")
Back to Journals » International Journal of Women's Health » Volume 9
Female sexual dysfunction: a focus on flibanserin
Authors Lodise NM
Received 24 September 2016
Accepted for publication 18 January 2017
Published 11 October 2017 Volume 2017:9 Pages 757—767
DOI https://doi.org/10.2147/IJWH.S83747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Nicole M Lodise
Department of Pharmacy Practice, Albany College of Pharmacy and Health Sciences, Albany, NY, USA
Abstract: Flibanserin is the first US Food and Drug Administration (FDA)-approved option for sexual dysfunction, specifically low sexual desire. Until recently, there were no FDA-approved medication options to assist the ~40% of women affected by female sexual dysfunction (FSD). Often, patients report feeling uncomfortable discussing sexual health, identifying a strong need for health care professionals (HCPs) to proactively reach out to patients to identify concerns and initiate a discussion about sexual health and the available treatment options. Within the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DMS-5), the criteria of female sexual interest/arousal disorder (FSIAD) are outlined, encompassing one of the most common sexual concerns, formerly in its own category defined as hypoactive sexual desire disorder (HSDD) or low sexual desire. HSDD is the absence or deficiency of sexual interest and/or desire leading to significant distress and interpersonal difficulties. HCPs offer an important service in assessing their patients and providing information about treatment considerations while ensuring patient comfort with this topic. This article provides an overview of the types and potential causes associated with FSD and the role of flibanserin in practice as a treatment option. Despite a need for additional study in diverse populations, flibanserin has demonstrated efficacy with increased female sexual function index (FSFI) total and desire domain scores in clinical studies indicating benefit in sexual desire. Common patient or provider-administered assessment tools to assist in identifying affected patients and patient counseling strategies are reviewed.
Keywords: female sexual dysfunction, low sexual desire, hypoactive sexual desire disorder, pharmacotherapy, flibanserin
Introduction
Female sexual dysfunction (FSD) is patient specific and may present as changes in a patient’s orgasm, concerns with vaginal pain and penetration and/or female sexual interest/arousal disorder (FSIAD), including low sexual desire or hypoactive sexual desire disorder (HSDD).1 Table 1 provides a summary of the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) criteria for FSD. A 2006 review by Hayes et al2 estimated the prevalence of female concerns with desire to be 64%, orgasm to be 35%, arousal to be 31% and pain concerns estimated to be 26%. In comparison, Shifren et al3 surveyed more than 30,000 females in the US noting a prevalence of any type of sexual dysfunction in ~40% of respondents. Patients may present with one type of sexual dysfunction or a combination, although less common, with the possibility of personal distress associated with each. Low sexual desire is the most commonly reported sexual health problem with a prevalence of 38.7% compared to a 10% approximate prevalence when patients experience low desire and associated personal distress.3 The Women’s International Study of Health and Sexuality (WISHeS) study in 2006 estimated a prevalence of low sexual desire in premenopausal and postmenopausal women of 14% and 9%–26%, respectively.4 More recently, Rosen et al5 surveyed ~700 women across the US at multiple clinical sites identifying ~7.4% of women reporting low sexual desire, specifically HSDD. Although a range of prevalence rates exist, sexual dysfunction among women is commonly reported and may represent a significant concern and opportunity for education. Low sexual desire is the most common type and identifies a key area for clinicians to proactively engage their patients in open communication to ensure that affected patients are identified and recommended options, as necessary, are discussed with the patient.
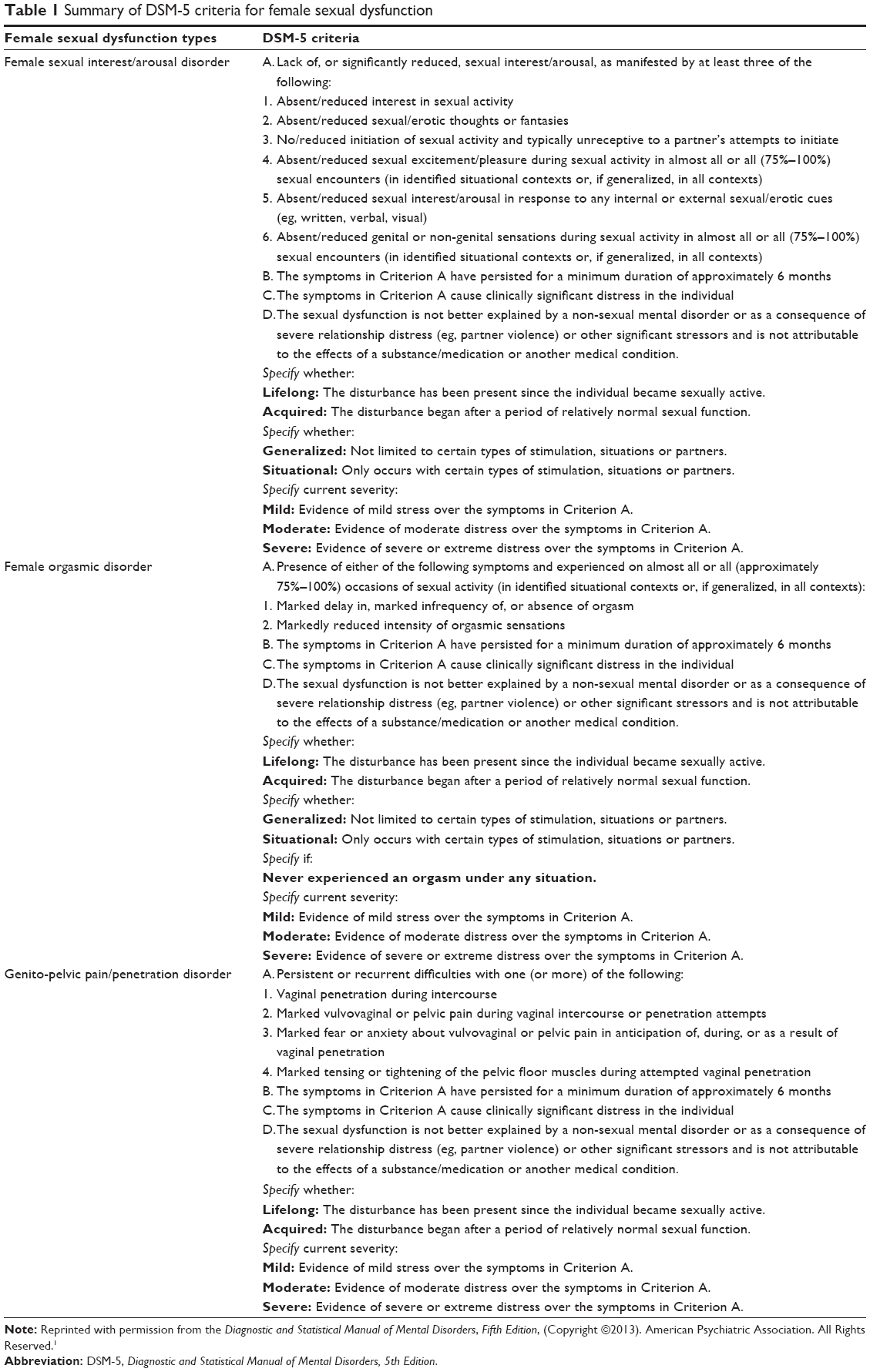 | Table 1 Summary of DSM-5 criteria for female sexual dysfunction |
Normal sexual response has been defined through various models. One of the initial models from Masters and Johnson proposed a linear model to describe the sexual response identifying the following four stages: excitement, plateau, orgasm and resolution.6 In comparison, the model by Kaplan expanded on this model from Masters and Johnson to further incorporate the importance of desire and modified the phases to focus on desire, excitement and orgasm.6 More recently, the model by Basson et al presented a further variation of the earlier models with a combined circular and linear focused model that centers on sexual stimuli, emotional intimacy and psychological components as factors contributing to overall sexual activity demonstrating the complexity and ever-evolving assessment of sexual response.6 Each of these models, although differing in their area of focus, represent the complexity and multifactorial nature of an individual’s sexual response.
The pathophysiology of sexual functioning, and therefore dysfunction, involves the role of neurotransmitters in addition to possible hormonal contributors. Neurotransmitters such as dopamine, norepinephrine and serotonin have involvement in a patient’s sexual response, with dopamine and norepinephrine providing an excitatory effect versus serotonin having an inhibitory effect.7,8 Hormonal changes, associated with estrogen in naturally occurring or surgically induced menopausal patients, may also alter a patient’s sexual activity and interest. Specifically, estrogen reductions may increase vaginal dryness and dyspareunia, increasing the potential for sexual dysfunction.9,10
FSD can possibly affect any woman at any age.11,12 Existing factors such as medication use, current medical conditions and psychological factors also contribute to the possibility of FSD. Medications and current medical conditions such as cardiovascular disease, diabetes mellitus and gynecologic cancers in addition to the use of antidepressants or the use of recreational drugs may increase the possible risk for sexual dysfunction.11,13,14 Relationship issues as well as life stressors may also demonstrate a psychological impact on a patient’s sexual health and functioning.12,13,15
One of the most common types of sexual dysfunction is low sexual desire with associated distress, formerly known as HSDD. Within the DSM-5, HSDD is now a part of the criteria for FSIAD; however, this terminology may still be referred to in clinical practice and has been utilized within the criteria of several previous studies evaluating medications to treat low sexual desire. Treatment approaches for low sexual desire have focused on the use of behavioral modifications, possible use of testosterone, off-label pharmacologic options and complementary therapies. Until recently, with the availability of flibanserin, there were no available FDA-approved treatment options. A literature search was completed utilizing PubMed to identify published articles within the last 10 years (2006–2016) in humans and available in English for evaluating the safety, efficacy and patient counseling considerations associated with flibanserin as a treatment option for low sexual desire. Key search words included flibanserin, HSDD and FSD. A total of 58 articles were identified.
This article focuses solely on key features regarding flibanserin, while the use of additional pharmacologic options investigated to treat FSD or low sexual desire is described in previous publications.7,16–23
Patient assessment tools
The DSM-5 classifies female sexual disorders as female orgasmic disorder, FSIAD and genito-pelvic pain/penetration disorder (Table 1).1 The DSM-5 further includes four specific subtypes to categorize dysfunction onset as follows: lifelong dysfunction indicating a sexual problem present from the first sexual experience; acquired dysfunction identifying sexual health issues that arise after a time of normal sexual activity; generalized dysfunction referring to sexual issues not limited to a specific situation or partner, while situational dysfunction occurs with specific partners or situations.1 As a complement to DSM-5, health care professionals (HCPs) may successfully incorporate additional tools to assess a patient. These tools may be administered either by the patient or the provider to assist in collecting information or initially identifying a patient’s possible sexual health concerns. Despite possible tools and patient interest for additional sexual health information from HCPs, challenges in initiating communication on sexual health continue to be present in clinical practice across patient ages with identified concerns such as a need for further HCP sexual health knowledge and limitations on available time to discuss with patients.24–26 It is important for HCPs to remain cognizant of these considerations to optimize the patient–HCP interaction regarding sexual health.
When screening for FSD, specifically low sexual desire, available tools may assist HCPs and often have had demonstrated use within clinical studies. Several validated questionnaires may be used including the brief sexual symptom checklist, the female sexual function index (FSFI) and the decreased sexual desire screener (DSDS).27–29 The brief sexual symptom checklist uses one initial question to assess a patient’s satisfaction with their sexual functioning and based on this response, patients may provide further information to identify possible sexual problems and interest in discussing further with their HCP.27 The FSFI is a 19-question tool covering six domains assessing desire, arousal, orgasm, lubrication, pain and satisfaction. Each domain is associated with a maximum score of up to six points out of the total FSFI score (maximum total score on all domains is 36 points). The FSFI desire score is based on 2 of the 19 questions within the tool focused on sexual desire: “Over the past four weeks, how often did you feel sexual desire or interest?” and “Over the past four weeks, how would you rate your level of sexual desire or interest?”28 The FSFI desire score has also been used as a primary or secondary end point in studies evaluating the efficacy of medications used to treat low sexual desire. The lower the FSFI score, the higher the likelihood of sexual dysfunction. The FSFI is a longer questionnaire assessing each type of sexual dysfunction including desire; in comparison, the DSDS offers a condensed option for HCPs to solely assess low sexual desire. Although brief, the DSDS provides questions focused on desire using a “yes/no” format such as “Are you bothered by your decreased sexual desire or interest”.29 With each tool, clinicians are encouraged to engage in a more detailed discussion with a patient regarding their sexual health including the use of open-ended questioning on when and how the dysfunction is occurring while using the responses from the administered questionnaires to facilitate the interaction.
More recently, Weinfurt et al30 described the development process of a lengthier assessment tool to assess sexual functioning in males and females, the PROMIS Sexual Function and Satisfaction Measures version 2.0 tool. This tool offers another option to broadly assess patients regarding overall sexual health. Another tool, described by Flynn et al,31 in comparison to the brief option of the DSDS, is a nonspecific tool, called the “checklist screener” to assess sexual functioning. This tool includes an initial question regarding if a patient has had any problems or concerns over the past year for a minimum of 3 months such as “pain during or after sexual activity”; “difficulty having an orgasm” and “whether the patient enjoyed sexual activity”.31 Despite this tool’s general focus, it does provide another opportunity to gather this type of information from patients to further initiate a patient discussion.
Treatment
The multifactorial nature of FSD and low sexual desire indicates a need for various approaches to assist patients. Upon completion of the use of a patient assessment tool or through general open-ended questioning within a visit, it is important for HCPs to consider possible causes, if known, regarding a patient’s identified low sexual desire to best target possible, customized treatment options whether nonpharmacologic or pharmacologic to assist the patient. For example, if the cause is medication related, an initial approach may be to seek out alternative agents not known to increase the risk of sexual dysfunction. If a patient has described relationship or stress considerations, a recommendation referring the patient to a couple’s counselor may be an initial step in the overall treatment approach. Given the number of factors that may affect low sexual desire, it is critical for the HCP to create a treatment plan addressing any of the possible contributors.
Nonpharmacologic and behavioral recommendations
Nonpharmacologic and behavioral recommendations offer an important step in a patient’s treatment plan to consider, especially in patients uncomfortable in trying pharmacologic options. One of the goals of an HCP is to assess nonpharmacologic avenues that may offer possible improvement in low sexual desire. As described earlier, for example, recommendation for couple’s counseling may be advantageous if relationship issues are identified. Other nonpharmacologic options are also being explored. Recent studies evaluating the use of a sacral nerve stimulator for its use in treating FSD symptoms have demonstrated statistically significant benefits with desire, orgasm, lubrication and satisfaction.16,32,33 In addition, Oakley et al34 evaluated the use of twice weekly acupuncture for 5 weeks to treat low sexual desire in a small patient population of premenopausal females (N=15). Despite the lack of blinding and small patient enrollment as limitations, improvements in FSFI desire and total scores were noted, indicating the need for further evaluation of acupuncture in larger patient samples to assess its role in low sexual desire. With the significant potential for psychological and lifestyle causes, behavioral strategies represent an integral component in a patient’s plan.10 The use of cognitive behavioral therapy or use of a sex therapist has demonstrated positive benefits in sexual dysfunction including low sexual desire.35 With the use of either of these approaches, the focus centers on addressing the behaviors and thoughts associated with sexual activity in an effort to establish new routines and associations to address sexual concerns. With any patient experiencing sexual health concerns, the importance of incorporating behavioral strategies with or without the use of medications will be critical in a patient’s overall treatment plan to address concerns.36
Pharmacologic – flibanserin
There are several agents that have been investigated as possible treatment options to assist patients with FSD, specifically low sexual desire. These agents include testosterone, bupropion, sildenafil, melanocortin receptor agonists and the use of complementary products such as dehydroepiandrosterone (DHEA); however, until recently, there were no FDA-approved options specifically for FSD.7,16–23 Flibanserin is now the first FDA-approved pharmacologic option for low sexual desire or HSDD. Flibanserin focuses on the role of neurotransmitters within the sexual response. It acts as a serotonin 5-HT1A agonist in addition to a 5-HT2A antagonist. Through this action, it reduces the inhibitory effect of serotonin while increasing the excitatory effect of dopamine.37,38 Flibanserin has had prior submissions and denials with its approval secondary to side effects; however, in 2015, the US Food and Drug Administration (FDA) voted 18 to 6 to recommend the approval of Flibanserin as a treatment for HSDD in premenopausal women.39,40 Although there are important safety considerations and monitoring associated with this agent, it does fill a gap and opens the opportunity for further medication approvals in this therapeutic area. Furthermore, with patient and clinician awareness about the availability of this medication, it may serve as a way to further facilitate the discussion about sexual health with patients.
Flibanserin – dosing and pharmacokinetics
Flibanserin is available as a 100 mg tablet and is recommended to be taken orally once daily at bedtime.41,42 Dosing at bedtime is advised to minimize side effects including somnolence, hypotension and syncope.42 Administration of flibanserin with food does increase the extent of absorption while slowing the rate of absorption.42 Flibanserin’s bioavailability is 33% and is 98% protein bound; has a half-life of 11 hours and is extensively metabolized by the liver through cytochrome P450 3A4 (CYP3A4); however, it is also metabolized by CYP2C19.42 Flibanserin’s exposure increases 4.5-fold resulting in an increased risk of hypotension and syncope in patients with hepatic impairment.42 Given the dramatic increase in exposure, use in patients with any level of hepatic impairment should be avoided. Although metabolism is less with CYP2C19, patients who are poor metabolizers of CYP2C19 should also receive additional counseling, but may continue to use as tolerated, regarding increased side effects due to elevated exposure.42 Use in geriatric patients is currently not advised due to a lack of safety and efficacy data in this specific population.42
Flibanserin – safety and cost considerations
The side effect profile of flibanserin includes a potential for dizziness, somnolence, nausea and fatigue as the most commonly reported in clinical trials (~10% incidence of each).43–47 The possibility for drug interactions with strong CYP3A4 inhibitors (eg, itraconazole and ketoconazole) is also present with flibanserin. This interaction warrants proactive patient counseling on the risk and the importance in comprehensively reviewing all other current medications utilized by the patient. The combination with CYP3A4 inhibitors increase flibanserin levels and related side effects such as hypotension and syncope.41,42 In addition to interactions with CYP3A4 inhibitors, flibanserin also presents a significant interaction when used in combination with alcohol. This combination increases the risk of hypotension and syncope and is contraindicated.42 Given this interaction, flibanserin use is restricted through a risk evaluation and mitigation strategy (REMS) program requiring both the prescriber and the pharmacy to be certified (www.AddyiREMS.com).48
In addition to use restrictions due to adverse effects, cost may also present an important factor, with patients considering flibanserin use as the availability of insurance coverage and the depth of coverage varying greatly. Therefore, flibanserin’s manufacturer established flibanserin-affordable access cards to assist in reducing patient cost burden.48
Flibanserin – efficacy
The efficacy of flibanserin continues to be debated regarding its overall clinical significance and the potential for variability with its effect among patients; however, statistical significance has been demonstrated within several efficacy and safety studies available on flibanserin. Most recently, a thoughtful review and meta-analysis focused on this debate analyzing previous published and unpublished randomized clinical trials on flibanserin indicating an overall modest clinically significant efficacy.49 The analysis considered important limitations in the clinical trials including the limited diversity among study populations since many medical conditions and the use of various medications were excluded among study participants potentially reducing generalizability.49 In addition, the possible limitations with the broad use of flibanserin were identified due to the higher risk of adverse effects versus placebo such as hypotension and syncope due to the interaction with alcohol. This analysis demonstrates the need for continued evaluation of flibanserin in patients with expanded medical and medication histories beyond what was represented in study populations to further assist HCPs in better defining the role of flibanserin.49 Despite concerns, currently, this medication represents the only approved option for patients but does require strong patient-specific counseling regarding adverse effects and drug and alcohol interactions with use. As the primary randomized clinical trials evaluating flibanserin use have been reviewed in great detail elsewhere, this article provides a brief review of select end point results for comparison among recent studies used in assessing flibanserin’s safety and efficacy in supporting flibanserin’s FDA approval.49 Flibanserin has been evaluated predominantly in premenopausal female patients with an initial study focusing on postmenopausal patients. Table 2 recaps select end points from each of these trials for comparison.43–47,50 The DAISY and VIOLET trials were both 24-week randomized, double-blind, placebo-controlled studies evaluating the use of flibanserin in premenopausal females. Both trials included various dosing options with DAISY evaluating 50 mg twice daily (N=392) and 100 mg once daily at bedtime (N=395) compared to placebo (N=398) and VIOLET evaluating 50 mg once daily (N=295) and 100 mg once daily (N=290) at bedtime versus placebo (N=295). Improvements in the number of sexually satisfying events, FSFI desire and total scores and overall distress reported with the Female Sexual Distress Scale-Revised (FSDS-R) total and Item 13 scores were noted in both trials, specifically demonstrating improvements with the 100 mg once daily dosing.43,44 The ROSE and SUNFLOWER studies further assessed continued efficacy versus possible withdrawal effects and overall adverse effects, respectively.45,47 Within the ROSE trial, participants who responded positively to an open-label 24-week trial taking either 50 mg or 100 mg per day of flibanserin (N=333) were randomized and blinded to receive additional 24 weeks of their optimal flibanserin dose (N=163) versus placebo (N=170). Although a decline in primary and secondary outcomes was reported in both the flibanserin and placebo groups, there continued to be a statistically significant difference between flibanserin and placebo in the number of sexually satisfying events and the FSFI desire score demonstrating less of a decline in the flibanserin group at 48 weeks.47 The SUNFLOWER study was a 52-week open-label study focused on the safety and tolerability of flibanserin. Participants involved with earlier flibanserin randomized trials were invited to participate within the SUNFLOWER trial (N=1,725 eligible to include with 962 completing the full 52 weeks).45 Primary end points included incidence of somnolence, sedation, fatigue, dizziness, nausea and vomiting in addition to serious adverse effects and discontinuations. Somnolence was reported most commonly followed by fatigue, dizziness, nausea, sedation and vomiting. More than 95% of the adverse effects were reported as mild or moderate; however, ~10% of participants discontinued treatment due to adverse effects. Although a secondary end point in this trial, efficacy was demonstrated by increased FSFI total and desire scores indicating improvements in sexual desire compared to baseline.45 Another trial focusing on the efficacy and safety of flibanserin in premenopausal women was the BEGONIA study.46 BEGONIA was a randomized placebo-controlled 24-week study evaluating flibanserin 100 mg at bedtime (N=542) compared to placebo (N=545). At study completion, improvements were noted in the number of sexually satisfying events, FSFI desire and total scores in addition to reported distress within the FSDS-R total and Item 13 scores. Somnolence and dizziness were identified as the most common adverse effects associated with flibanserin use.
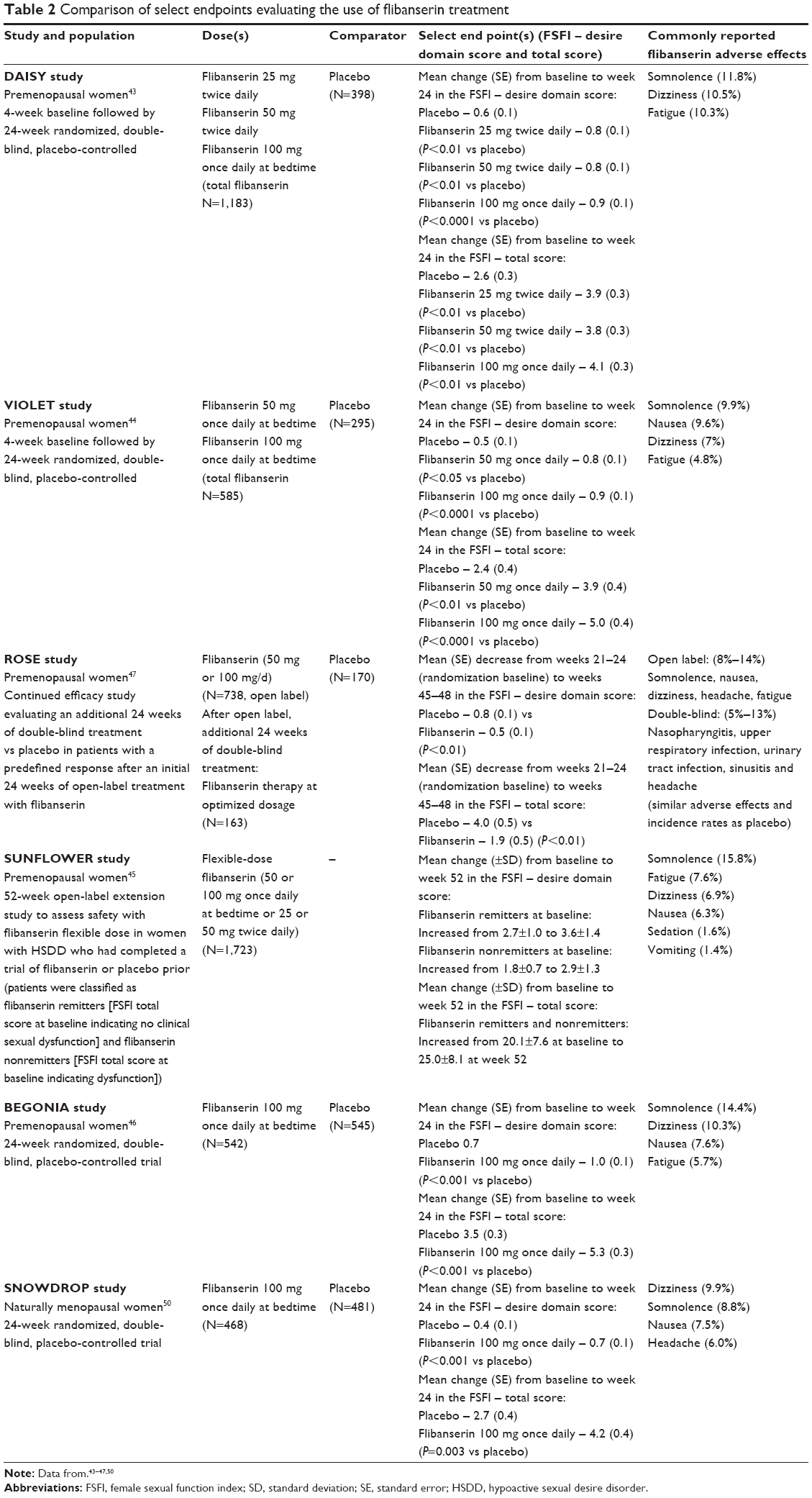 | Table 2 Comparison of select endpoints evaluating the use of flibanserin treatment |
Although the majority of data available is specific for premenopausal females and the current approval is for use only in premenopausal patients, flibanserin is also evaluated in postmenopausal patients. The SNOWDROP trial was a randomized, double-blind, placebo-controlled trial in naturally postmenopausal women assessing the use of flibanserin 100 mg at bedtime (N=468) compared to placebo (N=481) in postmenopausal women for 24 weeks. The number of sexually satisfying events, FSFI desire scores and distress based on the FSDS-R total and Item 13 scores showed a statistically significant improvement in the flibanserin group compared to placebo at 24 weeks.50 The FDA has summarized flibanserin’s overall demonstrated efficacy as statistically significant improvements in sexual desire with an estimated increase of ~0.5–1.0 additional sexually satisfying event per month.51 Given the modest efficacy and potential for significant side effects, discussion is ongoing to further define the clinical significance of efficacy results and the broad applicability and use of flibanserin across diverse patient populations. Despite this, flibanserin does offer the first approved option for female patients with low sexual desire and opens an opportunity to further engage in patient-specific dialogue regarding sexual health.
Flibanserin – study limitations
One of the limitations when assessing the efficacy of flibanserin across available studies involves the different tools used (objective versus patient reported) as primary and secondary end points and potential concerns identified regarding the usefulness of the information collected by tools such as the e-Diary to demonstrate a significant clinical outcome.52 Common tools used in clinical trials to evaluate a medication’s effectiveness for sexual dysfunction have included the use of patient diaries, the number of satisfying sexual events (SSEs), the FSFI tool assessing reduced desire and overall sexual dysfunction and the FSDS-R total and Item 13 score to assess personal distress. Despite use in study trials, there may be challenges in determining the significance of the information collected through tools such as e-Diaries.53 The use of patient-reported outcomes such as the FSFI tool may be considered more beneficial in not only collecting components of sexual health but also evaluating treatment options versus the use of e-Diaries.52,53 In flibanserin studies, patient diaries were used as primary outcomes while the FSFI tool was used as a secondary outcome (DAISY, VIOLET trials) compared to later studies (BEGONIA, SNOWDROP trials), the FSFI tool was identified as a primary outcome instead.43,44,46,50,53
With potential concerns of inconsistency in the assessment of clinical outcomes based on the varied measurement tools used across trials, Table 2 focuses on the FSFI desire and total scores for the reader to consider in assessing similar outcomes across select trials.
Patient counseling strategies and flibanserin use in practice
Patient counseling strategies
As described earlier, there may be challenges for patients and HCPs when considering discussions regarding sexual health.24–26 At a minimum, HCPs may simply engage patients in open-ended questions regarding whether a patient has any sexual health concerns in addition to the use of available tools or communication models to further assist in initiating a conversation. HCPs play a pivotal role in offering guidance addressing specific questions and discussion on possible treatment approaches to consider.
When additional tools are considered for use, as previously described, the checklist screener or the brief DSDS screener may be possible options to incorporate to initiate a patient conversation and collect information.29,31 In addition, structured models such as the Sexual Health Model (SHM) and the Permission, Limited Information, Specific Suggestions and Intensive Therapy (PLISSIT) model have been used to assist in discussing sexual health concerns.54 Annon’s widely referenced PLISSIT model focuses on the abovementioned four components within individual patient interactions to assist the patient and the HCP in reviewing the patient’s sexual health considerations.55 This model has been consistently identified as a possible option to assist health professionals in providing a guide to a comprehensive discussion on sexual health but may also be consulted as an approach to enhance patient care.56–59 This model also offers the HCP the opportunity to provide additional information on resources, treatment options and possible referrals within a comfortable environment. SHM is another approach that offers an opportunity to engage patients.60 This model uses a group approach to discuss sexual health with a focus centered on behavioral modifications. The use of this model, however, may be limited based on a patient’s comfort level to participate in a group environment but does offer a cost-effective method to target several patients.54 Although the SHM model focuses primarily on behavioral modifications, both the PLISSIT and the SHM models do reinforce the benefit of including patient discussion on behavioral strategies.36 Ultimately, the approach used to initiate a discussion will be individualized for the HCP and the patient. Each of the abovementioned options assist in facilitating an organized, detailed patient conversation on this topic and may be used to not only collect this information but also offer a supportive environment to discuss treatment strategies regarding sexual health considerations.
Flibanserin use in practice
Low sexual desire is a commonly reported sexual health problem with a prevalence ranging from 10% to over 30%. Although several investigated agents have been explored, currently, there is only one FDA-approved option, flibanserin. Flibanserin is approved to treat low sexual desire in premenopausal females. The combination with the use of behavioral approaches should be considered. Despite concerns regarding the impact and clinical significance of flibanserin’s efficacy, there are demonstrated improvements showing an increase, although small, in sexual desire in select patients. If flibanserin is selected as a treatment option, patients must also receive counseling regarding the concomitant use with strong CYP3A4 inhibitors and be advised to avoid use with alcohol due to an increased risk of hypotension and syncope.
As the first approved medication for low sexual desire, even with counseling considerations and concerns regarding broad use and efficacy, flibanserin provides an option for patients desiring an FDA-approved medication to address low sexual desire. As described in the Jaspers et al’s article,49 additional study of flibanserin in diverse populations will be advantageous to further define flibanserin’s role and the patients best suited for use to ensure optimal efficacy.
The approval of flibanserin is an opportunity and a call to HCPs to further engage in discussion with their patients regarding sexual health while promoting the ongoing investigation of additional pharmacologic options to address FSD.
Acknowledgment
No grants, equipment or drugs were received by the author in support of this publication.
Disclosure
The author reports no conflicts of interest in this work.
References
American Psychiatric Association. Sexual dysfunctions. In: American Psychiatric Association, editor. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Publishing; 2013. | ||
Hayes RD, Bennett CM, Fairley CK, Dennerstein L. What can prevalence studies tell us about female sexual difficulty and dysfunction? J Sex Med. 2006;3(4):589–595. | ||
Shifren J, Monz BU, Russo PA, Segreti A, Johannes CB. Sexual problems and distress in United States women: prevalence and correlates. Obstet Gynecol. 2008;112(5):968–969. | ||
Leiblum S, Koochaki PE, Rodenberg CA, Barton IP, Rosen RC. Hypoactive sexual desire disorder in postmenopausal women: US results from the Women’s International Study of Health and Sexuality (WISHeS). Menopause. 2006;13(1):46–56. | ||
Rosen RC, Connor MK, Miyasato G, et al. Sexual desire problems in women seeking healthcare: a novel study design for ascertaining prevalence of hypoactive sexual desire disorder in clinic-based samples of US women. J Womens Health. 2012;21(5):505–515. | ||
Hayes RD. Circular and linear modeling of female sexual desire and arousal. J Sex Res. 2011;48(2–3):130–141. | ||
Woodis CB, McLendon AN, Muzyk AJ. Testosterone supplementation for hypoactive sexual desire disorder in women. Pharmacotherapy. 2012;32(1):38–53. | ||
Pfaus JG. Reviews: pathways of sexual desire. J Sex Med. 2009;6(6):1506–1533. | ||
Levine KB, Williams RE, Hartmann KE. Vulvovaginal atrophy is strongly associated with female sexual dysfunction among sexually active postmenopausal women. Menopause. 2008;15(4 pt 1):661–666. | ||
Kingsberg SA, Woodard T. Female sexual dysfunction: focus on low desire. Obstet Gynecol. 2015;125(2):477–486. | ||
Buster JE. Managing female sexual dysfunction. Fertil Steril. 2013;100(4):905–915. | ||
Latif EZ, Diamond MP. Arriving at the diagnosis of female sexual dysfunction. Fertil Steril. 2013;100(4):898–904. | ||
Faubion SS, Rullo JE. Sexual dysfunction in women: a practical approach. Am Fam Physician. 2015;92(4):281–288. | ||
Sharma JB, Kalra B. Female sexual dysfunction: assessment. J Pak Med Assoc. 2016;66(5):623–626. | ||
Brotto LA, Blitzer J, Laan E, Leiblum S, Luria M. Women’s sexual desire and arousal disorders. J Sex Med. 2010;7(1 pt 2):586–614. | ||
Houman J, Feng T, Eilber KS, Anger JT. Female sexual dysfunction: is it a treatment disease? Curr Urol Rep. 2016;17(28):1–6. | ||
Segraves RT, Clayton A, Croft H, Wolf A, Warnock J. Bupropion sustained release for the treatment of hypoactive sexual desire disorder in premenopausal women. J Clin Psychopharmacol. 2004;24(3): 339–342. | ||
van Rooij K, Poels S, Worst P, et al. Efficacy of testosterone combined with a PDE5 inhibitor and testosterone combined with a serotonin (1A) receptor agonist in women with SSRI-induced sexual dysfunction. A preliminary study. Eur J Pharmacol. 2015;753:246–251. | ||
Nurnberg HG, Hensley PL, Heiman JR, Croft HA, Debattista C, Paine S. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300(4): 395–404. | ||
Berman JR, Berman LA, Toler SM, Gill J, Haughie S; Sildenafil Study Group. Safety and efficacy of sildenafil citrate for the treatment of female sexual arousal disorder: a double-blind, placebo controlled study. J Urol. 2003;170(6 pt 1):2333–2338. | ||
Safarinejad MR. Evaluation of the safety and efficacy of bremelanotide, a melanocortin receptor agonist, in female subjects with arousal disorder: a double-blind placebo-controlled, fixed dose, randomized study. J Sex Med. 2008;5(4):887–897. | ||
Labrie F, Archer DF, Koltun W, et al. Efficacy of intravaginal dehydroepiandrosterone (DHEA) on moderate to severe dyspareunia and vaginal dryness, symptoms of vulvovaginal atrophy, and of the genitourinary syndrome of menopause. Menopause. 2016;23(3):243–256. | ||
Labrie F, Archer D, Bouchard C, et al. Effect of intravaginal dehydroepiandrosterone (Prasterone) on libido and sexual dysfunction in postmenopausal women. Menopause. 2009;16(5):923–931. | ||
Fuzzell L, Fedesco HN, Alexander SC, Fortenberry JD, Shields CG. “I just think that doctors need to ask more questions”: sexual minority and majority adolescents’ experiences talking about sexuality with healthcare providers. Patient Educ Couns. 2016;99(9):1467–1472. | ||
McCool ME, Apfelbacher C, Brandstetter S, Mottl M, Loss J. Diagnosing and treating female sexual dysfunction: a survey of the perspectives of obstetricians and gynaecologists. Sex Health. 2016;13(3):234–240. | ||
Clark RD, Williams AA. Patient preferences in discussing sexual dysfunctions in primary care. Fam Med. 2014;46(2):124–128. | ||
Hatzichristou D, Rosen RC, Derogatis LR, et al. Recommendations for the clinical evaluation of men and women with sexual dysfunction. J Sex Med. 2010;7(1 pt 2):337–348. | ||
Rosen R, Brown C, Heiman J, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual dysfunction. J Sex Marital Ther. 2000;26(2):191–208. | ||
Clayton A, Goldfischer ER, Goldstein I, DeRogatis L, Lewis-D’Agostino DJ, Pyke R. Validation of the decreased sexual desire screener (DSDS): a brief diagnostic instrument for generalized acquired female hypoactive sexual desire disorder (HSDD). J Sex Med. 2009;6(3):730–738. | ||
Weinfurt KP, Lin L, Bruner DW, et al. Development and initial validation of the PROMIS® sexual function and satisfaction measures version 2.0. J Sex Med. 2015;12(9):1961–1974. | ||
Flynn KE, Lindau ST, Lin L, et al. Development and validation of a single-item screener for self-reporting sexual problems in U.S. adults. J Gen Intern Med. 2015;30(10):1468–1475. | ||
Pauls RN, Marinkovic SP, Silva WA, Rooney CM, Kleeman SD, Karram MM. Effects of sacral neuromodulation on female sexual function. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):391–395. | ||
Signorello D, Seitz CC, Berner L, et al. Impact of sacral neuromodulation on female sexual function and the correlation with clinical outcome and quality of life indexes: a monocentric experience. J Sex Med. 2011;8(4):1147–1155. | ||
Oakley SH, Walther-Liu J, Crisp CC, Pauls RN. Acupuncture in premenopausal women with hypoactive sexual desire disorder: a prospective cohort pilot study. Sex Med. 2016;4(3):e176–e181. | ||
Gunzler C, Berner MM. Efficacy of psychosocial interventions in men and women with sexual dysfunctions – a systematic review of controlled clinical trials: part 2 – the efficacy of psychosocial interventions for female sexual dysfunction. J Sex Med. 2012;9(12):3108–3125. | ||
Brotto LA. Flibanserin. Arch Sex Behav. 2015;44(8):2103–2105. | ||
Reviriego C. Flibanserin for female sexual dysfunction. Drugs Today. 2014;50(8):549–556. | ||
Stahl SM, Sommer B, Allers KA. Multifunctional pharmacology of flibanserin: possible mechanism of therapeutic action in hypoactive sexual desire disorder. J Sex Med. 2011;8(1):15–27. | ||
Gellad WF, Flynn KE, Alexander GC. Evaluation of flibanserin: science and advocacy at the FDA. JAMA. 2015;314(9):869–870. | ||
Roehr B. FDA committee recommends approval for “female Viagra”. BMJ. 2015;350:h3097. | ||
FDA. Flibanserin Medication Guide; 2015. Raleigh, NC: Sprout Pharmaceuticals-Guide approved by the Food and Drug Administration (FDA). Available from: http://www.fda.gov/downloads/Drugs/DrugSafety/UCM459254.pdf. Accessed May 1, 2016. | ||
Flibanserin [full prescribing information]; 2015. Raleigh, NC: Sprout Pharmaceuticals, A Division of Valeant Pharmaceuticals North America. Available from: www.addyi.com. Accessed May 1, 2016. | ||
Thorp J, Simon J, Dattani D, et al. Treatment of hypoactive sexual desire disorder in premenopausal women: efficacy of flibanserin in the DAISY study. J Sex Med. 2012;9(3):793–804. | ||
DeRogatis LR, Komer L, Katz M, et al. Treatment of hypoactive sexual desire disorder in premenopausal women: efficacy of flibanserin in the VIOLET study. J Sex Med. 2012;9(4):1074–1085. | ||
Jayne C, Simon JA, Taylor LV, Kimura T, Lesko L; SUNFLOWER Investigators. Open-label extension study of flibanserin in women with hypoactive sexual desire disorder. J Sex Med. 2012;9(12):3180–3188. | ||
Katz M, DeRogatis LR, Ackerman R, et al. Efficacy of flibanserin in women with hypoactive sexual desire disorder: results from the BEGONIA trial. J Sex Med. 2013;10(7):1807–1815. | ||
Goldfischer E, Breaux J, Katz M, et al. Continued efficacy and safety of flibanserin in premenopausal women with hypoactive sexual desire disorder (HSDD): results from a randomized withdrawal trial. J Sex Med. 2011;8(11):3160–3172. | ||
Valeant [webpage on the Internet]. Flibanserin Valeant Access Program; 2016. Raleigh, NC: Sprout Pharmaceuticals, A Division of Valeant Pharmaceuticals North America. Available from: http://www.valeantaccessprogram.com/addyi/. Accessed May 1, 2016. | ||
Jaspers L, Feys F, Bramer WM, Franco OH, Leusink P, Laan ETM. Efficacy and safety of flibanserin for the treatment of hypoactive sexual desire disorder in women: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(4):453–462. | ||
Simon JA, Kingsberg SA, Shumel B, Hanes V, Garcia M, Sand M. Efficacy and safety of flibanserin in postmenopausal women with hypoactive sexual desire disorder: results of the SNOWDROP trial. Menopause. 2014;21(6):633–640. | ||
FDA [webpage on the Internet]. FDA News Release: FDA Approves First Treatment for Sexual Desire Disorder. US Department of Health and Human Services: Food and Drug Administration (FDA); 2015. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm458734.htm. Accessed May 1, 2016. | ||
Sang JH, Kim TH, Kim SA. Flibanserin for treating hypoactive sexual desire disorder. J Menopausal Med. 2016;22(1):9–13. | ||
Kingsberg SA, Althof SE. Satisfying sexual events as outcome measures in clinical trial of female sexual dysfunction. J Sex Med. 2011;8(12):3262–3270. | ||
Farnam F, Janghorbani M, Raisi F, Merghati-Khoei E. Compare the effectiveness of PLISSIT and sexual health models on women’s sexual problems in Tehran, Iran: a randomized controlled trial. J Sex Med. 2014;11(11):2679–2689. | ||
Annon JS. The PLISSIT model: a proposed conceptual scheme for the behavioral treatment of sexual problems. J Sex Educ Ther. 1976; 2:1–15. | ||
Rostamkhani F, Ozgoli G, Merghati Khoei E, Jafari F, Alavi Majd H. Effectiveness of the PLISSIT-based counseling on sexual function of women. J Nurs Midwifery. 2012;22:1–9. | ||
Rostamkhani F, Jafari F, Ozgoli G, Shakeri M. Addressing the sexual problems of Iranian women in a primary health care setting: a quasi-experimental study. Iran J Nurs Midwifery Res. 2015;20(1):139–146. | ||
Rutte A, van Oppen P, Nijpels G, et al. Effectiveness of a PLISSIT model intervention in patients with type 2 diabetes mellitus in primary care: design of a cluster-randomised controlled trial. BMC Fam Pract. 2015;16:69. | ||
Khakbazan Z, Daneshfar F, Behboodi-Moghadam Z, Nabavi SM, Ghasemzadeh S, Mehran A. The effectiveness of the Permission, Limited Information, Specific Suggestions, Intensive Therapy (PLISSIT) model-based sexual counseling on the sexual function of women with Multiple Sclerosis who are sexually active. Mult Scler Relat Disord. 2016;8:113–119. | ||
Robinson BB, Munns R, Weber-Main A, Lowe M, Raymond N. Application of the sexual health model in the long-term treatment of hypoactive sexual desire and female orgasmic disorder. Arch Sex Behav. 2011;40(2):469–478. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.