")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Feeding Experiences of HIV-Exposed Preterm Infants Among Mothers Living with HIV in Addis Ababa, Ethiopia: A Qualitative Study
Authors Getachew B , Solomon S , Ramet BT, Mezgebu T, Ewnetu DB, MacDonald N
Received 13 August 2021
Accepted for publication 15 October 2021
Published 2 November 2021 Volume 2021:13 Pages 973—981
DOI https://doi.org/10.2147/HIV.S333537
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Biniam Getachew,1,* Semaria Solomon,2,* Blen Teshome Ramet,2 Tirumebet Mezgebu,2 Demelash Bezabih Ewnetu,2 Noni MacDonald3
1Independent Public Health Consultant, Addis Ababa, Ethiopia; 2St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Dalhousie University, Halifax, Nova Scotia, Canada
*These authors contributed equally to this work
Correspondence: Biniam Getachew Addis Ababa, Ethiopia
Tel +251 911 380964
Email [email protected]
Introduction: Providing adequate nutrition to preterm infants who are born to HIV-positive mothers is more challenging due to the mother’s underlying health and nutrition status. The understanding of these issues and active participation of the mothers have a significant role in giving continuous care for HIV-exposed preterm infant. Hence, this study aimed to explore the experience of HIV-positive mothers’ feeding practice of their preterm infants, and health workers to identify barriers and facilitators of feeding HIV-exposed preterm infants.
Methods: A phenomenological qualitative study design was conducted in Addis Ababa, Ethiopia, between May 1, 2016 and March 31, 2017. Mothers who gave birth to HIV-exposed preterm infants at the study sites’ follow-up clinic were traced and invited by the healthcare providers to voluntarily participate in this study. Fifteen in-depth interviews with mothers of HIV-exposed preterm infants and seven key informant interviews with health professionals and policymakers were carried out. The interviews were transcribed and translated and then manually analyzed thematically.
Results: The health education given during antenatal care (ANC) did not consider the feeding practice needs for HIV-exposed preterm infants. Child health status, desire to have a healthy infant, financial constraints and family support were among the influential factors in the feeding practice of HIV-exposed preterm infants mentioned by the study participants. HIV-exposed preterm infant feeding procedure neither has a guideline nor is clearly mentioned in the national HIV guidelines.
Conclusion: The desire to have a healthy infant was a major facilitator for feeding of HIV-exposed premature infants. However, financial constraints majorly limited the option to be only exclusive breastfeeding. This became even more problematic for the mother if the premature infant became ill and could not breastfeed well.
Keywords: HIV/AIDS, HIV-exposed, preterm infant, infant feeding, Ethiopia
Introduction
Proper nutrition in infants is essential for optimal growth, resistance to infection, and neurologic and cognitive development.1,2 This is especially important for preterm infants.3 Providing adequate nutrition to preterm infants born to HIV-positive mothers is more challenging because of the mother’s underlying health and nutrition status.4,5
Infants born alive before 37 weeks of gestation are considered premature.6 Different studies reported that the prevalence of preterm ranges from 9% to 13% in Ethiopia.7–11 A previous study done in six public hospitals in Addis Ababa showed 72% of preterm babies were exclusively breastfed at discharge from the neonatal intensive care unit (NICU).12
A review from several studies established the importance of Highly Active Antiretroviral Therapy (HAART) on minimizing mother-to-child transmission (MTCT) of HIV.13 A systematic and meta-analysis published in 2018 showed 10% of MTCT of HIV in Ethiopia.14 HIV-positive women on HAART during pregnancy, especially if started before or in the first trimester of pregnancy, have a high rate of preterm deliveries.15,16 A cohort study done in the USA showed 19% of HIV-infected pregnant women gave birth to preterm babies.17 In Northwest Ethiopia, a 17% incidence of preterm delivery among HIV-infected mothers was reported.18
Feeding options for HIV-exposed preterm infants include exclusive breast milk, donor expressed breast milk and preterm formula.19 WHO guidelines only recommend replacement formula feeding for HIV-infected mothers when it is completely “acceptable, feasible, affordable, and safe”. If these conditions are not met, mothers are advised to exclusively breastfeed for 6 months of life, introduce appropriate complementary foods thereafter and continue breastfeeding for the first 12 months of life.20,21 As like WHO guideline, the Ethiopian Ministry of Health prevention of mother-to-child transmission (PMTCT) guideline advises counseling HIV-positive pregnant women on the importance of exclusive breastfeeding for the first 6 months of life, followed by supplementation with appropriate complementary feeding for at least 12 months.22 Mixing formula milk and breast milk also increases the risk of MTCT.23
Given the importance of good nutrition for the longer-term health and well-being of premature infants and the added goal of decreasing HIV risk to infants, maternal decisions on infant feeding practices have a big impact. Unfortunately, there is a paucity of evidence documenting the feeding experience of HIV-exposed preterm infants in Ethiopia. Therefore, the objective of this study was to explore the experience of HIV-positive mothers’ feeding practice of their preterm infants and health workers to identify barriers and facilitators of feeding HIV-exposed preterm infants.
Methods
Study Design, Study Area and Study Period
A phenomenological qualitative study design involved in-depth interviews of HIV-positive mothers and key informant interviews of healthcare providers and policymakers to examine feeding practice of HIV-exposed preterm infants. The study was carried out between May 1, 2016 and March 31, 2017. The study was conducted in Addis Ababa, the capital city of Ethiopia, with the population estimated to be 3.1 million.24 The study was conducted at St. Paul’s Hospital Millennium Medical College (SPHMMC) and Addis Ababa University Medical Faculty – Tikur Anbesa Specialized Hospitals (TASH), two of the biggest referral hospitals in Ethiopia. The two hospitals provide services to more than 5 million population in the city and also serve as a referral point for rural population. SPHMMC provides ANC services for 4000 clients per month on average, while TASH provide more than 1000 ANC services to pregnant women. At SPHMMC, there are 1904 HIV patients on HAART. Since both hospitals are public facilities, most of the clients belong to lower socio-economic group. The hospitals were selected due to the high caseloads of HIV-positive pregnant women.
Study Population and Subject
All HIV-positive mothers who gave birth to live preterm infants during the study period at the designated sites were the cohort from whom the study subjects were selected. The inclusion criteria were mothers who had HIV-exposed preterm infants that were admitted to the NICU, passed through preterm feeding options and practices, had a follow-up at an HIV-exposed infant clinic during the data collection period, needed to have a phone so that they be could contacted for consent and volunteered to participate in the study. The exclusion criteria were women either unable to communicate and pass correct information due to any mental or medical problems (illness) or whose infants had major physical problems. Mothers meeting the inclusion criteria were recruited using purposive sampling. Fifteen mothers of HIV-exposed preterm infants were traced through the follow-up clinic and invited by healthcare providers at the clinic to voluntarily participate in the study. The clinic staff helped to establish a good relationship between data collectors and interviewee by explaining the purpose of the study and emphasizing the importance of explaining what they feel about the services and that all the information was confidential. Those who agreed were contacted by one researcher via phone who obtained informed consent and then the place and time for the interviews were set up. The site for each interview was chosen to be private and agreeable to the mother. Informed consent was also obtained from the 15 key informants; 2 Pediatricians, 3 nurses and 2 officers from MoH (Ethiopia) interviewed from the Ministry of Health. Moreover, the purpose of the study was explained in detail to all interviewees.
Operational Definition
Preterm infant: a neonate born alive before 37 completed weeks of gestation.
HIV-exposed preterm infant: a preterm infant born to mothers living with documented HIV-positive result.
Exclusive breastfeeding: the infant receives only breast milk with in the first 6 months. No other liquids or solids are given – not even water – with the exception of oral rehydration solution, or drops/syrups of vitamins, minerals or medicines.
Data Collection
Prior to the data collection, the researcher had several preparatory meetings to review the data collection techniques and tools. The in-depth and key informant interview guides were developed by the research team based on literature review and expert opinion to ensure the study objectives could be addressed. The key topics included in the tools were about information the mother got during antenatal care about preterm infant feeding, actual experience of preterm infant feeding, and the facilitators and barriers of preterm infant feeding. The tools were pretested on two HIV-positive mothers who gave birth to preterm infant to make sure the tools addressed the objectives. The mothers who participated in the pretest were from another study setting (hospital). In-depth and key informant interviews were conducted using a pre-tested semi-structured open-ended questions probe, after obtaining informed consent from the study participants. In-depth interviews were done with the mothers who had HIV-exposed preterm infant. The face-to-face interviews were conducted by one of the researchers using the local language - Amharic. All interviews were audio-recorded with a voice recorder and the interviewer also took field notes. The duration of interviews ranged from 30 to 90 minutes; however, almost half of the interviews took more than 60 minutes as the researcher allowed participants to continue expressing feelings as they wished. Only one interview was done per day.
Analytic strategies used in the field included a continuous review of field notes in order to check whether or not the research objectives were met, to determine whether new interview questions need to be added, to further research emergent ideas and to decide if the study needed more data, ie, had saturation been reached. The saturation was noted by redundant inputs from newly recruited study participants.
Data Analysis
Preliminary analysis was done manually after each interview (listening to the audio recording and reviewing the field notes). The interviews were then transcribed and translated to English by an external person. The translated transcripts were reviewed and ambiguous portions clarified by repeated listening and re-reading. After complete transcription and translation of the interviews, the data were coded manually by two researchers and using the codes, themes were identified for detailed analysis. When there were differences in translation and coding, a third researcher involved to resolve the differences. Data triangulation among the study participants was part of the data analysis.
Ethical Consideration
Ethical clearance and approval were obtained from the Institutional Review Board (IRB) of St. Paul’s Hospital Millennium Medical College (P.M 23/251). Informed consent was obtained from each study participant, including publication of their response as long as it was anonymized, then the place and time for the interviews were set up to maintain privacy and confidentiality. The identity of the respondents was anonymized for confidentiality. This study was conducted in accordance with the Declaration of Helsinki. All methods were performed in accordance with the relevant guidelines for reporting qualitative studies (COREQ).25
The study was funded by a small grant from Ethiopia-Canada Maternal, Newborn and Child Health Project at the University of Alberta Canada (https://www.ualberta.ca/medicine/about/social-accountability/globalhealth/mnch-projects/ethiopia-mnch/about.html) supported in part by MicroResearch (www.microresearch.ca).
Results
Sociodemographic characteristics of HIV-positive mothers who gave birth to HIV-exposed preterm infants are depicted in Table 1. Two-third of key informants are between 20 and 34 years of age. Six of the study participants were illiterate, and most of them live in urban area. One-third of the mothers who gave birth to HIV-exposed infants were not married and all of them had ANC follow-up.
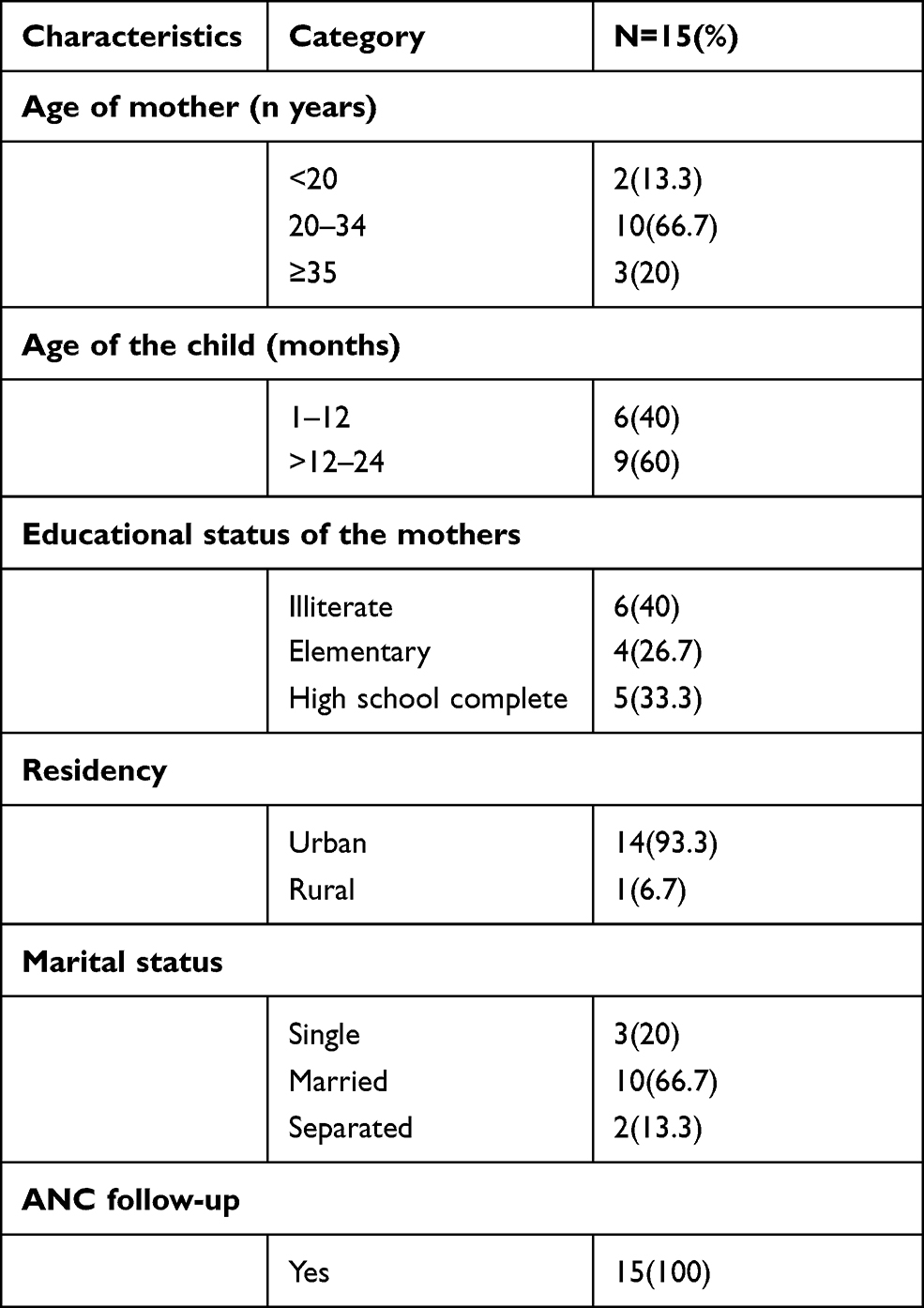 |
Table 1 Demographic Characteristics of HIV-Positive Mothers Who Gave Birth to Preterm Newborn |
The main themes identified were knowledge of MTCT of HIV including the role different feeding practices play, the breastfeeding practices for HIV-exposed preterm infants and factors contributing to the breastfeeding practice for HIV-exposed preterm infants. The coded data were categorized according to the themes and organized based on informants (mothers who have HIV-exposed preterm infants, healthcare providers and officials from MoH).
Knowledge of the Mothers on How HIV Can Affect Their Newborn Child
HIV-infected women knew that the virus might be transmitted from them to their newborn while they were pregnant and after birth.
“I have taken the word of the healthcare providers to prevent the passing of the virus from me (the mother) to the newborn. But if it happens, it is God’s will. If it happens to my child, it is up to God.” HIV-infected woman.
There was a sense of fear among HIV-positive mothers about their newborn’s health status when they became pregnant. For instance, one interviewee said:
“I know my child might or might not have the disease. I pray to God that my child to be free of the disease. I am still worrying about this child since I have been pregnant” HIV infected woman lost her previous child.
Some interviewed mothers had regular antenatal care (ANC) follow-up, but others did not.
“Before pregnancy, I was tested for HIV and it was found that I am positive but I did not have any follow-up. I preferred to go to holy-water. When I did my first ANC visit at 8 months of pregnancy, they (nurses) offered me to test for HIV and it was found positive again. Then I start taking the pill (ART).” Unmarried HIV-infected woman.
Knowledge of HIV Transmission from Mother to Children
Participants mentioned that HIV can be transmitted from the mother to newborn during pregnancy, labor, and breastfeeding. Moreover, they also linked the transmission with the duration of breastfeeding.
“The nurse taught me (the mother) that the disease can be passed on to my child during pregnancy while the baby is inside my belly during delivery and breastfeeding. If I breastfeed my child without feeding another food item for six months then change to other infant food, the child can be healthy.” HIV-infected women and mother of two.
Message Received During Antenatal Care
Participants explained that they had received an important precautionary message to prevent the transmission of HIV from the mother to the newborn at their antenatal visits. Some participants noted that the healthcare providers taught them to take their HIV medication (ART) properly, to give birth at the health facility, to exclusively breastfeed up to 6 months then to quit and switch to other infant food, not to mix feeding, ie, complementary foods with breastfeeding, and to use a condom.
“Yes, they (healthcare providers) taught me (the mother) at the health center that it (HIV) can be passed from mother to child. The nurse advised me that I need to have a proper follow up and to take my pills (ART) on time. They told me to breastfeed only and not to mix something else. But I did not breastfeed him (the baby), the baby was never breastfed. Ohh they also told me to give birth at the hospital.” An HIV-positive mother who has her first birth.
But some stated that health education during ANC was not satisfactory. The healthcare providers at ANC clinic did not mention what the feeding practice should be if the HIV-positive mother might have a preterm infant.
“They (healthcare providers) didn’t teach me well, but I knew it before. They told me the disease can be passed to my child with breastfeeding and while cutting the umbilical cord. Therefore, I didn’t breastfeed. From birth until now the child did not breastfeed. No one has told me how to feed preterm infant before and after I have my child.” A mother who lives with HIV and member of peer educators.
Healthcare providers at the hospital stated that proper health education about feeding practices of HIV-exposed infants have been given during ANC, labor and delivery, and post-natal care but no focus on preterm infants feeding.
“I (healthcare provider) advise all mothers to exclusively breastfeed their HIV-exposed infant until 6 months then quit it and to start formula feeding together with other foods like porridge. But health education does not focus on HIV exposed preterm infants. I (healthcare provider) teach overall HIV exposed infants.” Health care provider at ANC clinic.
Feeding Practice at NICU (Neonatal Intensive Care Unit)
Health care providers were asked about the special care and treatment for HIV-exposed preterm infant and it was reported that regardless of HIV exposure, the care and treatment for all preterm infants were the same. All preterm infants were put on exclusive breastfeeding regardless their HIV-exposed status.
“The feeding practice for preterm infants at NICU is the same whether the newborn had HIV exposure or not. We (health care providers) encourage all mothers to breastfeed exclusively.” Health care provider at NICU.
Admission of the preterm neonate alone (without the accompanying mother) at NICU was mentioned as a rare but difficult challenge faced by the healthcare providers. The healthcare providers did not know the feeding plan of the mother, which makes the management more complicated for them. Another echoed challenge was a decreased breast milk production of the mothers of preterm infants.
“If a preterm infant admitted to NICU without being accompanied by the mothers, by then, we have no idea what was the mothers’ feeding preference which led us (NICU staffs) to more confusion.” Health care provider at NICU.
Feeding Practice by the Mother
Some mothers had exclusively breastfed up to 6 months and then switched to other powder milk and child food as they have been told during ANC follow-up.
“The nurses told me to breastfeed only to the child until six months without mixing other foods then I stopped the breastfeeding and started giving him additional foods like gruel and thin (liquid-like) porridge; that was what I did. And to let the child drink the milk using a cup, not a bottle.” A mother of HIV-exposed preterm infant.
In some cases, depending on the mothers’ health condition, the exclusive breastfeeding was switched to formula feeding even before 6 months.
“I started only breastfeeding on the 3rd day after birth, then I got sick after 4 months then I started powder milk (quit breastfeeding) for my child.” A mother of HIV-exposed preterm infant.
Most of the interviewed mothers had a low economic status which presented challenges for feeding their child after 6 months. The mothers felt their babies needed more supplementary foods, but they were unable to provide this.
“I know they (her twin children) need more food like egg and different foods but my shortage of money stops me to feed them food like that” A mother of twin HIV-exposed preterm infants.
The 2017 National PMTCT Guideline
Feeding of HIV-exposed preterm infants did not have a specific or separate guideline, rather it was part of the 2017 national PMTCT guideline. One MoH (Ethiopia) officers stated the 2017 guideline indicated exclusive breastfeeding until 6 months then to continue breastfeeding together with complementary feeding until 18 months.
“The feeding practice to all HIV exposed infants are six months of exclusive breastfeeding then continue the breastfeeding until 18 months together with complementary feeding. But recently, the MoH is developing a guideline to minimize the breastfeeding period to 12 months.” An officer at MoH.
Others stated that there was no specific guideline either for the HIV-exposed infants or preterm infants feeding practice or procedure in Ethiopia, rather it was part of comprehensive and integrated prevention of MTCT of HIV guideline. MoH (Ethiopia) officer mentioned
“There is no special feeding approach that has been implemented for HIV exposed preterm infant in Ethiopia but it was part of the national comprehensive and integrated prevention of mother-to-child transmission of HIV guideline.” MoH (Ethiopia) official.
Facilitators of Feeding Practice
Hoping for their child to be healthy especially their HIV-exposed infant was the driving force of deciding how to feed their preterm HIV-exposed infants. The below-mentioned facilitator was echoed by most of the study participants.
“I was feeding her (the newborn) properly wanting her to be healthy. I feed her good because I want my child to be negative (HIV). That is the main reason why I feed her (the child) well.” A 27-year-old HIV-positive mother.
Barrier and Challenges of Feeding Practice
Most of the mothers preferred to explain their challenges and barrier than the facilitating factors of feeding their HIV-exposed preterm infants. Among these reasons, when their HIV-exposed child got sick with any other disease and stopped feeding or had vomiting, the mothers felt disappointed and discouraged to feed the child.
“My child was sick. He (her child) was not fed well and was vomiting whatever he ate. He cried a lot. I was very sad. I almost thought he (her child) was dying. Thanks to God he is fine now and started eating good after I took him to treatment.” HIV-positive mother who uses formula feeding.
The main barrier and challenge mentioned by HIV-positive mothers who had a preterm baby was their low economic status. Because of that, even the mothers were unable to provide proper feeding for their HIV-exposed children.
“I would like not to breastfeed my child because I want to lessen the chance of my child having HIV but I cannot buy powder milk because I have no money until she (her child) becomes six months. So, I breastfeed her without any choice. I am poor. I cannot afford it (the powder milk).” A mother of two children
Husband and Family Support in Feeding Practice
Most married HIV-positive mothers explained that the husband was supporting them in recommended feeding practices for their HIV-exposed preterm infants. If HIV-positive women disclosed their status to their family, their family also supported or helped them in the recommended feeding practice. But most of the interviewees related this to financial support rather than the commitment of time and care.
“He (her husband) is the only one helping me to take care of my child. Yes, I have a family but they live far from here. He feeds the child whenever he is around. Sometimes he also prepares food for the child.” A married woman who used formula feeding.
Discussion
The major finding of this study was that health education given during ANC did not consider the feeding practice needs of HIV-exposed preterm infants. The main facilitator of proper recommended feeding practice for HIV-exposed preterm infants was the desire of the mothers for good health for the baby. Low socioeconomic status leading to financial constraints was the main challenge for mothers to follow any formula recommended feeding practices for their HIV-exposed preterm infant.
HIV-exposed preterm infant feeding practices were not highlighted in health education sessions during ANC visits even though HIV is associated with more premature deliveries. This left the mothers with HIV-exposed preterm infants without good information on how to best feed their infant in this context. In contrast to the 2016 Ethiopian Demographic and Health Survey,26 more than half (57%) of women age 15–49 knew about the three ways HIV can be transmitted from the mother to her infant. This might be due to the study participants being selected from hospitals ie the chance of health education might have been increased compared to those not utilizing hospital services. The knowledge and understanding of health care providers and mothers who have HIV-exposed preterm infants was not congruent with the national PMTCT guideline. A PMTCT guideline (2017) of the Ministry of Health (Ethiopia) suggests HIV-positive pregnant women on the importance of exclusive breastfeeding for the first 6 months of life, followed by the introduction of appropriate complementary feeding at 6 months with continued breastfeeding for at least 12 months. Discontinuing breastfeeding is recommended only when a nutritionally adequate and safe diet without breast milk is available. Weaning should be done gradually within a week.22 Contrary to the guideline, our study discovered that the health care providers were not educating HIV-infected pregnant women according to the national PMTCT guideline. Subsequent to few interviews with health care providers, MoH (Ethiopia) revised the guideline in 2017. This might be due to the health care providers were not aware of the new (2017) guideline during the study period. Efforts should be needed to ensure health care providers to know and familiarize themselves with the new guideline in a good time. A study in Kenya noted a similar problem.27
The desire to have a healthy infant was found to be a facilitator for breastfeeding of HIV-exposed infants by their mothers as financial constraint left them with no option other than exclusive breastfeeding. Similar to our findings, financial constraints precluded the option of formula feeding in different studies, especially from developing countries.27–29
Child health status was the main contributing factor for the HIV-exposed preterm infant feeding practice in our study. If the child was healthy and able to breastfeed, the mother breastfeed the infant. But, when the infant was sick and vomited and could not breastfeed, most mothers felt disappointed and were discouraged. The 2017 PMTCT guideline suggested health care providers should support the mother to practice with correct positioning and attachment of breastfeeding; moreover, the health care providers should advise the mother to return to health facility immediately if she encounters difficulty of breastfeeding.22 A study in South Africa stated that HIV-positive mothers tended to exclusively breastfeed their HIV-exposed infants to make their child healthy.30
Many earlier studies mainly focused on HIV-exposed term infant feeding practices, whereas our study specifically targeted HIV-exposed preterm infants. These infants are more likely than term infants to have periods when they do not breastfeed well. Hence, the importance of having recommendations for feeding HIV-exposed preterm infants, currently a neglected area in Ethiopian guidance.
There are limitations in this study. First, this study was conducted in the capital city of Ethiopia hence perspectives might not represent those in the rural part of the country. Second, the study only included those seen at a hospital; other urban mothers who did not seek hospital care might also have different perspectives. While the link to a hospital may have optimized the opportunity for education, there was no highlighting in this teaching any best practices for feeding premature infants nor was their teaching on how best to manage if the premature baby became ill and would not breastfeed. Lastly, the study area, which is Addis Ababa, is a large city made up of variety of cultural, economic and ethnic populations, hence, the study subjects may not reflect this diversity.
Conclusions
The desire to have a healthy infant was a major facilitator for feeding of HIV-exposed premature infants according to usual HIV feeding recommendations. However, financial constraints were a major factor limiting the option of exclusive breastfeeding. This became even more problematic for the mother if the premature infant became ill and could not breastfeed well. The Ministry of Health (Ethiopia) guidance does not highlight how to best feed HIV-exposed premature infants even though premature delivery is more common with HIV infection. This gap needs to be addressed by the Ministry and all parties on the ground. Furthermore, there needs to be an implementation strategy developed so that all HIV-positive mothers receive appropriate infant feeding instructions during their pregnancy and follow-up following delivery.
Abbreviation
ANC, antenatal care; ART, antiretroviral therapy; HAART, highly active antiretroviral therapy; MTCT, Mother to child transmission; MoH, Ministry of Health; NICU, neonatal intensive care unit; PMTCT, prevention of mother to child transmission; WHO, World Health Organization.
Data Sharing Statement
Anonymized data will be shared up on request to the corresponding author.
Ethics Approval and Consent to Participate
Ethical clearance and approval were obtained from the Institutional Review Board (IRB) of St. Paul’s Hospital Millennium Medical College (P.M 23/251). Informed consent was obtained from each study participant. All methods were performed in accordance with the relevant guidelines for reporting qualitative studies (COREQ).
Acknowledgments
We would like to acknowledge Ethiopia-Canada Maternal, Newborn and Child Health Project and St. Paul’s Millennium Medical College Hospital for funding this research. The authors are grateful to MicroResearch (www.microresearch.ca) and Robert Bortolussi for mentoring and support with the analysis and manuscript review.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Ethiopia-Canada Maternal, Newborn and Child Health Project and St. Paul’s Hospital Millennium Medical College provided modest funding for this work. The funder has no role in this research.
Disclosure
The authors declare that there is no conflicts of interest in this work.
References
1. Katona P, Katona-Apte J. The interaction between nutrition and infection. Clin Infect Dis. 2008;46(10):1582–1588. doi:10.1086/587658
2. Nyaradi A, Li J, Hickling S, Foster J, Oddy WH. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front Hum Neurosci. 2013;7:97. doi:10.3389/fnhum.2013.00097
3. Kumar RK, Singhal A, Vaidya U, Banerjee S, Anwar F, Rao S. Optimizing nutrition in preterm low birth weight infants-consensus summary. Front Nutr. 2017;4:20. doi:10.3389/fnut.2017.00020
4. WHO Guidelines Approved by the Guidelines Review Committee. Guideline: Updates on HIV and Infant Feeding: The Duration of Breastfeeding, and Support from Health Services to Improve Feeding Practices Among Mothers Living with HIV. Geneva: Copyright (c) World Health Organization 2016; 2016.
5. World Health Organization. Guidelines on HIV and infant feeding. Principles and Recommendations for Infant Feeding in the Context of HIV and a Summary of Evidence. WHO, UNAIDS, UNFPA, unicef; 2010.
6. March of Dimes, PMNCH, Save the Children, WHO. Born Too Soon: The Global Action Report on Preterm Birth. Geneva: World Health Organization; 2012.
7. Sema A, Tesfaye F, Belay Y, Amsalu B, Bekele D, Desalew A. Associated factors with low birth weight in Dire Dawa City, Eastern Ethiopia: a Cross-Sectional Study. Biomed Res Int. 2019;2019:2965094. doi:10.1155/2019/2965094
8. Mulualem G, Wondim A, Woretaw A. The effect of pregnancy induced hypertension and multiple pregnancies on preterm birth in Ethiopia: a systematic review and meta-analysis. BMC Res Notes. 2019;12(1):91. doi:10.1186/s13104-019-4128-0
9. Mekonen DG, Yismaw AE, Nigussie TS, Ambaw WM. Proportion of preterm birth and associated factors among mothers who gave birth in Debretabor town health institutions, northwest, Ethiopia. BMC Res Notes. 2019;12(1):2. doi:10.1186/s13104-018-4037-7
10. Aregawi G, Assefa N, Mesfin F, et al. Preterm births and associated factors among mothers who gave birth in Axum and Adwa Town public hospitals, Northern Ethiopia, 2018. BMC Res Notes. 2019;12(1):640. doi:10.1186/s13104-019-4650-0
11. Kelkay B, Omer A, Teferi Y, Moges Y. Factors associated with singleton preterm birth in Shire Suhul General Hospital, Northern Ethiopia, 2018. J Pregnancy. 2019;2019:4629101. doi:10.1155/2019/4629101
12. Degaga GT, Sendo EG, Tesfaye T. Prevalence of exclusive breast milk feeding at discharge and associated factors among preterm neonates admitted to a neonatal intensive care unit in public hospitals, Addis Ababa, Ethiopia: a Cross-Sectional Study. Pediatric Health Med Ther. 2020;11:21–28. doi:10.2147/PHMT.S215295
13. Siegfried N, van der Merwe L, Brocklehurst P, Sint TT. Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection. Cochrane Database Syst Rev. 2011;7:CD003510.
14. Kassa GM. Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2018;18(1):216. doi:10.1186/s12879-018-3126-5
15. Kowalska A, Niemiec T, El Midaoui A, Burkacka E. Effect of antiretroviral therapy on pregnancy outcome in HIV-1 positive women. Med Wieku Rozwoj. 2003;7(4 Pt 1):459–468.
16. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. World Health Organization; 2016.
17. Watts DH, Williams PL, Kacanek D, et al. Combination antiretroviral use and preterm birth. J Infect Dis. 2013;207(4):612–621. doi:10.1093/infdis/jis728
18. Kebede B, Andargie G, Gebeyehu A. Birth outcome and correlates of low birth weight and preterm delivery among infants born to HIV-infected women in public hospitals of Northwest Ethiopia. Health. 2013;05(07):25–34. doi:10.4236/health.2013.57A4004
19. Agostoni C, Buonocore G, Carnielli VP, et al. Enteral nutrient supply for preterm infants: commentary from the European society of paediatric gastroenterology, hepatology and nutrition committee on nutrition. J Pediatr Gastroenterol Nutr. 2010;50(1):85–91. doi:10.1097/MPG.0b013e3181adaee0
20. WHO Guidelines. Approved by the Guidelines Review Committee. Guidelines on HIV and Infant Feeding 2010: Principles and Recommendations for Infant Feeding in the Context of HIV and a Summary of Evidence. Geneva: Copyright (c) World Health Organization 2010; 2010.
21. World Health Organization. Guideline: Updates on HIV and Infant Feeding: The Duration of Breastfeeding, and Support from Health Services to Improve Feeding Practices Among Mothers Living with HIV. WHO; 2016.
22. Federal Democratic Republic of Ethiopia Ministry of Health. National Comprehensive and Integrated Prevention of Mother-To-Child Transmission of HIV Guideline; 2017.
23. Coovadia HM, Rollins NC, Bland RM, et al. Mother-to-child transmission of HIV-1 infection during exclusive breastfeeding in the first 6 months of life: an intervention cohort study. Lancet. 2007;369(9567):1107–1116. doi:10.1016/S0140-6736(07)60283-9
24. Ethiopia Federal Ministry of Health. Health and Health Related Indicators 2005 E.C (2012/2013) Version 2; 2014.
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Central Statistical Agency (CSA)[Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016: HIV Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2018.
27. Lang’at PC, Ogada I, Steenbeek A, et al. Infant feeding practices among HIV-exposed infants less than 6 months of age in Bomet County, Kenya: an in-depth qualitative study of feeding choices. Arch Dis Child. 2018;103(5):470–473. doi:10.1136/archdischild-2017-314521
28. Laar SA, Govender V. Factor influencing the choices of infant feeding of HIV-positive mothers in Southern Ghana: the role of counsellors, mothers, families and socio-economic status. J AIDS HIV Res. 2011;3(7):129–137.
29. Olantona FA, Ginigeme ON, Roberts AA, Amu EO. Infant feeding practices in the first six months of life among HIV positive mothers attending teaching hospitals in Lagos, Nigeria. Niger J Paediatr. 2014;4(1):64–69.
30. Jama NA, Wilford A, Masango Z, et al. Enablers and barriers to success among mothers planning to exclusively breastfeed for six months: a qualitative prospective cohort study in KwaZulu-Natal, South Africa. Int Breastfeed J. 2017;12(1):43. doi:10.1186/s13006-017-0135-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.