")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Feasibility of full and rapid neuromuscular blockade recovery with sugammadex in myasthenia gravis patients undergoing surgery – a series of 117 cases
Authors Vymazal T, Krecmerova M, Bicek V, Lischke R
Received 24 July 2015
Accepted for publication 11 September 2015
Published 15 October 2015 Volume 2015:11 Pages 1593—1596
DOI https://doi.org/10.2147/TCRM.S93009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Tomas Vymazal,1 Martina Krecmerova,1 Vladimír Bicek,1 Robert Lischke2
1Department of Anaesthesiology and ICM, 2nd Faculty of Medicine, 23rd Surgical Department of 1st Faculty of Medicine, Charles University in Prague and Motol University Hospital, Prague, Czech Republic
Purpose: Myasthenia gravis (MG) is an autoimmune disease interfering with neuromuscular transmission. Patients are at risk of postoperative residual curarization (PORC) if nondepolarizing muscle relaxants are used. Clinically inapparent insufficient muscle strength may result in hypoventilation and postoperative bronchopneumonia. We describe a cohort of 117 cases in which sugammadex was used in MG patients undergoing surgery with muscle relaxation with rocuronium.
Methods and patients: We anesthetized 117 patients with MG using rocuronium and sugammadex as neuromuscular blockade reversal agent. One hundred five patients underwent surgical thymectomy and 12 underwent cholecystectomy (five laparotomic and seven laparoscopic). We measured time from sugammadex administration to recovery and to extubation, using the TOF-Watch® (series of four consecutive electrical impulses [the train-of-four] >0.9). We tracked peripheral capillary oxygen saturation (SpO2) <95%, elevation of partial pressure of carbon dioxide (pCO2) >10% above baseline, number of reintubations within the first 48 hours, and number of pneumonias within 120 hours, postoperatively. Results were processed as average, minimum, and maximum values.
Results: The period needed to reach train-of-four of 0.9 following sugammadex administration was on average 117 seconds (minimum of 105 seconds/maximum of 127 seconds) and differed within deviation <10%. The time to extubation following sugammadex administration was on average 276 seconds (minimum of 251 seconds/maximum of 305 seconds) and differed minimally among patients as well. We observed no SpO2 <95%, no pCO2 elevation >10% above a baseline, no emergent reintubation within the first 48 hours, and no pneumonia diagnosed on clinical basis within 120 hours, postoperatively in all 117 patients.
Conclusion: In this cohort of MG patients undergoing surgery using rocuronium and sugammadex, we did not observe any signs of postoperative residual curarization and respiratory depression. The neuromuscular blockade recovery was reliable, predictable, and rapid.
Keywords: neuromuscular blockade recovery, myasthenia gravis, general anesthesia, sugammadex
Introduction
Myasthenia gravis (MG) is a disease that affects neuromuscular transmission. Patients show unpredictable sensitivity and response to the administration of nondepolarizing muscle relaxants. The risk of residual neuromuscular blockade and postoperative respiratory failure with consequent complications is very high in such patients.1 This blockade may not be clinically apparent. Insufficient muscle strength may result in hypoventilation, oxygen desaturation, development of hypercapnia, micro- and macroaspirations, and postoperative bronchopneumonia in the postoperative period.2 An essential part of MG treatment, namely if there is a thymoma present (10%–15% of cases), is surgical thymectomy. Thymoma is most often a benign tumor of the thymus which produces acetylcholine receptor autoantibodies and can sometimes even produce autoantibodies against certain muscle proteins such as the titin and ryanodine receptor. Full thymectomy by partial sternotomy is the gold standard surgical treatment.3
Sugammadex selectively encapsulates steroid nondepolarizing muscle relaxants, thus leaving the receptor free for acetylcholine. Encapsulation is irreversible, and the whole complex is then excreted from the body through the urine. Efficiency and reliability of sugammadex has been repeatedly shown in several clinical studies.4 The aim of this case series was therefore to verify whether sugammadex can secure full and rapid neuromuscular blockade recovery with avoiding respiratory depression in patients with MG.
Methods and patients
With the approval of the local ethics committee of the Teaching Hospital Motol and with written consents of participants, we anesthetized 117 patients (from June 2010 to September 2014) with MG type IIa and IIb (Osserman’s classification) using general anesthesia (GA) with rocuronium and sugammadex as neuromuscular blockade reversal agent. Demographic data are shown in Table 1. One hundred five patients underwent surgical thymectomy with partial sternotomy and 12 patients underwent cholecystectomy (five laparotomic and seven laparoscopic). The degree of neuromuscular blockade was measured with the device TOF-Watch® (Organon, Mainline Medical Inc, Norcross, GA, USA) using a series of four consecutive electrical impulses (TOF, train-of-four). As the primary endpoints, we measured time from sugammadex administration to full muscle strength recovery (generally accepted value TOF 0.9) and to the removal of the endotracheal tube. As the secondary endpoints, we tracked clinical signs of the postoperative residual curarization (PORC) – peripheral blood hyposaturations lower than 95%, measured by standard pulse oximeter in bedside monitor of vital functions, elevation of partial pressure of carbon dioxide (pCO2) more than 10% (standard deviation >10%) above baseline (quiet spontaneous ventilation prior to induction to GA), measured by emergency capnometer EMMA Monitor® (Phasein AB, Danderyd, Sweden). Patients who underwent laparoscopic cholecystectomy had the arterial line, the number of reintubations within the first 48 hours following the surgery, and the incidence of acquired bronchopneumonias diagnosed on clinical basis (due to possible aspirations) within 120 hours, postoperatively.
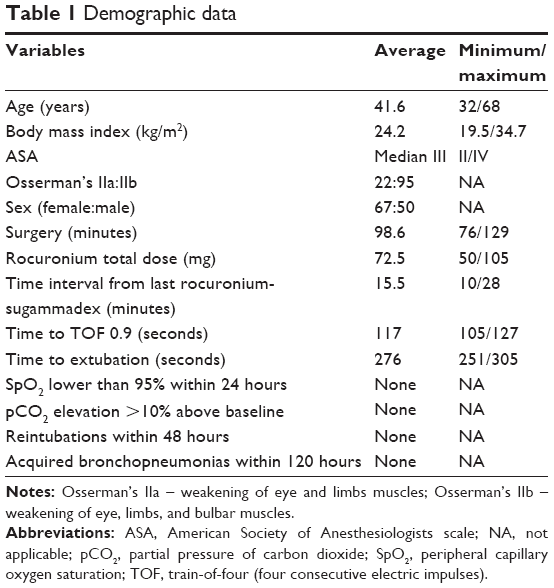 | Table 1 Demographic data |
GA was administered to all patients, starting with propofol (2 mg kg−1) and sufentanil analgesia, 0.2 μg kg−1 to a maximum dose of 0.8 μg kg−1. This was followed by inducing muscle relaxation with an unreduced dose of rocuronium of 0.6 mg kg−1 intravenously for orotracheal intubation and a maintenance dose of 0.15 mg kg−1 if TOF >0.6. GA was supplemented in all patients by the inhalation of O2+ air + isoflurane (up to 1.0% in the expired mixture). Depth of muscle relaxation was measured with the device TOF-Watch. In accordance with the manufacturer’s recommendations, the ulnar nerve was stimulated, and the accelerometry response of the adductor pollicis muscle was measured by the device. Calibration was performed. Dosage of all pharmaceuticals was converted based on the patient’s body weight. Benzodiazepines were not administered. In accordance with pharmaceutical company’s recommendations on deep muscle relaxation with a TOF between zero and one, sugammadex was administered at a dose of 4 mg kg−1, while a TOF measurement of two and more was followed by a dose of 2 mg kg−1. We measured the time from sugammadex administration to TOF 0.9. The needed time for extubation was measured from the moment of TOF reaching 0.9 till the removal of endotracheal tube from the patient’s airways. Results were processed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA), with average, minimum, and maximum values.
Results
Our patient population was heterogeneous, with large variations in age, body weight, duration of surgery, and total administered dose of rocuronium. The patient’s physical status was determined using the ASA (American Society of Anesthesiologists’) scale, with a median of III. The period needed to reach TOF of 0.9 following sugammadex administration was on average 117 seconds (minimum of 105 seconds/maximum of 127 seconds) and differed within a deviation <10%. The time to extubation following sugammadex administration was on average 276 seconds (minimum of 251 seconds/maximum of 305 seconds) and differed minimally among patients as well. All patients were transferred from the operating room to a monitored bed in the postoperative intensive care unit (ICU). We observed no fall of peripheral capillary oxygen saturation (SpO2) less than 95% on room air, no elevation of pCO2 more than 10% above the baseline measured for 4 hours in 30-minute intervals after admission to ICU. No patient needed reintubation due to respiratory failure within 48 hours following the surgery. None of our patients had clinical signs of acquired bronchopneumonia in 120 hours, postoperatively. The summary of the results is given in Table 1.
Discussion
The results from our series of 117 patients has shown that sugammadex has brought full and rapid neuromuscular blockade recovery in patients with MG. Patients at higher risk for muscle deficit and function due to MG were successfully reversed to a TOF 0.9. We observed no serious and significant fall in SpO2 and no hypoventilation in both the operation room and ICU. None of the patients needed reintubation within 48 hours. None of our patients had clinical bronchopneumonia 120 hours, postoperatively. The results of a search in PubMed database from June 2010 to January 2015 suggest that this is the most extensive published group of patients with the aforementioned disorder of neuromuscular transmission.
Steroid nondepolarizing muscle relaxants are a common part of the current overall GA.5 However, the administration of muscle relaxants is associated with many problems, including difficulties in the quantification of their effects, differences in the sensitivity of individual patients, and also effects related to age and sex.6,7 The result of often inadequate dosage of muscle relaxants is PORC, which increases the risk of hypoventilation and postoperative pneumonia. Residual neuromuscular blockade also contributes to postoperative aspiration. Studies in awake volunteers and surgical patients have demonstrated that TOF ratios of 0.7–0.9 are associated with impaired airway protective reflexes,8 upper airway obstruction,9 a decreased hypoxic ventilatory response,10 and postoperative hypoxemia.11 On the basis of these findings, several investigators have recommended that full recovery of neuromuscular function (TOF ratio of 0.9) should be present at the time of tracheal extubation.9,12,13 PORC (defined by the TOF ratio <0.9 at accelerometry monitoring of neuromuscular transmission) occurs in approximately 34% of patients (upon admission to ward after surgery) relaxed during the surgery using rocuronium without accelerometry monitoring.14
In principle, three procedures15 can be used for PORC treatment. The first is to continue artificial ventilation until full recovery of muscle strength, which is associated with the risks of prolonged ventilation and prolonged occupancy in the operating room that hinder the smooth running of the operational program. The second is to apply standard decurarization using the combination of atropine and neostigmine. Neostigmine is known for its “ceiling effect”.16 Disadvantages of this procedure include possible tachycardias (following atropine administration) and increased secretion from the respiratory tract, which is inconvenient, particularly in patients with incompetency of neuromuscular transmission and lower muscle strength and preexisting lung disease.7,17 The third and newest option that can only be applied after the application of rocuronium or possibly vecuronium is administration of sugammadex, which selectively binds to aminosteroid muscle relaxants, has no “ceiling effect”, and does not impact pulmonary function or hemodynamics.14
Similar to some published case reports describing the administration of sugammadex in patients with MG,18–22 we evaluated a group of 117 patients undergoing surgery with GA. Our results are consistent with the findings of other authors who described its administration in a clinical situation.4,23–25 We can say that the effect of sugammadex in patients with the diagnosis of MG is reliable and predictable.26 In a very short time, unaffected by patient’s age, body weight, surgery duration, or the total administered dose of rocuronium, it results in full recovery of neuromuscular transmission, guaranteeing full muscle strength. This will significantly reduce the risk of PORC18,25,26 including all its serious complications.17,27 We suggest sugammadex as a component of accelerated recovery after surgery to avoid PORC in MG patients.
Limitations
The limitations of this case series can be the enrolling of patients of only IIa and IIb per Osserman’s classification and the small number of the patients.
Conclusion
In the largest published cohort of MG patients undergoing surgery in GA using rocuronium and sugammadex, we did not observe any signs of PORC. The neuromuscular blockade recovery was reliable, predictable, and led rapidly to full neuromuscular transmission.
Disclosure
The authors report no conflicts of interest in this work.
References
Drachman DB. Myasthenia gravis and other diseases of the neuromuscular junction. In: Harrison’s Principles of Internal Medicine. New York, NY: McGraw-Hill Companies, Inc.; 2008:2672–2677. | ||
Valenstein E, Musulin M. Neuromuscular disorders. In: Civetta, Taylor & Kirby’s Critical Care. Philadelphia, PA: Lippincott Williams and Wilkins, A Wolters Kluwer Business; 2009:2235–2241. | ||
Bailey PD. Surgical approach to myasthenia gravis. In: Pearson’s Thoracic and Esophageal Surgery. New York, NY: McGraw-Hill Companies, Inc, 2008:655–668. | ||
Fennema H, Woo T, Jones K, et al. Sugammadex for rocuronium- or vecuronium-induced blockade reversal: a pooled analysis of 26 controlled studies. Poster presented at: sASA 2013 American Society of Anesthesiologists Annual Meeting; San Francisco, CA. Abstract A4013. | ||
Schaller SJ, Fink H. Sugammadex as a reversal agent for neuromuscular block: an evidence-based review. Core Evid. 2013;8:57–67. | ||
Adamus M, Gabrhelik T, Marek O. Influence of gender on the course of neuromuscular block following a single bolus dose of cisatracurium or rocuronium. Eur J Anaesthesiol. 2008;25:589–595. | ||
Racca F, Mongini T, Wolfler A, et al. Recommendations for anesthesia and perioperative management of patients with neuromuscular disorders. Minerva Anesthesiol. 2013;79:419–433. | ||
Sundman E, Witt H, Olsson R, et al. The incidence and mechanisms of pharyngeal and upper esophageal dysfunction in partially paralyzed humans: pharyngeal videoradiography and simultaneous manometry after atracurium. Anesthesiology. 2000;92:977–984. | ||
Eikermann M, Groeben H, Husing J, Peters J. Accelerometry of adductor pollicis muscle predicts recovery of respiratory function from neuromuscular blockade. Anesthesiology. 2003;98:1333–1337. | ||
Eriksson LI, Sato M, Severinghaus JW. Effect of a vecuronium-induced partial neuromuscular block on hypoxic ventilatory response. Anesthesiology. 1993;78:693–699. | ||
Bessinger U, Schimek F, Lenz G. Postoperative residual paralysis and respiratory status: a comparative study of pancuronium and vecuronium. Physiol Res. 2000;49:455–462. | ||
Debaene B, Plaud B, Dilly MP, Donati F. Residual paralysis in the PACU after a single intubating dose of nondepolarizing muscle relaxant with an intermediate duration of action. Anesthesiology. 2003;98:1042–1048. | ||
Baillard C, Bourdiau S, Le Toumelin P, et al. Assessing residual neuromuscular blockade using acceleromyography can be deceptive in postoperative awake patients. Anesth Analg. 2004;98:854–857. | ||
Carron M, Veronese S, Foletto M, Ori C. Sugammadex allows fast-track bariatric surgery. Obes Surg. 2013;23:1558–1563. | ||
Cerny V, Herold I, Cvachovec K, Sevcik P, Adamus M. Guidelines for managing neuromuscular block: not only Czech beer deserves a taste. Anesth Analg. 2011;112:482. | ||
Bartkowski RR. Incomplete reversal of pancuronium neuromuscular blockade by neostigmine, pyridostigmine, and edrophonium. Anesth Analg. 1987;66:594–598. | ||
Berg H, Roed J, Viby-Mogensen J, et al. Residual neuromuscular block is a risk factor for postoperative pulmonary complications. A prospective, randomised, and blinded study of postoperative pulmonary complications after atracurium, vecuronium and pancuronium. Acta Anaesthesiol Scand. 1997;41(9):1095–1103. | ||
Sugawara A, Sasakawa T, Hasegawa N, Takahata O, Iwasaki H. Administration of sugammadex to a patient with myasthenia gravis with fade of the train-of-four ratio. Masui. 2011;60:1082–1085. | ||
de Boer HD, van Egmond J, Driessen JJ, Booij LH. Sugammadex in patients with myasthenia gravis. Anaesthesia. 2010;65:653. | ||
Petrun AM, Mekis D, Kamenik M. Successful use of rocuronium and sugammadex in a patient with myasthenia. Eur J Anaesthesiol. 2010;27:917–918. | ||
Unterbuchner C, Fink H, Blobner M. The use of sugammadex in a patient with myasthenia gravis. Anaesthesia. 2010;65:302–305. | ||
Garcia V, Diemunsch P, Boet S. Use of rocuronium and sugammadex for caesarean delivery in a patient with myasthenia gravis. Int J Obstet Anesth. 2012;21:286–287. | ||
Komasawa N, Noma H, Sugi T, Sukenaga N, Kakiuchi H. Effective reversal of muscle relaxation by rocuronium using sugammadex in a patient with myasthenia gravis undergoing laparoscopic cholecystectomy. Masui. 2011;60:476–479. | ||
Porter MV, Paleologos MS. The use of rocuronium in a patient with cystic fibrosis and end-stage lung disease made safe by sugammadex reversal. Anaesth Intensive Care. 2011;39:299–302. | ||
Argiriadou H, Anastasiadis K, Thomaidou E, Vasilakos D. Reversal of neuromuscular blockade with sugammadex in an obese myasthenic patient undergoing thymectomy. J Anesth. 2011;25:316–317. | ||
de Boer HD, van Egmond J, Driessen JJ, Booij LH. A new approach to anesthesia management in myasthenia gravis: reversal of neuromuscular blockade by sugammadex. Rev Esp Anestesiol Reanim. 2010;57:181–184. | ||
Murphy GS. Residual neuromuscular blockade: incidence, assessment, and relevance in postoperative period. Minerva Anestesiol. 2006;72:97–109. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.