")
Back to Journals » Clinical Ophthalmology » Volume 14
Finite Element Analysis of Air Gun Impact on Post-Keratoplasty Eye
Authors Okamura K, Shimokawa A, Takahashi R, Saeki Y, Ozaki H, Uchio E
Received 31 October 2019
Accepted for publication 13 December 2019
Published 21 January 2020 Volume 2020:14 Pages 179—186
DOI https://doi.org/10.2147/OPTH.S236825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kanno Okamura, Asami Shimokawa, Rie Takahashi, Yusuke Saeki, Hiroaki Ozaki, Eiichi Uchio
Department of Ophthalmology, Fukuoka University School of Medicine, Fukuoka, Japan
Correspondence: Eiichi Uchio
Department of Ophthalmology, Fukuoka University School of Medicine, 7-45-1 Nanakuma, Jonan-ku, Fukuoka 814-0180, Japan
Tel +81 92 801 1011
Fax +81 92 865 4445
Email [email protected]
Purpose: Due to the mechanical vulnerability of eyes that have undergone penetrating keratoplasty (PKP), it is clinically important to evaluate the possibility of corneal wound dehiscence by blunt impact. We have previously developed a simulation model resembling a human eye based on information obtained from cadaver eyes and applied three-dimensional finite element analysis (FEA) to determine the physical and mechanical response to an air gun impact at various velocities on the post-PKP eye.
Methods: Simulations in a human eye model were performed with a computer using a FEA program created by Nihon, ESI Group. The air gun pellet was set to impact the eye at three-different velocities in straight or 12° up-gaze positions with the addition of variation in keratoplasty suture strength of 30%, 50% and 100% of normal corneal strength.
Results: Furthermore to little damage in the case of 100% strength, in cases of lower strength in a straight-gaze position, wound rupture seemed to occur in the early phase (0.04– 0.06 ms) of impact at low velocities, while regional break was observed at 0.14 ms after an impact at high velocity (75 m/s). In contrast, wound damage was observed in the lower quadrant of the suture zone and sclera in 12° up-gaze cases. Wound damage was observed 0.08 ms after an impact threatening corneoscleral laceration, and the involved area being larger in middle impact velocity (60 m/s) simulations than in lower impact velocity simulations, and larger damaged area was observed in high impact velocity cases and leading to corneoscleral laceration.
Conclusion: These results suggest that the eye is most susceptible to corneal damage around the suture area especially with a straight-gaze impact by an air gun, and that special precautionary measures should be considered in patients who undergo PKP. FEA using a human eyeball model might be a useful method to analyze and predict the mechanical features of eyes that undergo keratoplasty.
Keywords: air gun, finite element analysis, cornea, rupture, keratoplasty
Introduction
Globe rupture in eyes treated by corneal transplantation is a serious-clinical condition that may result in loss of vision.1,2 Several studies have reported the clinical outcome, incidence and causes of trauma in cases of globe rupture after keratoplasty.1–10 The incidence of traumatic globe dehiscence after penetrating keratoplasty (PKP) has been reported to be 0.23–5.8%.3,5,8–10 Keratoplasty exposes patients to a higher risk of globe rupture because the surgical wound may never regain the strength and stability of an intact cornea.1 The major types of trauma causing globe rupture in the post-PKP eye are: being accidentally struck by an object (33%) or child (13%), intentional trauma (20%) and falls (13%).3 In other studies, major causes of globe rupture in eyes undergoing keratoplasty were falls in elderly patients followed by blunt trauma, from a branch, airbag, fist or finger.1,5 Due to the mechanical vulnerability of eyes that undergo keratoplasty, it is clinically important to evaluate the corneal wound strength against blunt impact, and the risk of traumatic wound dehiscence. However, it is difficult to evaluate strain strength property of the post-keratoplasty eye, because an apparatus for measuring mechanical features of the eye has not been developed or introduced in clinical ophthalmology, and the possibility of tissue damage by these tests cannot be excluded, especially in a clinical situation.
A recent study reported increased damage with increased pressure and a shift in the damage profile over time in a mouse model of primary ocular blast injury using a device consisting of a pressurized air tank attached to a regulated paintball gun with a machined barrel.11 However, this study did not evaluate open ocular injury caused by blast injury.11 Therefore, we planned to research the kinetic phenomenon of blunt trauma to eyes that have undergone keratoplasty in a simulation method. Creating a human-like eye with raw data from the human eye for biomechanical simulations using finite element analysis (FEA) would help to investigate and better explain the physical and physiological responses to impact injuries.12 The other important benefit of biomechanical analysis obtained with computer models is that they may reduce the need for animal studies over time, which being increasingly restricted on ethical grounds.
We have previously developed a simulation model resembling a human eye based on information obtained from cadaver eyes, and applied three-dimensional FEA to determine the physical and mechanical conditions of impacting foreign bodies that cause an intraocular-foreign body.13 This model of the human eye was also used in our studies on airbag impact in the post-radial keratotomy eye,14 post-transsclerally fixated posterior chamber intraocular lens (PC-IOL) eye,15 and after photorefractive keratectomy.16 After refinement of the FEA model, we have recently evaluated the threshold of impact velocity of an airbag to induce suture breakage or globe rupture in the post-transsclerally fixated PC-IOL eye with different axial lengths, by using FEA.17
It was reported that the mean time from corneal keratoplasty to globe rupture or wound dehiscence was 6.5 months–6.2 years.1–3,7,8 Except for the report by Rohrbach et al,2 the interval between keratoplasty and traumatic wound dehiscence ranged from 6.5 to 22 months in other studies.1,7,8 It is interesting that corneal wound dehiscence occurred most frequently (37%) within the first year after surgery,3 and 37.5% of traumatic ruptures occurred in the first postoperative month.9 These reports suggest that the occurrence of corneal wound rupture depends on wound strength after surgery, and visual disability early after surgery also increases the risk of blunt trauma. Collating these factors, in this study, we extended the simulation model after revision to further determine the physical and mechanical response to an air gun impact at various velocities on the post-keratoplasty eye, with consideration of recovery of wound strength in a stepwise range using FEA.
Materials and Methods
A model human eye was created and used in computer simulations performed with FEA program, PAM-GENERISTM (Nihon ESI, Tokyo, Japan), described elsewhere.13 The model eye was created by setting the mass density of the cornea and sclera as constants, and element types including the three layers of the model eye (outer, middle and inner) as variables for meshing principles (Figure 1A).13 The material properties and geometry of the model were obtained from past experiments with three pairs of human cadaver eyes.13 The elastic properties and meshing principles of the model human eye were similar to those in previous reports.13,14 Poisson ratios of the cornea at 0.420 kg/mm3 and the sclera at 0.470 kg/mm3 were used to determine the standard stress strain curves for the cornea and sclera.18–20 The cornea was assumed to be spherical, with a central thickness of 0.5 mm and a central radius of curvature of 7.8 mm. The anterior chamber was set at a depth of 5.1 mm. The vitreous length was assumed to be 18.6 mm, and the posterior curvature of the retina was assumed to be 12.0 mm. The mass densities of ocular tissues from past reports were applied as follows: cornea, 1.149 kg/mm3; sclera, 1.243 kg/mm3; vitreous humor, 1.002 kg/mm3 and aqueous humor, 1.000 kg/mm3. A vitreous model as a solid mass was also assigned with a hydrostatic pressure of 20 mmHg (2.7 kPa).
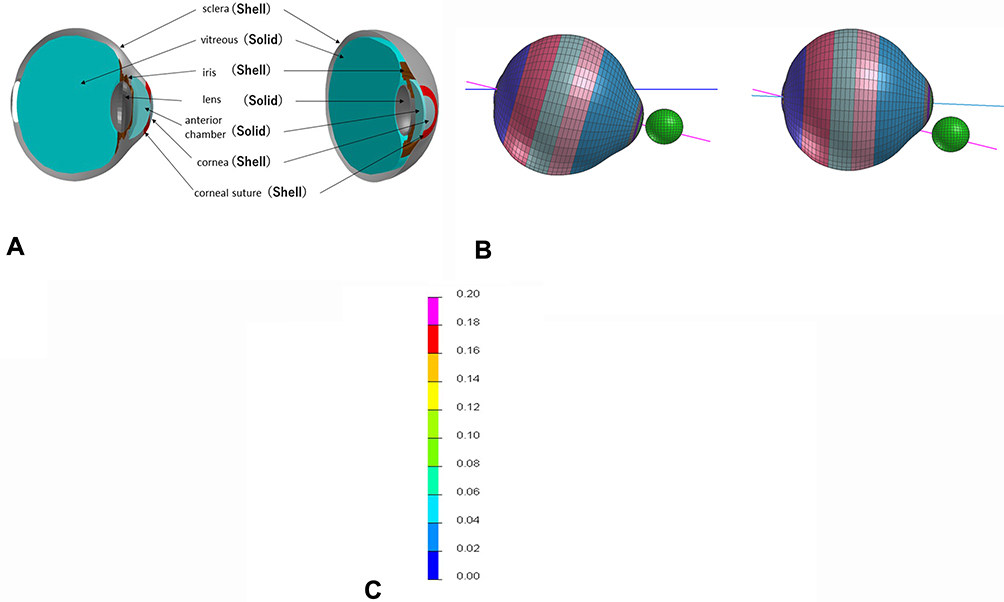 |
Figure 1 Simulation profile of model eye and deformation scale. (A) Sagittal and diagonal views of model eye and meshing principles of finite element analysis. (B) Eyeball and impacting air gun location in straight- (left) and 12° up-gaze (right) positions. (C) Color mapping scale of deformation of eye showing strain induced; warmer color of red represents greater deformation. Strain strength that induces corneal laceration is simulated to occur at 18.0% (red) and scleral laceration is simulated to occur at 6.8% (blue green). |
A biomechanical head of a dummy was created, assuming that everything excluding the eye was a solid element, to reduce the computing time. The Hybrid III model was modified by replacing the head of the dummy with a biomechanical model of the head in which an eye with a transplanted corneal graft was inserted.18,21 An air gun pellet (0.2 g), with 6 mm diameter and higher rigidity than an eyeball, was set to impact the eyeball in a straight- or 12° up-gaze position (Figure 1B) at initial velocities of 45, 60 and 75 m/s. The reference point for globe rupture was then calculated to be at a strain of 18.0% and stress of 9.45 MPa for the cornea, and at a strain of 6.8% and stress of 9.49 MPa for the sclera, which exceeded the tensile tolerance based on element deletion method.14 A new approach in this study was the addition of variation of keratoplasty suture strength of 30%, 50% and 100% of normal corneal strength, instead of calculating the limit of tensile force (N) of a 10–0 nylon suture. The suture region was assigned between 5.5 mm and 7.5 mm diameter, and strain that exceeded the tensile tolerance in this region was set to 5.4%, 9.0% and 18.0% in the case of strength variation of 30%, 50% and 100%, respectively.
Changes in the deformity of the eye and the strain induced were calculated by Virtual Performance Solver (VPS) (Nihon ESI) and evaluated by color mapping (Figure 1C). Breakage of the corneal suture was defined as the point at which the strain becomes intolerable due to deformation of the eye caused by air gun impact, when the strain exceeds the strain or stress value of the cornea based on element deletion method.22 In this study, the mapping properties were also revised owing to the development of computer technology since the previous study.17 Corneal wound strain was recorded sequentially at all velocities, and deformation of the eye was displayed sequentially in milliseconds in slow motion.
Results
Abundant data were extracted from this simulation study. Thus, it is difficult to display all the results. The results of each condition are shown in the frontal view, side view and sectional view of the deformed globe. Maximum strain observed in the frontal view was also obtained in all simulation conditions. Due to two eye gaze positions (0° and 12°), three strength variations (30%, 50% and 100%), and three impact velocities of the air gun (45, 60 and 75 m/s), 18 cases were simulated sequentially from the primary impact to the eyeball until 0.2 ms after the primary impact. Figure 2 shows the sequential change of maximum strain displayed graphically with color in 18 simulation conditions. Figure 2A shows the result of a case of 0° gaze, 30% strength and 45 m/s impact velocity (0-30-45), for example.
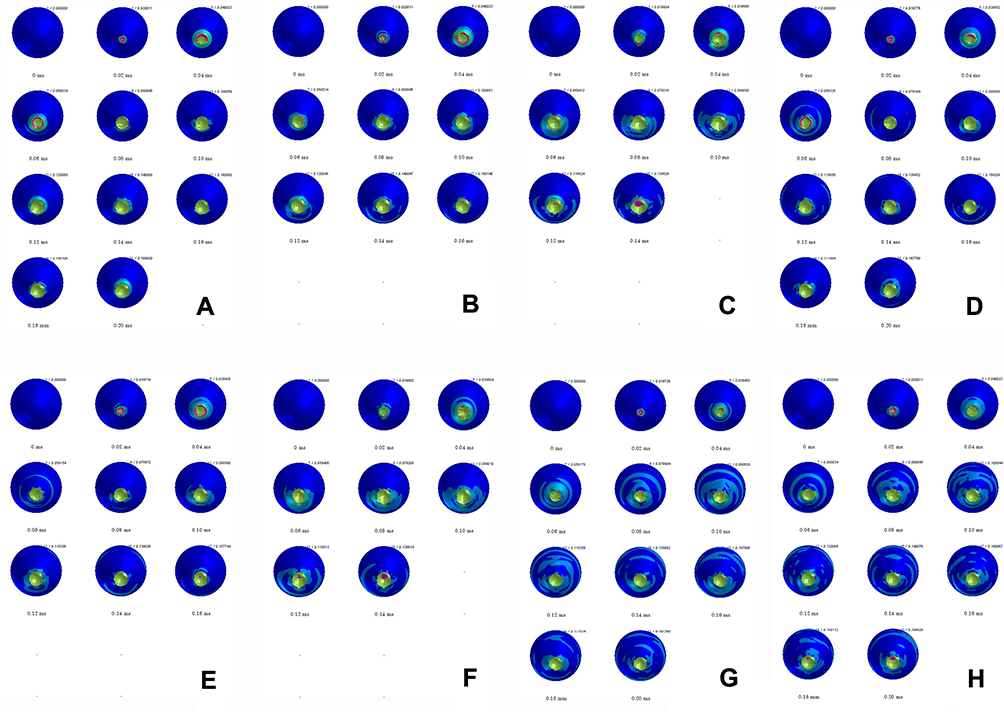 |
Figure 2 Sequential deformation of post-penetrating keratoplasty model eye upon airsoft gun impact at three different velocities and three different strain strengths in sutured area. (A) Case of straight-gaze position, strain strength 30% and impact velocity 45 m/s (0-30-45). (B) Case of straight-gaze position, strain strength 30% and impact velocity 60 m/s (0-30-60). (C) Case of straight-gaze position, strain strength 30% and impact velocity 75 m/s (0-30-75). (D) Case of straight-gaze position, strain strength 50% and impact velocity 45 m/s (0-50-45). (E) Case of straight-gaze position, strain strength 50% and impact velocity 60 m/s (0-50-60). (F) Case of straight-gaze position, strain strength 50% and impact velocity 75 m/s (0-50-75). (G) Case of straight-gaze position, strain strength 100% and impact velocity 45 m/s (0-100-45). (H) Case of straight-gaze position, strain strength 100% and impact velocity 60 m/s (0-100-60). (I) Case of straight-gaze position, strain strength 100% and impact velocity 75 m/s (0-100-75). (J) Case of 12° up-gaze position, strain strength 30% and impact velocity 45 m/s (12-30-45). (K) Case of 12° up-gaze position, strain strength 30% and impact velocity 60 m/s (12-30-60). (L) Case of 12° up-gaze position, strain strength 30% and impact velocity 75 m/s (12-30-75). (M) Case of 12° up-gaze position, strain strength 50% and impact velocity 45 m/s (12-50-45). (N) Case of 12° up-gaze position, strain strength 50% and impact velocity 60 m/s (12-50-60). (O) Case of 12° up-gaze position, strain strength 50% and impact velocity 75 m/s (12-50-75). (P) Case of 12° up-gaze position, strain strength 100% and impact velocity 45 m/s (12-100-45). (Q) Case of 12° up-gaze position, strain strength 100% and impact velocity 60 m/s (12-100-60). (R) Case of 12° up-gaze position, strain strength 100% and impact velocity 75 m/s (12-100-75). |
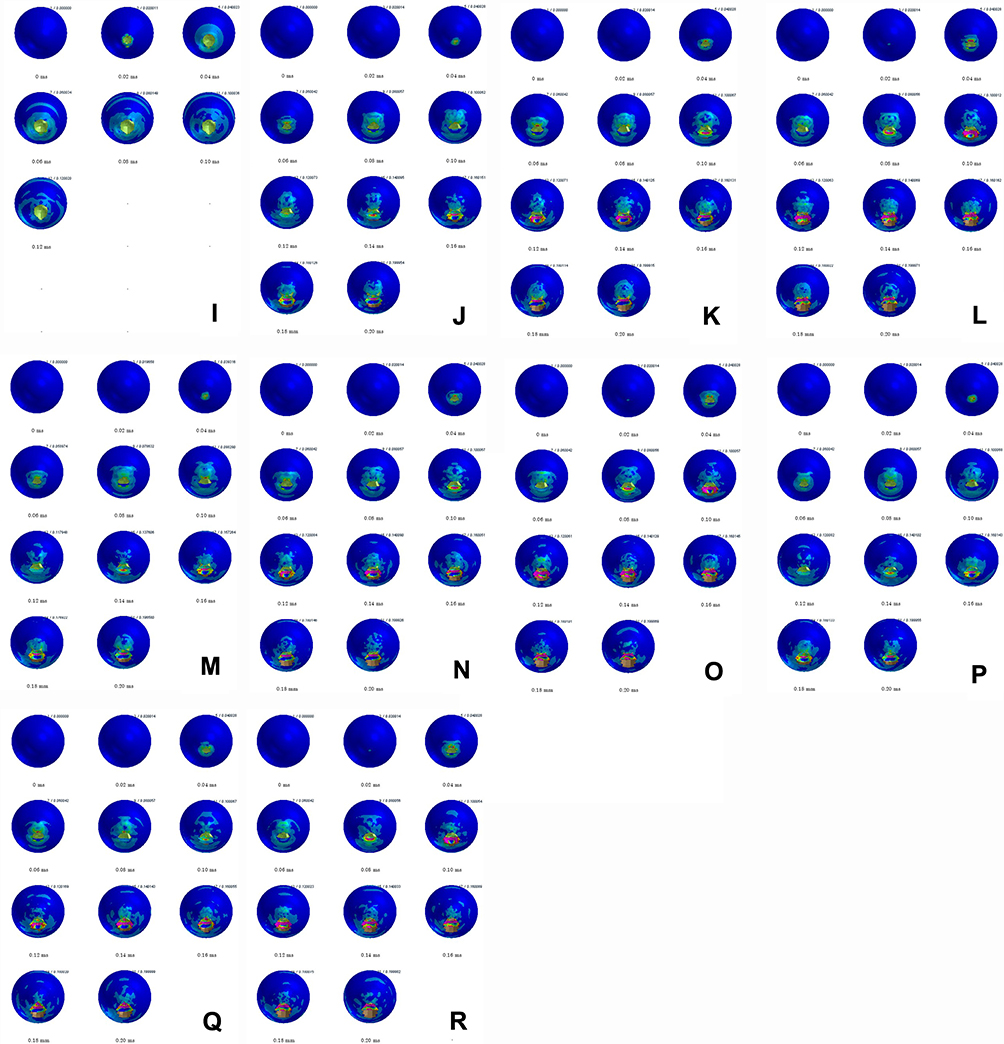 | 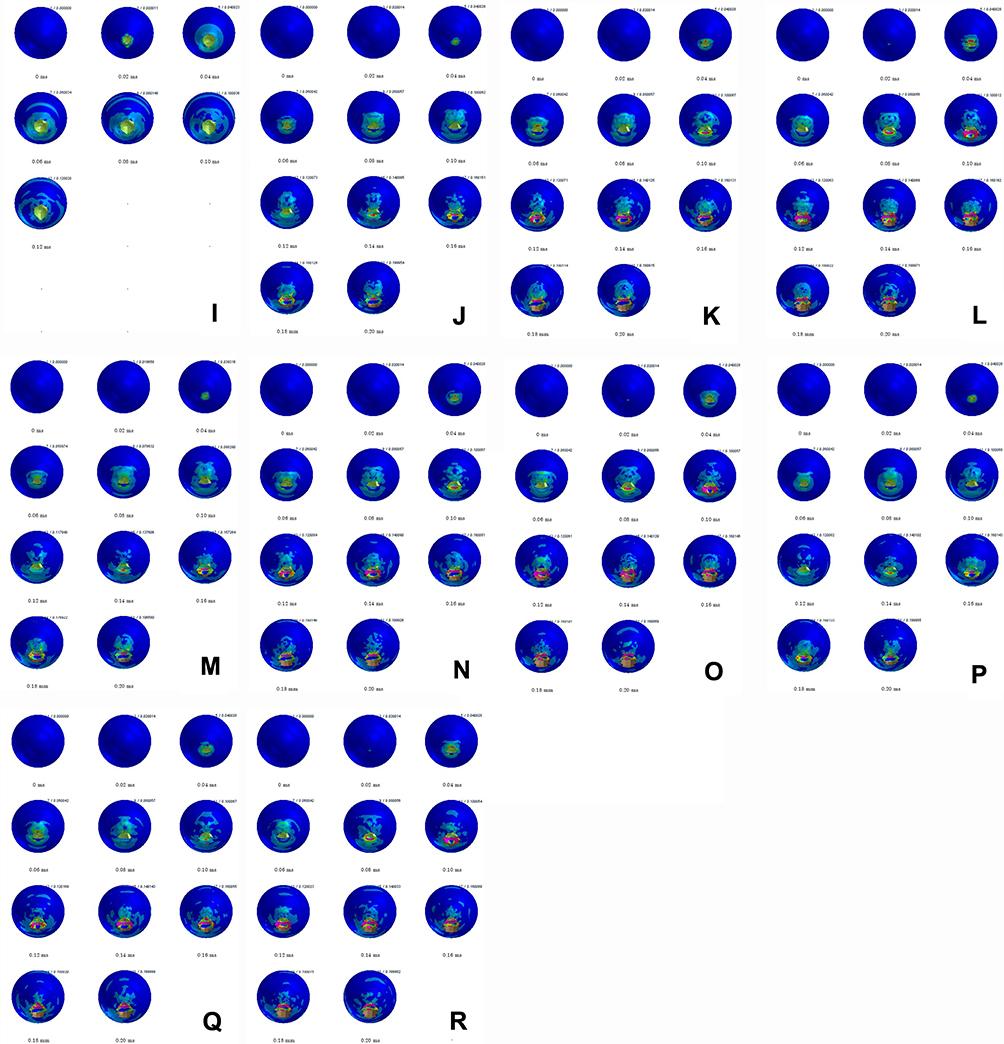 |
Figure 2 Continued. |
In general, simulation showed corneal damage was observed in all cases in the straight-gaze position (Table 1). However, the extent of damage varied according to the situation. In cases of 100% strength of the sutured region in the straight-gaze position, corneal strain hardly reached its threshold and graft dehiscence was not expected to occur in simulation (Figure 2G (0-100-45), Figure 2H (0-100-60) and Figure 2I (0-100-75)). In cases of 50% strength in the straight-gaze position, wound rupture seemed to occur in the early phase (0.04–0.06 ms) of impact at low speeds in simulation (Figure 2D (0-50-45), Figure 2E (0-50-60)). Despite the high-impact velocity (75 m/s), simulation showed corneal strain was limited in the early phase, but regional break was observed at 0.14 ms after the impact (Figure 2F (0-50-75)). Similar results were observed in cases of 30% strength in the straight-gaze position, and the corneal damage was dependent on the impact velocity (Figure 2A (0-30-45) and Figure 2B (0-30-60)), while regional break was found in the late phase (0.14 ms after impact) in cases with an impact velocity of 75 m/s in simulation (Figure 2C (0-30-75)).
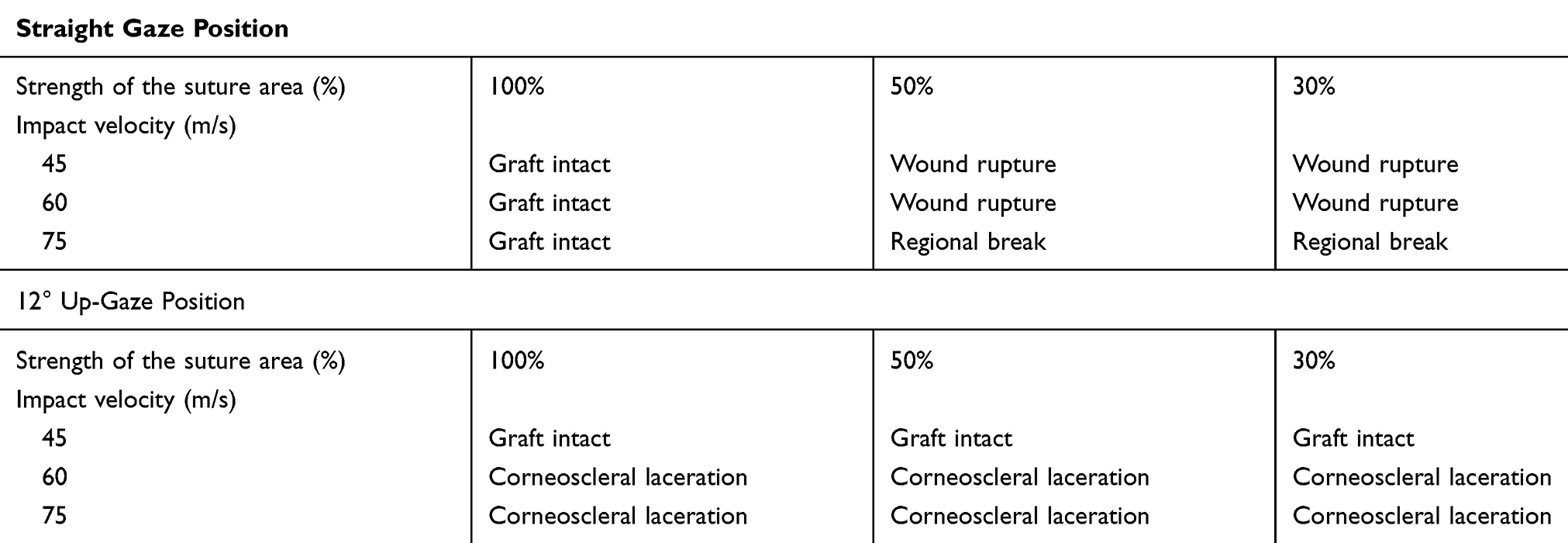 |
Table 1 Summary of Ocular Damage Observed in Simulation |
In contrast, simulation showed wound damage was observed in the lower quadrant of the cornea and adjacent sclera in 12° up-gaze cases (Table 1). Wound laceration hardly occurred at low impact velocity (45 m/s) (Figure 2M (12-50-45) and Figure 2P (12-30-45)) even in cases of 30% strength in simulation (Figure 2J (12-100-45)). At middle impact velocity (60 m/s), simulation showed wound damage was observed at 0.08 ms after the impact threatening corneoscleral laceration (Figure 2K (12-30-60), Figure 2N (12-50-60) and Figure 2Q (12-100-60)), and its area was larger than that in cases with low impact velocity. A larger damaged area was observed in high impact velocity cases and corneoscleral laceration was inevitable, while the extent of the damage did not show an apparent difference among all strengths in simulation (Figure 2L (12-30-75), Figure 2O (12-50-75) and Figure 2R (12-100-75)).
Discussion
Unlike with human bones and the ribcage, the injury biomechanics of soft organs, such as the human eye, are difficult to simulate due to limited available mechanical information. In addition, it is hard to simulate common causes of blunt trauma, such as from a finger, corner of a hard object or floor, because it is hard to estimate the physiological properties and impact velocity of these situations for simulation study. Thus, we selected an air gun pellet as the impacting object on the post-keratoplasty eye in this study because the physical properties and penetration speed are well known. While air gun ocular injury is a frequent cause of blunt trauma in children,23–27 blunt ocular rupture in the post-keratoplasty eye occurs relatively often in elderly patients.5 The incidence of globe rupture was reported to be 2.0% in eyes receiving PKP and 0.5% in eyes receiving deep anterior lamellar keratoplasty (DALK).5 The reported incidence of traumatic graft dehiscence among PKP eyes was 2.3 per 1000 person-years, and few cases of graft dehiscence were observed after DALK in other studies.6,14 These studies indicate that globe rupture after keratoplasty is a rare complication, and the incidence was higher after PKP than after DALK. Therefore, we carried out a simulation study on eyes after PKP in this study. However, it should be noted that globe rupture might occur in cases of DALK,6 and Descemet’s membrane might be considered a barrier against possible trauma, but there have been reports of cases of globe rupture after radial keratotomy28 and laser in situ keratomileusis.29 The cause of the dislocation of corneal graft was a fall or blunt trauma, from a branch, airbag, fist, or finger, in other reports.4,5 An air gun shot to the eye, especially to the post-keratoplasty eye, is a rare accident, but it can mimic an impact with a small object such as a branch, finger or fist; thus, this situation was adopted in this study. However, from the clinical standpoint in real life, a more common impacting object, such as an airbag while driving, seems more suitable for a simulation study of ocular injury, and we are planning a further simulation study based on our simulation model.
In this study, different results were observed in the two gaze positions. In straight-gaze position simulations, the avoidance of corneal laceration in 100% strength cases means that air gun impact does not necessarily result in serious globe damage if the property of the cornea is intact; in contrast, the damaged area coincided with the suture area and wound laceration was observed in the early phase (0.04–0.06 ms after the impact) in 30% and 50% strength cases at impact velocities of 45 m/s and 60 m/s, while regional break was observed at the same strength at high impact velocity (75 m/s) in the late phase (0.14 ms after the impact). The reason for the discordance in the phase of wound dehiscence between low-middle impact velocities and high impact velocity is unclear; however, these phenomena suggest the possibility of differences in kinetic and mechanical behavior after air gun impact according to the impact velocity on a millisecond scale, meaning that these so-called microenvironmental movements cannot be visualized unless a simulation study is carried out. Regarding postsurgical wound strength in PKP, several studies have been reported. Histopathological studies confirm that corneal wounds never regain their original strength, meaning that wound weakness persists for a long period after keratoplasty.30,31 Histopathological changes including incarceration of Bowman’s or Descemet’s membrane or retrocorneal fibrous tissue sealing the wound have been observed 25 years after surgery, indicating that corneal wounds continue to remain weak.30 Furthermore, postmortem studies of eyes that underwent PKP show incomplete wound healing microscopically at the graft-donor interface in 86.7% of patients.31 The results of these studies suggest that corneal damage around the suture area is most susceptible, especially in a straight-gaze impact by an air gun, and support our results.
In the simulation of 12° up-gaze, except at low impact velocity, corneoscleral damage and possible laceration were observed at middle and high impact velocities. The reason for these different results compared with straight-gaze simulations was not clear; however, the correlation between impact velocity and severity of the damaged area was considered to derive from the speculation that scleral factors play a more critical role in eccentric air gun impact due to kinetic energy also concentrated on the eccentric globe surface. We selected the 12° up-gaze position as the representation of a closing eye; therefore, these results support that prompt eye closing including protection of the eyelid itself may avoid serious corneal suture damage after PKP. Combining these results with those of our present study, it can be proposed that special precautionary measures should be considered in patients who have undergone PKP, especially elderly persons who are prone to injuries such as falls and being hit by objects. Therefore, detailed advice from ophthalmologists to avoid serious trauma including protective eyewear such as goggles is essential for patients who undergo PKP, even a long time after surgery. Recent studies also report that serious pediatric corneal damage has been increasing by air guns meaning that ocular damage is easily occur in 100% strength (intact) eye.32,33 These studies indicate the increasing necessity of regulations for eye protection, sales, and usage of air guns to prevent juvenile ocular injury due to air guns.32,33
There are several limitations of this study. First, weakness of the graft-recipient junction was simulated as a regional strain limit decrease in this study, while wound dehiscence occurs linearly around the graft-recipient junction clinically even if the suture remains across the graft-recipient junction. However, it is impossible to simulate a linear, so-called single-dimensional, strength decrease in the current simulation model; therefore, we introduced a concentric, so-called two-dimensional, sutured region in this study. Further refinement in computer technology will enable us to carry out more accurate simulation of air gun ocular impact that is closer to the clinical situation. Secondly, in several simulation cases, especially those with high impact velocity in the straight-gaze position, graphic output terminated before 0.16 ms. Because a high-velocity air gun pellet has a tendency to move into the eyeball due to its high energy, further simulation was interrupted according to element deletion method.14 These results, on the other hand, reflect the possibility of an intraocular foreign body injury from an air gun pellet as a small object penetrating injury.
In conclusion, FEA using a human eyeball model might be a useful method to analyze and predict the mechanical features of blunt ocular trauma after surgery including keratoplasty. The present study also revealed that wound suture strength, which has a critical relation with wound healing, primarily affects the clinical outcome and visual prognosis of blunt trauma such as that due to an air gun impact.
Ethics
The tissue from human cadavers referred to in this study relates to earlier, entirely separate experiments, and that no human tissue was used specifically for the study.
Acknowledgments
This work was supported by a Grant-in-Aid for Encouragement of Scientists (15K10911) from the Ministry of Education, Science, Sports and Culture of Japan. We thank Dr. W. Gray for editing this manuscript.
Disclosure
The authors report no conflict of interest in this work.
References
1. Tzelikis PF, Fenelon EM, Yoshimoto RR, Rascop GP, Queiroz RL, Hida WT. Traumatic wound dehiscence after corneal keratoplasty. Arq Bras Oftalmol. 2015;78(5):310–312. doi:10.5935/0004-2749.20150081
2. Rohrbach JM, Weidle EG, Steuhl KP, Meilinger S, Pleyer U. Traumatic wound dehiscence after penetrating keratoplasty. Acta Ophthalmol Scand. 1996;74(5):501–505. doi:10.1111/j.1600-0420.1996.tb00608.x
3. Meyer JJ, McGhee CN. Incidence, severity and outcomes of traumatic wound dehiscence following penetrating and deep anterior lamellar keratoplasty. Br J Ophthalmol. 2016;100(10):1412–1415. doi:10.1136/bjophthalmol-2015-307604
4. Steinberg J, Eddy MT, Katz T, Fricke OH, Richard G, Linke SJ. Traumatic wound dehiscence after penetrating keratoplasty: case series and literature review. Eur J Ophthalmol. 2012;22(3):335–341. doi:10.5301/ejo.5000057
5. Kawashima M, Kawakita T, Shimmura S, Tsubota K, Shimazaki J. Characteristics of traumatic globe rupture after keratoplasty. Ophthalmology. 2009;116(11):2072–2076. doi:10.1016/j.ophtha.2009.04.047
6. Kalantan H, Al-Shahwan S, Al-Torbak A. Traumatic globe rupture after deep anterior lamellar keratoplasty. Indian J Ophthalmol. 2007;55(1):69–70. doi:10.4103/0301-4738.29502
7. Agrawal V, Wagh M, Krishnamachary M, Rao GN, Gupta S. Traumatic wound dehiscence after penetrating keratoplasty. Cornea. 1995;14(6):601–603. doi:10.1097/00003226-199511000-00013
8. Bowman RJ, Yorston D, Aitchison TC, McIntyre B, Kirkness CM. Traumatic wound rupture after penetrating keratoplasty in Africa. Br J Ophthalmol. 1999;83(5):530–534. doi:10.1136/bjo.83.5.530
9. Elder MJ, Stack RR. Globe rupture following penetrating keratoplasty: how often, why, and what can we do to prevent it? Cornea. 2004;23(8):776–780. doi:10.1097/01.ico.0000133996.99520.c4
10. Lam FC, Rahman MQ, Ramaesh K. Traumatic wound dehiscence after penetrating keratoplasty-a cause for concern. Eye (Lond). 2007;21(9):1146–1150. doi:10.1038/sj.eye.6702407
11. Hines-Beard J, Marchetta J, Gordon S, Chaum E, Geisert EE, Rex TS. A mouse model of ocular blast injury that induces closed globe anterior and posterior pole damage. Exp Eye Res. 2012;99(3):63–70. doi:10.1016/j.exer.2012.03.013
12. Viano DC, King AI, Melvin JW, Weber K. Injury biomechanics research: an essential element in the prevention of trauma. J Biomech. 1989;2(5):403–417. doi:10.1016/0021-9290(89)90201-7
13. Uchio E, Ohno S, Kudoh J, Aoki K, Kisielewicz LT. Simulation model of an eyeball based on finite element analysis method on a supercomputer. Br J Ophthalmol. 1999;3(10):1106–1111. doi:10.1136/bjo.83.10.1106
14. Uchio E, Ohno S, Kudoh K, Kadonosono K, Andoh K, Kisielewicz LT. Simulation of airbag impact on post-radial keratotomy eye using finite element analysis. J Cataract Refract Surg. 2001;27(11):1847–1853. doi:10.1016/S0886-3350(01)00966-X
15. Uchio E, Watanabe Y, Kadonosono K, Matsuoka Y, Goto S. Simulation of airbag impact on eyes with transsclerally fixated posterior chamber intraocular lens using finite element analysis. J Cataract Refract Surg. 2004;30(2):483–490. doi:10.1016/S0886-3350(03)00520-0
16. Uchio E, Kadonosono K, Matsuoka Y, Goto S. Simulation of airbag impact on eyes after photorefractive keratectomy by finite element analysis method. Graefes Arch Clin Exp Ophthalmol. 2003;241(6):497–504. doi:10.1007/s00417-003-0679-8
17. Huang J, Uchio E, Goto S. Simulation of airbag impact on eyes with different axial lengths after transsclerally fixated posterior chamber intraocular lens by using finite element analysis. Clin Ophthalmol. 2015;9:263–270. doi:10.2147/OPTH.S75180
18. Buzard KA. Introduction to biomechanics of the cornea. Refract Corneal Surg. 1992;8(2):127–138.
19. Greene PR. Closed-form ametropic pressure-volume and ocular rigidity solutions. Am J Optom Physiol Opt. 1985;62(12):870–878. doi:10.1097/00006324-198512000-00008
20. Hoeltzel DA, Altman P, Buzard K, Choe K. Strip extensiometry for comparison of the mechanical response of bovine, rabbit, and human corneas. J Biomech Eng. 1992;114(2):202–215. doi:10.1115/1.2891373
21. Ruan JS, Prasad P. Coupling of a finite element human head model with a lumped parameter Hybrid III dummy model: preliminary results. J Neurotrauma. 1995;12(4):725–734. doi:10.1089/neu.1995.12.725
22. Jiang B, Zhu F, Cao L, Presley BR, Shen MS, Yang KH. Computational study of fracture characteristics in infant skulls using a simplified finite element model. J Forensic Sci. 2017;62(1):39–49. doi:10.1111/jfo.2017.62.issue-1
23. Shuttleworth GN, Galloway P, Sparrow JM, Lane C. Ocular air gun injuries: a one-year surveillance study in the UK and Eire (BOSU). 2001–2002. Eye (Lond). 2009;23(6):1370–1376. doi:10.1038/eye.2008.275
24. Shuttleworth GN, Galloway PH. Ocular air-gun injury: 19 cases. J R Soc Med. 2001;94(8):396–399. doi:10.1177/014107680109400806
25. Aziz M, Patel S. BB gun-related open globe injuries. Ophthalmol Retina. 2018;2(10):1056–1061. doi:10.1016/j.oret.2018.03.006
26. Ahmadabadi MN, Karkhaneh R, Valeshabad AK, Tabatabai A, Jager MJ, Ahmadabadi EN. Clinical presentation and outcome of perforating ocular injuries due to BB guns: a case series. Injury. 2011;42(5):492–495. doi:10.1016/j.injury.2010.11.006
27. Ramstead C, Ng M, Rudnisky CJ. Ocular injuries associated with airsoft guns: a case series. Can J Ophthalmol. 2008;43(5):584–587. doi:10.3129/i08-131
28. Rashid ER, Waring GO
29. Sun CC, Chang SW, Tsai RR. Traumatic corneal perforation with epithelial ingrowth after laser in situ keratomileusis. Arch Ophthalmol. 2001;119(6):907–909.
30. Flaxel JT, Swan KC. Limbal wound healing after cataract extraction. A histologic study. Arch Ophthalmol. 1969;81(5):653–659. doi:10.1001/archopht.1969.00990010655010
31. Lang GK, Green WR, Maumenee AE. Clinicopathologic studies of keratoplasty eyes obtained post mortem. Am J Ophthalmol. 1986;101(1):28–40. doi:10.1016/0002-9394(86)90461-7
32. Lee R, Fredrick D. Pediatric eye injuries due to nonpowder guns in the United States, 2002–2012. J AAPOS. 2015;19(2):163–168. doi:10.1016/j.jaapos.2015.01.010
33. Jovanović MB. Eye injuries caused by shotgun and air-rifles treated at the University Eye Clinic in Belgrade 2000–2009. Srp Arh Celok Lek. 2014;142(1–2):6–9. doi:10.2298/SARH1402006J
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.