")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Fertility Desire And Associated Factors Among HIV Positive Women Attending ART Clinics In Amhara Region Referral Hospitals In Northwest Ethiopia, 2017
Authors Mekonnen B , Minyihun A
Received 4 July 2019
Accepted for publication 12 September 2019
Published 17 October 2019 Volume 2019:11 Pages 247—254
DOI https://doi.org/10.2147/HIV.S221941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Bilen Mekonnen,1 Amare Minyihun2
1Department of Clinical Midwifery, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Amare Minyihun
Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P.O. Box 196, Gondar, Ethiopia
Email [email protected]
Background: “Fertility desire” is the intention of people to have more children despite being diagnosed with HIV, whereas intentions denote a commitment to implement that desire. Despite the overwhelming effects of HIV on a fetus, there is a desire for fertility among people positive for the virus/disease worldwide. Therefore, this study aimed to assess fertility desires and factors associated with sexually active HIV positive reproductive-age women attending ART clinics at Amhara region referral hospitals, Northwest Ethiopia.
Methods: An institution-based cross-sectional study was conducted on reproductive-age women attending the clinics at the hospitals. A total of 427 eligible women were systematically included in the study. A semi-structured questionnaire was used to collect data via interviewer-administered techniques. EpiInfo7 and STATA 14 software was used for data entry and analysis, respectively. The logistic regression analysis method was used to identify factors associated with fertility desire. Factors that had p-values of ≤0.05 were considered statistically significant.
Results: The findings indicated that 40.3% (95% CI; 35.7%, 45.0%) of the participants reported they had the desire to have children in the future. Variables such as women in the age group of 25–34 years (AOR= 2.80, 95% CI; 1.68, 4.68), participating with their sexual partner (AOR=3.52, 95% CI; 1.36, 9.13) and married women (AOR=2.32, 95% CI; 1.05, 5.10) had a positive association with the outcome variable, whereas having one or more live children (AOR=0.19, 95% CI; 0.09, 0.39) and having no formal education (AOR= 0.51, 95% CI; 0.29, 0.89) had a negative association with fertility desire.
Conclusion: The proportion of sexually active HIV-positive women with desire for children was high among women visiting referral hospitals. Therefore, programmers and policymakers need to expand new PMTCT services throughout the region and consider the effects of these factors on HIV-positive women, as they develop interventions.
Keywords: fertility desire, ART clinic, women, Amhara region, Ethiopia
Background
Human Immunodeficiency Virus (HIV)/Acquired Immunodeficiency Syndrome (AIDS) has become one of the world’s most detrimental public health problems and developmental challenges.1 Globally, 150,000 children are newly diagnosed with HIV/AIDS annually; of these, over 90% acquired it through mother-to-child transmission (MTCT). About half of the infected children will die without treatment before their second birthday.2
Fertility desire is the intention of men and women to have more offsprings despite the diagnosis of HIV, whereas intentions denote the commitment to implement the desire. Therefore, intention encompasses both desire and planning aspects. The desire for children means the expression of people living with HIV (PLWHIV) to have children in the future.3 Since most PLWHIV are of reproductive age, one of the unexpected effects of anti-retroviral treatment (ART) is the possibility to increase the fertility desire of people infected and affected with the disease.4
Worldwide, the majority of new infections occur among children born to HIV-positive mothers from who they acquire the infection.5 In addition, HIV positive people may indulge in high-risk sexual behavior, such as having multiple sexual partners, unprotected sex, and non-disclosure of their HIV status to sexual partners due to the desire for fertility.6,7 Thus, the desire to have children among HIV infected people has significant implications for the transmission of HIV to sexual partners and newborns in the future.8
The high discrepancy between desired total fertility and actual total fertility is greater among HIV-positive people than in the general population.9 As a result, the desire to have children among HIV-infected people may increase because of the improved quality of life and survival rate due to ART clinics and better reproductive health services.10,11 The connection between fertility and HIV/AIDS where preventive strategies clashed with the HIV epidemic in countries like Ethiopia is multifaceted; the fertility rate is very high and PMTCT service so low.12 Although the policy of the Ethiopian Government is supportive of HIV and reproductive health service integration, the services remain mostly vertical in terms of program administration, funding and service delivery.13,14
According to the Ethiopian Demographic Health Survey (EDHS), the country is characterized by culturally valued high fertility, high HIV prevalence, low level contraceptive use and mounting intentions to have children. The current total fertility rate of the country is 4.8% (2.6% in urban and 5.5% in rural settings). It is also stated that the adult national HIV prevalence (15–49 years) estimated for 2012 was 1.5%, although women had a higher HIV prevalence (1.9%) than men (1.0%).15
These high fertility rates and intentions are not disaggregated by HIV status in Ethiopia. Yet, there is a need to address the reproductive need of people living with HIV, for there is a complex relationship between HIV and fertility. Therefore, understanding the level of fertility desire and its associated factors is expected to play a crucial role in evidence-based decision making by all concerned stakeholders in Ethiopia and other countries with similar context.
Methods
Study Setting And Design
A facility-based cross-sectional study design was employed to investigate the theme from January to June 2017. The region has five referral hospitals, namely Debrebirhan, Debremarkos, Felegehiwot, Desse, and Gondar.
In 2016, the population of the Amhara region was projected to be over 21 million, 25% of the total inhabitants of the overall country; women formed 50.2% of the Amharas. According to EDHS 2016, the average total prevalence of HIV was 1.2%, but 1.8% among females.16 Nearly 205,969 HIV infected people of whom 62.1% were female lived in the region during the study,17 and about 15,653 women were attending an ART clinic.
Population
All HIV-positive sexually-active women of reproductive age (15–49 years) attending ART clinics in the hospitals were the source population, whereas all sexually-active HIV-positive women of reproductive age attending ART clinics in the hospitals and available at the time of data collection, were the study population. Sexually active HIV-positive 18 to 49 years of age were included in the study, but women who were pregnant, infertile, or had hysterectomy were excluded.
Sampling Procedure
The sample size of the study was calculated using the single population proportion formula with the assumption Za/2 at 95% confidence level = ±1.96, margin of error (w) = 5%, and a prevalence of reproductive desire of (p)42.16%,18 N= (Za/2) 2(P)(1-P)/(w)2= (1.96)2 (0.4216) (0.5784)/(0.05)2 =375; then adding 15% non-response rate yielded 432 (total sample size).
The participants were selected using the systematic random sampling technique. The total number of reproductive age women was estimated based on their flow pattern to the ART clinics in the previous six months. At each hospital, an ART clinic sampling interval (K) was obtained by dividing the total number of women attending the clinic (n) by the sample size set for each hospital. The first participant was selected randomly, and then every Kth woman was interviewed. The next woman was taken when the selected women were not eligible.
Measures And Operational Definitions
Future fertility desire, the dependent variable of the study was assessed by “Yes” or “No” question: “Would you like to have children in the future?” Socio-demographic characteristics (age, residence, ethnicity, religion, marital status, educational status, and occupation), service and client-related variables (provider counseling service, current family planning utilization, children born earlier, number of children at the moment, previous pregnancy history and last intended pregnancy), and HIV related factors (current ART status, CD4 level, disclosure of HIV status, and partner HIV status) were included in the model as independent variables.
Data Collection And Analysis
Using a semi-structured questionnaire and chart reviews, data were collected by face to face interviews to assess CD4 levels. Based on the local situation of the study area and the purpose of the study, the questionnaire was adapted from a variety of literature. A pre-test was administered on 22 individuals (5% of the sample) before starting the actual survey. The questionnaire, prepared in English, was translated to Amharic and back to English to maintain accuracy. A day-long training was given to data collectors and the supervisor about data collection procedures.
The collected data were entered into EPI info version 7 and exported to STATA version 14 for further analysis. Descriptive and summary statistics were analyzed. The proportion was calculated to estimate the level of fertility desire. To identify factors associated with fertility desire, bivariate and multivariable logistic regression models were employed. Bivariate analysis was done to screen candidate variables with less than 0.2 P-values for the final model. Finally, the multivariable logistic regression analysis model was fitted to identify significant factors associated with fertility desire. Variables that had significant associations and identified on the adjusted odds ratio (AOR) with a 95% CI, P-Value ≤0.05, were taken as statistically significant.
Results
Socio-Demographic, HIV And Fertility Characteristics Of Participants
A total of 427 participants, 50.0% of whom were in the 25–34 years age groups and with a mean age of 32.5 (± 0.31 SD) years were involved in the study, with a response rate of 98.8%. The majority (90.4%) of the participants lived in urban areas; 99.5% were Amhara by ethnicity; 50.6% were married, 35.6% had no formal education and 42.1% were housewives (Table 1).
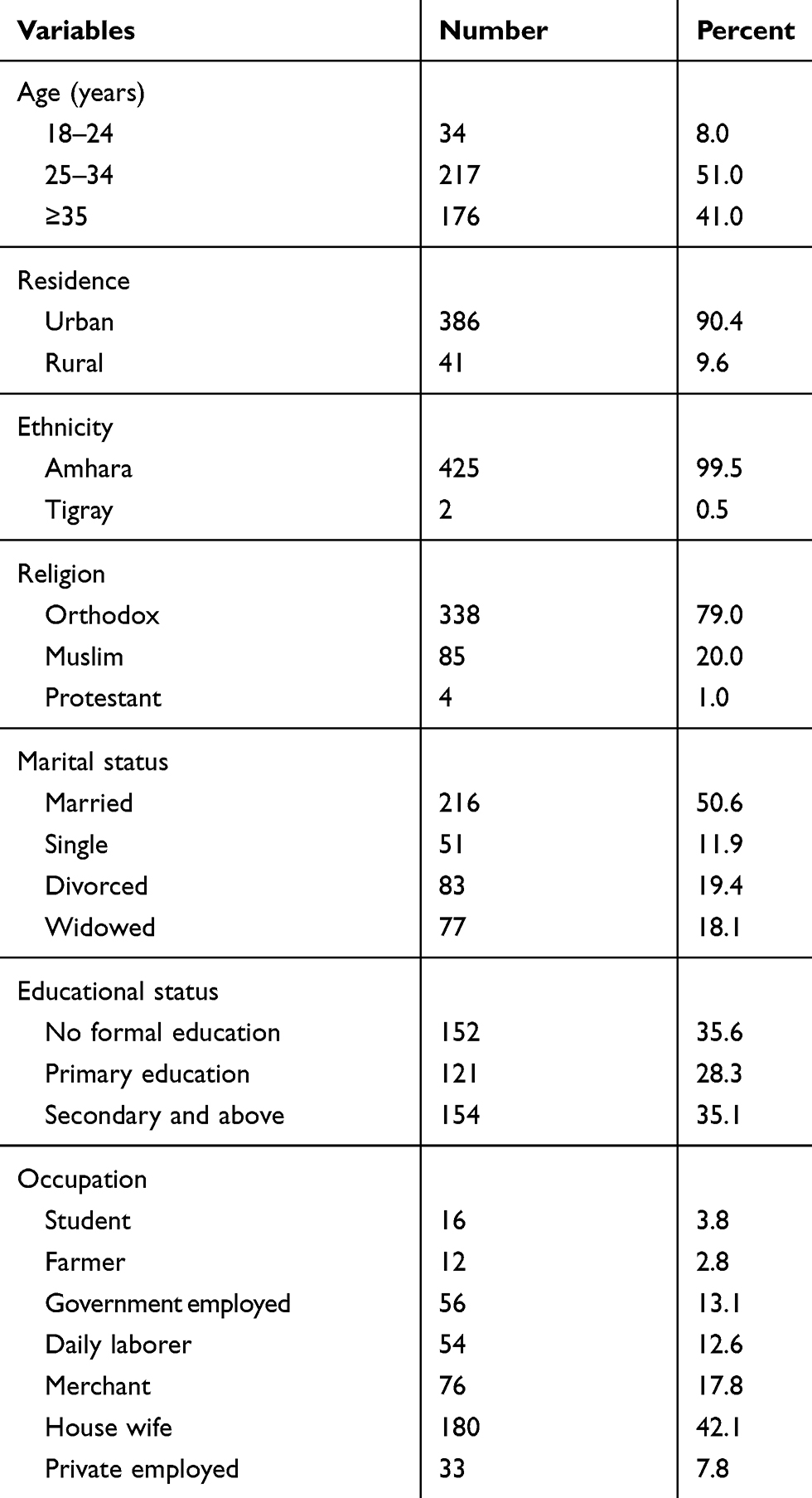 |
Table 1 Socio-Demographic Characteristics Of Sexually Active HIV Positive Reproductive Age Women Attending ART Clinics In Amhara Region Referral Hospitals, Northwest Ethiopia, 2017 (n=427) |
Of the 427 participants, more than half, 234 (55.3%), were living with HIV for more than 60 months. Almost all, 424 (99.3%), were taking ART drugs, 269 (63.0%) had regular partners, 25 (9.3%) didn’t disclose their status to their partners for fear that their spouses would leave or divorce them. Almost three-quarters, 210 (78.0%), of the participants’ partners were HIV positive. The majority of the participants, 370 (86.7%), were receiving counseling from health care providers, while only 203 (47.5%) of the participants were utilizing some form of modern family planning, (Table 2).
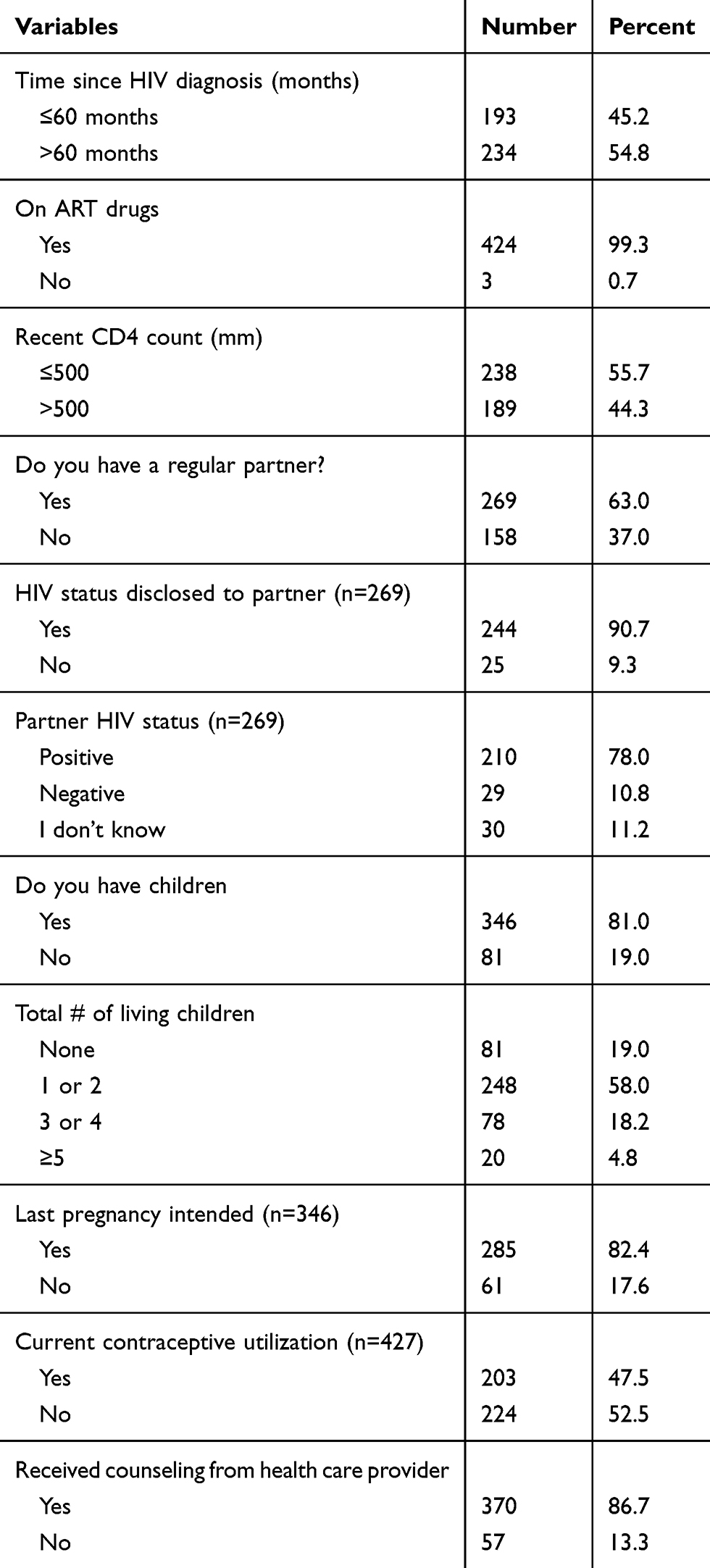 |
Table 2 HIV- And Fertility-Related Profile Of Sexually Active HIV Positive Reproductive Age Women Attending ART Clinics In Amhara Region Referral Hospitals, Northwest Ethiopia, 2017 (n=427) |
Factors Associated With Fertility Desire
Of all the variables in the bivariate logistic regression, age, marital status, educational status, regular partners and live children were found to be significantly associated with fertility desire at P-value of ≤0.05 (Table 3).
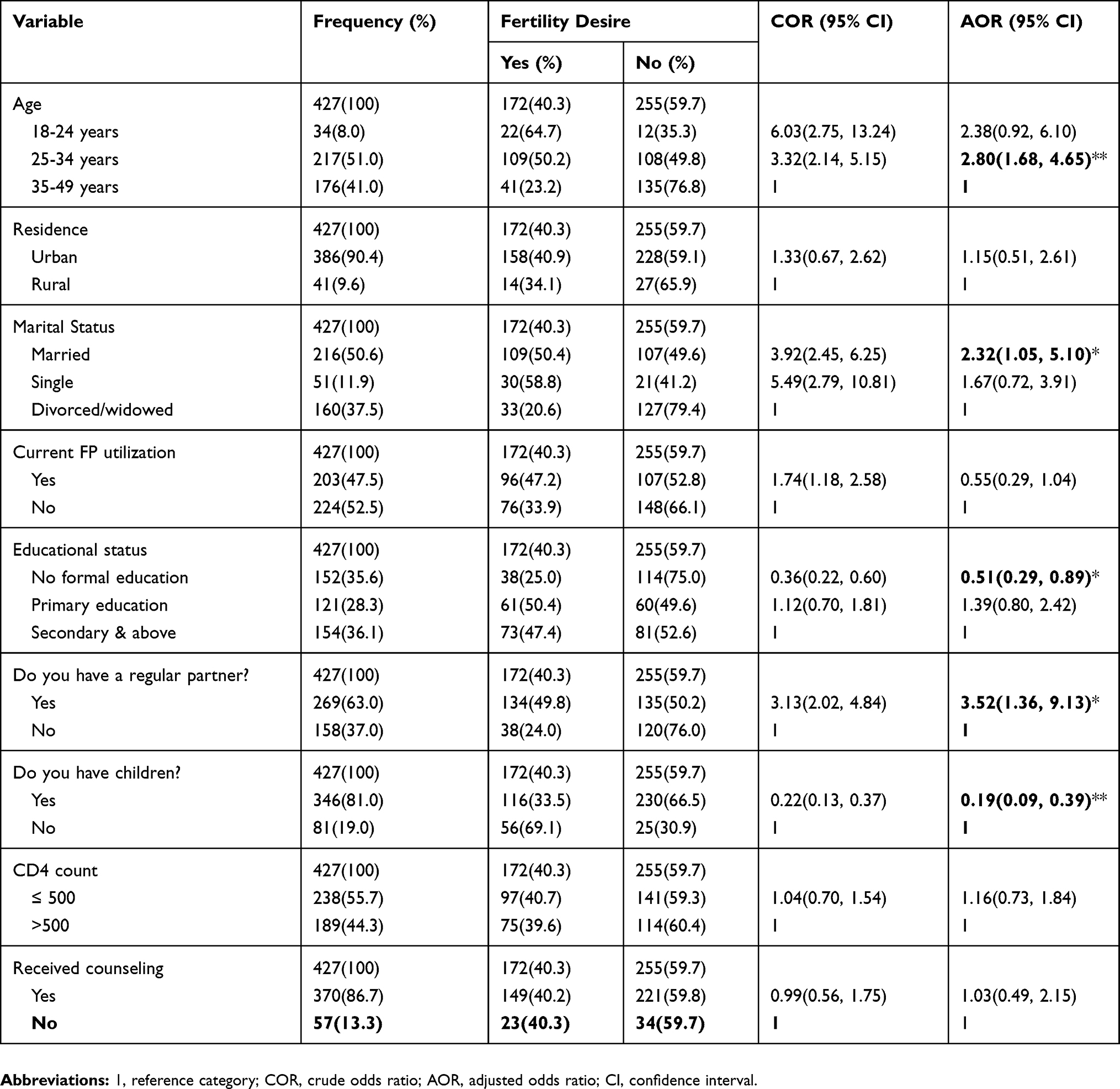 |
Table 3 Bivariate And Multivariable Analysis Of Factors Associated With Fertility Desire Among Sexually Active Reproductive Age Women Attending ART Clinic In Amhara Region Referral Hospital, Northwest Ethiopia, 2017 (n=427) |
The study showed that women aged 25–34 years were 2.8 times more likely to desire children compared to those aged 35–49 years (AOR= 2.80, 95% CI; 1.68, 4.65). Respondents who had no formal education were 49% less likely to desire children who had secondary or higher education (AOR= 0.51, 95% CI; 0.29, 0.89).
Women who had regular partners had almost four times (AOR=3.52, 95% CI; 1.36, 9.13) higher odds of fertility desire compared to their counterparts. Women who had one or more live children were 81% less likely to desire children than their counterparts (AOR=0.19, 95% CI; 0.09, 0.39). Respondents who were married at the time of the study were 2.32 times more likely to desire children compared to those who were divorced or widowed (AOR=2.32, 95% CI; 1.05, 5.10).
Discussion
This study aimed to assess fertility desire and factors associated among sexually active HIV positive reproductive age women attending the ART clinics of the Amhara region referral hospitals, Northwest Ethiopia. The prevalence of fertility desire was found to be 40.3% (95% CI; 35.72%, 45.02%). The finding is comparable with those of studies conducted in different regions of Ethiopia and reported 36.4 to 44.6%.19–22 It also is in line with the results studies in Tanzania (39.7%) and Uganda (35%).23,24 The similarity of the populations and study designs might have created the correspondence in results. Nonetheless, fertility desire among HIV-positive women reported in different parts of the country and in Africa, for example, Addis Ababa (54.6%), Harari (52.9%), Tigray (45.5%), Oromia (47.5%), and South Africa (80%), was higher than our finding.25–29 This might be due to the following circumstances: the study in Addis Ababa included both male and female HIV positive clients, the literature indicated that fertility desire among men was higher than among women and that might have increased the prevalence of the desire in the study. The other studies used different designs and included pregnant women which might have increased the proportion of fertility desire. A study in Nigeria reported a higher fertility desire (75.8%) than ours. In the same study, religion also played a role in determining fertility desire.30 However, it was not found to be a significant factor in our study. This might be because the majority of the participants were Muslims who practice polygamy; the wives also believe that having many children would attract husbands. Other studies in some parts of Ethiopia, like Mekelle, Finoteselam, and Nekemte reported results lower than ours, 24.4, 28.8%, and 30.7%, respectively. In the studies done in Mekelle and Nekemte, source populations and data collectors were health care providers working in the ART clinics. This might have created social desirability bias in that the client provided “No” answers to fertility desire questions. In the study in Finoteselam, the majority of the participants were pregnant women who said that their “current pregnancy” was unwanted. This might have decreased their future fertility desire.31–33 Another study done in Brazil had a lower finding (25.9%) compared to ours. The study used a convenient sampling method that had a probability of enrolling participants in the same status, for instance, people aged over 40 years had children which might have affected their fertility desire.34
The study showed that women who were 25–34 years of age were 2.8 times more likely to have future fertility desires compared to older women. This finding was in line with those of studies in Brazil, some parts of Ethiopia20,22,26,27,35 and a meta-analysis.36 Other studies showed that women’s ability to conceive decreased through time and their awareness of that decreased their fertility desire. Married couples were 2.32 times more likely to have a desire for future fertility compared to divorced or separated men and women. This finding was similar to studies done in Woreilu and Oromia, Ethiopia.21,28 Being married created a sense of security and reliable support to raise children. As opposed to the studies in Mekelle and Wolaita, Ethiopia showed that married women had low fertility desire. Explanations for these differences are not clear, but they are likely to be the result of using different source populations.22,37
Women who had no formal education were 49% less likely to desire future fertility compared to women in the secondary or above educational level. This result is comparable with that of a study done in the Oromia region. This establishes that these women may not have a sustainable or sufficient income to raise children.28
Women who had children were 81% less likely to have future fertility desires. This outcome is supported by other studies done in some areas in Ethiopia, African countries, Brazil and a Meta-analysis on fertility desire. This might be because participants who had regardless of the number might have attained the desired family sizes, and did not have future fertility desire.20,21,23,24,26,27,29,32,35,36,38 Women with regular partners had 3.52 times higher odds of future fertility desires. Having a partner would generate a steady and encouraging environment for a person’s life, and that in turn may influence women to have children and increase their family sizes.
Limitations
There is a risk of social desirability bias, whereby HIV-positive women may under-report their fertility desire because of pressure from health workers who encourage protected sex and contraceptive utilization. In addition, the study has not included men, who are a major stakeholder of fertility desire.
Conclusion
The study showed that almost two-fifths of women living with HIV/AIDS had a desire for children, and the proportion of such women was greater than those of other studies in Ethiopia. Aged 25–34 years, one or more live children, sexual partners, lack of formal education and marriage were notably associated with fertility desire. Therefore, programme designers and policymakers need to expand PMTCT services and consider the impact of the preceding factors on HIV-positive women when they plan interventions.
Ethics Approval And Consent To Participate
Ethical clearance was obtained from the Institutional Review Board of the University of Gondar. The study commenced after the permission letter was obtained from the five referral hospitals. Informed verbal consent was secured from study participants, which was approved and accepted by the ethics committee. Each respondent was informed about the objective of the study and assurance of confidentiality was given as the information they gave was not shared with other people or institutions. We informed participants who were unwilling to participate in the study and those who wished to halt their participation at any stage to do so without any restriction.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ART, Anti-Retroviral Therapy; CD4, Cluster Differentiation; FP, Family Planning; HIV, Human Immunodeficiency Virus; IUCD, Intra-Uterine Contraceptive Device; HAART, Highly Active Anti-Retroviral Therapy; MTCT, Mother to Child Transmission; PLWHIV, People Living With HIV; PMTCT, Preventing Mother to Child Transmission.
Availability Of Data And Materials
The datasets generated and analyzed during the current study are not publicly available due to the sensitive nature of the data but are available from the corresponding author upon reasonable request.
Acknowledgments
We express our deep gratitude to the University of Gondar for financial support, without which this project would not have been possible. Our special thanks and sincere appreciation also goes to the Amhara Regional Health Bureau, staff working in the five referral hospitals, study participants, data collectors, and other individuals or organizations that participated directly or indirectly in the study.
Author Contributions
Both authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS. UNAIDS 2016–2021 Strategy–On the Fast‐track to End AIDS. Geneva, Switzerland: UNAIDS; 2015.
2. UNAIDS. Global HIV Statistics FactSheet, Ending the AIDS Epidemic. November 2016.
3. Kodzi IA, Johnson DR, Casterline JBJDR. Examining the predictive value of fertility preferences among Ghanaian women. Demogr Res. 2010;22:965. doi:10.4054/DemRes.2010.22.30
4. UNAIDS JJGU. Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. 2010.
5. Newell ML. Vertical transmission of HIV-1 infection. Trans R Soc Trop Med Hyg. 2000;94(1):1–2. doi:10.1016/s0035-9203(00)90413-9
6. Kline A, Strickler J, Kempf J. Factors associated with pregnancy and pregnancy resolution in HIV seropositive women. Soc Sci Med. 1995;40(11):1539–1547. doi:10.1016/0277-9536(94)00280-7
7. Nakiganda LJ, Nakigozi G, Kagaayi J, et al. Cross-sectional comparative study of risky sexual behaviours among HIV-infected persons initiated and waiting to start antiretroviral therapy in rural Rakai, Uganda. BMJ Open. 2017;7(9):e016954. doi:10.1136/bmjopen-2017-016954
8. Chen JL, Phillips KA, Kanouse DE, et al. Fertility Desires and Intentions of HIV-Positive Men and Women. Fam Plann Perspect. 2001:144–165.
9. Haile F, Isahak N, Dessie AJHRS. Fertility desire and associated factors among people living with HIV on ART Eastern Ethiopia. J Trop Dis. 2014;2(137):2.
10. Harries J, Cooper D, Myer L, et al. Policy maker and health care provider perspectives on reproductive decision-making amongst HIV-infected individuals in South Africa. BMC Public Health. 2007;7(1):282.
11. Bankole A, Biddlecom AE, Dzekedzeke K. Women’s and men’s fertility preferences and contraceptive behaviors by HIV status in 10 sub-Saharan African countries. AIDS Educ Prev. 2011;23(4):313–328. doi:10.1521/aeap.2011.23.4.313
12. Hosegood VJAC. The demographic impact of HIV and AIDS across the family and household life-cycle: implications for efforts to strengthen families in sub-Saharan Africa. AIDS Care. 2009;21(sup1):13–21. doi:10.1080/09540120902923063
13. Balcha TT, Lecerof SS, Jeppsson AR. Strategic challenges of PMTCT program implementation in Ethiopia. J Int Assoc Physicians AIDS Care (Chic). 2011;10(3):187–192. doi:10.1177/1545109710369935
14. Assefa Y, Alebachew A, Lera M, et al. Scaling up antiretroviral treatment and improving patient retention in care: lessons from Ethiopia, 2005-2013. Globalization health. 2014;10(1):43.
15. CSA. Ethiopian Demographic and Health Survey; Key Indicators Report. Addis Ababa, Ethiopia; 2016.
16. ICF., C.C.E.a. Ethiopia Demographic and Health Survey 2016. E. Addis Ababa, and Rockville, Maryland, USA: CSA and ICF; 2016.
17. EPHI. HIV Related Estimates and Projections for Ethiopia–2017. Addis Ababa; 2017.
18. Tesfaye L, Admassu M, Getachew A, et al. Fertility desires and family planning demand among HIV-positive clients in follow-up care at antiretroviral treatment unit in Gondar university hospital, Ethiopia. Vulnerable Children Youth Stud. 2012;7(1):20–35.
19. Getachew M, Alemseged F, Abrea M, et al. Factors affecting fertility decisions of married men and women living with HIV in South Wollo Zone, Northeast Ethiopia. Ethiop J Health Dev. 2010;214–220.
20. Demissie DB, Tebeje B, Tesfaye T. Fertility desire and associated factors among people living with HIV attending antiretroviral therapy clinic in Ethiopia. BMC Pregnancy Childbirth. 2014;14(382). doi:10.1186/s12884-014-0382-2
21. Ahmed MM, Kahsay G, Miruts G, et al. Magnitude and factors affecting the fertility desire of people living with HIV infection in ethiopia- a cross sectional study. J AIDS Clin Res. 2014;5(9). doi:10.4172/2155-6113.1000343
22. Koyra HC, Biramo YB, Tufa EG. Fertility desire and associated factors among people living with HIV/AIDs at selected health facilities of Wolaita Zone, Southern Ethiopia: cross- sectional study. Am J Public Health Res. 2017;5(3):79–88.
23. Mmbaga EJ, Leyna GH, Ezekiel MJ, Kakoko DC. Fertility desire and intention of people living with HIV/AIDS in Tanzania: a call for restructuring care and treatment services. BMC Public Health. 2013;13(86). doi:10.1186/1471-2458-13-86
24. Gutin SA, Namusoke F, Shade SB, et al. Fertility desires and intentions among HIV-positive women during the post-natal period in Uganda. Afr J Reprod Health. 2014;18(3).
25. Menna T, Wordofa H. Prevalence of fertility desire and its associated factors among 15- to 49-year-old people living with HIV/AIDS in Addis Ababa, Ethiopia: a cross-sectional study design. HIV/AIDS - Res Palliat Care. 2017;9:167–176. doi:10.2147/HIV.S133766
26. Haile F, Isahak N, Dessie A. Fertility desire and associated factors among people living with HIV on ART, In Harari Regional State, Eastern Ethiopia. J Trop Dis. 2014;2(3).
27. Melaku YA, Zeleke EG, Kinsman J, Abraha AK. Fertility desire among HIV-positive women in Tigray region, Ethiopia: implications for the provision of reproductive health and prevention of mother-to-child HIV transmission services. BMC Women’s Health. 2014;14(1). doi:10.1186/s12905-014-0137-2
28. Mokwena K, Bogale YR. Fertility intention and use of contraception among women living with the human immunodeficiency virus in Oromia Region, Ethiopia. S Afr Family Pract. 2016;59(1):46–51. doi:10.1080/20786190.2016.1254931
29. Adler DH, Abar B, Bennie T, et al. Childbearing intentions among sexually active HIV-infected and HIV-uninfected female adolescents in South Africa. J AIDS HIV Res. 2017;9(7):159–163.
30. Talbot LA, Musiol RJ, Witham EK, et al. Falls in young, middle-aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health. 2005;5(1):86.
31. Pattaramongkolrit S, Sindhu S, Thosigha O, et al. Fall-related factors among older, visually-impaired Thais. Pac Rim Int J Nurs Res. 2013;17(2):181–196.
32. Abbawa F, Awoke W, Alemu Y. Fertility desire and associated factors among clients on highly active antiretroviral treatment at finoteselam hospital Northwest Ethiopia: a cross sectional study. Reprod Health. 2015;12:69. doi:10.1186/s12978-015-0063-2
33. Friedman SM, Munoz B, West SK, et al. Falls and fear of falling: which comes first? A longitudinal prediction model suggests strategies for primary and secondary prevention. J Am Geriatr Soc. 2002;50(8):1329–1335.
34. Kalula SZ, Ferreria M, Swingler G, et al. Prevalence of falls in an urban community-dwelling older population of Cape Town, South Africa. J Nutr Health Aging. 2015;19(10):1024–1031.
35. Souza MR, Do Amaral WN, Guimarães RA, et al. Reproductive desire among women living with HIV/AIDS in Central Brazil: prevalence and associated factors. PLoS One. 2017;12(10):e0186267.
36. Berhan Y, Berhan A. Meta-analyses of fertility desires of people living with HIV. BMC Public Health. 2013;13(409). doi:10.1186/1471-2458-13-409
37. Alemayehu B, Aregay A. Desire to procreate among people living with HIV/AIDS: determinants in Ethiopia: a cross-sectional study. J AIDS HIV Res. 2012;4(5). doi:10.5897/JAHR11.042
38. Regassa T, Fantahun M. Fertility desire and reproductive health care needs of men and women living with HIV/AIDS in Nekemte, East Wollega, Ethiopia. Sci Technol Arts Res J. 2012;1(3):31–38. doi:10.4314/star.v1i3.98797
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.