")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Fathers’ Experiences of Being Present at an Unplanned Out-of-Hospital Birth: A Qualitative Study
Authors Jarneid H , Gjestad K , Røseth I , Dahl B
Received 14 July 2020
Accepted for publication 24 September 2020
Published 23 October 2020 Volume 2020:13 Pages 1235—1244
DOI https://doi.org/10.2147/JMDH.S272021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Henriette Jarneid,1 Kristin Gjestad,1 Idun Røseth,1,2 Bente Dahl1
1Centre for Women’s, Family and Child Health, Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg N-3603, Norway; 2Department of Child and Adolescent Mental Health, Telemark Hospital, Skien, Norway
Correspondence: Bente Dahl Email [email protected]
Purpose: The purpose of this study was to investigate fathers’ experiences of being present at an unplanned birth outside a maternity facility.
Materials and Methods: This was a qualitative interview study with 12 fathers from six of Norway’s eleven counties. All had been present at an unplanned out-of-hospital birth in 2015– 2020. Data were analyzed using systematic text condensation.
Results: The data analysis resulted in four themes. The first theme described the fathers’ stress and worry and how they managed to keep a cool head and think rationally in a totally unprepared situation. The second theme described the fathers’ need for help and the reassuring feeling provided by contact with health professionals. The third theme described how the birth increased the father’s attachment to his partner and baby, while the fourth theme described fathers’ feelings of exclusion and their reactions following the birth.
Conclusion: Fathers’ perceived lack of expertise and their fear of complications led to stress, worry and anxiety, but support from health personnel provided reassurance and control. Many fathers experienced mastery, pride and joy after the birth, but when arriving at hospital, they felt rejected and wished that maternity care staff had approached them to talk about the experience.
Keywords: born before arrival, experience, father, out-of-hospital birth, qualitative
Introduction
The number of unplanned out-of-hospital births is increasing in many countries.1 In Norway, there were 153 unplanned home births in 2018, while 171 women gave birth on their way to hospitaI in the same year.2 Unplanned births outside a maternity facility include all births that occur unintentionally for women who are not planning a home birth. Reasons may vary from a birth that occurs sooner than expected to a long and difficult journey to the nearest hospital. Due to increased centralization of maternity facilities in Norway, the risk of not arriving in time has increased.1 This means that more women give birth without the help of a midwife or nurse, and in many cases, the woman’s partner has to assist with the birth.
Studies show that women who have an unplanned out-of-hospital birth often experience the birth as dramatic.3,4 Ambulance personnel who have to assist women in childbirth feel unprepared and lack the necessary knowledge and experience.5,6 We have found no previous studies dealing with fathers’ experience of being present at such unplanned births. There are, however, studies of fathers’ experiences of planned home births when the midwife did not arrive in time,7 and of fathers’ experiences of potentially traumatic births in maternity units.8–10 These studies reveal that childbirth is often perceived as frightening and challenging. They also show that fathers are often confused about their role and concerned about the health of both mother and child, while also feeling a need to hide their own feelings to protect their partner during the birth. A lack of information and support during the birth process can adversely affect the father’s mental health, and he may have to deal with difficult emotions in the postpartum period.7,11,12
The World Health Organization (WHO) principles for perinatal care state that the care should be directed at the needs of the woman’s partner in addition to those of the woman and child.13,14 This highlights the need to provide care to fathers before, during and after the birth. The aim of the present study was to explore fathers’ experiences of being present at an unplanned out-of-hospital birth. Enhanced knowledge in this area can help to identify care needs of fathers present at this type of birth.
Materials and Methods
We chose a qualitative study design as this is suitable when there is little research on the topic and the purpose of the study is to enhance understanding of human experience.15 The Standards for Reporting Qualitative Research (SRQR) consisting of 21 items was followed when preparing the manuscript.16
Recruitment
We used social media to recruit a convenience sample17 of twelve fathers. We created a Facebook page with information about the study. Within a few days, we received about 20 inquiries from fathers who wanted to participate, and 14 of them met our inclusion criteria. After 12 interviews, we considered our data to be sufficiently rich to shed light on our research topic and we therefore decided to terminate our data collection. The recruitment process is described in Figure 1.
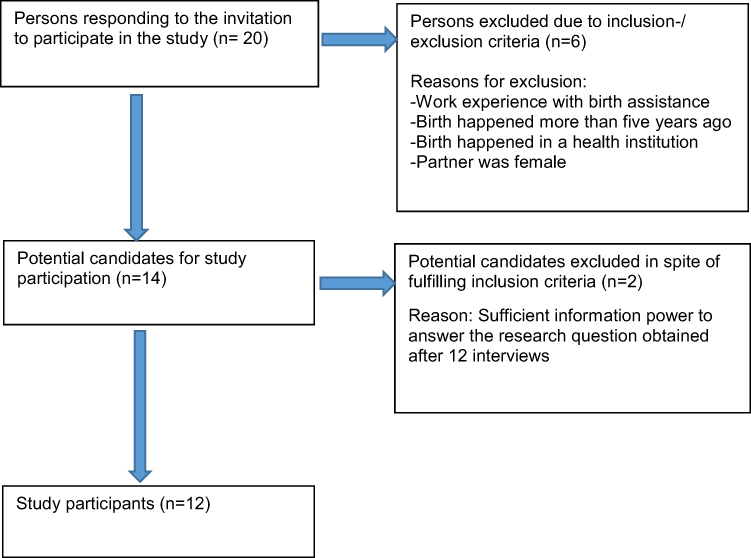 |
Figure 1 Participant recruitment process. |
Participants
We included fathers who had experienced an unplanned out-of-hospital birth in Norway during the past five years (2015–2020), if it was a term birth without complications. Further inclusion criteria were that the fathers spoke Norwegian and were capable of giving consent. Fathers with work experience of birth assistance were excluded. The fathers who participated in the study were aged 34–51 (average 40 years), and were all of Norwegian ethnicity. Three of them were first-time fathers, while the other nine had previously fathered children. They had varying levels of education and lived in six of Norway’s eleven counties.
Data Collection and Analysis
We conducted individual semi-structured interviews in January 2020.18 The first and second authors conducted all the interviews. Eight were face-to-face and four were online via video call. The interviews lasted from 12 to 43 minutes (average 29 minutes). Two of the interviews were relatively short, at 12 and 15 minutes. However, since these contained relevant information, we chose to include them in the study. We used an interview guide (Table 1), and began all the interviews with an open question in which the fathers were encouraged to talk about what happened on the day their child was born. They were then asked what they felt and thought when they realized that the birth would take place outside hospital. They were also asked if health professionals offered them a talk or debriefing in the first days after the birth. The interviews had no time limit, and the fathers were only interrupted when there was a need for elaboration or clarification. The interviews were audio recorded and transcribed verbatim.
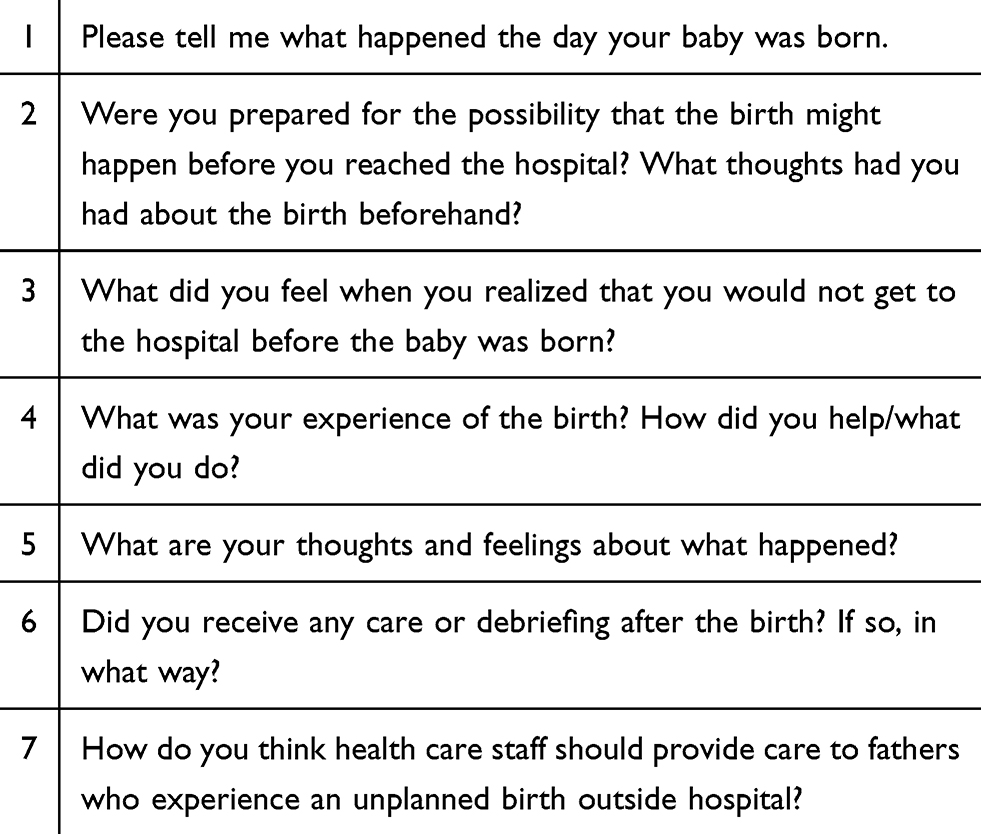 |
Table 1 Interview Guide |
The data were analyzed using systematic text condensation, a strategy for thematic cross-case analysis consisting of four steps.19 The analysis was performed by the first and second authors. It was then discussed and revised by all authors. First, we read all the interviews to gain a general idea of the material. Here, we found preliminary themes in the text, such as stress, chaos, gratitude, mastery and joy. We then read the text line by line and identified meaning units, ie, parts of the text that contained information relevant to our research topic. The meaning units were sorted into code groups. We then sorted the material in each code group into subgroups and condensed these. The code groups and subgroups are presented in Table 2. Finally, we summarized the knowledge from the condensates, ie, artificial quotations using the participants’ words, into an analytical text and used quotes to illustrate the text.
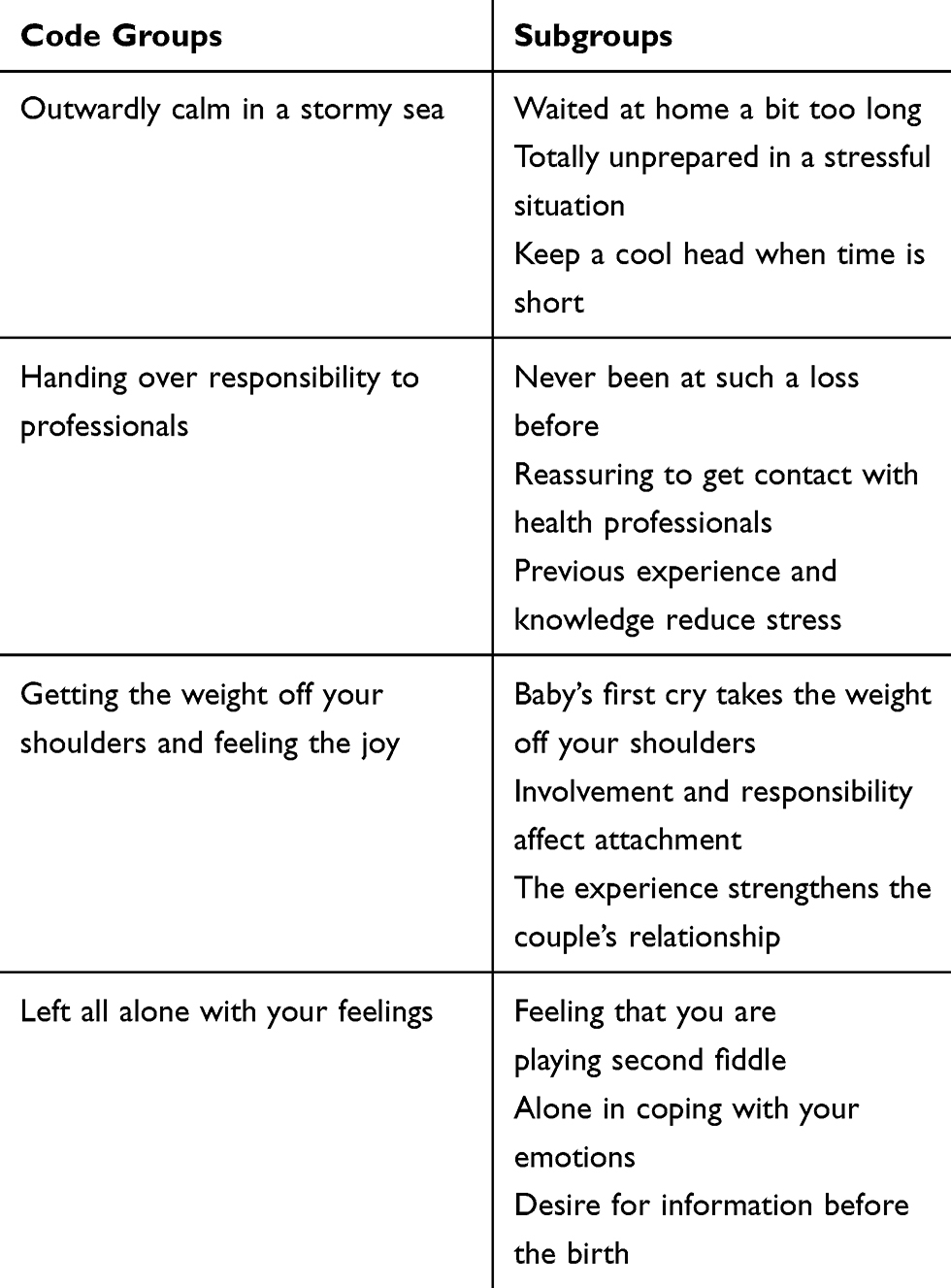 |
Table 2 Code Groups and Subgroups from the Analysis Process |
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki.20 It was approved by the Norwegian Center for Research Data (NSD: 808,536) and assessed by the Regional Committee for Medical and Health Research Ethics to be outside the scope of the Health Research Act (REK: 78,467). The informants received written and oral information about the study, and consented to participate before the interviews started. The informed consent included the use of anonymized responses. They were informed that participation was voluntary and that they could withdraw from the study at any time without having to provide a reason.
Participants were encouraged to contact their GP for a talk after the interviews if they experienced an emotional reaction as a result of their participation in the study. However, all the fathers found it pleasant to talk about the event, and none of them needed a further talk. It may have been significant that the interviewers were health professionals who aim for an empathetic approach in contact with people.
Results
The data analysis resulted in four themes. The first theme described the fathers’ worry about complications, and how they managed to keep a cool head and think rationally in a totally unprepared situation. The second theme described the fathers’ need for help, and the reassuring feeling of meeting health professionals. The third theme described how the birth increased the fathers’ attachment to their baby and partner. The fourth topic described the fathers’ feeling of exclusion and their reactions after the birth.
Outwardly Calm in a Stormy Sea
The fathers described several reasons for not reaching the hospital in time. For some, the distance to the hospital was the main factor, while others did not expect the birth as the baby was not due for a few more weeks. Others had imagined that giving birth would be more painful, and did not realize it had already started. One father said he realized what was happening but his partner did not. He tried to hurry her off to the hospital, but the birth took place sooner than they had imagined and they had to stay where they were. One first-time father said he had contacted the hospital when they suspected the birth had started, but the midwife told him on the phone that it would take time and that there was no need to go to the maternity ward yet. A second-time father said they were sent home from hospital twice for the previous birth. His partner did not want to go through that again, so they waited a little too long at home this time. He described it as follows:
“As this was the second birth, we kept comparing it to the first time. So we were a bit more relaxed than the first time, when we went in there a bit too soon when she started her contractions. We were sent home twice the first time (…) So we were very, like … ok, fine, let’s wait and see what happens. We’ve been here before, like.” (…) (Interview 8)
All the fathers were unprepared for the birth to take place outside hospital, and most experienced the situation as chaotic. They found that their focus and attention had changed and described the experience as overwhelming and surreal. Some described what happened as a feeling of being “outside themselves” or having “tunnel vision”, where time ran away from them and the birth took place beyond their control. Most were worried that complications would occur, and some were afraid of dropping the baby on the floor. To see the baby’s head emerge was a frightening experience. They were also frightened by the sight of the umbilical cord around the baby’s neck and they were unable to examine it closely. They just saw that the baby was purple and seemed lifeless. They felt overwhelmed by stress and unable to put into words what they were feeling in the situation, and in retrospect, they had difficulty in remembering how they thought and felt in the situation. They said there were no words to describe what they had experienced.
“You’re driving and then suddenly you see the baby being born and bumping down onto the floor next to you. I’m dead certain I’ll never in my life get a bigger shock than that … a traumatic experience, but still a fantastic thing that happened. You can’t beat that!” (Interview 3)
Many of the fathers described being able to stay calm in potentially stressful situations. Some said that although the birth was an extremely tense episode, they were not afraid or stressed. They had no time to become hysterical, as everything happened so quickly. Instead, they found that the adrenaline in their bodies enabled them to keep a cool head and think rationally. They were focused on the practical tasks and on doing the job right to prevent any harm. They felt that they were almost acting on instinct; they were completely focused on dealing with the situation and calling for help. When they realized they could not reach the hospital, they called the medical emergency number for assistance. They expressed a great mix of emotions, ranging from strong feelings of stress, worry and adrenaline to relief and joy when everything turned out well. Having an obvious job to do gave them a sense of direction and a feeling that they could help, which mitigated their overwhelming and insecure feelings. One of the participants explained how the adrenaline helped him to focus more sharply:
“ … You think more logically (…) when you get that boost of adrenaline, you’re more focused on what’s happening and you just get it done.” (Interview 2)
Handing Over Responsibility to Professionals
When the baby was being born, the fathers felt helpless. They did not want to be all alone in the situation, and hoped the ambulance would arrive as soon as possible, as they did not know what to do after the birth. Although their partner and the baby seemed to be fine, not all the fathers were sure about that. Most of them wanted to get to hospital as soon as possible, and felt that they lacked the necessary expertise and knowledge to handle the situation. One father described it as follows:
“I’ve never felt at such a loss in my entire life (…) You’re sort of completely useless because you don’t know anything about this and … things sort of follow their natural course.” (Interview 3)
Most fathers were on the phone to the emergency services during the event, and some were also talking to midwives. The health care staff seemed professional, calm and friendly. This reassured the fathers and gave them a sense of security and control. The professionals gave the fathers instructions and prepared them for what would happen and what they had to do. Some fathers pointed out that they did not feel afraid when they had this support on the phone. They were also reassured to hear that the ambulance was close, so there was little time to worry about something going wrong. Others, however, felt stressed until health professionals were physically present, and several felt relieved and reassured when the ambulance arrived. Then they could calm down and focus on taking care of their partner. They had done their best and could hand over the work to skilled professionals, and get to the hospital quickly if necessary. Many felt that the hospital was the safest place, and appreciated the emergency service and the health care professionals. However, some fathers did not feel confident that the ambulance staff had sufficient expertise, and thought they spent too long on various tasks. They also expressed concern that there was limited equipment in the ambulance. When a midwife was present, the fathers felt more relaxed and on arrival at the hospital, everything was the way it was supposed to be.
“When we got to the hospital, things kind of fell into place, because everything was there (…) I felt more comfortable there, with the people around that you’d expected to be there for the birth. Things did in fact go well, so you could begin to feel happy about it.” (Interview 10)
The fathers had all imagined that the birth would take place in secure surroundings with qualified personnel present, not in the bathroom at home or on the floor of a rather dirty car on the way to the hospital. But for most of them, the experience was quite different from their expectations. Those who had previously been present at births found that a useful experience; they therefore knew to a certain extent what would happen and what to do when the baby was born. One father said he felt sure the baby would be fine if he assisted the delivery, and many fathers had learned that fast births usually go well. This prior knowledge helped to decrease the fathers’ stress and anxiety. Fathers who had children already stated that the experience would probably have been different if the baby born outside hospital had been their first child.
“So I think the experience I had from our first child was very useful in that situation.” (Interview 12)
Getting the Weight off Your Shoulders and Feeling the Joy
Many fathers described being worried until the baby cried, and felt relieved when that happened. One father stated that it felt like a weight off his shoulders. All the fathers were grateful that the birth had been quick and without complications. Some experienced helping to deliver the baby as an extra kind of euphoria. They felt that they had made the best of the situation, and had a sense of mastery. They were proud and felt lucky. Most people thought it was a good experience, and many of the fathers who helped with the delivery said they would not mind doing it again. However, not all fathers felt this sense of mastery. Some pointed out that they did not want to assist the birth in the same way again, as there was no guarantee it would be equally successful the next time.
“It was a big relief when I heard baby’s first cry, of course.” (Interview 10)
Some fathers felt more strongly attached to the baby because they had assisted the delivery themselves. Others were unsure whether the birth itself and the circumstances surrounding it had any effect on their attachment to the baby, and believed their increased responsibility in the post-birth period had a greater influence on their relationship to the child. These fathers were more involved in responsibility for the baby because their partner had some health problems and complications postpartum, which meant that the fathers spent more time alone with the baby. One father explained it in this way:
“Having to do so much afterwards, things that the mother normally does, that definitely made me more attached (…) So that made it more like ‘we’ for things that are usually ‘mother-and-baby’ things.” (Interview 7)
For several fathers, the birth was an important experience they would not have wanted to miss. They felt a mixture of relief, happiness and love as their partner took the baby to her breast. They described their partner as “really brilliant”. They thought she had done a great job, and they loved and were proud of her. Two fathers pointed out that the experience had helped to strengthen their relationship. One father said that in the period after the birth he received many compliments from his family and friends for his effort. He himself felt that it was his partner who deserved the praise, as she had done the biggest job. He described a deep love and pride in her and the baby he had helped to deliver. He compared the feeling to his wedding day when his bride approached him down the aisle:
“(…) you feel a lump in your throat, and you feel some tears coming (…) like an explosion of warm feelings (…) Yes, the deep love you feel and the close bond to your wife, that means a lot … It’s a love that … It actually makes your whole marriage stronger, being able to achieve such great things together, like the birth of a baby.” (Interview 12)
Left All Alone with Your Feelings
Most fathers said they were not asked how they felt after the birth when they arrived at the hospital. There were no questions or offers of a follow-up talk, just a quick congratulation where they were told that they had done a good job. They said that the health care staff seemed busy, and some fathers felt rejected and unimportant. They were left with the feeling that there was no room for them. One father felt that he was playing second fiddle while all the focus was on the mother and child. Many were subsequently affected by the event, especially the first-time fathers whose partner was a first-time mother. Immediately after the birth, they did not understand what they needed; they stated that the hospital staff should have realized that they were having a difficult time and invited them to a follow-up talk. Not all the fathers needed this, but they all felt that the staff should have taken the time for a short chat with them while they were still in the hospital. Several fathers had talked a great deal about the situation with friends and family after the birth, which helped them to work through what had happened.
“They gave me lots of compliments because things had gone so well. Well, that was nice, of course, but there was no more talk about it (…) We could have had a talk (…) But none of them … because they had enough on their plate … it was very hectic (…) I thought it was weird that no one asked, because just then I really wanted to talk about it.” (Interview 10)
Several fathers found it emotional but also useful to talk about the experience after the event. Some said they were almost in tears, as it was an emotional experience and a lot to take in. Many experienced the birth as stressful, and some also described it as traumatic. One father said that even though he had worked through the experience, he would never forget his mental image of the baby on the car floor. Another reported having had an episode of breathlessness and palpitations a few weeks after the birth. He later realized that this had been a panic attack. One father related how he had ended up alone in a hotel room after the birth as there was no room for him in the hospital. Suddenly he felt terribly alone and lay there staring at the ceiling. The adrenaline had left his body, and he felt a cold shiver as he thought about what had happened that evening. However, as everything went well, the birth was still a positive experience for most fathers.
The fathers missed information on what to do in the case of an out-of-hospital birth. If they had been told during pregnancy care that this could happen, they would have been better prepared for possibly having to assist the delivery. This could have helped them to make a plan in the back of their mind on what would have to be done, focusing on the most important elements. One father wished that pregnancy courses could include brief information on what to expect if the birth takes place outside a maternity facility, and on the appearance of a newborn baby. Others suggested that all fathers should be given a small booklet with clear and easy-to-read information on what to do if you have to help with the birth yourself, preferably with drawings and instructions in order of priority. One father described it as follows:
“It might have been nice to have … a kind of little booklet, you know, that tells you a bit about what actually happens if you have to help deliver the baby yourself. They never gave me that at any of those … well, the thought never occurred to me that I’d have to do it either. But obviously in a situation like that, it would definitely have been useful to have some sort of checklist.” (Interview 8)
Discussion
Most studies dealing with unplanned childbirth outside hospital are based on the woman’s experience. This study helps to shed light on the event from the father’s perspective. Many fathers found they were overwhelmed by the situation and were worried that something might be wrong with the baby. They felt anxiety, great responsibility and helplessness during the birth, but joy and pride when everything turned out well. The support and instructions they received from health professionals before they reached the hospital were of great help. However, at the hospital, they felt like outsiders, and would have liked to talk to staff about the birth. In the following sections, we will discuss these findings in the light of relevant research.
All of the fathers in our study were unprepared for an out-of-hospital birth. Many were overwhelmed, stressed, and afraid that something was wrong or that complications would occur. Some pointed out that the experience was traumatic and unreal for them. Studies of fathers’ experiences of potentially traumatic births in maternity facilities show similar findings, as for instance an acute caesarian section, preterm birth or other adverse birth event.9,21 It also emerges that the unexpected experience of a birth that deviates from the norm can negatively affect the father’s mental health.8 To have to assist in the delivery of one’s own baby may be considered an experience of a birth that deviates from the norm. Several fathers described the experience as frightening, and told of the shock they felt. Fathers describe similar experiences when the midwife arrives too late for a planned home birth.7 Like some of the fathers in our study, they were emotionally affected by the event for a long time afterwards.
Many of the fathers mentioned their lack of knowledge and skills, and several felt helpless and at a loss. We see similar findings in the study by Elmir and Schmied,8 where some fathers felt powerless and helpless at being unable to fulfil their expected role of protecting their partner and the newborn baby. The fathers in our study who had previously been present at a birth stated that their prior experience reassured them. They were better prepared for what would happen than the first-time fathers. Nevertheless, all of the fathers were anxious to get help from health professionals, and expressed relief when the ambulance finally arrived. Most of the fathers stated that the birth was fast and that health care personnel arrived quickly. When help came, however, several fathers felt that the ambulance staff spent too long on various tasks. Time seemed to be going slowly. This can probably be seen in the context of their feeling of security. How secure they felt seemed to depend on how much help they received. Some fathers did not feel confident that the ambulance personnel had sufficient expertise. This is supported by findings from previous studies showing that ambulance staff themselves expressed feelings of nervousness and adrenaline, and were unsure of how to deal with out-of-hospital births.5,6 They worried about being responsible for the lives of mother and child and felt that they lacked the training, skills and knowledge to assist women in childbirth. The uncertainty shown by some ambulance staff made the fathers in our study want to get their partner and baby to hospital as soon as possible to receive help from better qualified health personnel. In cases where a midwife was present during the birth, the fathers felt more relaxed. Fathers often have confidence in a midwife, and studies show that the presence of a midwife is of great importance for a good birth experience.22,23
The fathers’ descriptions of feeling overwhelmed and insecure can be understood from a phenomenological perspective as an existential experience in which their everyday understanding of the world is challenged.24 The fathers’ experience contains aspects of what Gusich25 describes as an emotional trauma that arises when a situation is experienced as unimaginable and unreal, which also involves an altered state of consciousness and experience of time. Some of the fathers stated that they particularly found the expulsion phase to be an extreme experience beyond the scope of their imagination. Having an experience that is so “out of this world” that they can hardly take it in is in some sense like temporarily refusing to accept the situation. Some described how they almost held their breath until the baby cried or until clinicians had taken over the responsibility. They described entering an altered state of consciousness where their focus was narrowed down to the traumatic situation, such as the baby’s head looking purple and dead, or the umbilical cord coiled around its neck. Some felt that their subjective experience of time changed as the situation slowly unfolded before them, while others found that everything was happening very quickly. All these dimensions of a crisis reaction made it difficult for the fathers to fully understand and process the birth experience in the situation. At the same time, they were often able to act purposefully and be practically oriented, which could diminish their feeling of helplessness. Processing the experience often took time in the post-birth period, and was facilitated by a successful birth and the fathers receiving acknowledgement for having mastered the situation.
Internationally, the importance of family-centered care during pregnancy, childbirth and maternity has been highlighted.14,26 Here it is stated that care must also meet the needs of the woman’s partner, not merely those of the woman and the child. Both mothers and fathers want and need to talk about their experiences of childbirth.8,27–29 Talking about how the situation was experienced can be of great importance in processing the event.30 In spite of this, studies show that health professionals offer fathers little inclusion and care.9,31 Few men who experience traumatic births are given the opportunity to talk to health personnel after the birth.8 Similar findings were described in our study, where the fathers reported that clinicians mainly focused on the mother and child. Several felt rejected and unimportant, even though they understood that the main focus should be on their partner and baby. This may have hurt their feelings all the more because many of these fathers were the main person to care for mother and baby during the birth, but when the health professionals became involved, they immediately felt like a person of little importance. They felt they had been involved in something very special, and wanted acknowledgement by the health personnel. The professionals, for their part, indicated that the situation was normal and nothing out of the ordinary.
Studies show that mothers and fathers find dialogue with health professionals following childbirth to be a positive and meaningful experience.27,28 Fathers find that good communication can help them to process the event.9 However, another study found that structured interviews after childbirth do not greatly reduce the risk of post-traumatic stress and depressive symptoms.32 It is the ability of health professionals to tune in to the other, to be emotionally available, and to accept and acknowledge the other’s thoughts and feelings, which is important in helping the other to process challenging or traumatic events.29,33 All the fathers in our study wanted health care staff to offer a post-birth conversation to all fathers who had experienced out-of-hospital births. Regardless of the effect of this dialogue, the very offer to talk about the birth can help fathers feel more included and fulfil their wishes and needs.
Women with unplanned out-of-hospital births also express disappointment at health professionals’ lack of empathy and consideration for what they have been through.3,4 Lack of support may have been one of the reasons why some of the fathers’ partners suffered from various forms of postpartum complaints and complications, which in turn meant that the fathers had to shoulder much of the responsibility for the baby. However, this increased responsibility may have improved the attachment between father and child, because increased involvement is of great importance for parent–child attachment.30,34 But it may also have meant that the fathers had to repress their own feelings in order to care for the baby. Furthermore, some fathers may make an effort to avoid showing signs of weakness and keep their feelings to themselves to maintain their masculinity,9 which may make it difficult for health professionals to understand what these fathers actually need. In addition, a brief stay in the maternity ward may mean that fathers show no reaction to what has happened until they return home.35 This highlights the importance of health professionals including the woman’s partner in their care, even though he may not ask for it or show any sign that he needs it.
Adequate knowledge about childbirth and the possibility to process the event afterwards can give fathers a positive birth experience,9,36 and also provide a good start to the paternal role. Our study reveals a need for information, support and advice before, during and after childbirth for fathers who experience an unplanned out-of-hospital birth. The fathers in this study called for information about the appearance of a newborn baby, and what to do if they had to help to deliver the child themselves. Maternity care staff should relate to fathers in a way that makes them feel more prepared, cared for and included, which is also in line with the WHO recommendations on family-centered care.14 However, the study provides no information on the health professionals’ perceptions of the care they provided to these fathers. Further research should therefore address clinicians’ experiences when meeting fathers who have been present and assisted during an unplanned out-of-hospital birth.
Strengths and Limitations
Reflexivity deals with the researcher’s background and preunderstanding.37 Our relationship with the field under study could be a strength and a limitation. The authors all have a background in health care science. Three are midwives with clinical practice from maternity wards, theoretical knowledge of the topic and interest in fathers’ experiences of childbirth. One also teaches on a master’s degree course in midwifery. Another is a clinical psychologist, teaches midwife students and has research interests related to the topic. This enabled us to study the phenomenon from different perspectives and with different theoretical understandings. Our preunderstandings may have influenced the data collected and how the data were interpreted. However, some of the findings have surprised us, which suggests that we may have succeeded in bracketing our preunderstandings.
The internal validity38 of the study was strengthened by the choice of a qualitative study design with individual semi-structured interviews. This approach is suitable to shed light on people’s experiences, and formed a sound basis for the fathers to provide comprehensive and detailed information on how they experienced the birth. We used an interview guide that helped to provide structure and an overview during the interviews. Long distances made it difficult to conduct all interviews face-to-face, and some were therefore conducted via video call. This may have weakened the internal validity, as the context was not the same for all informants. We recruited a convenience sample to ensure that we had informants willing to participate in the study. This may have resulted in relevant information being lost because people who volunteer to participate in a study often differ from those who do not. Interviews were conducted up to five years after the birth, which may also have diminished the internal validity, since some of the informants may not have remembered all the details of the event.
The external validity38 of the study was enhanced by including both first-time fathers and those with previous children, with variation in age, location and level of education. One weakness is that there were relatively few first-time fathers, since previous experience seems to be of great importance for the birth experience. However, we considered that the sample had sufficient information power to shed light on our research topic.39 Our sample consisted solely of ethnic Norwegian fathers. The inclusion of fathers with different cultural backgrounds might have strengthened the external validity by providing alternative experiences, knowledge and traditions related to childbirth. However, the results of our study suggest how an unplanned complication-free birth outside a maternity facility may be experienced by fathers in countries with a similar health care system as in Norway.
Conclusion
The fathers experienced a variety of feelings in connection with the birth. Their perceived lack of the necessary knowledge and skills, coupled with fear of complications, led to feelings such as stress, worry and anxiety. The support they received from the emergency services gave them increased reassurance and control, especially in cases where a midwife was present. Several fathers experienced a high degree of mastery and pride, as well as the joy of stronger attachment to their partner and the baby they had helped to deliver. However, they felt excluded and rejected by health personnel at the hospital after the birth, and many stated that it might have been helpful to talk about the birth, and wished that the maternity care staff had taken such an initiative. Despite the lack of support, most fathers described the birth as a positive experience.
Acknowledgments
We would like to thank all the fathers who contributed to this study by sharing their experiences.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Engjom H, Morken N, Norheim O, Klungsoyr K. Availability and access in modern obstetric care: a retrospective population-based study. BJOG. 2014;121(3):290–299. doi:10.1111/bjo.12510
2. Norwegian Institute of Public Health, undated. Medisinsk fødselsregister – statistikkbank: fødte og fødsler per institution [Medical birth register, statistics bank: children born and births by institution]. Norwegian. Available from: http://statistikkbank.fhi.no.
3. Erlandsson K, Lustig H, Lindgren H. Women’s experience of unplanned out-of-hospital birth in Sweden – a phenomenological description. Sex Reprod Healthc. 2015;6(4):226–229. doi:10.1016/j.srhc.2015.06.002
4. Vik ES, Haukeland GT, Dahl B. Women’s experiences with giving birth before arrival. Midwifery. 2016;42:10–15. doi:10.1016/j.midw.2016.09.012
5. Persson A-C, Engström Å, Burström O, Juuso P. Specialist ambulance nurses’ experiences of births before arrival. Int Emerg Nur. 2019;43:45–49. doi:10.1016/j.ienj.2018.08.002
6. Vagle H, Haukeland GT, Dahl B, Aasheim V, Vik ES. Emergency medical technicians’ experiences with unplanned births outside institutions: a qualitative interview study. Nurs Open. 2019;6(4):1542–1550. doi:10.1002/nop2.354
7. Jouhki M-R, Suominen T, Åstedt-Kuri P. Supporting and sharing – home birth: fathers’ perspective. Am J Mens Health. 2015;9(5):421–429. doi:10.1177/1557988314549413
8. Elmir R, Schmied V. A meta-ethnographic synthesis of fathers’ experiences of complicated births that are potentially traumatic. Midwifery. 2016;32:66–74. doi:10.1016/j.midw.2015.09.008
9. Etheridge J, Slade P. Nothing’s actually happened to me: the experiences of fathers who found childbirth traumatic. BMC Pregnancy Childbirth. 2017;80(1). doi:10.1186/s12884-017-1259-y
10. Vallin E, Nestander H, Wells MB. A literature review and meta-ethnography of fathers’ psychological health and received social support during unpredictable complicated childbirths. Midwifery. 2019;68:48–55. doi:10.1016/j.midw.2018.10.007
11. Kerstis B, Nohlert E, Öhrvik J, Widarsson M. Association between depressive symptoms and parental stress among mothers and fathers in early parenthood: a Swedish cohort study. Ups J Med Sci. 2016;121(1):60–64. doi:10.3109/03009734.2016.1143540
12. Singley DB, Edwards LM. Men’s perinatal mental health in the transition to fatherhood. Prof Psychol Res Pr. 2015;46(5):309–316. doi:10.1037/pro0000032
13. Chalmers B, Mangiaterra V, Porter R. WHO principles of perinatal care: the essential antenatal, perinatal, and postpartum care course. Birth. 2001;28(3):202–207. doi:10.1046/j.1523-536x.2001.00202.x
14. World Health Organization (WHO). Second meeting of focal points on reproductive health/health of women and children in the European Region; 2002. Available from: https://apps.who.int/iris/bitstream/handle/10665/108363/E71412.pdf?sequence=1&isAllowed=y.
15. Schneider Z, Whitehead D, Lobiondo-Wood G, Haber J. Nursing and Midwifery Research: Methods and Appraisal for Evidence-Based Practice.
16. O’Brien B, Harris IB, Beckman T, Reed D, Cook D. Standards for reporting qualitative research. A synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:https://doi:10.1097/ACM.0000000000000388
17. Patton MQ. Qualitative Research & Evaluation Methods.
18. Kvale S, Brinkmann S. InterView: En Introduction Til Det Kvalitative Forskningsinterview [Interviews: An Introduction to Qualitative Research Interviewing]. Norwegian: Copenhagen: Hans Reitzel; 2002.
19. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40(8):795–805. doi:10.1177/1403494812465030
20. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects; 2018. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
21. Stefana A, Padovani E, Biban M. Fathers’ experiences with their preterm babies admitted to neonatal intensive care unit: a multi‐method study. J Adv Nurs. 2018;74(5):1090–1098. doi:10.1111/jan.13527
22. Hildingsson I, Cederlöf L, Widén S. Fathers’ birth experience in relation to midwifery care. Women Birth. 2011;24(3):129–136. doi:10.1016/j.wombi.2010.12.003
23. Thies-Lagergren L, Johansson M. Intrapartum midwifery care impact Swedish couple’s birth experiences – a cross-sectional study. Women Birth. 2019;32(3):213–220. doi:http://doi.10.1016/j.wombi.2018.08.163
24. Husserl E. Cartesian Meditations: An Introduction to Phenomenology. The Hague: Martinus Nijhoff Publishers; 1960.
25. Guisch G. A phenomenology of emotional trauma: around and about the things themselves. Hum Stud. 2012;35:505–518. doi:10.1007/s10746-012-9247-8
26. International Confederation of Midwives (ICM). Core document: philosophy and model of midwifery care; 2014. Available from: https://internationalmidwives.org/assets/files/definitions-files/2018/06/eng-philosophy-and-model-of-midwifery-care.pdf.
27. Baxter JD, McCourt C, Jarrett PM. What is current practice in offering debriefing services to post partum women and what are the perceptions of women in accessing these services: a critical review of the literature. Midwifery. 2014;30(2):194–219. doi:10.1016/j.midw.2013.12.013
28. Olin R-M, Faxelid E. Parents’ needs to talk about their experiences of childbirth. Scand J Caring Sci. 2003;17(2):153–159. doi:10.1046/j.1471-6712.2003.00105.x
29. Stolorow RD. A phenomenological-contextual, existential, and ethical perspective on emotional trauma. Psychoanal Rev. 2015;102(1):123–138. doi:10.1521/prev.2015.102.1.123
30. Brudal L. Psykiske Reaksjoner Ved Svangerskap, Fødsel Og Barseltid [Psychological Reactions to Pregnancy, Childbirth and Maternity]. Norwegian: Bergen: Fagbokforlaget; 2000.
31. Solberg B, Glavin K. Fedre ønsker en mer aktiv rolle i svangerskapsomsorgen og på helsestasjonen [Fathers want a more active role in pregnancy care and at the mother and child clinic]. Sykepl Forsk. 2018;13. doi:10.4220/Sykepleienf.2018.72006
32. Sheen K, Slade P. The efficacy of ‘debriefing’ after childbirth: is there a case for targeted intervention? J Reprod Infant Psychol. 2015;33(3):308–320. doi:10.1080/02646838.2015.1009881
33. Røseth I, Bongaardt R. A phenomenological understanding of postpartum depression and its treatment. In: Phenomenology and the Social Context of Psychiatry. Social Relations, Psychopathology, and Husserl’s Philosophy. Englander M, editor. London: Bloomsbury Academic; 2018:121–135.
34. Røseth I, Bongaardt R, Lyberg A, Sommerseth E, Dahl B. New mothers’ struggles to love their child. An interpretative synthesis of qualitative studies. Int J Qual Stud Health Well-Being. 2018;13(1):1490621. doi:https://dx.doi.10.10802F17482631.2018.1490621
35. Gustin LW. Psykologi for Sykepleiere [Psychology for Nurses]. Norwegian: Bergen: Fagbokforlaget; 2016.
36. Norwegian Ministry of Health and Care Services. En gledelig begivenhet: om en sammenhengende svangerskaps-, fødsels- og barselomsorg [A happy event: integrated pregnancy, childbirth and postnatal care]. (Meld. St. 12 (20082009)); 2009. Norwegian. Available from: https://www.regjeringen.no/contentassets/25a45886201046488d9c53abc0c8ad3a/no/pdfs/stm200820090012000dddpdfs.pdf.
37. Malterud K. The art and science of clinical knowledge: evidence beyond measures and numbers. Lancet. 2001;358(9279):397–400. doi:10.1016/S0140-6736(01)05548-9
38. Malterud K. Kvalitative Forskningsmetoder for Medisin Og Helsefag [Qualitative Research Methods for Medicine and Health Sciences].
39. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.