")
Back to Journals » International Journal of Women's Health » Volume 14
Fertility Improvement of Hysteroscopy with Chromopertubation in the Management of Infertile Women with Hysterosalpingography Evidence of Abnormal Tubal Patency: A Prospective Comparative Study
Authors Shen H, Lu Y, Su R, Wang K , Wang W, An J
Received 18 August 2022
Accepted for publication 4 November 2022
Published 15 November 2022 Volume 2022:14 Pages 1613—1619
DOI https://doi.org/10.2147/IJWH.S386746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Hailan Shen,1,* Ye Lu,2,* Ruide Su,1 Kai Wang,1 Wenrong Wang,1 Jian An2
1Department of Family Planning, Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 2Department of Gynecology, Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenrong Wang, Department of Family Planning, Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, 361000, People’s Republic of China, Email [email protected] Jian An, Department of Gynecology, Women and Children’s Hospital, School of Medicine, Xiamen University, Xiamen, 361000, People’s Republic of China, Email [email protected]
Purpose: To investigate the clinical value of hysteroscopy with chromopertubation (HSC) in infertile patients with hysterosalpingography (HSG) evidence of abnormal tubal patency.
Methods: The study consisted of 296 patients. HSG was performed as a preliminary test for the evaluation of fallopian tube status. Patients who desired to conceive naturally were treated with HSC in the next month or followed-up without additional treatment. The primary outcome was natural clinical pregnancy within 12 months after the procedure.
Results: In total, the number of clinical pregnancies was estimated to be 70 of 143 (48.95%) clinical pregnancies with management by HSC and 65 of 153 (42.48%) pregnancies with management comprising follow-up without additional treatment, and this was not significantly different (Log rank test, P = 0.516). Subgroup analysis showed that among women with bilateral abnormalities by HSG, patients receiving management with HSC tended to have a higher probability of pregnancy throughout the follow-up period than women without HSG (Log rank test, P = 0.005). No corresponding significant difference was found for women with a unilateral abnormality (P = 0.674).
Conclusion: HSC shows potential fertility improvement value for infertile patients with tubal factors. HSC may be complementary to HSG and could be incorporated as a modality of the fertility work-up.
Keywords: hysteroscopy, chromopertubation, hysterosalpingography, pregnancy, tubal patency
Introduction
Approximately 25% of couples actively attempting to become pregnant suffer from infertility in China.1 Given that tubal pathology is one of the main causes of female infertility, with a prevalence of up to 30%,2–4 evaluation of the fallopian tubes is a standard part of the fertility work-up. Currently, hysterosalpingography (HSG) is considered the first-choice tubal patency test in the work-up of infertile couples.5,6 Afterwards, diagnostic laparoscopy with chromopertubation may be the next step based on the HSG result.7–9 This procedure can achieve direct visualization of the fallopian tubes, and it not only is considered the gold standard for assessing tubal patency but also may have a treatment effect on future fertility improvement due to the tubal flushing step regardless of the hysteroscopy itself.10,11 However, the disadvantage of laparoscopy is that it is invasive and expensive.
Notably, in recent years, several studies have demonstrated that hysteroscopic procedures with either laparoscopy or pertubation could also play a possible role in the tubal patency assessment,12–14 with less invasion, lower costs and a similar assessment accuracy to that of the laparoscopic method.14 In the clinic, hysteroscopy with chromopertubation (HSC) could be performed as confirmation of true patency after HSG and as management of tubal obstruction by tubal cannulation under hysteroscopic guidance and subsequent injection of methylene blue into the tubal ostium.
To our knowledge, scant research has been published regarding the implementation of HSC after HSG during the fertility work-up. Therefore, we conducted a prospective comparative study to investigate the clinical value of HSC followed by HSG in the management of infertile women, with the natural pregnancy rate within one year of follow-up as the primary outcome. Given the reported discordance between HSG and hysteroscopy, the agreement rate of the above two procedures in our study population was also evaluated.
Methods
Study Population
The present study was a prospective comparative study conducted at the infertility gynaecology clinic of Women and Children’s Hospital, School of Medicine, Xiamen University. The study was carried out from November 2019 to February 2021. The medical ethics committee of Xiamen University approved the study (KY-2022-019-K01). This study was performed in compliance with the “Declaration of Helsinki”. The confidentiality and anonymity of the data and the voluntariness of participation were assured.
Women who underwent HSG in the evaluation of primary or secondary infertility were invited to participate in the study. The following patients were excluded: patients who had already undergone the surgery of one or both fallopian tubes; patients with anovulatory cycles not responding to ovulation induction or suspected diminished ovarian reserve (DOR); patients with ultrasonic evidence of uterine anomalies or lesions; patients with endometriotic cysts on ultrasonography or an obvious clinical sign suggestive of severe pelvic inflammatory disease (PID) or severe endometriosis; severe male factor infertility (total motile sperm count <106/mL); or a known iodine contrast allergy. After HSG, patients who were suspected of having uterine anomalies, intrauterine lesions, severe PID, bilateral tubal patency or severe bilateral tubal occlusion/hydrosalpinx were excluded. Patients who desired to conceive naturally were offered two strategies for subsequent treatment according to their willingness: follow-up without additional treatment or hysteroscopy with chromopertubation in the next month. Written informed consent was obtained from each patient. Data on parameters including age, body mass index, smoking status, primary or secondary infertility, HSG and hysteroscopy findings were recorded.
Procedures
HSGs were performed by gynaecologists between days 7 and 10 of the menstrual cycle. All HSG films were reviewed and interpreted by the same investigator. Five to 10 millilitres of lipid-soluble contrast medium (Ethiodized Poppyseed Oil Injection, Hengrui, Jiangsu, China) was injected into the uterine cavity with a catheter under sterile conditions. No premedication or prophylaxis was given. According to the obtained radiographs, the patency of the tube could be divided as follows: patency, defined as opacification of all fallopian tube segments, subsequently free of intraperitoneal spill; not so patent, defined as opacification of all fallopian tube segments, with delayed subsequent free intraperitoneal spill after pressurization; and occlusion, defined as opacification of a portion of the fallopian tube segments without subsequent free intraperitoneal spill (Figure 1).
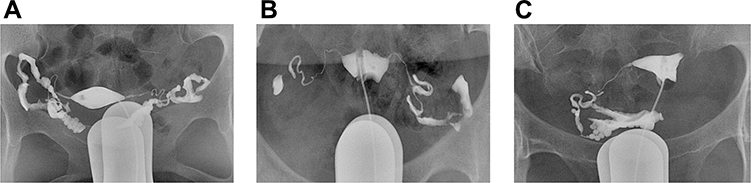 |
Figure 1 Diagnosis of fallopian tube pattern by hysterosalpingography (HSG). (A) Patency. (B) Not so patent. (C) Occlusion (unilateral). |
All hysteroscopic procedures were either performed or supervised by experts in infertility surgery experienced in hysteroscopy. Surgical procedures were conducted as outpatient surgeries under intravenous anaesthesia. The hysteroscopic procedure was performed during the early follicular phase of the menstrual cycle. All patients received antibiotics for prophylaxis to prevent secondary pelvic inflammatory disease. Hysteroscopy examination was performed using a rigid 0° optic with a 5.2-mm external sheath (Shenda, Shenyang, China). Distention was performed using normal saline solution at a pressure of 100 to 110 mmHg. A plastic catheter (KangGe, Shanghai, China) was inserted through the operating channel, and its tip was placed at the tubal ostium. Through the catheter, 2 to 20 millilitres methylene blue dye (Gentamicin Sulfate Injection 2.0 millilitres/80,000 units, Dexamethasone Sodium Phosphate Injection 0.5 millilitres/2.5 milligrams, Lidocaine Hydrochloride Injection 2.5 millilitres/0.05 grams, Methylthioninium Chloride Injection 1 millilitre/10 milligrams, and normal saline 20 millilitres) was injected slowly. According to the resistance and image during injection, the patency of the tube could be divided into patency, defined as no resistance during injection, where the catheter became blue because of the methylene blue dye flowing inside of it and normal colour of the endometrium; not so patent, defined as injection with resistance but with the catheter becoming blue because of the methylene blue dye flowing inside of it and the normal colour of the endometrium; and occlusion, defined as injection not possible because the uterine cavity became blue and because of backflow of methylene blue dye (Figure 2). The entire procedure was repeated on the other side. Surgical treatment was also performed if intrauterine pathology was detected incidentally.
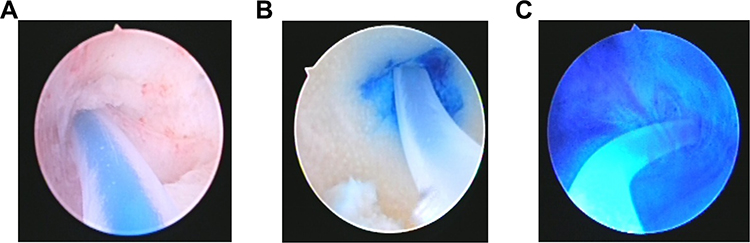 |
Figure 2 Diagnosis of fallopian tube patency by hysteroscopy with chromopertubation (HSC). (A) Patency. (B) Not so patent. (C) Occlusion. |
Outcomes
The primary outcome for the comparison of the two strategies was natural clinical pregnancy (defined as an intrauterine gestational sac detected on ultrasonography) within 12 months after the procedure. Censoring events were as follows: inability to conceive spontaneously at the last date of follow-up, referral to assisted reproductive technology during follow-up, or loss to follow-up. The secondary outcomes were concordance in the evaluation of tubal patency between HSG and hysteroscopy. Women with polycystic ovary syndrome continued with ovulation induction. Data were collected monthly until 12 months after the procedure.
Statistical Analysis
We used IBM SPSS Statistics for Windows, version 24.0 (Armonk, NY: IBM Corp) to conduct the statistical analysis. The chi-square test or Fisher’s exact probability method was used to compare differences between groups. Cohen’s kappa coefficient analysis was used to evaluate the consistency of the research methodology. A Kaplan‒Meier survival curve was constructed to determine the time-based rate of natural pregnancy. The curves of the two groups were tested by using the Log rank test. P < 0.05 was considered statistically significant.
Results
The General Characteristics of Patients
A total of 296 women and with a history of infertility who underwent HSG were included in this study (Figure 3). The age of the participants ranged from 18 to 45 years. Among them, 143 women received hysteroscopy with chromopertubation (HSC) in the next month following HSG and were assigned to the study group (Group: HSG+HSC). Additionally, there were 153 women in the control group (Group: HSG alone). Table 1 presents the baseline characteristics of the two groups.
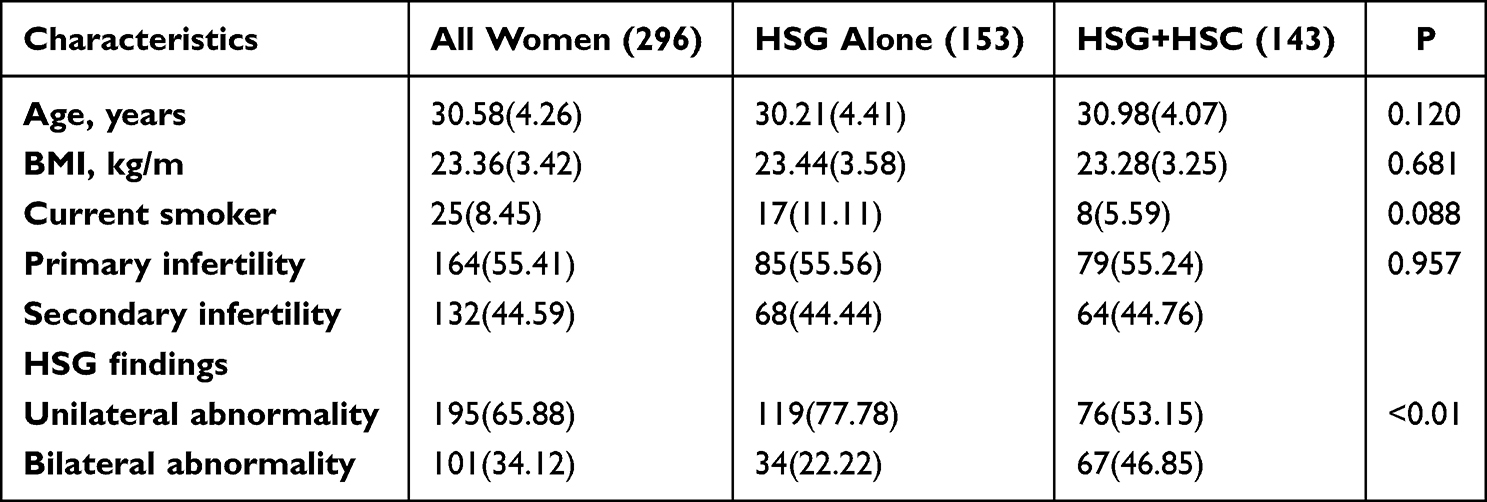 |
Table 1 Baseline Characteristics |
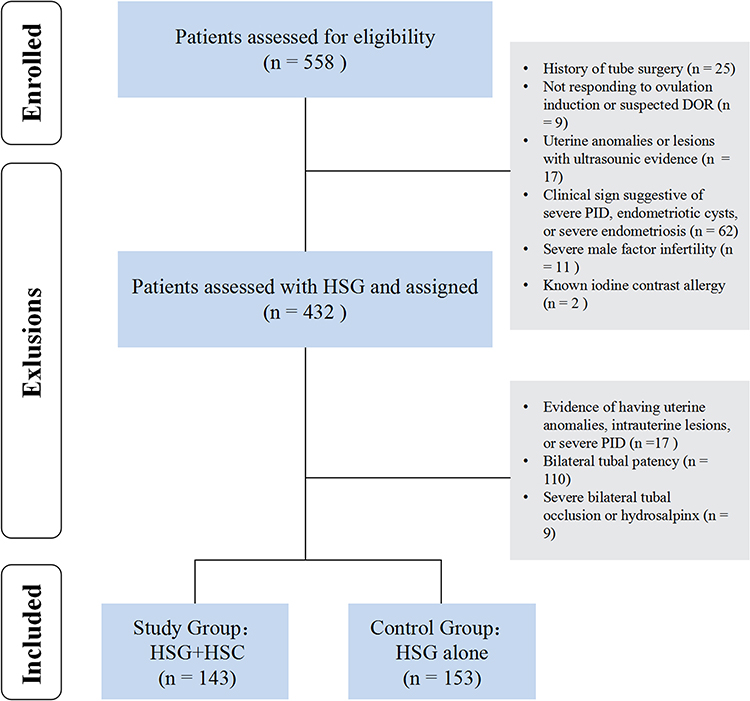 |
Figure 3 Study flow chart. |
Comparison of HSG and HSC in the Evaluation of Fallopian Tube Patency
The comparison of the HSG and HSC evaluation results of tubal patency is shown in Table 2. The agreement of tubal evaluation between HSG and HSC was 42.66%. There was no statistically significant (P value <0.001) agreement between HSG and hysteroscopy (k value = 0.128). The patency of the tube that could be evaluated by hysteroscopy seemed higher than that with HSG (68.18%, 195 out of 286 vs 26.57%, 76 out of 286). Additionally, four cases with endometrial polyps, 2 cases with uterine septum/subsetum, and 5 cases with intrauterine adhesion were detected incidentally and treated during hysteroscopy, even though the HSG showed normal uterine contour.
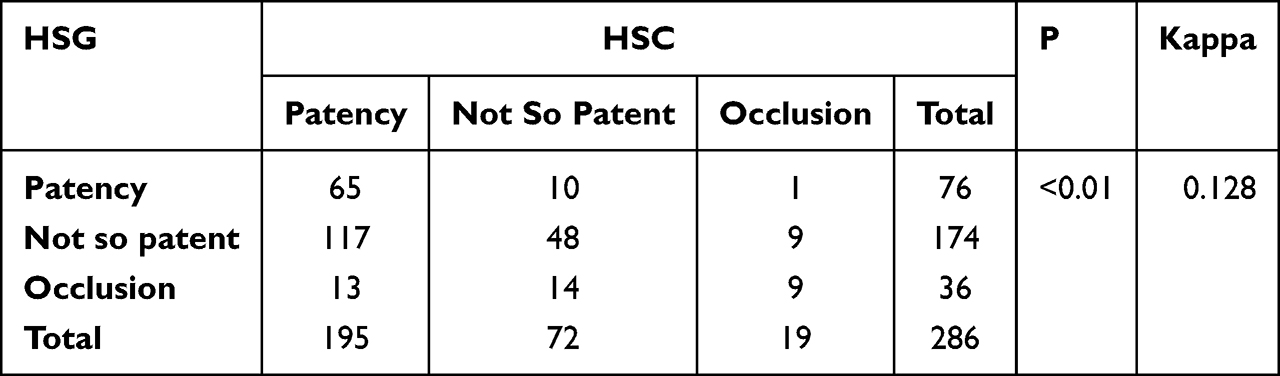 |
Table 2 Comparison Between the Evaluation of the Tube by Hysterosalpingography (HSG) and Hysteroscopy with Chromopertubation (HSC) |
Pregnancy Outcomes
In total, clinical management of HSG alone was estimated to lead to a clinical pregnancy in 65 of the 153 women (42.48%) and management by HSG+HSC did so in 70 of the 143 women (48.95%). There was no significant difference in the cumulative clinical pregnancy rates of the two groups (P = 0.516). Among all women, there were 2 cases of ectopic pregnancies, 5 cases of biochemical pregnancies and 3 cases of stillbirths. In addition, 32 cases were referred to ART, and 17 cases were lost to follow-up (Table 3).
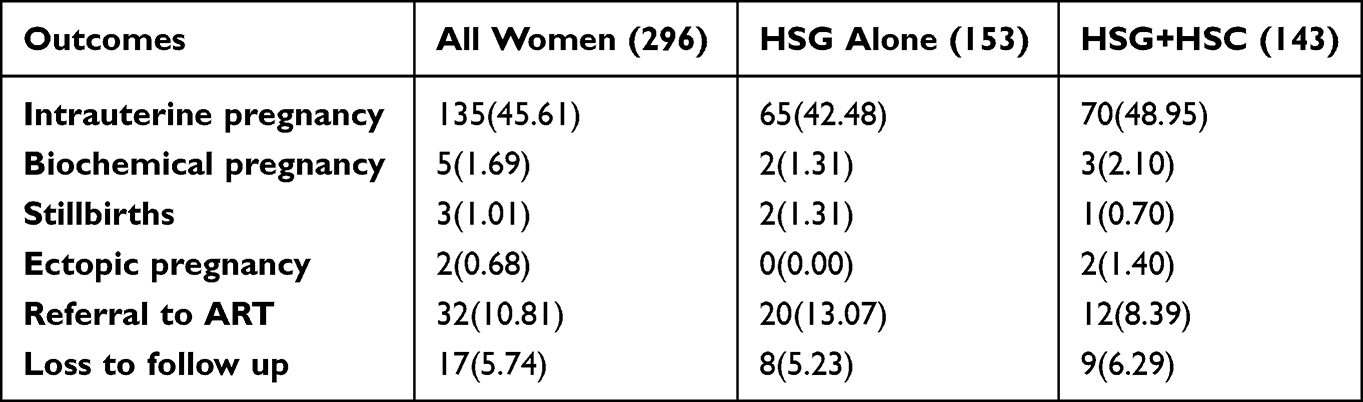 |
Table 3 Outcome During Follow-Up |
The cumulative clinical pregnancy rates for the women with different management strategies were compared, and no statistically significant differences were found (Figure 4A). Subgroup analysis based on HSG findings regarding unilateral or bilateral abnormalities was also performed. Unilateral abnormality was defined as one tube with patency and the other tube being not so patent or occluded, while bilateral abnormality was defined as both tubes being not so patent or occluded. Among the 101 patients with bilateral abnormalities by HSG, women being managed by HSG+HSC tended to have a higher probability of pregnancy throughout the follow-up period than women being managed by HSG alone (Log rank test, P = 0.005)(Figure 4B). There was no corresponding significant difference between the two groups among the 195 patients with unilateral abnormality (P = 0.674) (Figure 4C).
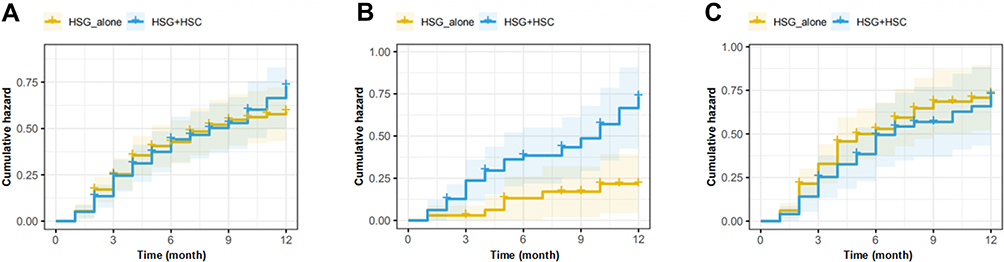 |
Figure 4 Time to clinical pregnancy for the management of hysterosalpingography (HSG) and hysteroscopy with chromopertubation (HSC) compared to HSG+follow-up. (A) Among all women (N=296). (B) Among women with bilateral abnormalities by HSG (N=101). (C) Among women with unilateral abnormalities by HSG (N=195). |
Discussion
HSG with oil contrast might enhance fertility given the underlying mechanism that oily medium will flush debris and dislodge mucus plugs from undamaged tubes.15 However, the subsequent fertility outcome still remains fair, with a reported ongoing pregnancy rate of 39.7% after hysterosalpingography with oil contrast.16 Given the potential positive effect of hysteroscopy on the chances of achieving a pregnancy,17 treatment with hysteroscopy with chromopertubation in the next month was offered and performed according to patients’ willingness in our clinic.
The findings of our study demonstrate that hysteroscopy with chromopertubation after HSG may serve as an effective management strategy in the work-up of infertile women, enabling a higher clinical pregnancy rate within one year of follow-up than HSG alone, especially in patients with suspected bilateral HSG abnormalities. To our knowledge, no study has addressed the issue of hysteroscopy with chromopertubation in terms of improving the pregnancy outcomes of infertile women who undergo HSG. Carta17 et al reported that the pregnancy rate within six months after hysteroscopy with chromopertubation in infertile women was 27%. Even though the included patients did not undergo HSG prior to hysteroscopy, they also demonstrated an improvement in fertility outcome after hysteroscopy with chromopertubation, which is in concordance with our results to some extent. The fertility-enhancing effect may be explained by the following presumed mechanisms: hysteroscopy chromopertubation could be considered as another tubal flushing following oil-based HSG and may function to enhance cilia movement, easing the transition of gametes through the fallopian tube.18 In addition, hysteroscopy examination could detect and manage a number of incidental findings of uterine pathology,19 which may affect fertility missed by HSG.
Additionally, our findings suggested that the agreement between HSG and hysteroscopy for the assessment of tubal patency was poor. A previous study demonstrated that selective pertubation with office hysteroscopy is a useful method for the assessment of tubal patency, with 82.9% accuracy and a positive predictive value of 87.5% compared with the laparoscopic method taken as the reference.14 On the other hand, Tan et al20 concluded that the positive predictive value of HSG for detecting patency or occlusion for both tubes was 87.2% and the kappa value was 0.898 [95% CI (0.838, 0.937), p < 0.001] compared to laparoscopy as the gold standard. The aforementioned two studies both indicate that the diagnostic accuracy of HSG and hysteroscopy for tube patency was clear. However, no researchers have compared the agreement of HSG and hysteroscopy alone or with laparoscopy taken as the gold standard reference. Our results that hysteroscopy seems to evaluate a more patent tube than HSG may be explained by tubal flushing with oil-based contrast prior to hysteroscopy15,21 and direct visualization and catheterization through the ostia under the guidance of hysteroscopy, potentially reducing cornual spasm with general anaesthesia.22
Our study also has some limitations. The modest sample size from a single hospital potentially limits the generalizability of the results, preventing us from conducting further investigation. In addition, some women in our study were referred to assisted reproductive technology (ART) during follow-up, which is uncontrollable and may also affect our results since we evaluated only the natural clinical pregnancy rate.
In summary, this study showed that hysteroscopy with chromopertubation made a positive contribution to the improvement of female infertility and may increase the chances of achieving a natural pregnancy. Hysteroscopy with chromopertubation could be recommended for infertile patients with abnormal tubal patency in clinical practice.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Zhou Z, Zheng D, Wu H, et al. Epidemiology of infertility in China: a population-based study. BJOG. 2018;125(4):432–441. doi:10.1111/1471-0528.14966
2. Lindsay TJ, Vitrikas KR. Evaluation and treatment of infertility. Am Fam Physician. 2015;91(5):308–314.
3. Otta SP, Reddy RG, Sangvikar S, Tripathy R. Ayurvedic management of female infertility due to tubal blockage. J Complement Integr Med. 2021;19(1):155–160. doi:10.1515/jcim-2020-0297
4. Facrquhar CM, Bhattacharya S, Repping S, et al. Female subfertility. Nat Rev Dis Primers. 2019;5(1):7. doi:10.1038/s41572-018-0058-8
5. O’Flynn N. Assessment and treatment for people with fertility problems: NICE guideline. Br J Gen Pract. 2014;64(618):50–51. doi:10.3399/bjgp14X676609
6. Infertility ACOG. Workup for the women’s health specialist: ACOG Committee opinion, number 781. Obstet Gynecol. 2019;133(6):e377–e384.
7. Lee FK, Lee WL, Wang PH. Is hysterosalpingography a good tool to confirm the patency of tubes? J Chin Med Assoc. 2017;80(5):275–276. doi:10.1016/j.jcma.2016.10.006
8. Laguerre MD, Arkerson BJ, Robinson MA, Moawad NS. Outcomes of laparoscopic management of chronic pelvic pain and endometriosis. J Obstet Gynaecol. 2022;42(1):146–152. doi:10.1080/01443615.2021.1882967
9. Lőrincz J, Jakab A, Török P. Comparison of current methods of tubal patency assessment. Orv Hetil. 2017;158(9):324–330. doi:10.1556/650.2017.30653
10. Ott J, Hager M, Nouri K, Marschalek J, Kurz C. Assessment of tubal patency: a prospective comparison of diagnostic hysteroscopy and laparoscopic chromopertubation. J Minim Invasive Gynecol. 2020;27(1):135–140. doi:10.1016/j.jmig.2019.03.006
11. Shokeir TA, Shalan HM, El-Shafei MM. Combined diagnostic approach of laparoscopy and hysteroscopy in the evaluation of female infertility: results of 612 patients. J Obstet Gynaecol Res. 2004;30(1):9–14. doi:10.1111/j.1341-8076.2004.00147.x
12. Parry JP, Riche D, Aldred J, et al. Proximal tubal patency demonstrated through air infusion during flexible office hysteroscopy is predictive of whole tubal patency. J Minim Invasive Gynecol. 2017;24(4):646–652. doi:10.1016/j.jmig.2017.02.010
13. Parry JP, Riche D, Rushing J, Linton B, Butler V, Lindheim SR. Performing the Parryscope technique gently for office tubal patency assessment. Fertil Steril. 2017;108(4):718. doi:10.1016/j.fertnstert.2017.07.1159
14. Török P, Major T. Accuracy of assessment of tubal patency with selective pertubation at office hysteroscopy compared with laparoscopy in infertile women. J Minim Invasive Gynecol. 2012;19(5):627–630. doi:10.1016/j.jmig.2012.03.016
15. Johnson NP, Farquhar CM, Hadden WE, Suckling J, Yu Y, Sadler L. The FLUSH trial--flushing with lipiodol for unexplained (and endometriosis-related) subfertility by hysterosalpingography: a randomized trial. Hum Reprod. 2004;19(9):2043–2051. doi:10.1093/humrep/deh418
16. Dreyer K, van Rijswijk J, Mijatovic V, et al. Oil-based or water-based contrast for hysterosalpingography in infertile women. N Engl J Med. 2017;376(21):2043–2052. doi:10.1056/NEJMoa1612337
17. Carta G, Palermo P, Pasquale C, et al. Office hysteroscopic-guided selective tubal chromopertubation: acceptability, feasibility and diagnostic accuracy of this new diagnostic non-invasive technique in infertile women. Hum Fertil. 2018;21(2):106–111. doi:10.1080/14647273.2017.1384856
18. Roest I, Hajiyavand AM, Bongers MY, et al. What is the fertility-enhancing effect of tubal flushing? A hypothesis article. J Obstet Gynaecol. 2022;1–7. doi:10.1080/01443615.2022.2054679
19. Wadhwa L, Rani P, Bhatia P. Comparative prospective study of hysterosalpingography and hysteroscopy in infertile women. J Hum Reprod Sci. 2017;10(2):73–78. doi:10.4103/jhrs.JHRS_123_16
20. Tan J, Deng M, Xia M, Lai M, Pan W, Li Y. Comparison of hysterosalpingography with laparoscopy in the diagnosis of tubal factor of female infertility. Front Med. 2021;8:720401. doi:10.3389/fmed.2021.720401
21. Wang R, Watson A, Johnson N, et al. Tubal flushing for subfertility. Cochrane Database Syst Rev. 2020;10:CD003718. doi:10.1002/14651858.CD003718.pub5
22. Gutmann JN. Imaging in the evaluation of female infertility. J Reprod Med. 1992;37(1):54–61.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.