")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Feeling "overloaded" and "shortcomings": milieu therapists' experiences of vulnerability in caring for severely mentally ill patients
Authors Bachmann L , Michaelsen R, Vatne S
Received 12 February 2016
Accepted for publication 21 April 2016
Published 13 July 2016 Volume 2016:9 Pages 285—296
DOI https://doi.org/10.2147/JMDH.S106310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Liv Bachmann, Ragnhild A Michaelsen, Solfrid Vatne
Faculty of Health Science, Molde University College, Molde, Norway
Background: Milieu therapists’ relationships with patients with severe mental illnesses are viewed as challenging. Elucidating vulnerability from their perspective in daily face-to-face encounters with patients might contribute to extending our knowledge about milieu therapists’ vulnerability and the dynamics of the interaction between patients in mental health services and expertise in building caring and therapeutic relationships. The aim of this project was to study educated milieu therapists’ experiences of their own vulnerability in their interactions with patients in mental health services.
Materials and methods: The data collection method was focus-group interviews. Thirteen part-time master’s in mental health students (eight nurses, three social workers, two social educators) participated. All participants had experience with community or specialized mental health services (2–8 years).
Results: The milieu therapists mainly related their experiences of vulnerability to negative feelings elicited by challenging work conditions, disclosed as two main themes: 1) “overloaded”, by the possibility of being physically and mentally hurt and the burdens of long-lasting close relationships; milieu therapists were extremely vulnerable because of their difficulty in protecting themselves; and 2) “shortcomings”, connected to feelings of despair associated with not acting in concordance with their professional standards and insecurity about their skills to handle challenging situations, which was a threat to their professional integrity. There seemed to be coherence between vulnerability and professional inauthenticity. A misunderstanding that professionalism refers to altruism seems to increase milieu therapist vulnerability.
Conclusion: Vulnerability in health care is of interest to multiple disciplines, and is of relevance for knowledge development in higher education. Extended knowledge and understanding about milieu therapists’ vulnerability might strengthen their personal and professional integrity in professional practice in mental health services. Health care managers’ focus on the supervision of individual professionals in practice and practical training is important. Further research on the coherence between vulnerability and professionalism is recommended.
Keywords: vulnerability, milieu therapists, mental health services, caring and therapeutic relationships, threat to professional integrity
Introduction
Milieu therapists’ relationships with patients with severe mental illness (SMI) are viewed as challenging and sometimes threatening,1 because mental illness is a condition that interferes with the individual’s cognitive, emotional, and social abilities. Pursuant to Kottler,2 the concept of challenging behavior is used to describe behavior characterized as manipulating, ignoring traditional social borders, irresponsible, captious, low in impulse control, and self-injurious. Such behavior might often complicate communication and milieu therapists’ and patients’ ability to establish a mutual understanding,3 which is an important basis of the therapeutic relationship.1 In addition, the relationship itself might be experienced as vulnerable. This study focuses on milieu therapists’ (nurses, social workers, and social educators) experience of their own vulnerability in interaction with patients in mental health services.
Milieu therapy as an activity-based and relational form of treatment
Health professionals with the title of milieu therapists in Norway undergo 3 years of training, and some complete an additional year of specialized education or a 2-year master’s degree. Milieu therapy, which originated in the “therapeutic society”,4 is an activity-oriented treatment directed toward the development of cognitive, social, and practical skills to learn coping mechanisms for living in society5 (eg, meals, personal hygiene, balance between rest and activities, social training, school and work conditions). In addition, milieu therapists’ relational competence has been emphasized as important. Such competence refers to what occurs in the interplay between the patients and the milieu therapists, eg, in their professional role, milieu therapists may mirror the patient’s behavior in an acknowledging manner, and consider their own reaction to the interplay.1,6,7
The literature regarding how health professionals in general are affected by their patients in individual therapy is extensive, and countertransference reaction is a well-known concept referring to professionals’ emotional reactions to their patients.8 However, international research on milieu therapists’ vulnerability in their daily close activity-based relational encounters seems to be scarce, particularly compared with similar research in other disciplines.9 Elucidating vulnerability from the milieu therapist’s perspective might contribute to extending our knowledge about their vulnerability and the dynamics of the interaction between patients in mental health services and expertise in building caring and therapeutic relationships.
Vulnerability in literature and research
Vulnerability has been linked to various vulnerable population groups and disease groups at risk of developing poor physical and mental and/or social health, former mental health patients, and professionals who provide care to those patients.10,11 Vulnerability is a general individual human condition.11,12 All people experience vulnerability, but they experience it in different ways and during different periods of life.13 Vulnerability must therefore be viewed as developing along a dynamic continuum, because it may change according to specific challenging situations, and may develop over time.14
The concept of vulnerability comes from the Latin word vulnerabilis, which means being susceptible to harm. The state of vulnerability is presented as exposure to or susceptibility to physical injury, emotional violation, attacks, and/or criticism.15 Kottow16 made an interesting distinction between types of vulnerability, marking the difference between being intact but fragile (vulnerable) and being injured and predisposed to compounded additional harm (susceptible). The possible harming effects might be strong or mild, and have internal mental and bodily influences and external social and physical influences as well.9 When the influences are negative, the consequences might be experienced as a risk of being internally or externally harmed or experiencing a loss. When experienced as positive, vulnerability can represent an opportunity for growth.15
Carel10 suggested that vulnerability plays a significant role in the interaction between nursing staff and their patients. She claimed that staff, through witnessing pain, illness, loss, anger, anxiety, and grief, adopted a kind of vulnerability within themselves. In this article, which focuses on milieu therapists’ perspective of vulnerability, we rely especially on the work of Spiers,11 who described individual vulnerability as the person’s experience of exposure to harm through challenges to his or her integrity, and the strategies that the person uses to protect himself or herself, independently or through support from others. The influences can be multidimensional, complex, and cumulative.
We found some empirical studies focusing on vulnerability from milieu therapists’ perspective in mental health care. While Horwitz17 showed that social workers may experience psychological trauma as a result of their work with children, Hem and Heggen18 presented nurses’ experience of vulnerability as a result of contradictory demands in different roles. Vulnerability can be a constructive element in the therapist’s relationship with their patients, but might also lead to a feeling of having shortcomings according to their professional nursing standard. In a study conducted in a multiprofessional context, including mental health, Thorup et al19 illustrated how mental health nurses’ life experiences of vulnerability and suffering affected their ethical awareness. Vulnerability might be hidden, sensitive, and experienced “as a knot in the stomach”, a revelation, or leading to “blind spots”.14 In addition, Larsen and Terkelsen20 found that professionals’ vulnerability was expressed through descriptions of feelings of guilt about their inability to provide good care. Moen and Larsen21 claimed that distance in the professional–patient relationship might be extended if nurses did not share their own experiences of vulnerability. Showing respect and ensuring equality in the professional–patient relationship were described as important qualities in being open and authentic or in tune. In several studies, nurses’ own vulnerability was presented as positive, in that it gives the nurses courage to help patients face their vulnerability. To sum up, the research literature illustrates that professionals experience vulnerability in different ways. Negative aspects of being at risk elicited unpleasant feelings, such as guilt and trauma, but some positive aspects, such as increased awareness of the patient’s situation, were also found. When professionals were more reflective, and had the courage to act differently and more creatively, the relationship was strengthened.
Aim
The aim of this project was to study milieu therapists’ experiences of their own vulnerability in interaction with patients in mental health services.
Materials and methods
In accordance with the purpose of this study to investigate human experiences, we chose a hermeneutic phenomenological approach. The data-collection method was focus-group interviews. This method is considered to be an efficient and flexible means of gathering qualitative data, and to be especially suitable for exploring a particular phenomenon.22,23 To initiate the conversation about the phenomenon, we used a vignette describing a challenging professional relationship at the start of two of the interviews, because we thought that this theme would be difficult for participants to discuss in a group. The vignette represented a real typical situation observed in practice that we considered not involving a high level of risk.1 Vignettes can be used in studies that aim to reveal the informants’ opinions, assumptions, and judgments.24–26
Vignette: “The story of Astrid and an outside walk”
Astrid, diagnosed with bipolar disorder (manic–depressive condition), has been hospitalized many times in the same acute ward, in the seclusion unit. Her condition is characterized by very high activity, many wishes at the same time, and angry and critical views of treatment and the system. An important part of the treatment is walking tours in the environment outside the ward. This story is about such a walk. The moment she and the nurse come out, Astrid starts to run at full speed along the walkway, shouting that she is only going to the end, and then will turn. The nurse follows, but Astrid, the patient, has a slightly jerky run: accelerating and stopping, and then speeding up again. The nurse suddenly shouts out: “If you do this, you will not be allowed to go out more today!” Astrid continues to run, as she reiterates that she is only going to the end of the road. One of the staff members, who has observed the scene, opens the window and yells, while laughing: “Do you need help with the running?” At the end, Astrid turns and comes back. When they meet, the nurse says humorously: “You certainly gave me good exercise today!” Astrid states without a smile: “I was just going off to the end”. She moves full speed ahead into the ward and her room, and slams the door sharply behind her.1
However, based on the transcripts of the first two interviews, we determined that we used too much time to talk about the vignette. In the third interview, the moderator thus chose to start directly with the informants’ practical experiences. Since in both cases, vulnerability seemed to be a relevant and meaningful theme to elaborate on, we assessed that using the vignette did not make a significant difference in the focus groups.
Informants
The director of the study of a part-time master’s in mental health program recruited the informants purposively. Eighteen students of different professions within mental health care were invited. The 13 students (eight nurses, three social workers, two social educators) provided written consent to participate, and had experience from community and specialized mental health services (2–8 years) (Table 1). Because they were part-time students, they all worked in mental health services during their studies.
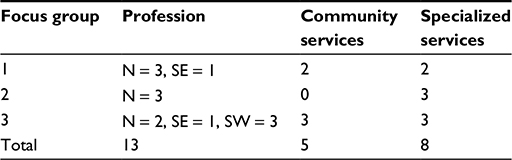 | Table 1 Characteristics of the informants Abbreviations: N, nurse; SW, social worker; SE, social educator. |
Data collection
The participants were divided into three groups (three to six students in each group). All focus-group interviews, which took place in 2013–2014, were 1.5 hours in duration. The interviews were audiotaped and transcribed verbatim. Typical questions/requests were: “How can we understand vulnerability from the health professionals’ perspective, and in what situations might they be vulnerable?” and “Tell us about a situation in which you interacted with a patient and felt vulnerable”. Follow-up questions were asked for the purpose of clarification and to encourage exploration.
Data analysis
The analysis method comprised four analytical steps based on Malterud’s27 systematic text condensation: to obtain a comprehensive understanding, to identify meaning units, to abstract the contents of the individual meaning units, and to summarize the significance of units. Through this process, we bore the aim of the study in mind and searched for participants’ descriptions of their experience of vulnerability in interactions with their patients.
The analysis started when the research group listened to the audiotapes and read the transcriptions separately to receive a general impression of the whole description and identify preliminary themes associated with vulnerability. According to the definitions of vulnerability and the summary of the research literature, we searched especially for unpleasant experiences (unpleasant emotions) of individually being at risk. At this stage, overall understanding was more important than the details.
Then, the researchers met to summarize their impressions. Based on intuition, some themes, such as vulnerability experienced as unpleasant feelings of being physically and personally harmed, emerged. In the second step, the researchers reread the transcripts separately, took notes, and marked out meaning units line by line. The researchers’ common reflections about these meaning units contributed to extending their understanding, and led to systematization and coding. The development of a matrix addressed the connection between the data and participants in the various focus-group interviews.
The third step involved systematic abstractions of meaning units, and the empirical data were reduced to decontextualized meaning units. The data were organized into thematic code groups across individual participants, and the specific content of the meaning units was reformulated into a general description (Table 2).
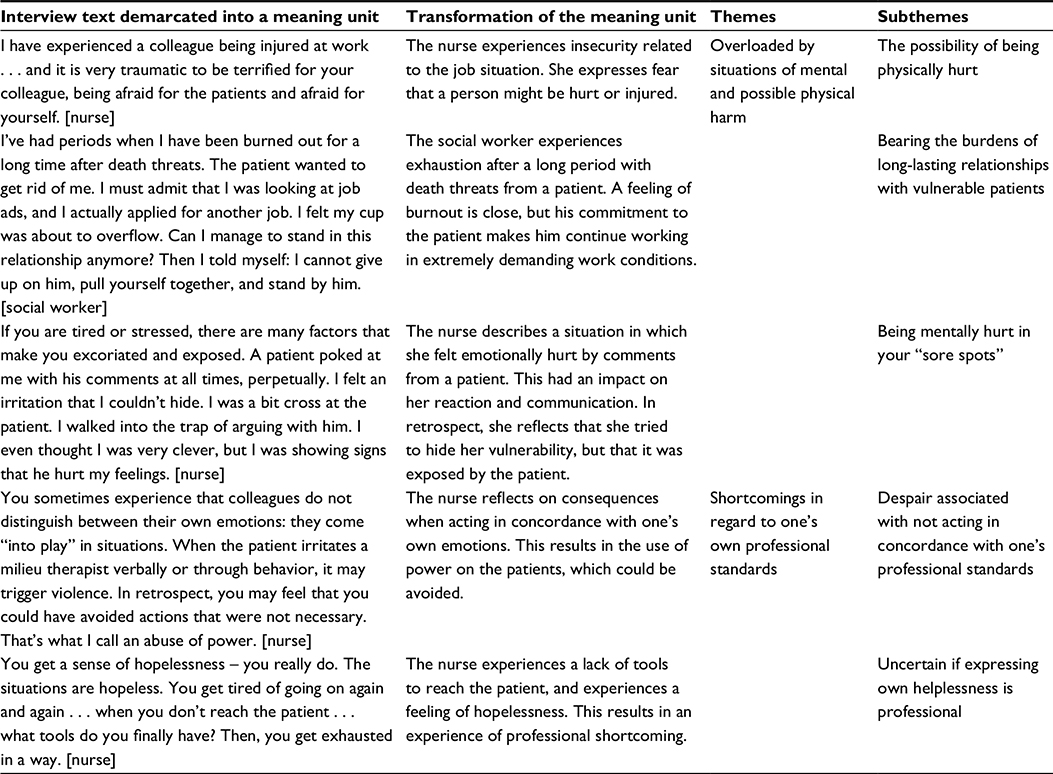 | Table 2 Examples of informants’ perspectives on themes and subthemes |
Ethical considerations
Norwegian Social Science Data Services approved the study and indicated that it was conducted in accordance with ethical guidelines. Informants received written and oral information about the requirements of participation in the study and the depersonalization of the data. The informants gave their written informed consent.
Results
The analysis disclosed two main themes linked to being at risk of harm, which contributed to participants’ negative feelings in their relationships with their patients. They experienced this as difficulty in protecting themselves from unpleasant feelings: 1) “It does something to me”, ie, overloaded by situations of mental and possible physical harm; and 2) shortcomings in regard to one’s own professional standards.
“It does something to me”: overloaded by situations of mental and possible physical harm
This overarching theme contained subthemes of the possibility of being physically hurt, bearing the burdens of long-lasting relationships with vulnerable patients, and being mentally hurt.
The possibility of being physically hurt
Several of the informants described situations in which they were afraid of becoming physically hurt, due to exposure to unexpected violent and aggressive behaviors in clinical settings. Also, because they sometimes underestimated the potential danger in situations with patients, they felt that sometimes they might be exposed to extreme risk of harm. One vivid description of risk of harm is in the following quotation. In this description, an informant explained that she was alone during an initial visit with a patient with a hostile attitude, and was not prepared for it:
I came into a dark room down in the basement. The patient appeared disconnected, and reacted with irritation to my questions. Suddenly, he left the room. I felt fear, my thoughts were spinning around, and I was thinking about rumors about professionals being hurt by mentally ill patients . . . and I was thinking: “Why did he leave the room? Was he going to fetch something?” I felt far away from people that might be able to help me.” [social educator]
She expressed a feeling of “being naïve” and felt “trapped in a corner, searching for possibilities to escape”, and thus became especially vulnerable.
Another nurse from the specialized mental health service described that she had witnessed threats directed at colleagues on a weekly basis and colleagues being physically injured. Her retrospective reflection:
One thing is the fear itself, but in retrospect, you get afraid of approaching the patient because he has done something to you. You get afraid of what will happen next time. Will he try to hit you again? Will he injure your colleagues? What kind of condition will the patient be in the next time you meet him? [nurse]
This utterance shows that the experience of being in danger (oneself or others being in danger) lies in the “back of one’s head”, and comes to the fore when one experiences similar situations. Some participants stated that they worked in a constant state of preparedness to protect themselves, in which they felt insecure. They exemplified this by assuring themselves that they carried a phone in their pocket and that the front door was nearby.
Being mentally hurt in your “sore spots”
Generally, the participants described that they felt that some patients could harm them personally in their “sore spots”, which were presented as a part of their personal baggage. These spots were described as, for example, “scars on your body”, influenced by the professionals’ life experiences and as something changeable with regard to their life situation. They reported that the influence of their personal history, their personal life, was “not only positive”.
When patients had knowledge about and spoke offensively about the professionals’ private and family issues, the latter experienced fear for their family and a feeling of humiliation. They referred to such fear, because they worked and lived in the same community as the patients, making it impossible to protect themselves from patients’ gaining knowledge about their private lives.
They know everything about me, what car I have, how old my kids are. It is difficult to protect myself from it. [social educator]
They experienced the patients as more “loose-tongued” than ordinary, and the insecurity that they felt (whether they could trust the patients or not) served as the background for the feeling of risk.
A number of informants expressed the view that some patients seemed to sense their “vulnerable spots” quickly and make offensive comments, eg, about their weight, appearance, spouses, children, and ethnicity. One of them told a story in which a patient from the same community identified him. He could never forget the abusive comments that this patient made about his wife. Because this happened after a situation in which limits were set for the patients through corrections and boundaries, he interpreted the act as an act of revenge.
Another gave an example from a meal situation:
I was asking the patient: “What do you want?” Then the patient bent toward me and said quietly: “I fancy your daughter.” It was a trigger and a torturous situation for me. [nurse]
The nurse felt vulnerable because the patient could take revenge through attacking his daughter, and felt that this experience increased his vulnerability of being at risk.
The following quote from a nurse served as another example of a patient’s comment:
“You’ve put on weight. Do you eat cake every day?” I sat and listened. It was true, I had filled out. The comment hurt, really. [nurse]
Another informant from a foreign culture expressed experiencing daily hateful comments based on race and color. This was described as hard to dispose, because of “your own personal luggage”. In such a condition, the milieu therapists were more susceptible to patients’ comments, and it could be easier for the patient to “reach into the core of sore spots that lay there and took place”, as one of the nurses expressed. Their responses in such situations of being at risk could be a quickened pulse, change in body language, change in the voice, heavily swallowing, sweating, and blushing.
However, another reflected on the need for the milieu therapist to be aware of the patient’s own vulnerability and disease in such situations:
It is important to keep in mind that the patients are ill, even if you have a good relationship and you are showing each other confidence. Something might happen tomorrow that might change the relationship. The symptom pressure can become so high that they fail to control themselves . . . not because they are mean, but because the symptoms become unmanageable for them. [nurse]
We interpret this expression as a professional understanding that patients’ vulnerability affects their behavior, and that unanticipated patient behaviors might have an impact on the relationship itself.
Bearing the burdens of long-lasting relationships with vulnerable patients
Informants described that long-lasting relationships involving mental and physical risks made them exposed to patients’ pain, impoliteness, rudeness, and aggressive behavior. Some struggled with keeping sufficient distance from the patient’s situation, and failed to put the pain away. They wanted to behave in a therapeutic and professional manner, but stated that it became “too much sometimes to carry all these stories”. They felt powerless.
However, one participant reported that despite feelings of exhaustion and burnout, he had the following “mantra”:
I have had periods when I have been burned out for a long time after death threats. The patients wanted to get rid of me. I must admit that I was looking at job ads, and I actually applied for another job. I felt my cup was about to overflow. Can I manage to stand in this relationship anymore? Then I told myself: “I cannot give up on him; pull yourself together and stand by him”. [social worker]
Long-lasting relationships made the professionals feel responsible for the patients when they were off duty as well. One participant provided an example. She had met a patient by coincidence and offered him a short ride in her car. She knew that the patient was having a difficult time, and she wanted to help him. During the ride, the patient got physically restless and behaved in a way that made her worried. She pulled her car over by the roadside, and said to him: “This is absolutely terrible. You can’t have it this way. I understand that you are very afraid.”
She saw that the patient was suffering and took responsibility, even though she was off duty. She spent the whole day with this psychotic patient. This led to a positive experience of a strong relationship with the patient based on trust and confidence.
Others described inexplicable bonds between the professional and the patient, eg, “becoming too close” to the patients, which had a burdensome impact on them. In particular, professionals in the community said that they had no opportunity to withdraw from such a professional–patient relationship. They described this feeling as becoming trapped because they were the “only one in the patient’s life”. The professional–patient relationship was so tight because no one else took responsibility for the patient in the professional’s absence. One participant described this as: “Sometimes, I feel the patient is like my name, which means he is my responsibility”. Therefore, time off duty was used to handle work experiences.
In such close relationships, the professionals felt a need to share their own experiences with others, but client confidentiality and promises to the patient limited what they could discuss with other professionals. They violated such restrictions to prevent “burning the candle at both ends”. However, they also expressed that breaking the confidentiality was an ethical dilemma for them.
Shortcomings in regard to one’s own professional standards
Despair associated with not acting in concordance with one’s professional standards
The informants expressed the feeling of being in a dilemma when institutional guidelines or house rules did not correspond with their ethical standards. Some exemplified this when acting against promptings of one’s conscience in situations using restraint with patients. This led to feelings of shortcoming and despair.
When experiencing a “lack of control” in situations, some participants described themselves as being unprofessional. Experiencing situations as chaotic led to a feeling of “handling too much and being stressed out”. Therefore the situations could become suboptimal, either for patients or for colleagues. Working under such conditions, the professionals’ own feelings could dominate their interaction with patients and lead to different reactions, eg, “pulling away”, keeping a distance from the patients, and not showing their more personal side. Other professionals stated that to retain control, they acted on the offensive by first trusting the patient and then chose to execute restraint. This ambivalence resulted in a feeling of despair, because it violated their caring standards:
You get a sense of hopelessness, you really do. What tools do you finally have? You get exhausted. [nurse]
Others stated that despite providing good care in accordance with their own standards, they had experienced that the patients mistrusted their good intentions, which led to a feeling of humiliation. One nurse presented an example about a situation in which she felt she interacted with a patient in her best professional manner, but was shocked when the patient called her “an actress”. She experienced a feeling of being cursed, and anger came over her:
I know he’s sick, but right there: how much should one really endure? It is not advisable to take it personally, but I actually did – it’s wrong. I should have acted more professional. [nurse]
In such situations, a feeling of powerlessness dominated the milieu therapists, and they felt unprepared to respond to the patients in a proper manner. They felt vulnerable when feeling that they had displayed shortcomings, as threats to their professional standards, to patients and colleagues. They illustrated this through examples of being devalued by patients and colleagues and experiencing feelings of being humiliated, feelings of dejection, shame, guilt, and powerlessness when acting “unprofessionally”. Acting unprofessionally was often related to situations in which they described insecurity regarding how to handle the situation, eg, a lack of professional competence and skill.
Uncertain about whether expressing own helplessness is professional
The informants had all experienced situations in which they were scared, helpless, and threatened. Some expressed that when they behaved in an honest manner and admitted their own anxiety, this had an impact on the situation and their relationship with the patient:
I’ve been in situations where I’ve been threatened with sharp objects. In one situation, I burst out: “Now, I get scared.” Then the patient answered: “Oh, that was not my intention”. [nurse]
Through expressing her own feelings of being scared, she experienced a de-escalation of the threatening situation. However, the informants had both positive and negative experiences of “mirroring” patient reactions, eg, reflecting what they thought the patient was feeling. Mirroring patients through providing direct feedback could either de-escalate or escalate the situation. The timing of mirroring the responses was thus crucial:
I must reflect whether he is angry or happy. The timing is crucial. When he is agitated, it is like adding fuel to the fire. There is a delicate balance. [nurse]
Another nurse spoke about a situation in which she feared a patient, that ended positively. To deal with her insecurity, she offered the patient a mountain walk:
I remember very well that I went up to the mountain and thought this is a completely surreal situation. I am walking on the mountain together with the person who I fear the most. On the way down, we shared our experiences from the trip. We talked about everything all the way down. We’d had a very nice experience together . . . it was a good ending. [nurse]
In this situation, she confronted her own insecurity. She overcame her fear, which strengthened her as a nurse and she became more confident in her professional role through a mutual, shared experience.
However, several informants felt as though they were acting unprofessionally when they revealed a personal side, eg, fear as a sign of insecurity. They believed that professionals should behave as secure and trustworthy carers of patients.
Summing up
The milieu therapists mainly discussed their experiences of vulnerability to negative feelings arising from challenging work conditions, such as exceptional patient behavior combined with their own personal sensitivities. Sometimes, they experienced a close relationship with these patients as life-threatening, and referred to the possibility of underestimating the potential of danger. In some cases, the professionals experienced these conditions, together with being emotionally close to patients or alone in extremely close interactions, as “too much”. Quite often, they also felt helpless with regard to how to handle a challenging and life-threatening situation in a satisfactory and professional manner, due to their lack of skills and insecurity about professionalism. Altogether, this led to an overload of negative feelings and perceived shortcomings in regard to their ideals of being a good milieu therapist. Over time, this could result in burnout for some therapists.
Due to these work conditions, milieu therapists are constantly prepared to handle challenging situations, which serves as a strategy for protecting themselves from possible harm. Self-protection might lead them to distance themselves from a caring relationship with the patients. However, the positive experience of giving voice to either the patients’ or their own vulnerability is an example of vulnerability as a strength in developing a therapeutic relationship.
Discussion
The main finding of this group of milieu therapists’ vulnerability illuminates, in accordance with Purdy’s15 definition, an openness to the environment that exposes one to various risks of harm, experienced as mental and physical threats. Threats were manifested in different ways, both personally (eg, toward themselves and their family), and professionally (eg, being a good carer and the experiences of difficulties in protecting themselves from harm). We interpret these conditions as threats to both their personal and professional integrity, which corresponds with Spiers’s11 definitions of individual vulnerability. Likewise, Spiers11 presented vulnerability as the extent to which a person is able to protect himself or herself from harm. In line with Carel,10 this shows that a milieu therapist in daily close relationships with this patient group seems to be more than ordinarily vulnerable. In the following sections, we highlight these aspects.
More than ordinarily vulnerable
The patients with SMI were often experienced as unpredictable and possibly violent, and the milieu therapists never knew what mental state they were in, eg, when they visited them at home. Situations could quickly change without warning. In community-based service especially, milieu therapists were constantly in a state of readiness for self-protection against being physically hurt. Similar experiences were described in the specialized services, but the milieu therapists could mostly rely on support from the staff in these contexts. Protection strategies that they used in the community-based services included ensuring that their mobile phone was nearby, locating themselves closely to the front door, and in some situations physically withdrawing from the patients. Such strategies were also described by Moen and Larsen.21 In the literature, violence and threats in mental health services are presented as a serious and growing problem.28,29 Moylan et al30 found that female mental health nurses expected violence as a part of their job, but questioned their competence in managing violence. When there is a discrepancy between external demands and the resources that the individual has to manage situations, the individual is exposed to risk of harm.31 Self-protection might then become the dominant strategy.
These findings are in accordance with the work of Sellman,32 who described individuals as having varying capacities to reduce their vulnerability. He related these capacities to three different risk levels: 1) individuals who can protect themselves from harm, 2) individuals who can rely on others to receive protection, and 3) individuals who are at risk in situations in which protection is not possible. Sellman32 defined individuals at level 3 as more than ordinarily vulnerable. We found that the informants’ encounters with patients with SMI occurred on all Sellman’s levels, but the milieu therapists in the community setting seemed to be extremely vulnerable because they were alone and unprotected in situations with possibly dangerous patients.
Furthermore, we highlight examples that participants provided regarding unpredictable attacks on “one’s sore spots”, which some informants viewed as revenge, eg, thus blaming the patients for a kind of evil,1 which “put them out of action”. Others reflected that such behavior could be an expression of patients’ vulnerability. We question whether this difference in understanding patients is a matter of variation in knowledge and understanding of mental illness, combined with personal vulnerability, such as “sore spots”. Being skilled in therapeutic actions and having insight into one’s own vulnerability might function as protection against getting hurt. The informants reported that “expressing their own feelings” could sometimes lead to a more positive relationship, supporting this interpretation, which has also been described in the literature and research.33,34 If milieu therapists lack the professional knowledge and skills to manage challenging situations in a therapeutic and safe manner, they may be exposed to being more than ordinarily vulnerable. The character of unexpectedness in their work conditions places them in situations in which they must constantly prepare themselves to manage difficult behavior, which is an example of the consequences of the cumulative effect of vulnerability.11 This is also in accordance with Kottow’s16 description of susceptibility as being injured and predisposed to additional harm. Because of this, milieu therapists might be prejudiced and thus interpret the situation as more harmful than the patients intended. This might lead to extensive use of self-protection strategies, eg, self-defense mechanisms and emotional withdrawal by distancing oneself from the patient.19,21,34 Over time, such working conditions result in emotional exhaustion and burnout, as supported by a study conducted by Acker.35 In addition, constantly working with a bad conscience of shortcomings might result in compassion fatigue.36,37 Therefore, professionals distance themselves from patient involvement they have no remaining energy to display therapeutic empathy for the patients’ struggles, eg, using mirroring as a therapeutic approach.
Coherence between vulnerability and inauthenticity
A main result of this study, supported by international research, is that vulnerability is a hindrance to acting as a sensitive, caring, and therapeutic professional. A protective attitude made nurses “invulnerable”, but at the same time they had to give up their sensitivity38,39 and authentic life as a caring person.40,41
Vulnerability is described as a quality attributed to human life in general.11,12 Being authentic as a fellow human is thus an important aspect of being personal.38,39 Thorup et al19 gave support to this notion. They found that personal and professional integrity referred to being a unique person with a distinctive identity and self-understanding. Managing one’s own emotions when faced with the patient’s suffering is then of great therapeutic importance. Furthermore, Daniel38 claimed that vulnerability enables a sincere commitment to the professional–patient relationship, but milieu therapists must accept their own vulnerability and use the insight that vulnerability gives as a tool in a challenging caring and therapeutic relationship. Recognition of this aspect of the role and insight into the complexity of it can strengthen the professional–patient relationship and the professional’s self-esteem. Research has shown that being open and in tune gave professionals an opportunity to identify themselves with the patients’ behavior and problems. When mirroring their understanding in a reflecting way in their communication with patients, professionals’ solutions became more creative,20,42 and de-escalation of patients’ challenging behavior could take place.6,34 We also found that when the milieu therapists gave voice to their perceived personal infringement, they experienced a positive change in the relationship: vulnerability then became strength. Although they described themselves as unprofessional, similar to Hem and Heggen’s18 findings, when milieu therapists “put a lid on” their own vulnerability, their job became “too much to bear”. Balance in threatening situations can be viewed as a dichotomy between therapeutic professionalism with expertise, on the one hand, and being human, on the other hand, which might be felt as an unattainable ideal in situations of extreme insecurity.
Increased vulnerability because of misunderstanding of professionalism of caring
The professionals in this study felt that their shortcomings in relationships with patients with SMI became a threat to their identity as individuals offering professional quality services and to their professional integrity. They felt unprepared to handle challenging and threatening situations professionally. The feeling of guilt described by Larsen and Terkelsen20 might increase the threat. In addition, some of the informants felt an obligation to bear the burden of the patients’ vulnerability: “over a long period, being the only person for the patient”. These are examples of altruistic or unconditional care.
The literature presents professional identity as the integration of personal values, understanding, and motivations regarding being professional, where knowledge, skills, and attitudes, become internalized as part of professional socialization.43 The informants’ statements can be interpreted as reflecting a lack of integration of personal ideal values of good caring and integration of professional knowledge and skills, making these professionals more than ordinarily vulnerable.
It seems as though the professionals perceived professionalism as separating their private life or feelings from their professional role, instead of using their private life as a therapeutic attitude and skill. The current psychiatric nursing curriculum places an emphasis on reciprocity and openness, but instructs health care personnel to refrain from sharing their personal problems.44 Therefore, professionals’ assumptions of professionalism might primarily be linked to a theoretical ideal regarding approaching disease and suffering. By excluding their own subjectivity, their self-understanding of being professional while building on equality as humans will be difficult to execute in practice. We question whether there is a misconception of what it is to be a professional therapeutic carer in mental health. If so, this misunderstanding increases professionals’ vulnerability. New theories about mature care give support to such coherence.
Recently, Pettersen,45 a Norwegian philosopher, criticized the fact that there is no agreement regarding the definition of the concept of care as an altruistic practice: “Care is seen as selfless and compassionate focus on what is the concrete others’ immediate needs”.45 Pettersen contrasted mature care to Løgstrup’s ethical demands of caring for another’s life as one-sided and not reciprocal. Løgstrup’s46 perspective has had a great influence on Scandinavian nursing education. Based on Gilligan’s47 concept of mature care, Petterson45 developed a theory that defined mature care as a relational activity and that considered reciprocity to be a core element. Reciprocity implies that persons involved in a caring relationship have equal worth and a need to practice self-care, which is also a therapeutic ideal. In this theory and in milieu therapy, reflection and dialogue with the patients as an authentic person (eg, the carer reflects his or her own feelings and needs in the caring situation), were highlighted as important skills. Furthermore, Petterson45 makes important distinctions between different types of care, eg, informal care provided in families and professional care, such as nursing care, which have different aims and a different knowledge base.
Increased attention to conflicting aspects of professionalism must be discussed and developed in both clinical and educational settings that pertain to professional practice. This could lead to a better understanding of professionals’ perception of their own vulnerability in the professional–patient relationship.48 Research shows that developing professional therapeutic skills in a dialogue with patients with SMI, based on self-reflection, and reflecting patients’ behavior and possible experiences, are tools that strengthen the milieu therapist’s professionalism.1,6,7,34
Conclusion
Based on this research, we determine that vulnerability is of interest across multiple disciplines and is of relevance for knowledge development in higher education and mental health services. Extended knowledge and understanding about health professionals’ vulnerability might strengthen their personal and professional integrity in professional practice in mental health services, which is of great importance for the therapeutic treatment of this vulnerable patient group. This study contributes some new knowledge, especially about milieu therapists’ vulnerability in the mental health context, but the findings must be considered in light of the fact that the study included a limited group of health professionals from a limited geographical area in Norway.
The degree to which the milieu therapists felt vulnerability illustrates the great need for extended practice-relevant professional knowledge and skills, which requires practical training during both education and in the clinical setting.6 In addition, supervision in practice, especially with a focus on individual vulnerability in concrete practice, is crucial. Research shows that milieu therapists need to translate theory into concrete practice. In an action-research project on developing concrete therapeutic knowledge in practice, practical exercises (through reflection on concrete situations in practice), role-play of new skills, and theory courses led to more professional skilled communication.1,40,41 Additionally, the responsibility of the leaders and highly educated professionals is to focus on building a culture where the openness of being vulnerable as milieu therapists is an accepted theme to discuss, and discussing how to apply it in professional care work. Further research is needed about the outcomes of implementing professional knowledge and skills development related to milieu therapists’ vulnerability in the clinical area. We recommend that community health services give greater attention to security in milieu therapists’ working conditions by evaluating how community health care services are organized, and improving assessments of potentially dangerous patients.49
Acknowledgment
The informants and the manager of the master’s program in mental health are gratefully acknowledged.
Disclosure
The authors report no conflicts of interest in this work.
References
Vatne S. Korrigere og Anerkjenne: Relasjonens Betydning i Miljøterapi. [Correcting and acknowledging: the significance of relationships in milieu therapy]. Oslo: Gyldendal Akademisk; 2006. | ||
Kottler JA. On Being a Therapist. San Francisco: Jossey-Bass; 1993. | ||
Procter N, Hammer HP, McGarry D, Wilson RL, Froggatt T. Mental Health: A Person-Centred Approach. Cambridge: Cambridge University Press; 2014. | ||
Jones M. The Therapeutic Community. New York: Basic Books; 1953. | ||
Gunderson J. A reevaluation of milieu therapy for nonchronic schizophrenic patients. Schizophr Bull. 1980;6(1):64–69. | ||
Vatne S, Hoem E. Acknowledging communication: a milieu-therapeutic approach in mental health care. J Adv Nurs. 2008;61(6):690–698. | ||
Vatne S, Bjørnerem H, Hoem E. Development of Professional Knowledge in Action: Experiences from an Action Science Design Focusing on Acknowledging Communication in mental health. Molde, Norway: Høgskolen i Molde; 2009. | ||
Rossberg JI, Karterud S, Pedersen G, Friis S. An empirical study of countertransference reactions toward patients with personality disorders. Compr Psychiatry. 2007;48(3):225–230. | ||
Perraud S, Delaney KR, Carlson-Sabelli L, Johnson ME, Shephard R, Paun O. Advanced practice psychiatric mental health nursing, finding our core: the therapeutic relationship in 21st century. Perspect Psychiatr Care. 2006;42(2):215–226. | ||
Carel C. A reply to “Towards an understanding of nursing as a response to human vulnerability” by Derek Sellman: vulnerability and illness. Nurs Philos. 2009;10(3):214–219. | ||
Spiers J. New perspectives on vulnerability using emic and etic approaches. J Adv Nurs. 2000;31(3):715–721. | ||
Gjengedal E, Ekra E, Hol H, et al. Vulnerability in health care- reflections on encounters in everyday practice. Nurs Philos. 2013;14(2):127–138. | ||
Henriksen JO, Vetlesen AJ. Nærhet og Distanse: Grunnlag, Verdier og Etiske Teorier i Arbeid med Mennesker. [Proximity and distance: the basis, values and ethical theories of working with people]. Oslo: Gyldendal Akademisk; 2000. | ||
Rogers AC. Vulnerability, health and health care. J Adv Nurs. 1997;26(1):65–72. | ||
Purdy IB. Vulnerable: a concept analysis. Nurs Forum. 2004;39(4):25–33. | ||
Kottow MH. The vulnerable and the susceptible. Bioethics. 2003;17(5–6):460–471. | ||
Horwitz M. Social worker trauma: building resilience in child protection social workers. Smith Coll Stud Soc Work. 1998;68(3):363–377. | ||
Hem MH, Heggen K. Being professional and being human: one nurse’s relationship with a psychiatric patient. J Adv Nurs. 2003;43(1):101–108. | ||
Thorup CB, Rundqvist E, Roberts C, Delmar C. Care as a matter of courage: vulnerability, suffering and ethical formation in nursing care. Scand J Caring Sci. 2012;26(3):427–435. | ||
Larsen IB, Terkelsen TB. Coercion in a locked psychiatric ward: perspectives of patients and staff. Nurs Ethics. 2014;21(4):426–436. | ||
Moen EA, Larsen IB. Her er det faktisk hele meg som er på jobb: om å bruke erfaringer med egen psykisk helse i profesjonelle relasjoner. [All of me is actually present at work: using the experiences of one`s own mental health in professional relationships]. Tidsskr Psykisk Helsearbeid. 2013;10(1):15–24. | ||
Knodel J. The design and analysis of focus group studies in social science research: a practical approach. In: Morgan, DL, editor. Successful Focus Groups: Advancing the State of the Art. Newbury Park (CA): Sage; 1993:35–50. | ||
Plummer-D’Amato P. Focus group methodology – part 1: considerations for design. Int J Ther Rehabil. 2008;15(2):69–73. | ||
Jegerby U. Att Bedöma en Social Situation: Tillämpning av Vinjettmetoden. [To interpret a social situation . Application of the vignette method]. Stockholm: Socialstyrelsen; 2007. | ||
Barter C, Renold E. “I wanna tell you a story”: exploring the application of vignettes in qualitative research with children and young people. Int J Social Res Methodol. 2000;3(4):307–323. | ||
Malterud K. Fokusgrupper som Forskningsmetode for Medisin og Helsefag. [Focus groups as research method for medical and health education]. Oslo: Universitetsforlaget; 2012. | ||
Malterud K. Kvalitative Metoder i Medisinsk Forskning: En Innføring. [Qualitative methods in medical research: a prime]. 3rd ed. Oslo: Universitetsforlaget; 2011. | ||
Nolan P, Dallender J, Soares J, Thomsen S, Arnetz B. Violence in mental health care: the experiences of mental health nurses and psychiatrists. J Adv Nurs. 1999;30(4):934–941. | ||
Moxness Ø. Velkommen inn! Tenker Helsedirekotratet mer på pasienten enn den ansatte i psykisk helsevern? 2014. Available from: https://sykepleien.no/2014/02/velkommen-inn. Accessed May 30, 2016. | ||
Moylan LB, Cullinan MB, Kimpel JE. Differences in male and female nurses’ responses to physical assault by psychiatric patients: a supplemental finding of a mixed-methods study. J Psychosoc Nurs Ment Health Serv. 2014;12;52(12):36–42. | ||
Lind MS. Sårbarhed. [Vulnerability]. Nord Sygeplejeforskning. 2012;2(1):56–63. | ||
Sellman D. Towards an understanding of nursing as a response to human vulnerability. Nurs Philos. 2005;6(1):2–10. | ||
Schibbye AL. The role of “recognition” in the resolution of a specific interpersonal dilemma. J Phenomenol Psychol. 1993;24(2):175–189. | ||
Vatne S, Fagermoen MS. To correct and to acknowledge: two simultaneous and conflicting perspectives of limit-setting in mental health nursing. J Psychiatr Ment Health Nurs. 2007;14(1):41–48. | ||
Acker GM. The challenges in providing services to clients with mental illness: managed care, burnout and somatic symptoms among social workers. Community Ment Health J. 2010;46(6):591–600. | ||
Ledoux K. Understanding compassion fatigue: understanding compassion. J Adv Nurs. 2015;71(9):2041–2050. | ||
Tuvesson H, Eklund M, Wann-Hansson C. Stress of conscience among psychiatric nursing staff in relation to environmental and individual factors. Nurs Ethics. 2012;19(2):208–219. | ||
Daniel LE. Vulnerability as a key to authenticity. Image J Nurs Sch. 1998;30(2):191–192. | ||
Kirkevold M. Den gamles integritet. [The integrity of the elderly]. In: Kirkevold M, Brodtkorb K, Ranhoff AH, editors. Geriatrisk Sykepleie: God Omsorg til den Gamle Pasienten. Oslo: Gyldendal Akademisk; 2008. | ||
Savage AT, Conrad AB. Vulnerability as a consequence of the neonatal nurse-infant relationship. J Perinat Neonatal Nurs. 1992;6(3):64–75. | ||
Stenbock-Hult B, Sarvimäki A. The meaning of vulnerability to nurses caring for older people. Nurs Ethics. 2011;18(1):31–41. | ||
Malterud K, Fredriksen L, Gjerde MH. When doctors experience their vulnerability as beneficial for the patients: a focus-group study from general practice. Scand J Prim Health Care. 2009;27(2):85–90. | ||
Takase M, Maude P, Manias E. Impact of the perceived public image of nursing on nurses’ work behaviour. J Adv Nurs. 2006;53(3):333–343. | ||
Reamer FG. Boundary Issues and Dual Relationships in the Human Services. 2nd ed. New York: Columbia University Press; 2012. | ||
Pettersen T. Conceptions of care: altruism, feminism, and mature care. Hypatia. 2012;27(2):366–389. | ||
Løgstrup KE. Den etiske fordring. [The ethical demand]. Oslo: Cappelen; 1999. | ||
Gilligan C. In a different voice: psychological theory and women’s development. Cambridge, Mass: Harvard University Press; 1982. | ||
Borg M, Karlsson B. Hjemmet som samarbeidsarena: muligheter og begrensninger i lokalbasert psykisk helsearbeid. [The home as an arena for cooperation- possibilities and limitations in community-based mental health care]. Tidsskr Psykisk Helsearbeid. 2013;10(2):105–114. | ||
Norwegian Directorate of Health. Sammen om Mestring: Veileder i Lokalt Psykisk Helsearbeid og Rusarbeid for Voksne. [Together in coping : A guide to local mental health care and drug awareness for adults. A tool for local communities and specialized health care service]. Oslo: Directorate of Health; 2014:148. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.