")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Fertility Desire and Its Determinants Among People Living with HIV in Antiretroviral Therapy Clinic of Teku Hospital, Nepal
Authors Shrestha N , Pokharel R, Poudyal A , Subedi R , Mahato NK, Gautam N, KC D , Dhungana GP
Received 21 October 2019
Accepted for publication 20 December 2019
Published 15 January 2020 Volume 2020:12 Pages 41—46
DOI https://doi.org/10.2147/HIV.S235502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Namuna Shrestha, 1 Rajani Pokharel, 2 Anil Poudyal, 3 Ranjeeta Subedi, 3 Namra Kumar Mahato, 3 Nitisha Gautam, 3 Dirghayu KC, 3 Govinda Prasad Dhungana 4
1Chitwan Medical College, Chitwan, Nepal; 2Maharajgunj Medical Campus, Maharajgunj, Kathmandu, Nepal; 3Nepal Health Research Council, Kathmandu, Nepal; 4Department of Community Medicine and Public Health, Chitwan Medical College, Chitwan, Nepal
Correspondence: Namuna Shrestha
Tel +977 9841611718
Email [email protected]
Background: Pregnancy in people Living with HIV/AIDS (PLHIV) involves significant public health risks, including the risk of HIV transmission to uninfected partners and the fetus. Despite the growing importance of fertility issues for HIV-infected people, little is known about their fertility desires in Nepal. This study, therefore, aimed to determine the magnitude of and factors associated with the fertility desire of PLHIV.
Patients and Methods: A cross-sectional study was conducted among 280 PLHIV attending the antiretroviral therapy (ART) clinic in Teku Hospital, Nepal. A standard semi-structured questionnaire was administered to participants using systematic random sampling. Data were entered using Epi-data 3.1 and analyzed using SPSS software version 20.
Results: Out of the total participants, 12.1% desired to have a child. Among those having this desire, 44.1% had not decided when to have a child. Reasons for desiring a child were having no children (44.1%), wanting to have a child of different sex than the previous one (29.4%), followed by wanting to have another child (26.5%). Factors such as being male (COR: 3.1, 95% CI: 1.3– 7.0), being ≤ 40 years of age (COR: 3.8, 95% CI: 1.5– 9.4), higher age at marriage (COR: 7.7, 95% CI: 1.5– 39.6), middle socio-economic status (COR: 3.5, 95% CI: 1.7– 7.3), having no children (COR: 22.9, 95% CI: 8.6– 60.8) or fewer children (COR: 74.8, 95% CI: 9.7– 575.1), greater CD4 count (COR: 2.8, 95% CI: 1.3– 5.9) and having moderate knowledge of prevention of mother-to-child transmission (COR: 5.4, 95% CI: 2.3– 12.7) had higher odds of having fertility desire.
Conclusion: Around one in every ten participants had a desire for fertility despite their HIV status. This calls for special attention in promoting integrated services for HIV and reproductive health. It will be important to include counseling and other services for those with fertility desire alongside providing ART.
Keywords: ART, factors, fertility desire, Nepal, PLHIV
Introduction
In 2017, approximately 31,020 people were living with HIV and 304 pregnancies were recorded among HIV-positive women in Nepal.1 Health concerns, socio-demographic and cultural norms, fear about vertical transmission and financial issues were the factors that traditionally reduced the fertility desires of people living with HIV/AIDS (PLHIV).2,3 However, many changes have occurred in recent years.4
As a result of combination antiretroviral therapy (cART) and improvements in reproductive health services, the desire for fertility among PLHIV has increased.2 Along with these factors, PLHIV can contemplate childbearing for various socio-cultural reasons.5,6
There may be significant implications for fertility desire in PLHIV, including the risk of transmission to partners and newborns. Although prophylactic treatment minimizes the risk of vertical transmission from mother to infant, almost all new infection in children is through maternal transmission.7
Despite extensive studies elsewhere, there is a relative paucity of literature on the fertility desires of PLHIV in Nepal. This study attempts to fill that void. Studying fertility desire and intentions directly is essential to focus on the subset of HIV-infected men and women who are most likely to become pregnant by choice. This is an important subpopulation whose counseling and service needs differ substantially from others. Thus, this study aims to assess fertility desire and its determinants among PLHIV.
Methods
This cross-sectional study was conducted at the antiretroviral therapy (ART) centre operated by Sukraraj Tropical and Infectious Disease Control Hospital (Teku Hospital, the only tertiary-level Infectious & Tropical Disease Hospital in Nepal), as it was the first hospital to provide ART services and to cater to a huge number of PLHIV. Sexually active HIV-infected men and women above the age of 15 years attending the ART clinic at Teku Hospital were included in the study. Partners of the participants were not included.
The total sample size of 280 was calculated by taking a prevalence of 55% at 95% confidence interval (CI) and allowable error of 10% of prevalence, correcting for the finite population (N=1271) and adding a non-response level of 10%. A list of PLHIV (N=1271) attending the ART centre was obtained, which became the sampling frame. Estimating that data collection would take a total of 50 days and that we required 280 samples, sample collection per day was estimated as:
Sample collection per day=280/50=5.6≈6 samples/day
Assuming that 20 patients visited the ART clinic per day, the sampling interval was calculated as:
Sampling interval=20/6=3.3≈3
Taking every third respondent as the sample, the sampling unit was drawn until the required sample size was obtained.
A face-to-face interview was used as a technique for data collection. The researcher was involved in interviewing the participants. Data were collected through a semi-structured questionnaire. Pretesting was carried out in 10% of the sample among PLHIV visiting the ART clinic at Tribhuwan University Teaching Hospital (TUTH) and necessary changes were made following pretesting.
Data were entered in Epi-data 3.1 and exported to SPSS version 20.0 for analysis. Bivariate analysis was carried out to assess the association between different independent variables and fertility desire. Similarly, variables that were found to be significant in the bivariate analysis were further subjected to multiple regression analysis to identify the strong predictors of fertility desire.
The study was carried out in accordance with the principles of the Declaration of Helsinki. As the study participants included PLHIV attending the ART clinic, the ethical principles of respect, beneficence and justice were maintained throughout the data-collection process. Ethical clearance for conducting the study was obtained from Chitwan Medical College Institutional Review Committee. Consent from the respective health facility was taken prior to approaching the patients. Verbal informed consent from participants was ensured after informing the participants about the objectives of the study and their right to decline or withdraw from the study. Confidentiality and anonymity of the participants were maintained by assigning unique identification codes. In developing countries such as Nepal, social stigma and discrimination are attached to being diagnosed as HIV positive; to protect their privacy rights, we ensured that informed consent was obtained from the participants themselves for those <18 years of age. Verbal informed consent and waiver of parental consent were approved by Chitwan Medical College Institutional Review Committee.
Results
In total, 280 PLHIV above 15 years of age were interviewed. More than half (54.6%) of the participants were male. More than one-third of the participants were Janajatis, followed by 27% each of Brahmins and Chhetris. The majority (83%) of the participants were Hindus. The age of the participants ranged from 16 to 58 years, with the mean age being 38.7 years (SD±7.5). The majority of participants (97.9%) were married or in a relationship. The mean age at marriage was 21.8 years (SD±3.8).
To assess the socio-economic status, a modified version of the Kuppuswamy Socioeconomic Status Scale8 (Kuppuswamy 1976) was used. This scale takes into account defined variables such as education, occupation and income to evaluate socio-economic status. Categorization was carried out based on the obtained total score by adding up three of the above-mentioned variables. The classification was made as lower (0–10), middle (11–25) and upper (26–29). About three-quarters of the participants were in the lower socio-economic class in the Socioeconomic Status Scale of Kuppuswamy (Table 1).
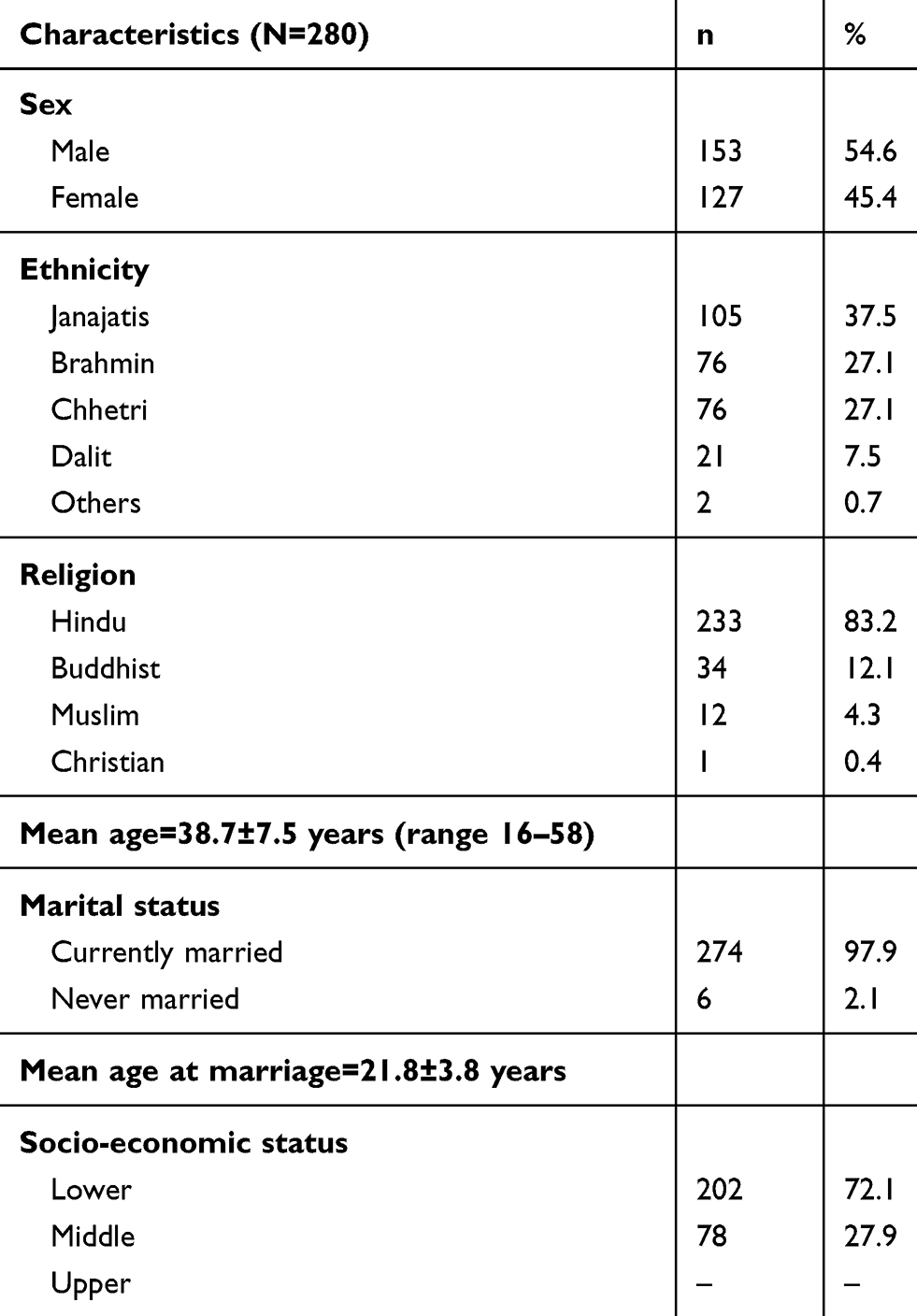 |
Table 1 Socio-Demographic Characteristics of the Participants |
Most participants (86.8%) were sexually active in the 6 months prior to the study. Most of the participants (93.8%) had disclosed their HIV status to their partner. About 93% of the participants' partners had been tested, of whom 200 (73%) were positive. The majority (90.1%) of the participants or their partner had used condoms consistently during their sexual activity in the past 6 months. Furthermore, 93.8% of the respondents or their partners were using at least one modern contraceptive method, of which all of the respondents or their partner were using a condom (Table 2).
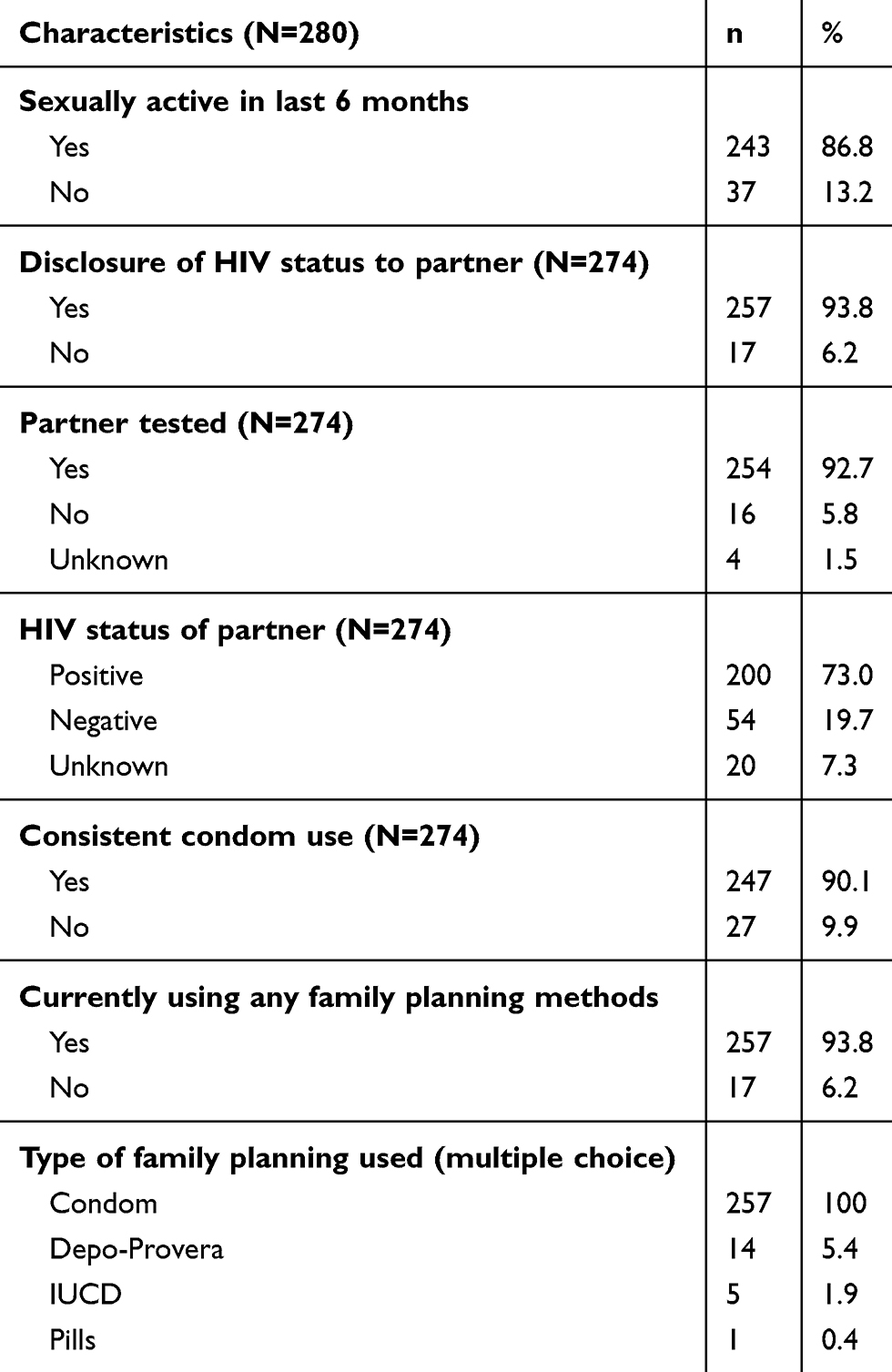 |
Table 2 Sexual and Reproductive Characteristics of the Participants |
Only about one-quarter (24.6%) of the participants had a CD4 count >500 cells/mm3. Most of the participants (91%) were on ART. About 60% of the participants had been on ART for >12 months. To assess knowledge of prevention of mother-to-child transmission (PMTCT), five questions were asked, including multiple-response questions. For a possible maximum score of 8; correct answers scored 1, while incorrect or unsure answers scored 0. Using Bloom’s criteria, a total score of ≥80% indicated good knowledge; 60–80% indicated moderate knowledge; and a score of <60% indicated poor knowledge. The results indicated that only 3.9% of the participants had a good knowledge regarding PMTCT. Most of the participants (91.6%) had previously had children, with about half already having two children (Table 3).
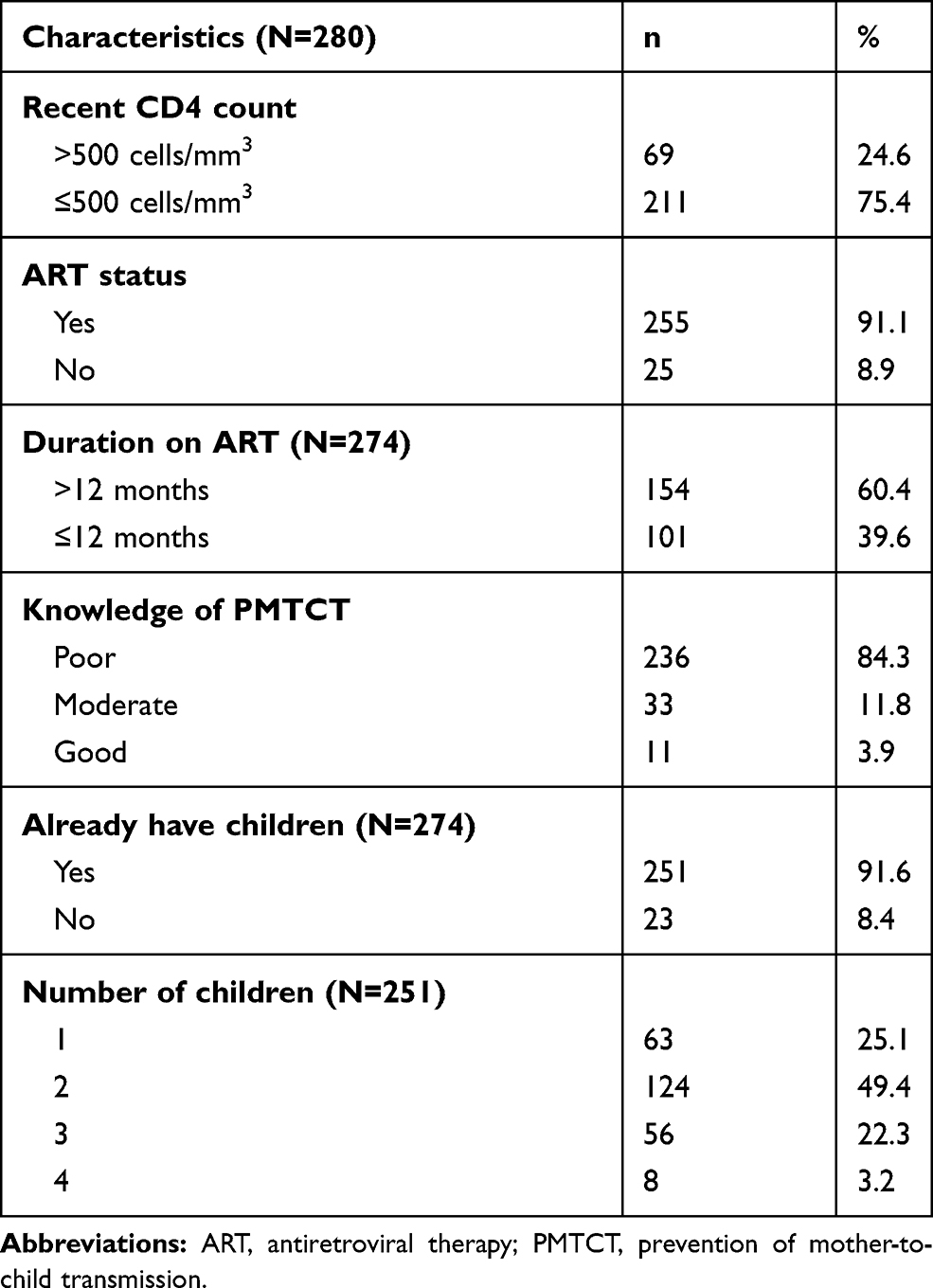 |
Table 3 Clinical Characteristics of the Participants |
Fertility desire was assessed by asking the question “Have you thought of having children since you found out that you were HIV infected?”, with a response of yes/no. Out of the total participants, 12.1% reported a desire to have a child. Among those who wanted children, more than half of the participants (55.8%) decided to have a child within or after 12 months. Regarding the reasons for desiring a child, 44.1% reported having no children, followed by 26.5% thinking it best if they had another child and 5% wanting to have a son/daughter (Table 4).
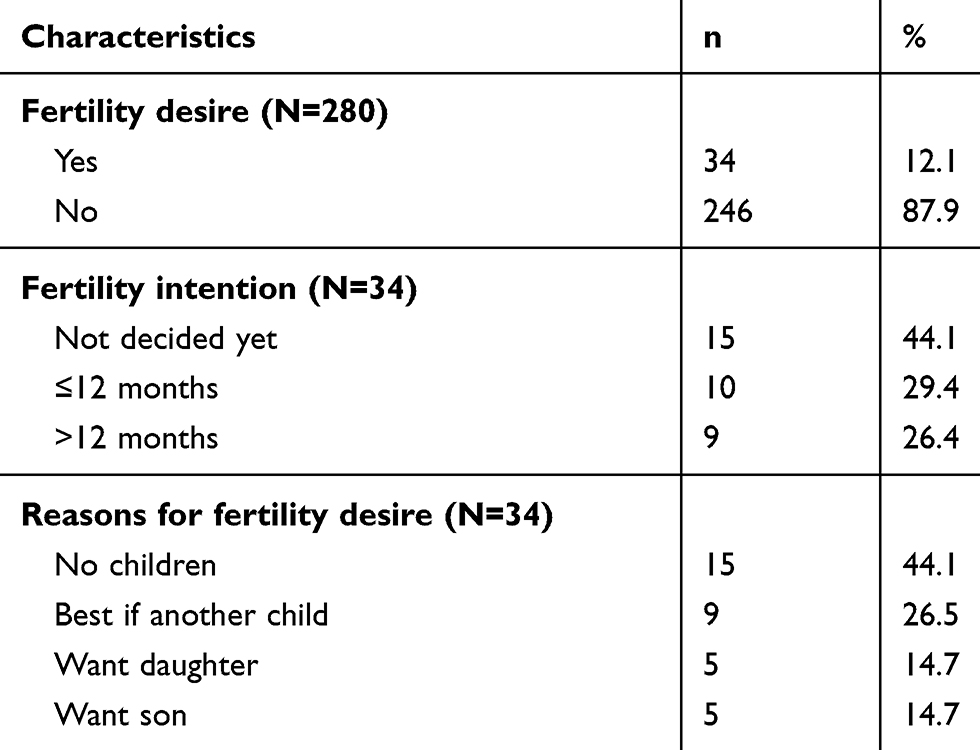 |
Table 4 Fertility Desire of the Participants |
An attempt was made to identify the factors associated with fertility desire among PLHIV. In the bivariate binary logistic regression analysis, factors found to affect fertility desire among PLHIV were being male (crude odds ratio [COR]: 3.1, 95% CI: 1.3–7.0), being aged ≤40 years (COR: 3.8, 95% CI: 1.5–9.4), higher age at marriage (>30 years) (COR: 7.7, 95% CI: 1.5–39.6), middle socio-economic status (COR: 3.5, 95% CI: 1.7–7.3), having no children (COR: 22.9, 95% CI: 8.6–60.8), having one child among those with children (COR: 74.8, 95% CI: 9.7–575.1), having a higher CD4 count (>500 cells/mm3) (COR: 2.8, 95% CI: 1.3–5.9) and having moderate knowledge of PMTCT (COR: 5.4, 95% CI: 2.3–12.7). Only one variable, number of children, was found to be statistically significant with the fertility desire in the multiple binary logistic regression analysis (Table 5).
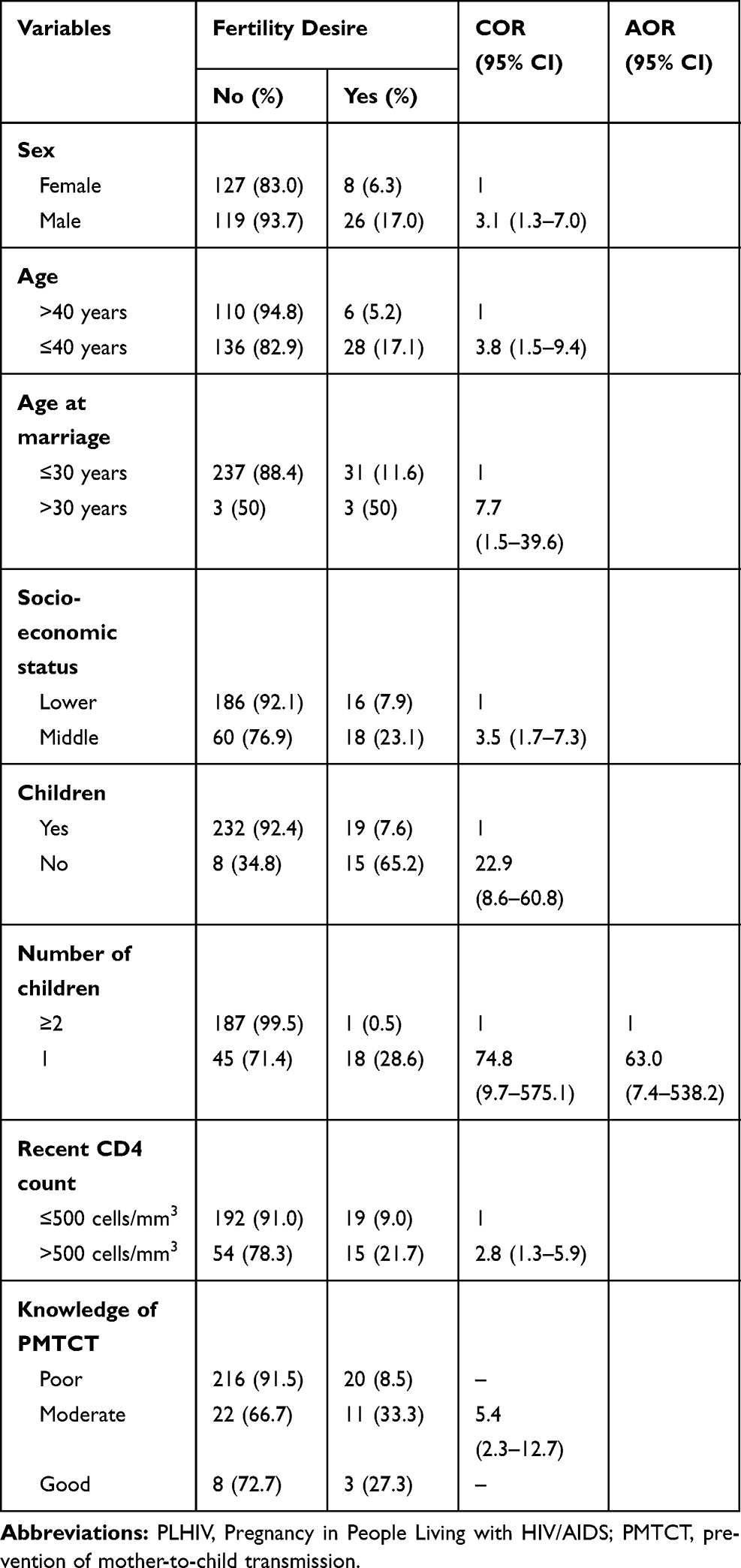 |
Table 5 Factors Associated with Fertility Desire Among PLHIV |
Discussion
In this cross-sectional study, we examined fertility desire and its determinants among 280 PLHIV aged above 15 years, with a mean age of 38.7 years. Almost all of the participants (97.9%) were married, living with their sexual partners. The study showed that 86.8% had been sexually active in the past 12 months, while 90.1% reported consistent condom use during sexual activity. Among the married participants, the majority had disclosed their status to their partner, whereas 6.2% PLHIV did not know their partner’s status. Among the participants, 12% had fertility desire, and the reasons behind this were having no children, wanting to have a second child and a preference for a child of a particular sex.
In Nepal, more than 90% of HIV-infected people are of reproductive age: 15–49 years.9 Thus, it is crucial to understand their reproductive health needs and associated factors to develop programmes and policies for safe reproduction while minimizing HIV transmission. In this study, 12% of the participants had fertility desire, which is in line with a study conducted in Uganda, which reported that 18% PLHIV desired more children.10 However, the fertility desire proportion in the present study is lower than in a cross-sectional study in rural Tanzania, in which 37.1% of participants had a desire for a child or an additional child among the PLHIV between the age of 15 and 49 years and receiving services at the local NGO.11 The lower proportion of fertility desire in ourstudy could be partly ascribed to the awareness and fear of the risk of HIV transmission to their children.
Among the participants with fertility desire, male participants were more likely than females to desire children (OR: 3.1, 95% CI: 1.3–7.0). Various studies in South Africa, Uganda and Ethiopia have shown that the men have a higher desire than women to have children.12–14 Although these studies were carried out in different settings with different sample sizes, a common finding is that men are more likely than women to want children. Men’s greater desire may be due to a wish to leave something behind – their name, lineage, etc. – while women may be more concerned about the negative effects of pregnancy on their health, the future of the children if they are orphaned and the risk of their children being infected with HIV.
Having children in Nepalese society provides a sense of security and can be a matter of social identity and status. The tendency to desire children was higher for those participants who did not have children (OR: 22.9, 95% CI: 8.6–60.8). Participants with one child were more likely to desire children compared to those with two or more children (AOR: 68.6, 95% CI: 7.6–617.8). Consistent with this study, a facility-based comparative cross-sectional study among PLHIV under highly active ART in Ethiopia showed that having no living children (AOR: 13.1, 95% CI: 5.3–32.3) or having fewer than three living children (AOR: 4.2, 95% CI: 2.2–8.0) was associated with fertility desire.14 Similarly, a study in Papua New Guinea revealed that having no children in the family (AOR: 3.6, 95% CI: 1.5–8.9) was associated with fertility desire in PLHIV.15
Having a CD4 cell count >500 cells/mm3 was associated with fertility desire in a study conducted among HIV-infected people starting ART in Uganda. This may be due to the improvement in their health status increasing the commitment of these people to achieve their reproductive desires.13 Similarly, this study found that the odds of having fertility desire among participants with a CD4 count >500 cells/mm3 was 2.8 times higher than in participants with a CD4 count ≤500 cells/mm3 (COR: 2.8, 95% CI: 1.3–5.9).
In contrast to the study carried out in Papua New Guinea,15 knowledge of PMTCT was found to be associated with fertility desire in the present study. Fertility desire was 5.4 times higher among the participants having moderate knowledge of PMTCT than in those having poor knowledge (95% CI: 2.3–12.7). Perhaps knowledge of PMTCT enables the participants to make decisions regarding their reproductive health needs and thus affects their desire to have children.
Possible limitations of this study include the cross-sectional nature of the study, which prevented us from establishing cause-and-effect relationships; the small sample size, so the results may not be generalizable; the lack of a limit on the age range, when it would have been better if only people of reproductive age had been included,; only verbal consent being taken from the participants, which may raise ethical concerns; and the failure to include questions regarding permanent methods of family planning.
Conclusions
This study demonstrated that a considerable proportion (12%) of PLHIV have a desire for fertility. Factors that influenced fertility desire among respondents were being male, aged 40 years or below, higher age at marriage, middle socio-economic status, having no children or one child, greater CD4 count and moderate knowledge of PMTCT. The desire for children by PLHIV implies the need for necessary counseling and reproductive services to support them to conceive and have children safely in the future. Those who do not want to have a child require effective contraception.
Acknowledgment
We would like to acknowledge all the participants who participated in this study, and the ART Clinic, Teku Hospital.
Disclosure
The authors report no conflicts of interest in this work. The abstract of this paper was presented as an oral presentation at the First National Population Conference (FNPC) 2014, held in Kathmandu, Nepal, from 5 to 7 June 2014. The abstract of this paper was published in the FNPC proceedings report and a link to the report is at https://nepal.unfpa.org/sites/default/files/pub-pdf/FNPCProceedingReport.pdf.
References
1. NCASC. Country progress report NEPAL: to contribute to global AIDS monitoring report 2017; 2018. Available from: https://www.unaids.org/sites/default/files/country/documents/NPL_2018_countryreport.pdf.
2. Dube AL, Baschieri A, Cleland J, et al. Fertility intentions and use of contraception among monogamous couples in northern Malawi in the context of HIV testing: a cross-sectional analysis. PLoS One. 2012;7(12):e51861. doi:10.1371/journal.pone.0051861
3. Withers M, Dworkin S, Harrington E, et al. Fertility intentions among HIV-infected, sero-concordant couples in Nyanza province, Kenya. Cult Health Sex. 2013;15(10):1175–1190. doi:10.1080/13691058.2013.811289
4. Behboodi-Moghadam Z, Nikbakht-Nasrabadi A, Ebadi A, Esmaelzadeh–Saeieh S, Mohraz M. Fertility desire in Iranian women with HIV: a qualitative study. Iran J Public Health. 2015;44(8):1126.
5. Andia I, Kaida A, Maier M, et al. Highly active antiretroviral therapy and increased use of contraceptives among HIV-positive women during expanding access to antiretroviral therapy in Mbarara, Uganda. Am J Public Health. 2009;99(2):340–347.
6. Kakaire O, Osinde MO, Kaye DK. Factors that predict fertility desires for people living with HIV infection at a support and treatment centre in Kabale, Uganda. Reprod Health. 2010;7(1):27.
7. Lindegren ML, Byers RH
8. Bairwa M, Rajput M, Sachdeva S. Modified Kuppuswamy’s socioeconomic scale: social researcher should include updated income criteria, 2012. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine. 2013;38(3):185.
9. (NCASC) NCfAaSC. Country progress report on HIV/AIDS Response. Nepal: Ministry of Health and Population, National Centre for AIDS and STD Control (NCASC); 2014. Available from: https://www.unaids.org/sites/default/files/country/documents/NPL_narrative_report_2014.pdf.
10. Nakayiwa S, Abang B, Packel L, et al. Desire for children and pregnancy risk behavior among HIV-infected men and women in Uganda. AIDS Behav. 2006;10(1):95.
11. Mmbaga EJ, Leyna GH, Ezekiel MJ, Kakoko DC. Fertility desire and intention of people living with HIV/AIDS in Tanzania: a call for restructuring care and treatment services. BMC Public Health. 2013;13(1):86.
12. Myer L, Morroni C, Rebe K. Prevalence and determinants of fertility intentions of HIV-infected women and men receiving antiretroviral therapy in South Africa. AIDS Patient Care STDS. 2007;21(4):278–285.
13. Wagner GJ, Wanyenze R. Fertility desires and intentions and the relationship to consistent condom use and provider communication regarding childbearing among HIV clients in Uganda. ISRN Infect Dis. 2012;2013:478192. doi:10.5402/2013/478192
14. Regassa T, Fantahun M. Fertility desire and reproductive health care needs of men and women living with HIV/AIDS in Nekemte, East Wollega, Ethiopia. Sci Technol Arts Res J. 2012;1(3):31–38.
15. Aska ML, Chompikul J, Keiwkarnka B. Determinants of fertility desires among HIV positive women living in the Western highlands province of Papua New Guinea. World J AIDS. 2011;1(04):198.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.