. Also in the neoadjuvant setting for AOC, bevacizumab seems to be feasible and safe, but a balance between CRR at IDS, safety, survival is not defined.
Further studies addressing this topic are necessary, waiting for data from ongoing trials that will clarify these doubts.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. | ||
Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi24–vi32. | ||
Schorge JO, Eisenhauer EE, Chi DS. Current surgical management of ovarian cancer. Hematol Oncol Clin North Am. 2012;26(1):93–109. | ||
The European Medicines Agency. European public assessment report. Avastin product information. Avastin-H-C-582-II-23, August 2008. Available from: http://www.emea.europa.eu/docs/en_GB/document_library/EPAR_–_Assessment_Report_–_Variation/human/000582/WC500029270.pdf. Accessed January 24, 2009. | ||
Shih T, Lindley C. Bevacizumab: an angiogenesis inhibitor for the treatment of solid malignancies. Clin Ther. 2006;28(11):1779–1802. | ||
Perren TJ, Swart AM, Pfisterer J, et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365(26):2484–2496. | ||
Burger RA, Brady MF, Bookman MA, et al; Gynecologic Oncology Group. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med. 2011;365(26):2473–2483. | ||
Avastin Bevacizumab. Summary of opinion (post authorisation) [webpage on the Internet]. European Medicines Agency; 2017 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion/human/000582/WC500226190.pdf. Accessed January 18, 2019. | ||
Highlights of prescribing information. AVASTIN (bevacizumab) injection, for intravenous use Initial U.S. Approval: 2004 [webpage on the Internet]. Revised 06/2018.Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/125085s323lbl.pdf. Accessed January 18, 2019. | ||
FDA Approves Genentech’s Avastin (Bevacizumab) Plus Chemo-therapy as a Treatment for Women With Advanced Ovarian Cancer Following Initial Surgery [webpage on the Internet]. June 2018. Available from: http://ovarian.org/about-ovarian-cancer/treatment/493-2018-06-13-21-09-18. Accessed January 18, 2019. | ||
Robert AB, Danielle E, Krishnansu ST. Final overall survival (OS) analysis of an international randomized trial evaluating bevacizumab (BEV) in the primary treatment of advanced ovarian cancer: a NRG oncology/Gynecologic Oncology Group (GOG) study. J Clin Oncol. 2018;36(15 Suppl):5517. | ||
Oza AM, Cook AD, Pfisterer J, et al; ICON7 trial investigators. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015;16(8):928–936. | ||
Stuart G, Avall-Lundqvist E, Du Bois A, et al. 3rd international ovarian cancer consensus Conference: outstanding issues for future consideration. Ann Oncol. 2005;16(suppl 8):viii36–viii38. | ||
Bergmann TK, Gréen H, Brasch-Andersen C, et al. Retrospective study of the impact of pharmacogenetic variants on paclitaxel toxicity and survival in patients with ovarian cancer. Eur J Clin Pharmacol. 2011;67(7):693–700. | ||
Komatsu M, Wheeler HE, Chung S, et al. Pharmacoethnicity in paclitaxel-induced sensory peripheral neuropathy. Clin Cancer Res. 2015;21(19):4337–4346. | ||
Pignata S, Scambia G, Katsaros D, et al; Gynecologic Cancer InterGroup (GCIG) Investigators. Carboplatin plus paclitaxel once a week versus every 3 weeks in patients with advanced ovarian cancer (MITO-7): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2014;15(4):396–405. | ||
Academic.oup.com. ICON8: A GCIG phase III randomised trial evaluating weekly dose- dense chemotherapy integration in first-line epithelial ovarian/fallopian tube/primary peritoneal carcinoma (EOC) treatment: Results of primary progression- free survival (PFS) analysis. Available from: https://academic.oup.com/annonc/article/28/suppl_5/mdx440.039/4109951. Accessed January 18, 2019. | ||
Marchetti C, De Felice F, Di Pinto A, et al. Dose-dense Weekly chemotherapy in advanced ovarian cancer: an updated meta-analysis of randomized controlled trials. Crit Rev Oncol Hematol. 2018;125:30–34. | ||
Jiang H, Tao W, Zhang M, Pan S, Kanwar JR, Sun X. Low-dose metronomic paclitaxel chemotherapy suppresses breast tumors and metastases in mice. Cancer Invest. 2010;28(1):74–84. | ||
Gonzalez-Martin A, Gladieff L, Tholander B, et al; OCTAVIA Investigators. Efficacy and safety results from OCTAVIA, a single-arm phase II study evaluating front-line bevacizumab, carboplatin and weekly paclitaxel for ovarian cancer. Eur J Cancer. 2013;49(18):3831–3838. | ||
Gonzalez-Martin A, Gladieff L, Tholander B, et al; OCTAVIA Investigators. Updated results from OCTAVIA (front-line bevacizumab, carboplatin and weekly paclitaxel therapy for ovarian cancer). Eur J Cancer. 2014;50(4):862–863. | ||
Chan JK, Brady MF, Penson RT, et al. Weekly vs. Every-3-Week paclitaxel and carboplatin for ovarian cancer. N Engl J Med. 2016;374(8):738–748. | ||
Oza AM, Selle F, Davidenko I, et al. Efficacy and safety of bevacizumab-containing therapy in newly diagnosed ovarian cancer: ROSiA single-arm phase 3B study. Int J Gynecol Cancer. 2017;27(1):50–58. | ||
A prospective randomised phase III trial to evaluate optimal treatment duration of first-line bevacizumab in combination with carboplatin and paclitaxel in patients with primary epithelial ovarian, fallopian tube or peritoneal cancer. AGO-OVAR17. Ongoing, NCT number: NCT01462890, ClinicalTrials.gov. | ||
Roche. Avastin summary of product characteristics. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR__Product_Information/human/000582/WC500029271.pdf. Accessed February 7, 2017. | ||
Selle F, Colombo N, Korach J, et al. Safety and efficacy of extended bevacizumab therapy in elderly (≥70 years) versus younger patients treated for newly diagnosed ovarian cancer in the International ROSiA study. Int J Gynecol Cancer. 2018;28(4):729–737. | ||
Gourley C, A M, Perren T. Molecular subgroup of high-grade serous ovarian cancer (HGSOC) as a predictor of outcome following bevacizumab. J Clin Oncol. 2014;32(15 Suppl):5502. | ||
Kommoss S, Winterhoff B, Oberg AL, et al. Bevacizumab may differentially improve ovarian cancer outcome in patients with proliferative and mesenchymal molecular subtypes. Clin Cancer Res. 2017;23(14):3794–3801. | ||
Marchetti C, Romito A, Musella A, et al. Combined plasma fibrinogen and neutrophil lymphocyte ratio in ovarian cancer prognosis may play a role? Int J Gynecol Cancer. 2018;28(5):939–944. | ||
Farolfi A, Petrone M, Scarpi E, et al. Inflammatory indexes as prognostic and predictive factors in ovarian cancer treated with chemotherapy alone or together with bevacizumab. A multicenter, retrospective analysis by the MITO group (MITO 24). Target Oncol. 2018;13(4):469–479. | ||
Stuart GC, Kitchener H, Bacon M, et al. 2010 gynecologic cancer intergroup (GCIG) consensus statement on clinical trials in ovarian cancer: report from the fourth ovarian cancer consensus Conference. Int J Gynecol Cancer. 2011;21(4):750–755. | ||
National Comprehensive Cancer Network. Epithelial ovarian cancer, including fallopian tube cancer and primary peritoneal cancer, 2015 ver1.2015. Available from: http://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf. Accessed January 18, 2019. | ||
Morgan RJ, Alvarez RD, Armstrong DK, et al; National Comprehensive Cancer Network. Epithelial ovarian cancer. J Natl Compr Canc Netw. 2011;9(1):82–113. | ||
Vergote I, Tropé CG, Amant F, et al; NCIC Clinical Trials Group. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med. 2010;363(10):943–953. | ||
Kehoe S, Hook J, Nankivell M, et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (chorus): an open-label, randomised, controlled, non-inferiority trial. The Lancet. 2015;386(9990):249–257. | ||
McClung EC, Wenham RM. Profile of bevacizumab in the treatment of platinum-resistant ovarian cancer: current perspectives. Int J Womens Health. 2016;8:59–75. | ||
Genentech Inc. Avastin Prescribing Information. San Francisco, Genentech; 2011. | ||
Rouzier R, Gouy S, Selle F, et al. Efficacy and safety of bevacizumab-containing neoadjuvant therapy followed by interval debulking surgery in advanced ovarian cancer: results from the ANTHALYA trial. Eur J Cancer. 2017;70:133–142. | ||
Daniele G, Lorusso D, Scambia G, et al. Feasibility and outcome of interval debulking surgery (IDS) after carboplatin-paclitaxel-bevacizumab (CPB): a subgroup analysis of the MITO-16A-MaNGO OV2A phase 4 trial. Gynecol Oncol. 2017;144(2):256–259. | ||
Salani R, O’Malley DM, Copeland LJ, et al. Feasibility of interval cytoreduction following neoadjuvant chemotherapy with carboplatin, weekly paclitaxel, and bevacizumab for advanced ovarian cancer – a phase 1 study. Int J Gynecol Cancer. 2014;24(4):682–686. | ||
Petrillo M, Paris I, Vizzielli G, et al. Neoadjuvant chemotherapy followed by maintenance therapy with or without bevacizumab in unresectable high-grade serous ovarian cancer: a case-control study. Ann Surg Oncol. 2015;22(S3):S952–S958. | ||
RandomizedA Arandomized. Open-label, multicentric phase II trial of pembrolizumab (Keytruda®) with chemotherapy versus chemotherapy alone (standard of care) as neo adjuvant treatment of ovarian cancer not amenable to front line debulking surgery. NEOPEMBROV. Ongoing, NCT number: NCT03275506, ClinicalTrials.gov. | ||
A phase III, multicenter, randomized, study of Atezolizumab versus placebo administered in combination with paclitaxel, carboplatin, and bevacizumab to patients with Newly-Diagnosed stage III or stage IV ovarian, fallopian tube, or primary peritoneal cancer. IMagyn050. Ongoing, NCT number: NCT03038100, ClinicalTrials.gov. | ||
A Randomized Phase II Trial of Avastin (A) or Avastin and Erlotinib (AE) as First Line Consolidation Chemotherapy After Carboplatin, Paclitaxel, and Avastin (CTA) Induction Therapy for Newly Diagnosed Advanced Ovarian, Fallopian Tube, Primary Peritoneal Cancer & Papillary Serous or Clear Cell Mullerian Tumors. Ongoing, NCT number: NCT00520013, ClinicalTrials.gov. | ||
A randomized phase II trial of Carboplatin-Paclitaxel-Bevacizumab vs Carboplatin-Paclitaxel-Bevacizumab-Rucaparib vs Carboplatin-Paclitaxel-Rucaparib in patients with advanced (stage III B-C-IV) ovarian, primary peritoneal and fallopian tube cancer preceded by a phase I dose escalation study on Rucaparib-Bevacizumab combination. MITO 25. Ongoing, NCT number: NCT03462212, ClinicalTrials.gov. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.