")
Back to Journals » Patient Preference and Adherence » Volume 13
Feasibility and efficacy of nurse-led team management intervention for improving the self-management of type 2 diabetes patients in a Chinese community: a randomized controlled trial
Authors Guo Z, Liu J, Zeng H, He G, Ren X, Guo J
Received 27 April 2019
Accepted for publication 19 July 2019
Published 14 August 2019 Volume 2019:13 Pages 1353—1362
DOI https://doi.org/10.2147/PPA.S213645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Zhihua Guo, Jing Liu, Hui Zeng, Guoping He, Xiaohong Ren, Jia Guo
Xiangya School of Nursing, Central South University, Changsha 410013, Hunan, People’s Republic of China
Aim: The aim of this study was to examine the feasibility and efficacy of nurse-led team management (NLTM) intervention at improving the self-management of patients with type 2 diabetes (T2D) at community settings in Changsha, Hunan, China.
Background: China has become the country with the largest number of patients with diabetes, and that number is growing, causing increasing pressure on the health care system. At present, the main diabetes management model in China is teamwork guided by general practitioners. However, the number of general practitioners is insufficient, and their work is overloaded, which leads to poor outcomes of diabetes management. Therefore, it is important to explore alternative methods of diabetes management, such as NLTM.
Patients and methods: In a randomized controlled trial, 171 T2D patients were randomized into the control or intervention arm. Participants in the control group received routine management from the community health service center, whereas the intervention group received 12 months NLTM intervention in addition to the standard care. The diabetes self-management scale, fasting blood sugar, and glycosylated hemoglobin A1c (HbA1c) were assessed at baseline and at 6 and 12 months after the start of the intervention.
Results: Baseline data were comparable between arms. Repeated-measurement analysis showed that self-management of the intervention group improved compared with the control group after the intervention (P<0.05). There were no significant differences in HbA1c at 6 months, whereas after 12 months of intervention, there was a significant difference in HbA1c between the two groups (F=10.114, P<0.05). The intervention had no significant effect on fasting blood sugar.
Conclusion: The NLTM intervention has resulted in an impact of practical significance on T2D self-management, and was beneficial for controlling the level of HbA1c. The study has demonstrated the feasibility and efficacy of using NLTM in the management of T2D in a Chinese community.
Keywords: type 2 diabetes, nurse-led team management, self-management
Introduction
Diabetes mellitus is a metabolic disorder characterized by hyperglycemia. In recent years, the incidence of diabetes has been increasing rapidly worldwide. According to the International Diabetes Federation, the number of people living with diabetes aged 18-99 years reached 451 million in 2017, and may rise to 693 million by 2045.1 China is the country with the highest number of diabetics, with about 114 million patients, and type 2 diabetes (T2D) accounts for more than 90% of all diagnosed cases of diabetes.2–4 Diabetes causes a variety of complications and a high rate of disability and mortality, and brings a heavy disease burden to society, which has become a serious public health problem that affects the sustainable development of the economy and society.5 Diabetes itself cannot currently be cured; patients need lifelong treatment, plus hypoglycemic drugs and lifestyle adjustments to control the disease’s progress. In addition, diabetes has prolonged and recurrent characteristics, requiring patients and their families to have the ability to perform self-monitoring and management of the disease. Therefore, finding appropriate ways to improve the level of self-management of diabetic patients is very important and meaningful.
Previous studies have confirmed that prevention and treatment in community health settings is the most important approach to effectively control diabetes.6,7 The integration of team management into community-based chronic disease management is an important model of basic medical and health services in China. In 2009, China incorporated diabetes case management into basic public health services and formulated corresponding management service specifications, which requires all community health services to be available to diabetic patients over 35 years old.8 Diabetes management has become one of the routine tasks of community health service providers in China. Community health centers provide free diabetes screenings, follow-ups, health education, health checkups, and disease classification intervention to urban and rural residents. By the end of 2017, 26 million patients with diabetes had been registered in the diabetes management system, and the number will reach 35 million by 2020.9
With the development of multidisciplinary team management, the guidelines for the prevention and treatment of T2D in China (version 2018) suggested that team members for diabetes management in community settings should consist of general practitioners, nurses, nutritionists, rehabilitators, and patients.10 However, with the increasing prevalence of diabetes but a severe shortage and maldistribution of generalist practitioners, it is difficult for general practitioners in local health care settings to undertake the increasingly onerous patient management services.11,12 Team management led by general practitioners is the main form of diabetes management in China; with doctor-led team management, the doctors not only take charge of treatment, but also of follow-ups, health education, archives management, team communication, and similar related tasks. Doctor-led diabetes team management focuses more on the diagnosis and treatment of diseases and less on time for family visits, telephone follow-ups, and health education, which leads to poor diabetes management outcomes due to the imbalance between the small number of general practitioners and the heavy workload. Some primary health service institutions in other countries have gradually changed from general-practitioner-led management to nurse-led team management (NLTM), and have effectively improved patient outcomes.13,14 The implementation of NLTM could significantly improve the self-management ability and glycosylated hemoglobin A1c (HbA1c) levels of diabetic patients in the community.15–18 A systematic review claimed that the nurse’s role of involvement in creating patient awareness, managing diabetes, and providing education about diabetes self-management is highly prominent in diabetes care.18 Thus, there is practical significance to exploring and promoting the NLTM model due to the situation of patients and community nurses being different in China.
In this study, we aimed to investigate the feasibility and efficacy of an NLTM intervention at improving the level of diabetes self-management and controlling blood glucose levels in Chinese community health settings.
Conceptual framework for the study
The conceptual model in this study was based on the chronic care model launched by Wagner and colleagues in 1999.19 The chronic care model has been considered to be an effective framework for improving the quality of diabetes care.20 This model includes six core elements for the provision of optimal care of patients with chronic diseases.21 The current study has addressed these six elements via NLTM intervention in the community for T2D (Table 1).
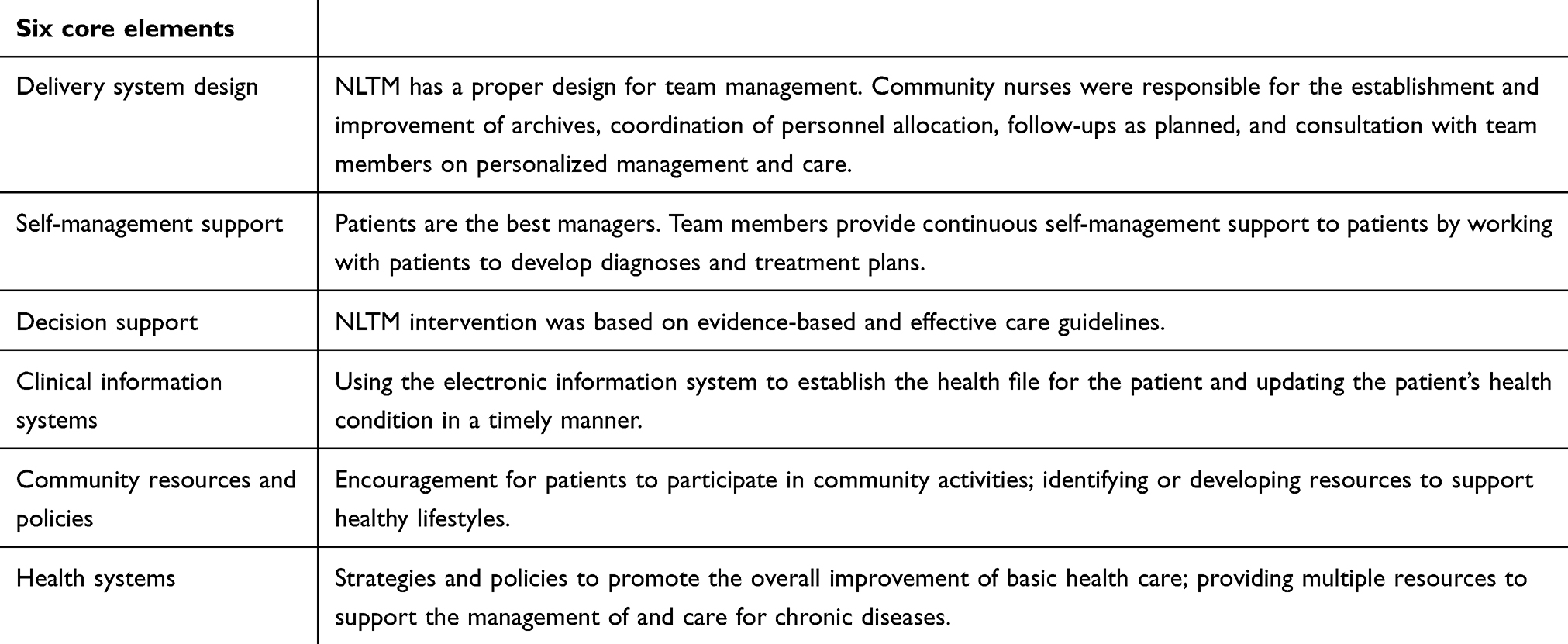 |
Table 1 The chronic care model in NLTM |
Patients and methods
Sample size calculation
Our study was to take HbA1c as the main effective index. According to the previous evidence,22 the HbA1c in the control group decreased by about 0.08% after 12 months, and that in the intervention group decreased by about 0.86%. Assuming a 10% loss in 12-month follow-up. Finally, a total of 171 samples, 86 in the intervention group and 85 in the control group, were included in the study.
Design, participants, and setting
We conducted a randomized controlled trial between March 2014 and March 2015, recruiting patients from the Wangyuehu community in the city of Changsha, Hunan Province. This community has registered 3351 patients with diabetes, 1639 of whom have T2D. Eligible participants: 1) were at least 18 years old; 2) had a confirmed T2D diagnosis; 3) were settled in Changsha; 4) were able to speak, understand, and read Mandarin; and 5) were willing to participate in this study. All procedures, including human subjects, were conducted in accordance with the guidelines set out in the recently revised Helsinki protocol. Written informed consent was obtained from each patient prior to the study. The study was approved by the institutional review board Committee of Medical College of Biology, Xi’an Jiaotong University. The ethical review number was 2014–008.
A simple randomized method was applied to tag patient from numbers 1 to number 171 in a non-repetitive and non-sequential manner. In this random sequence, the number assigned to the control group was less than 86, and the number assigned to the intervention group was 86–171. Patients in the control group received standard care, including four face-to-face follow-up visits (each with 20–30 mins diabetes health education) per year, free measurement of fasting blood sugar (FBS) four times per year, and a free physical examination in the community service station once per year. The intervention group, in addition to the standard care, received the NLTM intervention for 12 months.
Nurse-led team management (NLTM) intervention
The NLTM intervention was designed and planned in consultation with investigators, diabetes specialists, community doctors and nurses, a nutritionist, and patients and families regarding the content, frequency, and scheduling of the intervention. The team was composed of community nurses, community doctors, a clinical nursing specialist, three diabetes specialists, a nutritionist, and nursing post-graduates. Before the intervention, we trained the team, and the training content covered diabetes specialty knowledge, diet, and exercise knowledge; follow-ups, health education, and communication skills; and relevant policies and regulations. The NLTM intervention aimed to increase knowledge, enhance the compliance with diabetes self-management, provide emotional support, and solve problems. It consisted of 12 follow-up visits, 6 health lectures, and 6 free diabetes expert consultation services.
Twelve follow-up visits were conducted by community nurses and nursing graduate students, including 4 family follow-up visits during the 2nd, 4th, 8th, and 10th months, 6 telephone follow-up consultations during the 1st, 3rd, 5th, 7th, 9th, and 11th months, and 2 outpatient follow-up visits during the 6th and 12th months. Blood glucose monitoring diaries were distributed to patients at each family follow-up visit to remind patients to monitor their FBS at their convenience so that nurses could check and record the results. Each home visit lasted 20–30 mins, and the telephone consultation lasted 5–10 mins. The content of follow-up visits was based on the registration form of follow-up services for patients with T2D, including the measurements of FBS and blood pressure, evaluating medication adherence, adverse drug reactions and expiration of drugs, assessing patients’ diet and exercise, and providing individual health education and emotional support according to patients’ conditions. For patients with FBS controlled below 7.0mmol/L and without adverse drug reactions and complications, the next follow-up was scheduled for appointment. For those who were unsatisfied with their FBS control or who had adverse drug reactions, we organized team discussions and provided appropriate suggestions and guidance based on the patient’s situation, and followed up by telephone within two weeks. Patients who were not satisfied with the control of their FBS and who had new complications or recently aggravated drug reactions were recommended to be transferred to a diabetes physician at the superior hospital, and it was recommended that the referral be actively followed up on within two weeks.
The intervention group also attended a 60 min health lecture on diabetes at the community health service center during the 1st, 3rd, 6th, 8th, 10th, and 12th months. The main content of the lecture included diet management, exercise management, drug therapy, psychological adjustment, blood glucose monitoring, and insulin injection technology. The lectures were delivered by diabetes experts from the hospital affiliated with Central South University. We distributed diabetes education pamphlets according to the content of every lecture. After each lecture, the experimental group was provided with a free 1 hr expert consultation service related to knowledge, coping skills of the diabetes and psychological care.
We adopted an interactive approach and personalized treatment, allowing the participants to express their thoughts on treatment and intervention, and the intervention was adjusted based on the individualized situations and demands of the participants.
Measures
We collected demographic information (ie, age, gender, education level, occupational status, personal monthly income, types of medical insurance, marital status, and status of smoking and drinking) as well as disease-specific data (ie, time since T2D diagnosis, family history of diabetes mellitus, drug treatment regimens, and diabetic complications situation). Biomarkers included FBS and HbA1c.
Diabetes self-management was measured using the Diabetes Self-Management Scale originally developed and tested in China by Zhang.23 Its 22 items include five dimensions on dietary management, exercise management, drug management, blood glucose monitoring, and management of complications and risk factors. Responses to the questions were “never,” “occasionally,” “sometimes,” “usually,” and “always,” with scoring from 1 to 5 points, respectively; items 3, 4, 6, 9, and 10 were scored in reverse. Additionally, in the dimension of drug management, if participants did not receive medication or insulin treatment, the item’s score was 5 points. The total score of the scale ranges from 22 to 110; a higher total score indicates better self-management by the patients. According to the Cronbach’s alpha coefficients, the reliability coefficient for the scale has been reported as 0.75. The consistency of the test–retest reliability and content validity were 0.891 and 0.89, respectively.
Data collection
Data were collected at baseline and at 6 and 12 months of the intervention. We trained all the people who collected the data before beginning the collection process. In the first questionnaire on collection and physical examination, we registered and replenished the health records of the subjects, including the name, age, family information, disease-related information, and biochemical indicators. The questionnaire was filled out by the patients. The researchers and the community nurses were responsible for collecting and examining the items. The missing items were immediately filled out. The nurses recorded FBS and HbA1c levels in the patient files.
Data analysis
Independent-sample t-tests, χ2 tests, and Mann–Whitney U tests were used to compare the two study groups at the baseline. We used repeated-measurement analysis of variance to compare the total score of the diabetes self-management, as well as FBS and HbA1c levels, between the two groups. The difference in HbA1c between the two groups at different time points was further compared by multivariate analysis of variance. The significance level used in the study was 0.05.
Results
Participant characteristics
Of the 280 T2D patients living in the Wangyuehu community who were screened when they came to the community health center for services, 171 were recruited for the study and completed the baseline questionnaire: 86 in the intervention group and 85 in the control group. Of the original 280 T2D patients, 109 did not meet the criteria and were excluded, and 37 patients declined participation (Figure 1). During the 12-month follow-up, 143 participants completed the study, with 75 in the intervention group and 68 in the control group.
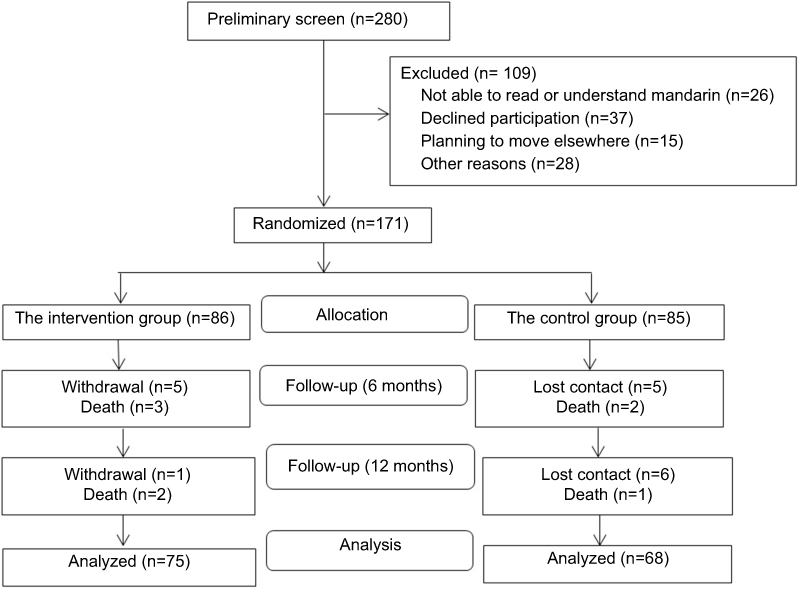 |
Figure 1 Flowchart of the participants. |
As shown in Table 2, there were no significant differences in any demographic or disease-related variables between groups at the baseline. Overall, participants were aged 63.7 years, 57.9% were female, and 62.6% reported being diagnosed with diabetes over five years ago.
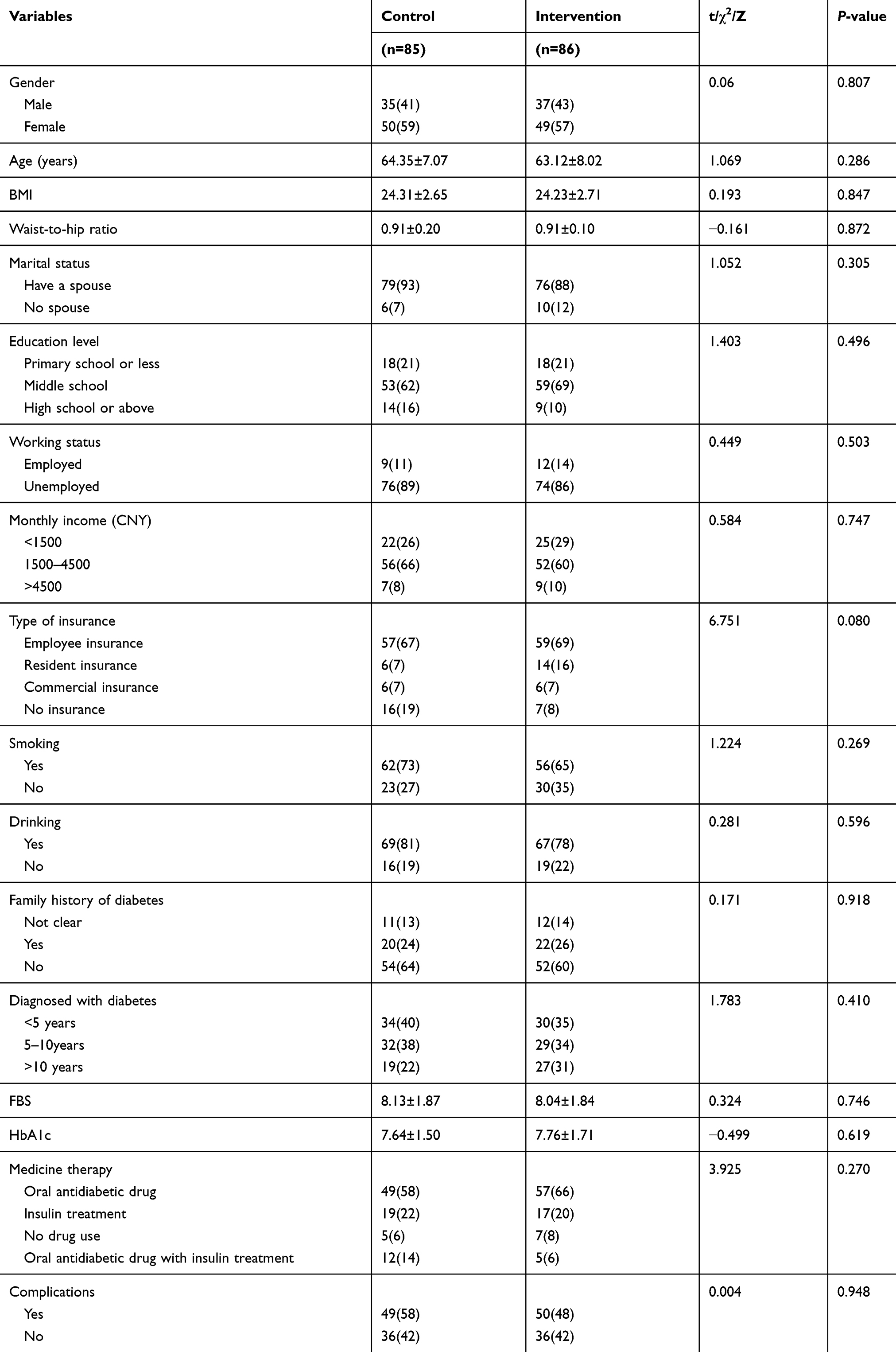 |
Table 2 Demographic and T2D information of the two groups |
Intervention outcomes
Compared with the control group, the mean score for diabetes self-management of the NLTM group demonstrated a better improvement over time than the control group after intervention (P<0.0001). The effect size of the NLTM intervention over time for diabetes self-management was 0.183 (Table 3).
 |
Table 3 Comparison of diabetes self-management (DSM) between the two groups |
Repeated-measurement analysis was used to analyze FBS and HbA1c before and after intervention (Table 4). No statistical differences were found in FBS in either pretests or posttests between the two groups. There was an interaction effect of intervention and time in HbA1c. Multivariate analysis of variance was used to further compare the HbA1c differences between the two groups at different time points (Table 5). The HbA1c results in the intervention group were lower than those in the control group after 12 months (P<0.05), but no statistical difference was indicated at 6 months.
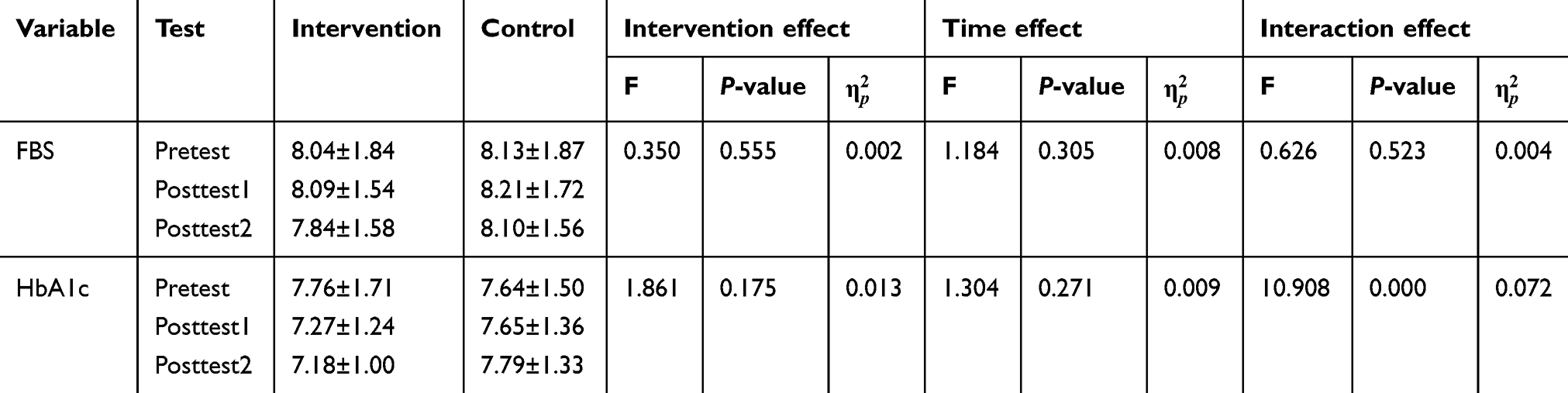 |
Table 4 Comparison of FBS and HbA1c between the two groups |
 |
Table 5 Comparison of HbA1c at different time points between the two groups |
Discussion
This study shows that NLTM intervention could enhance the level of self-management in T2D patients through different aspects. First, NLTM intervention could remind patients to manage themselves. Blood glucose monitoring diaries and telephone follow-up consultations were effective for patients to remind them to monitor and record blood glucose, and to facilitate staff viewing at the same time. Second, NLTM intervention could improve the level of diabetes-related knowledge and disease care awareness. We produced and distributed some diabetes education pamphlets with text and pictures based on the diabetes guidelines of the American Diabetes Association,24 the International Diabetes Federation,25 and the guidelines on Diabetes Care and Education in China.26 Holding a diabetes lecture is a way of promoting self-management education, and also provides opportunities for patients to communicate and learn from each other. Third, the family follow-up and expert consultation offered the patients and their families timely communication with health care providers for informational, emotional, and technical support to overcome a variety of barriers during their self-management time. The American Diabetes Association27 recommends that all patients with diabetes receive diabetes self-management education according to national standards. Beck J et al28 claimed that diabetes self-management education and support promote the knowledge, skills, and abilities necessary for diabetes self-care, as well as activities that assist individuals in implementing and sustaining the behaviors needed to manage their condition on an ongoing basis. This study, along with previous evidence, described changes in self-management after receiving education and management training.16,29,30
The results of the present study show that NLTM intervention improved HbA1c control in patients. As an important indicator of diabetes control, HbA1c reflects the recent average blood sugar levels of patients, and is closely related to the occurrence of diabetic complications.31 This finding was consistent with another study in Chengdu, China, which showed that team management led by community nurses was an effective nursing model to control blood sugar and prevent diabetes-related complications.22 Diabetes self-management education programs showed a significant decrease in HbA1c in the USA32,33 and Thailand.34 A systematic review and meta-analysis35 suggested that specially trained nurses appear to be more effective than physicians at educating patients with diabetes and cardiovascular diseases in the self-management of blood pressure and Hb1Ac in community settings, and nurse-led self-management support interventions can be included in routine primary care activities. Our study provided some educational intervention measures and highlighted the leading role of nurses in the intervention. The decrease of HbA1c levels indicates our intervention is beneficial to the control of blood sugar in patients with T2D.
Unexpectedly, we failed to find that NLTM had a significant impact on the decrease of FBS levels during the 12-month follow-up period, which was not consistent with previous findings that community-based diabetes self-management education could cause a significant reduction in FBS levels.36,37 Although the result was not significant between groups, the mean of FBG did drop from 8.04 mmol/L to 7.84 mmol/L in the intervention arm; whereas the mean kept the same level from 8.13 mmol/L to 8.10 mmol/L in the control arm. It may take more time to determine the effect of NLTM intervention on FBS.
The expectations of diabetes patients include having better control over diabetes, reducing impacts of the disease on their lives, and having timely access to competent guidance from health care professionals. Instituting NLTM could help achieve these goals. During the year of this study’s intervention, we ensured that we had effective communication with our participants at least once per month. As the contact time with the participants increased, the provider–patient relationship became much closer. To our delight, we found that the participants were more active in seeking help, and had an increase in trust and satisfaction with community health care workers. Most of the participants were willing to accept the NLTM model. Our study, along with previous evidence, suggests that community-based NLTM is an effective mode of care in terms of controlling blood glucose and preventing diabetes-related complications.22,35
Overall, NLTM intervention for improving the self-management of type 2 diabetes patients in a Chinese community is feasible and in line with the trend of medical development in China, and our study is meaningful for future scale-up. First, In February 2017, the Health and Family Planning Commission of the People’s Republic of China promulgated the national basic public health service standards (the third edition),38 which further added and explained the contents of health education in community health services, including the provision of health education materials, the health consultation activities not less than nine times per year, the health lectures at least once a month, and the provision of individualized health education. So, our intervention measures can be integrated into the routine. Besides, the number of practitioners (assistants) per 1000 resident population was 2.06 in 2013 and it will be increased to 2.5 in 2020, while the number of registered nurses per 1000 residents was 2.05 in 2013 and it will be increased to 3.14. The ratio of practitioners to registered nurses will be increased from 1:1 to 1:1.25.39 Thus, NLTM will be a more preferable model than the model of teamwork guided by practitioners as nurses are more sufficient. Last, there are nursing graduate students in the intervention team, and graduate students go to the community every year for internships, which is feasible for teaching units.
There were limitations in this study. The study mainly included diabetes patients in a large community of Changsha, which may cause a certain regional bias due to the average environmental and nutritional conditions may be significantly different in other regions and in rural areas. Furthermore, HbA1c results showed a statistical difference after 12 months, but no statistical difference at 6 months, which may indicate that intervention time is an important factor affecting the change in HbA1c. The 12-month follow-up may not be long enough to determine the effect of NLTM intervention. Third, we did not measure whether our intervention would increase the burden on nursing staff, which is an important aspect that may affect the feasibility of the NLTM intervention. Further studies encompassing multiple sites and a longer follow-up period and the measurement of the burden on nursing staff are suggested.
Conclusion
The NLTM intervention demonstrated preliminary efficacy at improving the level of self-management in patients with T2D, and it showed promising effects in terms of helping control HbA1c levels in T2D patients in a Chinese community. However, it failed to demonstrate a significant effect on the decrease in FBS during the 12-month follow-up period. Findings of this study suggest that NLTM can be applied to the management of T2D in community health settings.
Acknowledgments
The authors would like to acknowledge all the health care providers in the Wangyuehu community health service station for their cooperation in recruitment and interaction, providing a venue for lectures, and with corresponding conditions and equipment. The authors appreciate all the participants for their active involvement. We also acknowledge all the diabetes experts from the hospital affiliated with Central South University for their valuable lectures and consultation. The study was supported by the China Medical Board (CMB) Fund (11-085).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Jianping W, Linong J, Weiping J, et al. Standards of care for type 2 diabetes in China. Diabetes Metab Res Rev. 2016;32(5):442–458. doi:10.1002/dmrr.2827
3. Yong L. Epidemiology and research advances in diabetes mellitus in China. J Chongqing Med Univ. 2015;40(7):1042–1045.
4. International Diabetes Federation [webpage on the Internet]. IDF Diabetes Atlas 2017.
5. Shen X, Vaidya A, Wu S, Gao X. The diabetes epidemic in China: an integrated review of national surveys. Endocr Pract. 2016;22(9):1119–1129. doi:10.4158/EP161199.RA
6. Ing CT, Zhang G, Dillard A, et al. Social support groups in the maintenance of glycemic control after community-based intervention. J Diabetes Res. 2016;2016:7913258. doi:10.1155/2016/7913258
7. Egbujie BA, Delobelle PA, Levitt N, Puoane T, Sanders D, van Wyk B. Role of community health workers in type 2 diabetes mellitus self-management: A scoping review. PLoS One. 2018;13(6):e0198424. doi:10.1371/journal.pone.0198424
8. Health and Family Planning Commission of the People’s Republic of Chi-na. [webpage on the Internet]. National Basic Public Health Service Standa-Rds (Version 2011). Available from: http://www.gov.cn/zwgk/2011-05/24/content_1870181.htm.
9. General Office of the State Council. [webpage on the Internet]. General Office of the State Council on Issuing the Medium-and Long-Term Plan for the Control of chronic Diseases in China (2017–2025). Available from: http://www.gov.cn/zhengce/content/2017-02/14/content_5167886.htm.
10. Chinese Diabetes Society. National office for primary care. National guidelines for the prevention and control of diabetes in primary care (2018). Chin J of Intern Med. 2018;57(12):885–893.
11. Jingxian W. Measuring inequalities in the demographical and geographical distribution of physicians in China: generalist versus specialist. Int J Health Plann Manage. 2018;33(4):860–879. doi:10.1002/hpm.2539
12. Kristensen MA, Thorsen T. Increasing shortage of general practitioners in social deprived Danish communities. Ugeskr Laeger. 2014;176(11):V08130497.
13. DePue JD, Dunsiger S, Seiden AD, et al. Nurse-community health worker team improves diabetes care in American Samoa: results of a randomized controlled trial. Diabetes Care. 2013;36(7):1947–1953. doi:10.2337/dc12-1969
14. Houweling ST, Kleefstra N, van Hateren KJ, Groenier KH, Meyboom-de Jong B, Bilo HJ. Can diabetes management be safely transferred to practice nurses in a primary care setting? A randomised controlled trial. J Clin Nurs. 2011;20(9–10):1264–1272. doi:10.1111/j.1365-2702.2010.03562.x
15. Kim KB, Kim MT, Lee HB, Nguyen T, Bone LR, Levine D. Community health workers versus nurses as counselors or case managers in a self-help diabetes management program. Am J Public Health. 2016;106(6):1052–1058. doi:10.2105/AJPH.2016.303054
16. Whitehead LC, Crowe MT, Carter JD, et al. A nurse-led interdisciplinary approach to promote self-management of type 2 diabetes: a process evaluation of post-intervention experiences. J Eval Clin Pract. 2017;23(2):264–271. doi:10.1111/jep.12594
17. Trento M, Basile M, Borgo E, et al. A randomised controlled clinical trial of nurse-, dietitian- and pedagogist-led group care for the management of type 2 diabetes. J Endocrinol Invest. 2008;31(11):1038–1042. doi:10.1007/BF03345645
18. Vas A, Devi ES, Vidyasagar S, et al. Effectiveness of self-management programmes in diabetes management: A systematic review. Int J Nurs Pract. 2017;23(5). doi:10.1111/ijn.12571
19. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):2–4.
20. Stellefson M, Dipnarine K, Stopka C. The chronic care model and diabetes management in US primary care settings: a systematic review. Prev Chronic Dis. 2013;10:E26. doi:10.5888/pcd10.130016
21. Gammon D, Berntsen GK, Koricho AT, Sygna K, Ruland C. The chronic care model and technological research and innovation: a scoping review at the crossroads. J Med Internet Res. 2015;17(2):e25. doi:10.2196/jmir.3547
22. Ni YX, Liu SZ, Li JP, Diao YS, Dong T, Tao L. Effects of nurse-led team management on type 2 diabetes patients in the community. Hu Li Za Zhi. 2017;64(2):76–87. doi:10.6224/JN.000028
23. Jingjun Z, Ning L, Xiaomei L, et al. Development of diabetes self management scale and checkout of its reliability and validity. CNR. 2014;28(10):3578–3580.
24. American Diabetes Association. Standards of medical care in diabetes-2014. Diabetes Care. 2014;37(Supplement 1):S14–S80.
25. International Diabetes Federation. Global guideline for type 2 diabetes. Diabetes Res Clin Pract. 2014;104(1):1–52. doi:10.1016/j.diabres.2012.10.001
26. Li S, Xiaohui G. Introduction of the guidelines on nursing and education of diabetes mellitus in China. Chin J Diabetes. 2010;18(4):310.
27. American Diabetes Association. Third-party reimbursement for diabetes care, self-management education, and supplies. Diabetes Care. 2014;37(Supplement 1):S118–S119. doi:10.2337/dc14-S118
28. Beck J, Greenwood DA, Blanton L, et al. 2017 National standards for diabetes self-management education and support. Diabetes Care. 2017;43(5):449–464.
29. Miyamoto S, Dharmar M, Fazio S, Tang-Feldman Y, Young HM. mHealth technology and nurse health coaching to improve health in diabetes: protocol for a randomized controlled trial. JMIR Res Protoc. 2018;7(2):e45. doi:10.2196/resprot.9168
30. Philis-Tsimikas A, Walker C, Rivard L, et al. Improvement in diabetes care of underinsured patients enrolled in project dulce: a community-based, culturally appropriate, nurse case management and peer education diabetes care model. Diabetes Care. 2004;27(1):110–115. doi:10.2337/diacare.27.1.110
31. Yuan C, Lai CW, Chan LW, Chow M, Law HK, Ying M. The effect of diabetes self-management education on body weight, glycemic control, and other metabolic markers in patients with type 2 diabetes mellitus. J Diabetes Res. 2014;2014:789761.
32. Hughes MM, Yang E, Ramanathan D, Benjamins MR. Community-based diabetes community health worker intervention in an underserved Chicago population. J Community Health. 2016;41(6):1249–1256. doi:10.1007/s10900-016-0212-8
33. Kane EP, Collinsworth AW, Schmidt KL, et al. Improving diabetes care and outcomes with community health workers. Fam Pract. 2016;33(5):523–528. doi:10.1093/fampra/cmw055
34. Jaipakdee J, Jiamjarasrangsi W, Lohsoonthorn V, Lertmaharit S. Effectiveness of a self-management support program for Thais with type 2 diabetes: evaluation according to the RE-AIM framework. Nurs Health Sci. 2015;17(3):362–369. doi:10.1111/nhs.12198
35. Massimi A, De Vito C, Brufola I, et al. Are community-based nurse-led self-management support interventions effective in chronic patients? Results of a systematic review and meta-analysis. PLoS One. 2017;12(3):e0173617. doi:10.1371/journal.pone.0173617
36. Paz-Pacheco E, Sandoval MA, Ardena GJ, et al. Effectiveness of a community-based diabetes self-management education (DSME) program in a rural agricultural setting. Prim Health Care Dev. 2017;18(1):35–49. doi:10.1017/S1463423616000335
37. Hailu FB, Hjortdahl P, Moen A. Nurse-led diabetes self-management education improves clinical parameters in Ethiopia. Front Public Health. 2018;6:302. doi:10.3389/fpubh.2018.00302
38. National Health Commission of the People’s Republic of China. [webpage on the Internet]. National Basic Public Health Service Standards (The Third Edition), Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/04/20170417104506514.pdf.
39. General Office of the State Council. [webpage on the Internet]. Outline of the National Medical and Health Service System Planning (2015–2020), Available from: http://www.gov.cn/zhengce/content/2015-03/30/content_9560.htm.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.