")
Back to Journals » Journal of Asthma and Allergy » Volume 13
Fertility Treatment Resulting in Live Births in Women with Asthma – Associated with Perennial Allergy?
Authors Tidemandsen C , Vejen Hansen A, Backer V , Gade EJ, Ali Z , Suppli Ulrik C
Received 22 January 2020
Accepted for publication 3 April 2020
Published 24 April 2020 Volume 2020:13 Pages 145—152
DOI https://doi.org/10.2147/JAA.S246873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Casper Tidemandsen,1 Anne Vejen Hansen,1 Vibeke Backer,2 Elisabeth Juul Gade,3 Zarqa Ali,4 Charlotte Suppli Ulrik1,2
1Department of Respiratory Medicine, Hvidovre Hospital, Hvidovre, Denmark; 2Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 3Department of Gynecology and Obstetrics, Rigshospitalet, Copenhagen, Denmark; 4Department of Dermatology and Wound Healing Centre, Bispebjerg Hospital, Copenhagen, Denmark
Correspondence: Casper Tidemandsen
Respiratory Research Unit Hvidovre, Department of Respiratory Medicine, Hvidovre University Hospital, Kettegård Alle 30, Hvidovre DK-2650, Denmark
Tel +45 50751516
Email [email protected]
Background: Asthma has been linked with prolonged time to pregnancy compared to healthy controls, also asthma has been linked to a higher need for fertility treatment. However, knowledge of the possible association between allergy and need for fertility treatment is limited. Our aim was to explore a possible difference in having had fertility treatment in women with asthma and live births in those with perennial allergy (animals, fungi and dust mites) compared to no allergy/seasonal allergy. The primary outcome of interest was fertility treatment.
Patients and Methods: Women enrolled in the Management of Asthma during Pregnancy (MAP) program at Hvidovre Hospital, DK, were included in the present analysis provided they fulfilled the following criteria: 1) diagnosed with asthma and current anti-asthma therapy and 2) first visit to the respiratory outpatient clinic within the first 18 weeks of pregnancy. Participants were divided into two groups: asthma with perennial allergy (cases) and asthma with seasonal/no allergy (controls). Logistic regression analysis was applied, and findings expressed as odds ratios (OR).
Results: Among women with asthma and perennial allergy (n=544 cases), 13.8% (n=75) had fertility treatment, compared to only 10.1% (n=39) among women with asthma and seasonal/no allergy (n=388, controls) (OR 1.43, 95% CI 0.95– 2.16, p=0.087). This association remained statistically insignificant after adjusting for confounders, including BMI (OR 1.19, 95% CI 0.77– 1.84, p=0.433). In women ≥ 35 years of age, 28% (n=44) and 20% (n=19), respectively, among cases and controls had fertility treatment (OR 1.60, 95% CI 0.87– 2.94, p=0.132), and likewise, statistically insignificant after adjusting for confounders (OR 1.41, 95% CI 0.74– 2.69, p< 0.293).
Conclusion: In women with asthma and live births, our study revealed a trend towards an association between perennial allergy and a higher need for fertility treatment compared to seasonal/no allergy.
Keywords: asthma, allergy, pregnancy, IVF, ART, fertility, atopy
Background
In the western world, both asthma and infertility are among the most common chronic conditions among women of reproductive age.1 Asthma is estimated to affect 8–12% of the young population, whereas infertility is estimated to affect about 10% of the young population.2,3
Recent studies have reported impaired fertility in couples where the women suffer from asthma.4,5 A register study by Gade et al6 showed a prolonged time to pregnancy (TTP) and a tendency towards an increased number of miscarriages among women with asthma, particularly among those with severe asthma and above 30 years of age. This is further supported by Hansen et al5 who reported a higher need for fertility treatment among women with asthma compared to women without asthma. Whether well-controlled asthma improves fertility is not entirely clear, Källen et al7 found an increased incidence of infertility (involuntary childlessness) among women prescribed anti-asthma drugs. However, Grzeskowiak et al showed that women with asthma treated with only rescue asthma medication had reduced fertility compared to those treated with asthma controller medication (15% lower (0.85 (95% CI 0.75–0.96))).8 The available evidence, therefore, suggests that poorly controlled asthma may have a negative impact on fertility. Furthermore, a lower number of children among allergic women have been found by Karmaus and Botezan.9 However, Gade et al found no significant association between allergy, defined as a positive skin prick test, and changes in time to pregnancy.6 They found that women with only allergy had comparable time to pregnancy as the general population.6 While women with both asthma and allergy experienced prolonged TTP, which was comparable to having asthma alone.6 The data on asthma combined with allergy are contradictive; however, most recent data points towards an association between reduced fertility and female asthma.
Most available studies have primarily compared fertility in women with asthma and healthy controls. So far little evidence has been published comparing different sub-groups of women with asthma, in regard to fertility.
Our aim was to explore a possible difference in having had fertility treatment in women with asthma and live births in those with perennial allergy (animals, fungi and dust mites) compared to no allergy/seasonal allergy. The primary outcome was fertility treatment.
Patients and Methods
Materials
Management of Asthma during Pregnancy (MAP) program was initiated in 2007, it is a prospective cohort study with pregnant women which consecutively have been recruited through the Department of Gynecology and Obstetrics, Hvidovre Hospital, Denmark. If pregnant and referred to Hvidovre Hospital (HvH) (approximately 7.000 per year, corresponding to 10% of infants born in Denmark) the women received a welcome letter from the Department of Gynecology and Obstetrics informing the women about the study and an invitation to participate in the MAP-program. The acceptance to participate was done by e-mail ([email protected]). If the women accepted the invitation, they were given a scheduled appointment (by letter) at the out-patient clinic in the Respiratory department. All participating women with asthma were included within the first 18 weeks of their pregnancy, and were followed-up assessment of asthma control, including spirometry and exhaled nitric oxide, approximately every 4 weeks throughout pregnancy.
Data come from the same cohort reported in 2019 comparing the entire asthma cohort to non-asthmatic controls in regards to the need for fertility treatment.5
Methods
Information on fertility treatment (2007 to 2013) was obtained from the Danish National Assisted Reproductive Technology (ART) registry and the Medical Birth Registry. The Danish ART registry includes all ART treatment-cycles performed in public and private fertility clinics in Denmark since 1994, with intrauterine insemination (IUI) cycles added in 2006. Reporting to the ART registry is mandatory for both public and private clinics. A unique personal identification number enables identification of all treatment cycles received by each individual woman, and thereby mapping of the complete fertility treatment history. Women identified in the Danish ART registry were cross-linked with the Danish Medical Birth registry to identify all live births from the same woman.
Outcome
The variables that were analyzed were fertility treatment-related live births and births after spontaneous conception in women with perennial allergy (animals, fungi and dust mites) compared to women with asthma and seasonal allergy or no allergy.
Fractional Exhaled Nitric Oxide (FeNO)
The measurement of Fe
Spirometry
Spirometry was performed using the Easy One Ultrasonic spirometer (NDD; Zurich, Switzerland), according to the American Thoracic Society (ATS)/European Respiratory Society recommendation,11 and predicted values for FEV1 and FVC were calculated according to reference equations.12 FEV1% ≥80% of the predicted value and a FEV1/FVC-ratio, value of >0.7, were considered within the normal range. .
Allergy
Allergy status was based on the previous testing for atopy, that is skin prick testing13 and/or measuring blood levels of specific IgE to common aeroallergens and evaluated according to international guidelines, together with patient-reported allergic symptoms, including, eg, symptoms of rhino-conjunctivitis and asthma, triggered by relevant exposure, as evaluated at the first visit to the respiratory outpatient clinic by one specialist in respiratory medicine (CSU).
The Cohort was divided into two main groups, perennial allergy (ie, cases) and seasonal/no allergy (ie controls), and subsequently further divided into three subgroups: “perennial allergy” (animals, fungi and dust mite), “seasonal allergy” (airborne allergens, eg, pollen, that appear only during certain times of the year) and “no allergy”. Patients with both perennial and seasonal allergy were allocated to the perennial allergy group.
Statistical Analysis
The Data were analyzed by using IBM SPSS Statistics version 22.0. Utilizing the two-tailed Student’s t-test we analyzed continuous and primarily descriptive variables. Binary outcomes of interest were analyzed using the chi-square test. To estimate the odds ratio (OR) we used logistic regression analysis with 95% confidence intervals (CI) for the association between allergic appearance (ie, cases vs controls) and fertility treatment. The OR was adjusted for the following potential confounding variables: body mass index (BMI), smoking status, maternal age at time of giving birth, primiparity, being single and in a same-sex partnership, allergy treatment and asthma severity (defined according to GINA-guidelines14). A p-value <0.05 was considered significant.
We chose to include the following variables in our model: body mass index (BMI), as high BMI has been shown to influence fertility negatively,15 maternal age as increasing age lowers the female fertility,16 smoking status as smoking decreases fertility,17 being single and in a same-sex partnership,18 allergy treatment19 into our model.
Results
Baseline Characteristics
A total of 872 women with asthma, contributing to 932 pregnancies, were included in the present analysis. The cohort was divided into two main groups: Those with perennial allergy (n=544) and those with seasonal/no allergy (n=388). Women with perennial allergy (cases) were older and more often non-smokers compared to the control group, see Table 1 for detailed numbers. Subsequently, those with seasonal/no allergy was further subdivided into seasonal (n=210) vs no allergy (n=178).
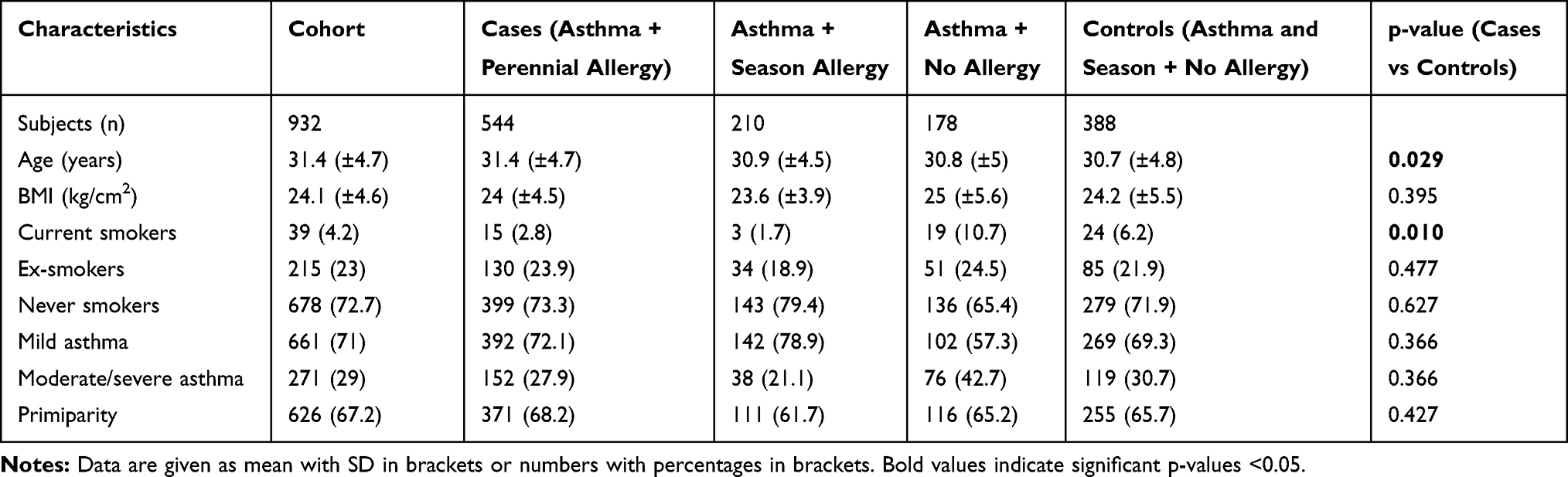 |
Table 1 Demographic Characteristics of the Study Population Comprising 932 Individuals Divided in Different Groups After Allergy Status |
Asthma Characteristics
No significant differences were found between cases and controls regarding lung function (FEV1 < 80% vs FEV1 > 80%; p=0.237), FENO (low/high) (FENO ≤ 50 ppb vs FENO > 50 ppb; p=0.360) or prescribed treatment with inhaled corticosteroids (ICS) (yes/no) (p=0.168) among women who conceived naturally and in those conceiving after fertility treatment.
Baseline characteristics, including use of asthma medication and lung function, of the cohort are presented in Table 2.
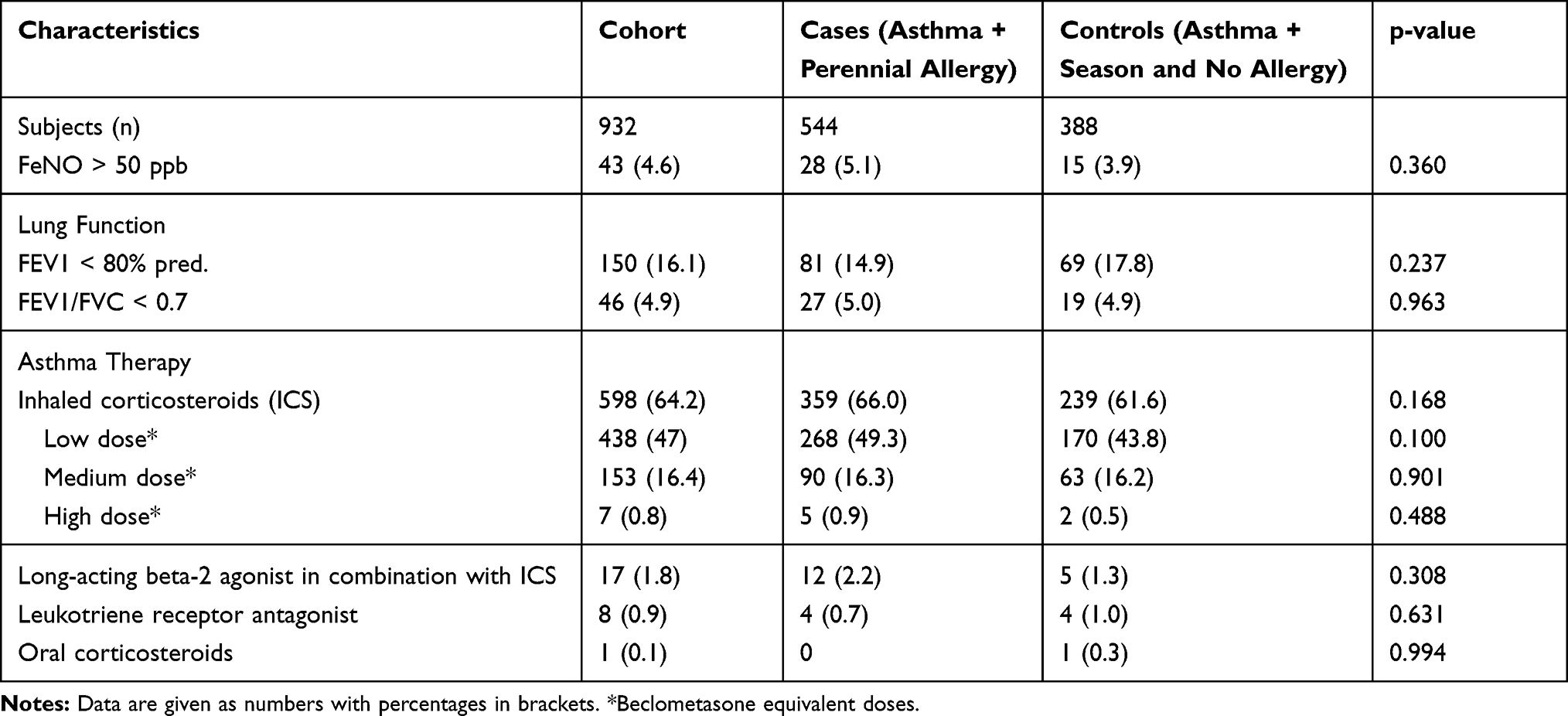 |
Table 2 Characteristics of the Lung Function and Asthma Therapy in the Cohort at First Visit in the Management of Asthma During Pregnancy Program |
Fertility Treatment Among Cases and Controls
The prevalence of fertility treatment ahead of live births was 13.8% (n=75) among women with asthma and perennial allergy compared to 10.1% (n= 39) in the control group (OR 1.43, 95% CI 0.95–2.16, p<0.087). After adjusting for BMI, status, primiparity, age, being single, smoking, in same-sex relationship, asthma severity, and allergy treatment (oral antihistamine, eye drops and nasal steroids) the association remained statistically non-significant (OR 1.19, 95% CI 0.77–1.84, p = 0.433). Repeating the analysis with women only contributing to their first pregnancy did not change the overall observations (n=872).
When looking at the different types of fertility treatment (IUI and ART, there was no significant difference between groups in regard to IUI treatment (OR 1.23, 95% CI 0.67–2.27, p=0.510) and Assisted Reproductive Technology (ART= IVF and ICSI) treatment (OR 1.54, 95% CI 0.91–2.60, p = 0.109), also after adjusting for confounders (Table 3).
 |
Table 3 Mode of Conception and Specified Fertility Treatment in Women with Asthma in Regards to Allergy with Live Births |
Fertility Treatment Stratified by Age Among Women with Asthma and Perennial Allergy vs Women with Asthma and Seasonal/No Allergy
After stratifying cases and controls into two age-groups, ie, of women <35 years and women ≥35 years, we re-analyzed fertility treatment and no significant association was found between women with asthma and perennial allergy and women with asthma and seasonal/no allergy in regard to fertility treatment. In women ≥35 years, it was 28% (n=44) and 20% (n=19) of cases and controls, respectively (OR 1.60, 95% CI 0.87–2.94, p=0.132)
Causes of Infertility in Women Who Received Fertility Treatment, Cases vs Controls
When exploring causes of infertility in the two groups there was no significant difference, ie, male factor, female factor, combined or idiopathic, between the women with asthma and perennial allergy and women with asthma and seasonal/no allergy. The causes of infertility were equally distributed within each group (Table 4). Likewise, no difference was found between the groups in type of fertility treatment.
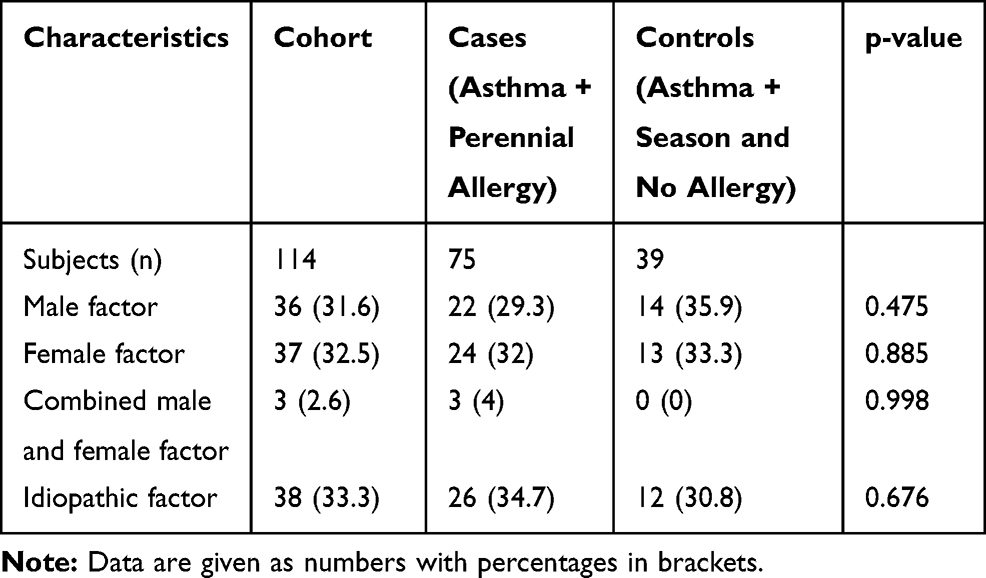 |
Table 4 Characteristics of the Reasons for Fertility Treatment Within Those Who Received Fertility Treatment, Management of Asthma During Pregnancy Program |
Discussion
In this study, our findings did not reach statistical significance; however, one could argue we found a trend towards that more women with perennial allergy conceived after fertility treatment compared to women with either seasonal allergy or no allergy.
As shown in the study by Gade et al6 and Hansen et al5 when stratifying for age (aged 35 years or older), the association between asthma and need for fertility treatment was stronger compared to the general population. In our study of allergic asthma patients, we found no statistical difference between the two asthma groups when dividing the cohort in <35 years and women ≥35 years. Our contradictive results could be explained by a possible underpowered study.
In the study conducted by Tata et al,20 there was no association between allergic disease and need for fertility treatment. However, they showed an increased fertility within the younger participants with allergic diseases compared to women without allergic diseases. In our study, we found a trend towards an increased association between asthma with perennial allergy and infertility compared to only asthma and infertility. The explanation for this finding could be that perennial due to its daily symptoms and thereby chronic feature has a greater effect on both the lungs and systemically. This assumption is based on a review of available studies, Ulrik21 that describes that loss of lung function was higher in patients with daily symptoms compared to those having seasonally asthma. Leading to the assumption that perennial asthma was more severe than seasonal asthma. Furthermore, earlier findings have indicated that years exposed to low-grade systemic inflammation in women with asthma may have an influence on fertility,22–24 in our study we found no difference within the groups as regards to age, a possibility could be that an allergic component does not influence fertility more over time. After adjusting for basic and lifestyle-related factors there was still no significant difference.
However, a trend towards more women receiving ART among the cases compared to the controls (8.5% vs 5.7% p=0.109) was found. This could point towards a more difficult treatable infertility due to a higher level of atopic disease.
Strengths and Limitations
A strength of the study is that it was conducted at a hospital with a large number of deliveries covering 10% of all births every year in Denmark and that the hospital covers a population with a wide range of socio-economical classes. Because of national data on fertility treatment, we have complete coverage of those who received fertility treatment. The risk of selection bias is very low due to this national register design. Most important, the same physician validated all the cases who were diagnosed with asthma and allergy therefore the validity of the diagnoses is very high.
One limitation of the study is that only women with asthma and live births were included. Thus, women with asthma who received fertility treatment without conceiving were not included, which is a potential bias, but unfortunately, we do not have access to these data.
Another important bias is a possible underpowered study, as the result shows a trend of an association between perennial allergy and increased need for fertility treatment, but the results are not significant. After a thorough review of the power calculation, the cohort should be almost double in size, to be able to detect a significant difference. Finally, on the basis of the prevalence of asthma in Denmark,25 out of all the women with asthma giving birth each year at Hvidovre Hospital, approximately two-third are enrolled in the MAP program. It is of course a possibility that the last third of the women with asthma who do not choose to be enrolled in the MAP program is different from the two-thirds that do. Several studies have shown that people who voluntarily participate in studies are more resourceful and socio-economically strong women.26–29 In our cohort, all participants have voluntarily participated; therefore, it should not be a difference related to this in the present study.
Interpretation in the Context of Other Studies
Publication on the effect of allergies on fertility is limited. There are studies published addressing allergy and pregnancy. It has been proposed that mast cell products such as histamine and prostaglandins can cause contractions in the uterus tissue. The uterus lining is in abundance of mast cells. The myometrium fibers produce muscle contractions when exposed to the right allergen.30 It is possible this also holds true at conception, as the embryo need to attach to the endometrium in the uterus.
Another possibility could be that the immune system acts in an autoimmune way. The immune system reacts to the embryo being implanted in the uterus lining, a reaction to the embryo antigen. It has earlier been made a convincing connection between autoimmune diseases and adverse pregnancy outcome.31 A study in 2010 found a connection between drug allergy, need for fertility treatment and adverse pregnancy outcomes.32
It has been hypothesized that the underlying reason for asthma affecting fertility negatively is the increased inflammatory level in the body is increased. Growth factors have been shown to be involved in the inflammatory response of asthma33 and are also known to play an important role in the process of implantation of the embryo.34 Balance between Th1 and Th2 responses in the adaptive immune system has been considered important. As the allergic response also is Th2 driven it is not unlikely this is a contributing factor to asthma affecting fertility. This mismatch in Th1 and Th2 response may be of importance.34 Following these hypotheses, it seems likely that allergy in combination with asthma can affect fertility, but we are still in need of a better understanding of the actions, interactions and immunological functions.
As far as asthma severity or asthma therapy and the need for fertility treatment, we found no association.
Conclusion
A trend towards an association between perennial allergy and asthma and the need for fertility treatment compared to seasonal/no allergy, possibly statistically insignificant due to the relatively small sample size. The trend towards an association between female asthma with perennial allergy and a reduction in fertility needs to be further explored, preferably with a larger sample size.
Data Sharing Statement
Raw data were generated at Hvidovre hospital. Derived data supporting the findings of this study are available from the corresponding author CT on request.
Ethics and Consent Statement
The MAP study is approved by the Research Ethics Committee of the Capital Region of Denmark (H-D-2007-0051) and permission has also been obtained from the Danish Data Protection Agency (2007-41-0770). Al participants have given consent for publication.
Author Contributions
The MAP program was initiated and developed by CSU. AVH and ZA have composed the data set. CT had full access to all of the data in the study and takes responsibility for the accuracy of the data analysis. CT drafted and revised the manuscript, VB, AVH, ZA, EJG and CSU contributed substantially to the interpretation, and the writing of the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
We want to acknowledge the financial support from Novartis. The abstract of this paper was presented at the EACCI Conference 2019 as a poster presentation with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nielsen HS, Schmidt L, Nyboe Andersen A, et al. Forebyggelse Af Nedsat Frugtbarhed. København: Vidensråd for Forebyggelse; 2016.
2. Kwon HL, Belanger K, Bracken MB. Asthma prevalence among pregnant and childbearing-aged women in the United States: estimates from national health surveys. Ann Epidemiol. 2003. doi:10.1016/S1047-2797(03)00008-5
3. Vander Borght M, Wyns C. Fertility and infertility: definition and epidemiology. Clin Biochem. 2018;62:2–10. doi:10.1016/j.clinbiochem.2018.03.012
4. Gade EJ, Thomsen SF, Lindenberg S, Backer V. Fertility outcomes in asthma: a clinical study of 245 women with unexplained infertility. Eur Respir J. 2016;47(4):1144–1151. doi:10.1183/13993003.01389-2015
5. Hansen AV, Ali Z, Malchau SS, Blafoss J, Pinborg A, Ulrik CS. Fertility treatment among women with asthma: a case-control study of 3689 women with live births. Eur Respir J. 2019;53(2):1800597. doi:10.1183/13993003.00597-2018
6. Gade EJ, Thomsen SF, Lindenberg S, Kyvik KO, Lieberoth S, Backer V. Asthma affects time to pregnancy and fertility: a register-based twin study. Eur Respir J. 2014;43(4):1077–1085. doi:10.1183/09031936.00148713
7. Källén B, Otterblad Olausson P. Use of anti-asthmatic drugs during pregnancy. 1. Maternal characteristics, pregnancy and delivery complications. Eur J Clin Pharmacol. 2007. doi:10.1007/s00228-006-0257-1
8. Grzeskowiak LE, Smithers LG, Grieger JA, et al. Asthma treatment impacts time to pregnancy: evidence from the international SCOPE study. Eur Respir J. 2018;51(2):1702035. doi:10.1183/13993003.02035-2017
9. Karmaus W, Botezan C. Does a higher number of siblings protect against the development of allergy and asthma? A review. J Epidemiol Community Health. 2002;56(3):209–217. doi:10.1136/jech.56.3.209
10. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
11. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Series “‘ATS/ERS Task Force: standardisation of lung function testing ’” Edited by V. Brusasco, R. Crapo and G. Viegi. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
12. Quanjer P, Tammeling G, Cotes J, Pedersen O, Peslin R, Yernault J. Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl. 1993;16:5–40. doi:10.1183/09041950.005s1693
13. Heinzerling L, Mari A, Bergmann KC, et al. The skin prick test - European standards. Clin Transl Allergy. 2013;3(1):1–10. doi:10.1186/2045-7022-3-3
14. Www.ginasthma.com. GINA-guidelines. Available from: www.ginasthma.com.
15. Zain MM, Norman RJ. Impact of obesity on female fertility and fertility treatment. Women’s Health. 2008;4(2):183–194. doi:10.2217/17455057.4.2.183
16. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice and The Practice Committee of the American Society for Reproductive Medicine. Female age-related fertility decline: committee Opinion No. 589. Fertil Steril. 2014;101(3):633–634. doi:10.1016/j.fertnstert.2013.12.032.
17. Sansone A, Di Dato C, de Angelis C, et al. Smoke, alcohol and drug addiction and male fertility. Reprod Biol Endocrinol. 2018;16:1. doi:10.1186/s12958-018-0320-7
18. Nazem TG, Chang S, Sekhon L, et al. Do same sex couples and single women undergoing ovulation induction with oral agents and intrauterine insemination have outcomes comparable to infertile heterosexual couples? Fertil Steril. 2017;108(3):e7–e8.
19. Wasilewska E, Małgorzewicz S. Impact of allergic diseases on fertility. Eur Respir J. 2019;36(5):507–512. doi:10.5114/ada.2019.89501
20. Tata LJ, Hubbard RB, McKeever TM, et al. Fertility rates in women with asthma, eczema, and hay fever: a general population-based cohort study. Am J Epidemiol. 2007;165(9):1023–1030. doi:10.1093/aje/kwk092
21. Ulrik CS. Outcome of asthma: longitudinal changes in lung function. Eur Respir J. 1999;13(4):904. doi:10.1034/j.1399-3003.1999.13d35.x
22. Koga K, Mor G. Expression and function of Toll-like receptors at the maternal-fetal interface. Reprod Sci. 2008;15(3):231–242. doi:10.1177/1933719108316391
23. Yoshinaga K. Review of factors essential for blastocyst implantation for their modulating effects on the maternal immune system. Semin Cell Dev Biol. 2008;19(2):161–169. doi:10.1016/j.semcdb.2007.10.006
24. Zybzhitskaia LB, Shapovalova EA, Lavrova OV, Dymarskaia I, Arzhanova ON. [Placenta of normal women and of patients with bronchial asthma of various degrees of severity (immunohistochemical and histological study)]. Morfol. 2014;145:46–52. Russian.
25. Thomsen SF, Ulrik CS, Larsen K, Backer V. Change in prevalence of asthma in Danish children and adolescents. Ann Allergy Asthma Immunol. 2004;92(5):506–511. doi:10.1016/S1081-1206(10)61757-7
26. Lagerlund M, Sparén P, Thurfjell E, Ekbom A, Lambe M. Predictors of non-attendance in a population-based mammography screening programme; socio-demographic factors and aspects of health behaviour. Eur J Cancer Prev. 2000;9(1):25–34. doi:10.1097/00008469-200002000-00004
27. Banks E, Beral V, Cameron R, et al. Comparison of various characteristics of women who do and do not attend for breast cancer screening. Breast Cancer Res. 2002. doi:10.1186/bcr418
28. Lagerlund M, Maxwell AE, Bastani R, Thurfjell E, Ekbom A, Lambe M. Sociodemographic predictors of non-attendance at invitational mammography screening - a population-based register study (Sweden). Cancer Causes Control. 2002;13(1):73–82. doi:10.1023/A:1013978421073
29. Sabates R, Feinstein L. The role of education in the uptake of preventative health care: the case of cervical screening in Britain. Soc Sci Med. 2006;62(12):2998–3010. doi:10.1016/j.socscimed.2005.11.032
30. Garfield RE, Irani AM, Schwartz LB, Bytautiene E, Romero R. Structural and functional comparison of mast cells in the pregnant versus nonpregnant human uterus. Am J Obstet Gynecol. 2006;194(1):261–267. doi:10.1016/j.ajog.2005.05.011
31. Breckler LA, Hale J, Taylor A, Dunstan JA, Thornton CA, Prescott SL. Pregnancy IFN-γ responses to foetal alloantigens are altered by maternal allergy and gravidity status. Allergy Eur J Allergy Clin Immunol. 2008;63(11):1473–1480. doi:10.1111/j.1398-9995.2008.01718.x
32. Ohel I, Levy A, Zweig A, Holcberg G, Sheiner E. Pregnancy complication and outcome in women with history of allergy to medicinal agents. Am J Reprod Immunol. 2010. doi:10.1111/j.1600-0897.2010.00845.x
33. Silvestri M, Bontempelli M, Giacomelli M, et al. High serum levels of tumour necrosis factor-α and interleukin-8 in severe asthma: markers of systemic inflammation? Clin Exp Allergy. 2006;36(11):1373–1381. doi:10.1111/j.1365-2222.2006.02502.x
34. Zenclussen AC, Fest S, Busse P, Joachim R, Klapp BF, Arck PC. Questioning the Th1/Th2 paradigm in reproduction: peripheral levels of IL-12 are down-regulated in miscarriage patients. Am J Reprod Immunol. 2002;48(4):245–251. doi:10.1034/j.1600-0897.2002.01136.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.