")
Back to Journals » Cancer Management and Research » Volume 14
Family History of Cancers Increases Risk of Renal Cell Carcinoma in a Chinese Population
Authors Xing S , Ruan X, Huang J, Yan J, Lin W, Huang J, Liu J, Huang D, Na R, Xu D
Received 1 June 2022
Accepted for publication 18 August 2022
Published 30 August 2022 Volume 2022:14 Pages 2561—2568
DOI https://doi.org/10.2147/CMAR.S376784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Siwei Xing,1,* Xiaohao Ruan,1,* Jingyi Huang,1,* Jiaqi Yan,1 Wenhao Lin,1 Jinlun Huang,1 Jiacheng Liu,1 Da Huang,1 Rong Na,2 Danfeng Xu1
1Department of Urology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Division of Urology, Department of Surgery, Queen Mary Hospital, The University of Hong Kong, Hong Kong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rong Na, Division of Urology, Department of Surgery, Queen Mary Hospital, The University of Hong Kong, 102 Pok Fu Lam Road, Hong Kong, People’s Republic of China, Email [email protected] Da Huang, Department of Urology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, 197 Ruijin 2nd Road, Shanghai, 200025, People’s Republic of China, Email [email protected]
Purpose: To explore the impact of family history (FH) on renal cell carcinoma (RCC) and its pathological subtype clear cell RCC (ccRCC) in a Chinese population; a significant association has previously been determined not only in familial cancer syndrome but also in sporadic cases in western populations.
Methods: Consecutive patients with kidney tumors from October 2017 to May 2021 at a tertiary hospital in Shanghai were enrolled in the study. Demographic and clinical information was collected, including age, gender, FH (positive or negative, types of cancers, degree of relatives, etc.), pathological diagnosis, and Fuhrman grades.
Results: A positive FH of any cancer was observed in 26.5% of the RCC patients, while only 16.8% patients with benign kidney tumor were found to have a positive FH. A strong correlation was observed between FH of any cancers in first-degree relatives and RCC (odds ratio [OR]=4.60, 95% confidence interval [CI]: 1.95– 10.85, P=5.50× 10− 5) or ccRCC (OR=4.63, 95% CI: 1.95– 11.02, P=9.63× 10− 5). In subgroup analysis, FH of digestive cancers was significantly associated with RCC (OR=4.42, 95% CI: 1.35– 14.51, P=0.005) or ccRCC (OR=4.14, 95% CI: 1.25– 13.75, P=6.84× 10− 4). Similar results were found in multivariate analyses. However, no significant association was observed between FH and age at onset.
Conclusion: FH was an independent risk factor for RCC and ccRCC in this Chinese population. FH of any cancer in first-degree relatives and FH of digestive cancers were found to be the most significant risk factors for kidney cancers.
Keywords: Chinese population, family history, renal cell carcinoma, risk factor, multivariate regression analysis
Introduction
As the seventh most common malignant carcinoma worldwide, the incidence of kidney cancer has been increasing rapidly over the past few years.1 Among the different pathological types, renal cell carcinoma (RCC) may account for over 80% of kidney cancers.2 In contrast to the increased exploration of innovative treatment targets and prognostic models, knowledge on the risk factors for and predisposition to the disease has barely evolved.
Risk factors including age, gender, smoking, and alcohol intake have been found to be correlated with RCC.3–6 An excess accumulation of adipose tissue, particularly visceral adipose tissue, has also been observed in the development of RCC,7–9 which makes obesity another general risk factor. Although most cases are sporadically diagnosed, a family history (FH) of cancer should also be considered as a valuable factor, especially since certain genetic mutations in genes such as Von Hippel–Lindau (VHL), fumarate hydratase, and succinate dehydrogenase B have established associations with RCC.10–12
In addition, a positive FH in relatives of RCC patients may be associated with disease onset and outcome. For example, sequential research from the Swedish public health service found that patients with a positive FH had a 4.58-fold higher risk (95% confidence interval [CI]: 2.87–6.94) of RCC and could also suffer from subsequent cancer after the onset of RCC.13,14 Studies regarding the association between FH and RCC risk have mostly focused on western populations.4,13 Unfortunately, related research based on an eastern population, such as Japanese15 or Korean,16 focused on genotyping and genetic mutations and did not provide explicit data on patients’ epidemiological features.
To our knowledge, no similar study has been published based on a Chinese population to date. This prompted us to explore the association between FH and the clinical onset of RCC and provide evidence for risk evaluation in affected individuals. In the present study, we evaluated the association between FH of different types of kidney cancers at different levels of relatives and the risk of RCC, using a consecutive surgical cohort, in Chinese patients.
Patients and Methods
Study Population and Study Design
This is a retrospective study based on a group of consecutive patients with kidney tumors undergoing partial or radical surgery from October 2017 to May 2021 at Ruijin Hospital, a tertiary hospital in Shanghai, China. The study was approved by the institutional review board of Shanghai Ruijin Hospital (central IRB no. KY2016-343, 24 Nov 2016, version 03), and written informed consent was obtained from each participant. Patients were excluded from the present study if they were uncertain about either the type of cancer of a positive FH or the overall situation of the FH of cancer.
A total of 484 cases were finally included in the present study. To ensure data integrity and legitimacy, FH of cancers was collected by investigators through a structured questionnaire (positive or negative, types of cancers, degree of relatives, etc.).
A first-degree FH was defined as having direct blood relatives with a cancer history. FH of digestive cancers was defined as positive FH of gastric and colonic cancers. Other detailed demographic and clinical information was collected before and after surgery, including age, gender, pathological diagnosis, and Fuhrman grades.
All surgical specimens were independently examined and graded by two experienced pathologists. Carcinoma of Fuhrman grade 1–2 was defined as the low-grade group, while that of Fuhrman grade 3–4 was defined as the high-grade group.17,18
Statistical Analyses
The chi-squared test or Fisher’s exact test was used in univariable analysis for categorical variables. Multivariable logistic regression analysis was conducted to further evaluate the associations. Survival analysis for disease-free survival (age at onset) was evaluated by the log-rank test (Kaplan–Meier). A two-tailed P<0.05 was considered statistically significant. All statistical analyses were performed using GraphPad Prism (version 6.00 for Windows, GraphPad Software) and SPSS Statistics (IBM Corp., IBM SPSS Statistics for Windows, version 24.0, released 2016).
Results
Demographic Observation Revealed a Higher Co-Morbidity of Positive FH with RCC
Demographic characteristics and baseline information of the study cohort are shown in Table 1. Among 484 cases, 389 (80.4%) were pathologically diagnosed as RCC, and the rest were diagnosed as benign tumors, such as complicated renal cyst, angiomyolipoma, or oncocytoma. Of the patients with RCC, 311 were diagnosed as clear cell renal cell carcinoma (ccRCC), which accounted for 79.9% of all RCC. Detailed information on the subtypes of RCC is presented in Table 2. The median age of the patients was 57 years (interquartile range [IQR]: 14–89 years).
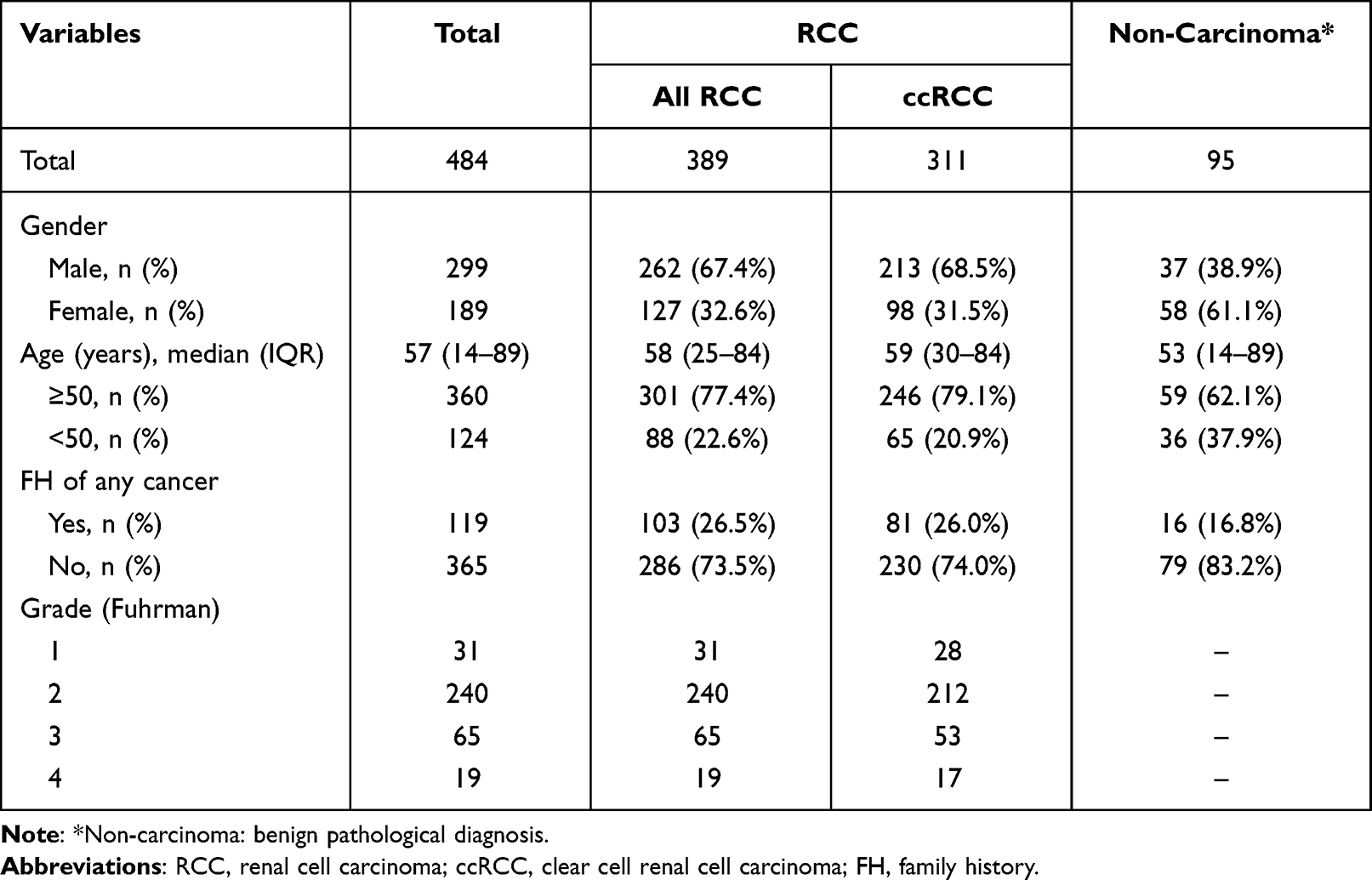 |
Table 1 Demographic Characteristics and Baseline Information of the Study Cohort |
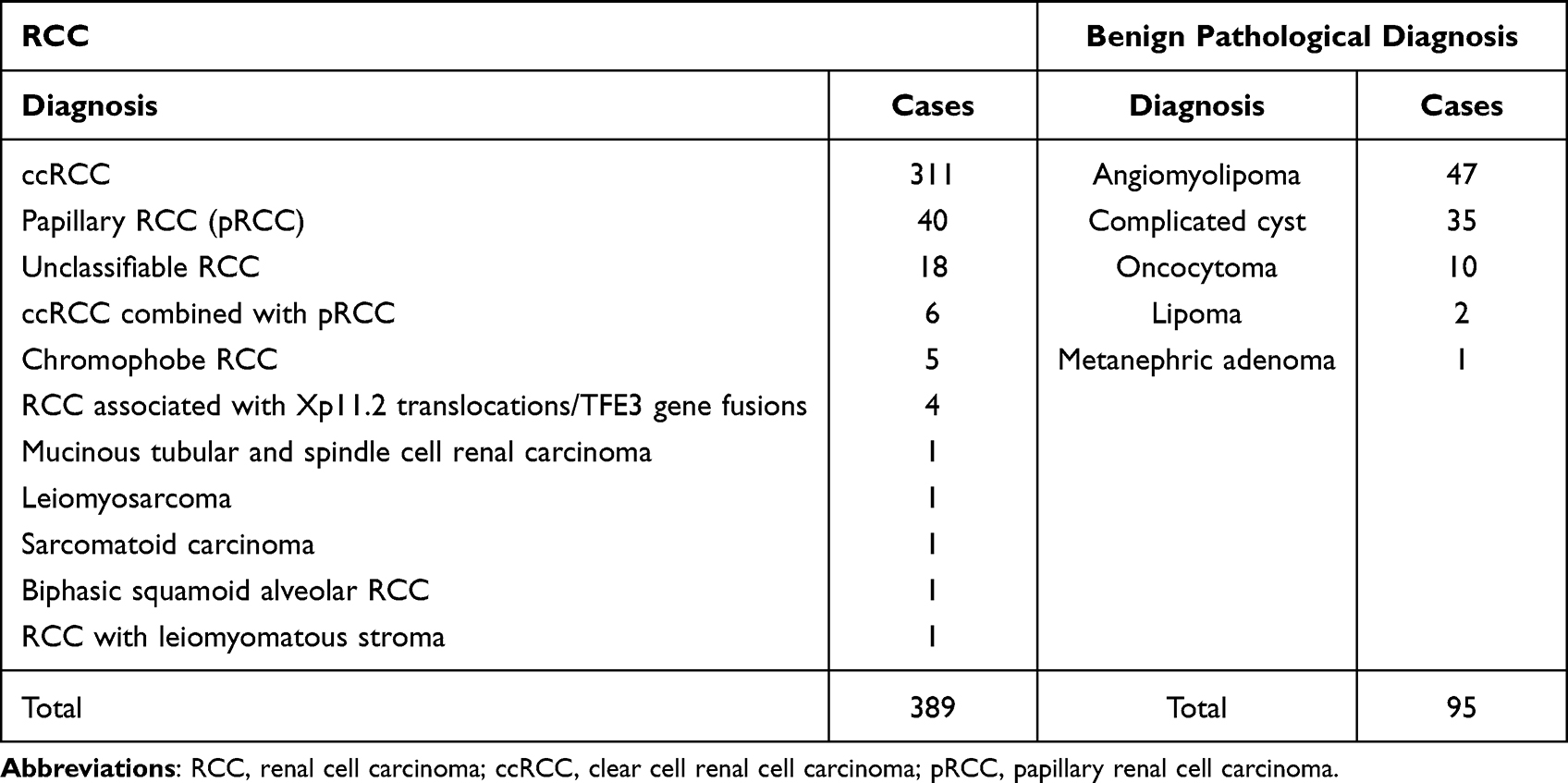 |
Table 2 Subtype Information of RCC and Benign Pathological Diagnosis |
A positive FH of any cancer was observed in 26.5% of the RCC patients (26.0% of ccRCC), while only 16.8% patients with a benign kidney tumor were found to have a positive FH (Table 1). Further stratification analyses discovered that most of the positive FHs presented in a first-degree relative (98 out of 119, 82.4%). Regarding types of cancers, seven cases of RCC (1.8% positive rate) had a positive FH of RCC, six of whom were ccRCC patients (1.9% positive rate), while none of the patients with a benign kidney tumor had a positive FH of RCC (Table 3). Digestive cancers were established as the most frequent co-morbidity.
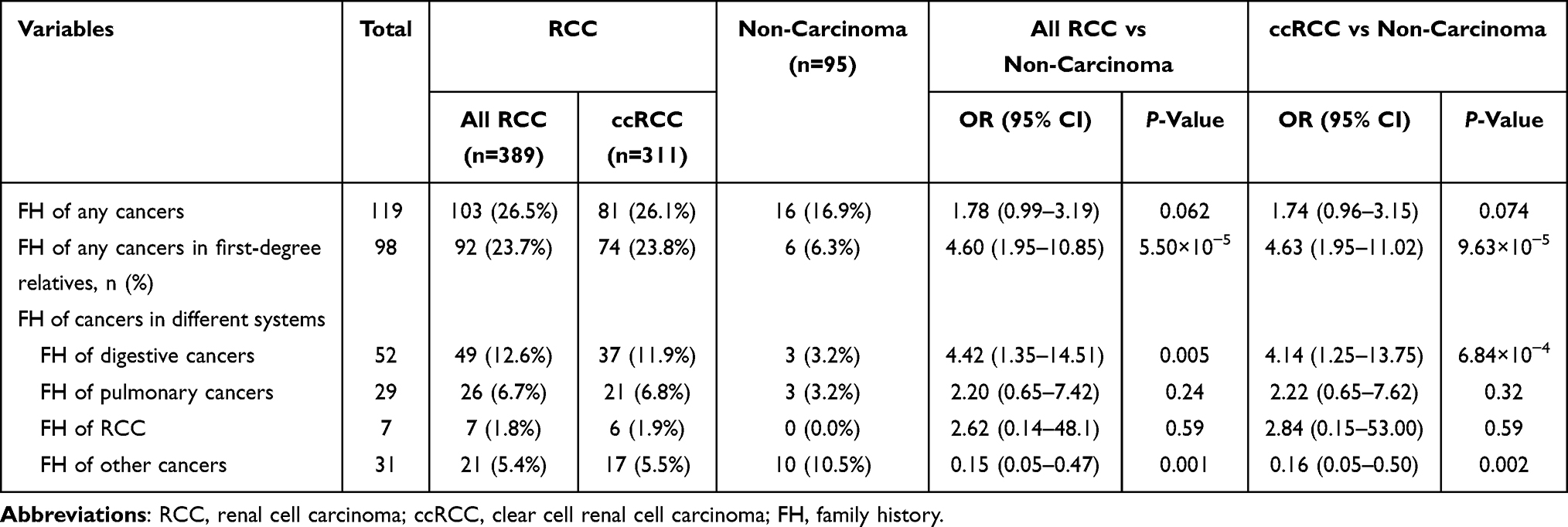 |
Table 3 Association Between Family History and RCC |
FH Could Be Considered as an Independent Risk Factor for RCC
We then set out to evaluate the influence of FH on RCC incidence, and notably the most common pathological type, ccRCC.
FH of any cancers increased the risk of RCC (odds ratio [OR]=1.78, 95% CI: 0.99–3.19, P=0.062) and ccRCC (OR=1.74, 95% CI: 0.96–3.15, P=0.074) (Table 3) at marginally significant levels. The percentages of RCC patients and ccRCC patients with a positive FH of any cancer in first-degree relatives were 23.7% (OR=4.60, 95% CI: 1.95–10.85, P=5.50×10−5) and 23.8% (OR=4.63, 95% CI: 1.95–11.02, P=9.63×10−5), respectively, which were significantly higher than those in patients with benign tumors (6.3%) (Table 3). These results indicate that a positive FH in first-degree relatives may be a risk factor for RCC and ccRCC.
We then evaluated whether a positive FH of specific types of cancers could be associated with the risk of RCC or ccRCC. We observed that 12.6% of the RCC patients (OR=4.42, 95% CI: 1.35–14.51, P=0.005) and 11.9% of the ccRCC patients (OR=4.14, 95% CI: 1.25–13.75, P=6.84×10−4) had a positive FH of digestive cancers, which was significantly higher than in patients with benign tumors (3.2%) (Table 3). No association was observed between FH of other specific cancer types and RCC or ccRCC.
To further examine whether FH could be an independent risk factor for RCC, we performed multivariate logistic regression analyses adjusting for gender and age (Table 4). The results suggested that FH of any cancer was independently and significantly associated with RCC (OR=1.85, 95% CI: 1.01–3.37, P=0.045). This association was even stronger in patients with a positive FH in first-degree relatives (OR=4.36, 95% CI: 1.83–10.42, P=0.001). In addition, a positive FH of digestive cancers was an independent risk factor for RCC (OR=4.02, 95% CI: 1.21–13.36, P=0.023). We discovered that their influence was also significant in the sole pathological type ccRCC (Table 4).
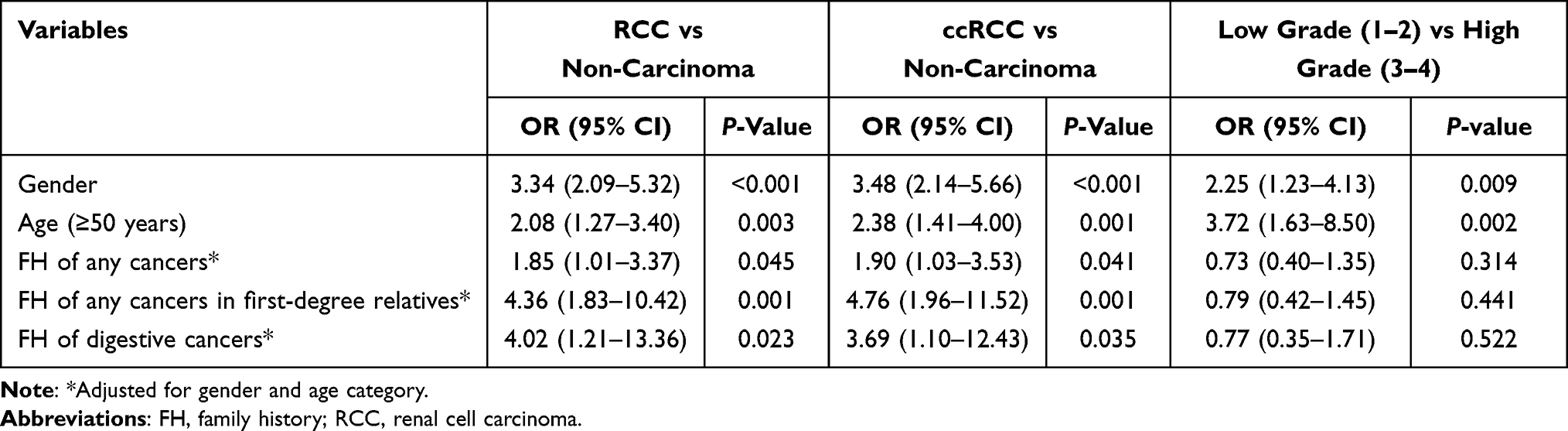 |
Table 4 Multivariate Logistic Regression Analyses Evaluating the Association Between FH and RCC |
FH Did Not Share an Association with Age at Onset or Pathological Grading
Next, we investigated whether FH could also serve as a prognostic indicator. We employed the following two common factors for assessment: pathological grading and age at onset of the disease.
We performed multivariate logistic regression analysis to evaluate the influence of FH on prediction of pathological grades. However, after adjustment for gender and age, no significant association was observed between FH and high Fuhrman grade (grade 3–4) of RCC (Table 4).
We then analyzed the association between FH and age at onset. No significant association was found between early age at onset (<50 years), a potential indicator of poorer prognosis, and FH (all P>0.05) (Table 5) through Kaplan–Meier analyses. Moreover, survival analyses did not find any significant link between FH and age at onset (all P>0.05) (Figure 1A–F).
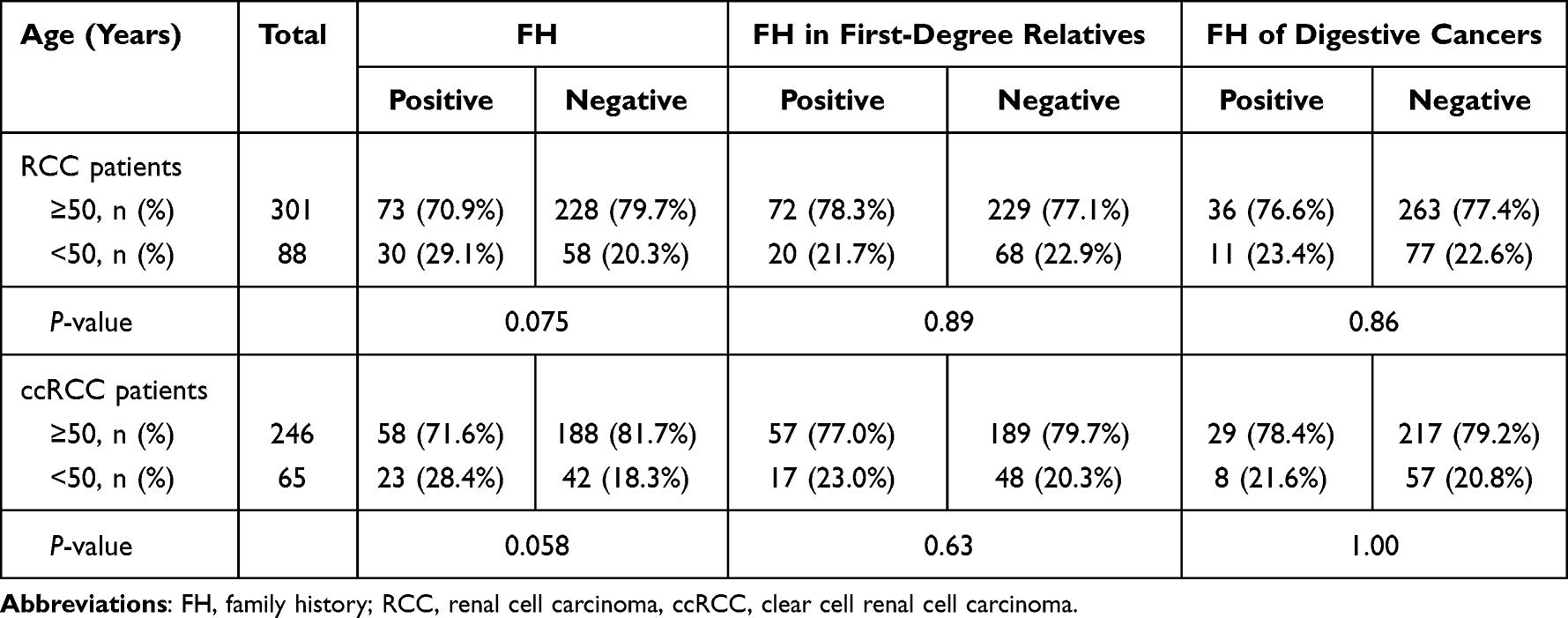 |
Table 5 Association Between FH and Age at Onset |
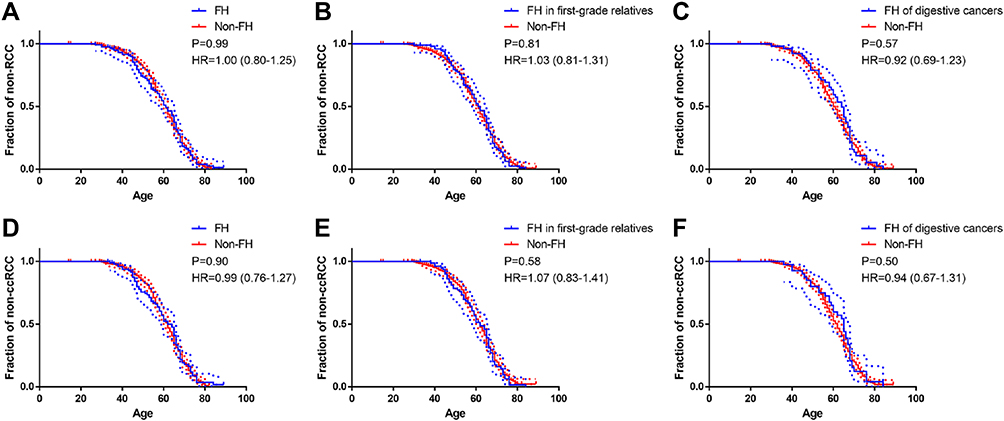 |
Figure 1 Results of Kaplan–Meier survival analyses: (A) association between FH of all cancer and age at onset of RCC; (B) association between FH in first-degree relatives and age at onset of RCC; (C) association between FH of digestive cancer and age at onset of RCC; (D) association between FH of all cancer and age at onset of ccRCC; (E) association between FH in first-degree relatives and age at onset of ccRCC; (F) association between FH of digestive cancer and age at onset of ccRCC. P-values obtained by log-rank test. HR obtained by log-rank test, with 95% CI in parentheses. Abbreviations: FH, family history; RCC, renal cell carcinoma; ccRCC, clear cell renal cell carcinoma; HR, hazard ratio; CI, confidence interval. |
Discussion
This is the first time that the association between FH and RCC has been evaluated in a Chinese population. We found that:1 FH of any cancers was a risk factor for RCC and ccRCC;2 FH of any cancers in first-degree relatives and FH of digestive cancers were stronger risk factors for RCC and ccRCC;3 and FH was not associated with pathological grade (Fuhrman grade) or age at onset (early onset). Significant correlations are summarized and visualized in Figure 2.
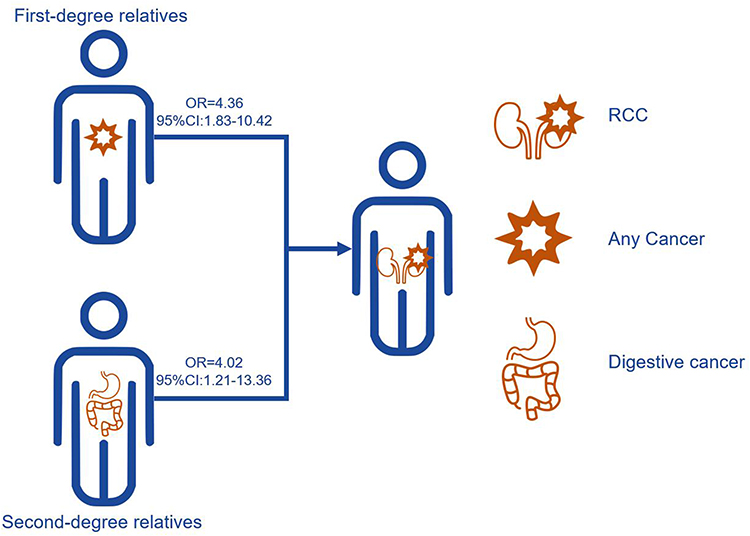 |
Figure 2 Graphic presenting significant correlations between FH and RCC. FH of any cancers in first-degree relatives and FH of digestive cancers are considered as risk factors for RCC. Abbreviations: FH, family history; RCC, renal cell carcinoma; OR, odds ratio; CI, confidence interval. |
Our findings are consistent with those of previously published results from other countries in people of other ethnicities.4,13,16 However, the importance of positive FH in patients with renal tumors has not yet been discussed thoroughly. Most of the related literature focused on hereditary patterns of RCC types, such as VHL disease,19 hereditary papillary RCC,11 and hereditary leiomyomatosis.16,20 In our study, we did not come across many familial cases of RCC, although all positive FHs of RCC were found in patients with malignant renal tumors. Instead, we established that FH is an independent risk factor for RCC.
Unlike for other cancers, a positive FH did not have an influence on age at onset. For example, a positive FH of prostate cancer (PCa) or BRCA‐related cancers was related to an earlier age at onset of PCa.21 Besides, FH of colorectal cancer (CRC) was also considered to be associated with early-onset CRC (age <50 years).22 The unusual discovery in this study of RCC has not been reported in any other epidemiological research, to our knowledge.
The positive association of first-grade-relative FH with RCC was easy to interpret considering that genetic or epigenetic modifications are more likely to be passed on to the patient. We also observed that most of the FH (~90%) was in first-degree relatives. This could be due to the family planning (one-child) policy in China in the past decades that limited the size of the family.23 This could lead to a lack of second-degree relatives. Another possible reason could be the poor medical infrastructure, absence of disease registration, and insufficient vital statistics before the 2000s,24 which made it difficult for people and medical workers to capture information on FH (people died without the exact reason being known).
Our results also showed FH of digestive cancers to be a significant risk factor for RCC in this Chinese population. Several reviews mentioned an observational link between gastrointestinal stromal tumor and onset of RCC, indicating the potential predisposition syndromes and advocating clinical phenotyping and characterization of genotypic features.25,26 Familial digestive cancers are likely to be related to Lynch syndrome, sharing a close link with malfunction of mismatch repair (MMR) genes in the DNA repair process.27–29 Evidence also showed that expression of MMR genes was downregulated in RCC30 and specific gene expression was related only in ccRCC.31 However, whether MMR gene mutations are associated with RCC in the Chinese population is still unknown, and is worthy of further investigation given the relatively high incidence of digestive cancers in China. Another speculation could arise from the fact that obesity, and specifically the accumulation of adipose tissue in individuals, is considered a risk factor for both RCC and CRC,9,32 and investigations at a molecular level may be required to confirm this.
Our study has several limitations. First, as this was a single-center retrospective study, our results may not represent the entire Chinese population. However, as this center is a tertiary hospital in Shanghai, people from all over the country come here to seek its services. Secondly, the number of cases was relatively small in the present study, because we only included cases with a concrete demographic FH, which was collected through clinical interview. This may have introduced an inevitable bias of omission and also resulted in a limited statistical power to observe some potential differences, for instance, the relationship between FH and age at onset. Nevertheless, our study provides the first evidence on this topic based on a Chinese population. Further research in a larger population and necessary improvement of the study design, such as confirmation of the FH by histopathological examination, may help to advance and augment the findings of our study.
Abbreviations
FH, family history; RCC, renal cell carcinoma; ccRCC, clear cell renal cell carcinoma; OR, odds ratio; CI, confidence interval; IQR, interquartile rage; MMR, mismatch repair; IRB, institutional review board.
Data Sharing Statement
The data and materials generated and analyzed during the current study are available from Dr. Rong Na on reasonable request.
Ethics Approval
The research was carried out according to the principles set out in the Declaration of Helsinki 1964 and all subsequent revisions, and the relevant institutional review board (IRB) at Ruijin Hospital approved the study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
The patients or parent/guardian/next of kin (in the case of minors or deceased patients) provided written informed consent for the publication of any data and/or accompanying images.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (81772741, 81972405, and 81972645), Shanghai Youth Talent Support Program, and the Shanghai Sailing Program (22YF1440500).
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
2. Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017;15:804–834. doi:10.6004/jnccn.2017.0100
3. Padala SA, Barsouk A, Thandra KC, et al. Epidemiology of renal cell carcinoma. World J Oncol. 2020;11:79–87. doi:10.14740/wjon1279
4. Christensen MB, Wadt K, Jensen UB, et al. Exploring the hereditary background of renal cancer in Denmark. PLoS One. 2019;14:e0215725. doi:10.1371/journal.pone.0215725
5. Gansler T, Fedewa SA, Flanders WD, Pollack LA, Siegel DA, Jemal A. Prevalence of cigarette smoking among patients with different histologic types of kidney cancer. Cancer Epidemiol Biomarkers Prev. 2020;29:1406–1412. doi:10.1158/1055-9965.EPI-20-0015
6. Washio M, Mori M, Mikami K, et al. Risk factors for renal cell carcinoma in a Japanese population. Asian Pac J Cancer Prev. 2014;15:9065–9070. doi:10.7314/APJCP.2014.15.21.9065
7. Greco F, Cirimele V, Mallio C, Zobel B, Grasso R. Increased visceral adipose tissue in male patients with clear cell renal cell carcinoma. Clin Cancer Investig J. 2018;7(4):132. doi:10.4103/ccij.ccij_62_18
8. Greco F, Mallio CA, Grippo R, et al. Increased visceral adipose tissue in male patients with non-clear cell renal cell carcinoma. Radiol Med. 2020;125:538–543. doi:10.1007/s11547-020-01146-6
9. Greco F, Quarta LG, Grasso RF, Beomonte Zobel B, Mallio CA. Increased visceral adipose tissue in clear cell renal cell carcinoma with and without peritumoral collateral vessels. Br J Radiol. 2020;93:20200334. doi:10.1259/bjr.20200334
10. Gossage L, Eisen T, Maher ER. VHL, the story of a tumour suppressor gene. Nat Rev Cancer. 2015;15(1):55–64. doi:10.1038/nrc3844
11. Verine J, Pluvinage A, Bousquet G, et al. Hereditary renal cancer syndromes: an update of a systematic review. Eur Urol. 2010;58:701–710. doi:10.1016/j.eururo.2010.08.031
12. Woodward ER, Ricketts C, Killick P, et al. Familial non-VHL clear cell (conventional) renal cell carcinoma: clinical features, segregation analysis, and mutation analysis of FLCN. Clin Cancer Res. 2008;14:5925–5930. doi:10.1158/1078-0432.CCR-08-0608
13. Hemminki K, Li X. Age-specific familial risks for renal cell carcinoma with evidence on recessive heritable effects. Kidney Int. 2004;65:2298–2302. doi:10.1111/j.1523-1755.2004.00650.x
14. Chen T, Fallah M, Sundquist K, Liu H, Hemminki K. Risk of subsequent cancers in renal cell carcinoma survivors with a family history. Eur J Cancer. 2014;50:2108–2118. doi:10.1016/j.ejca.2014.05.003
15. Furuya M, Yao M, Tanaka R, et al. Genetic, epidemiologic and clinicopathologic studies of Japanese Asian patients with Birt-Hogg-Dube syndrome. Clin Genet. 2016;90:403–412. doi:10.1111/cge.12807
16. Seo JY, Ahn JY, Keam B, et al. Genotypic and phenotypic characteristics of hereditary leiomyomatosis and renal cell cancer syndrome in Korean patients. Ann Lab Med. 2021;41:207–213. doi:10.3343/alm.2021.41.2.207
17. Delahunt B, Eble JN, Egevad L, Samaratunga H. Grading of renal cell carcinoma. Histopathology. 2019;74:4–17. doi:10.1111/his.13735
18. Becker A, Hickmann D, Hansen J, et al. Critical analysis of a simplified Fuhrman grading scheme for prediction of cancer specific mortality in patients with clear cell renal cell carcinoma–Impact on prognosis. Eur J Surg Oncol. 2016;42:419–425. doi:10.1016/j.ejso.2015.09.023
19. Patel PH, Chadalavada RS, Chaganti RS, Motzer RJ. Targeting von Hippel-Lindau pathway in renal cell carcinoma. Clin Cancer Res. 2006;12:7215–7220. doi:10.1158/1078-0432.CCR-06-2254
20. Forde C, Lim DHK, Alwan Y, et al. Hereditary leiomyomatosis and renal cell cancer: clinical, molecular, and screening features in a cohort of 185 affected individuals. Eur Urol Oncol. 2020;3:764–772. doi:10.1016/j.euo.2019.11.002
21. Xu Y, Huang D, Wu Y, et al. Family history is significantly associated with prostate cancer and its early onset in Chinese population. Prostate. 2019;79:1762–1766. doi:10.1002/pros.23900
22. Gausman V, Dornblaser D, Anand S, et al. Risk factors associated with early-onset colorectal cancer. Clin Gastroenterol Hepatol. 2020;18:2752–9 e2. doi:10.1016/j.cgh.2019.10.009
23. Gietel-Basten S, Han X, Cheng Y. Assessing the impact of the “one-child policy” in China: a synthetic control approach. PLoS One. 2019;14:e0220170. doi:10.1371/journal.pone.0220170
24. Wei W, Zeng H, Zheng R, et al. Cancer registration in China and its role in cancer prevention and control. Lancet Oncol. 2020;21:e342–e9. doi:10.1016/S1470-2045(20)30073-5
25. Przybycin CG, Magi-Galluzzi C, McKenney JK. Hereditary syndromes with associated renal neoplasia: a practical guide to histologic recognition in renal tumor resection specimens. Adv Anat Pathol. 2013;20:245–263. doi:10.1097/PAP.0b013e318299b7c6
26. Agaimy A, Hartmann A. Uncovering hereditary tumor syndromes: emerging role of surgical pathology. Semin Diagn Pathol. 2018;35:154–160. doi:10.1053/j.semdp.2018.01.001
27. Sinicrope FA. Lynch syndrome-associated colorectal cancer. N Engl J Med. 2018;379:764–773. doi:10.1056/NEJMcp1714533
28. Biller LH, Syngal S, Yurgelun MB. Recent advances in Lynch syndrome. Fam Cancer. 2019;18:211–219. doi:10.1007/s10689-018-00117-1
29. Pellat A, Netter J, Perkins G, et al. Syndrome de Lynch : quoi de neuf? [Lynch syndrome: what is new?]. Bull Cancer. 2019;106:647–655. French. doi:10.1016/j.bulcan.2018.10.009
30. Deguchi M, Shiina H, Igawa M, Kaneuchi M, Nakajima K, Dahiya R. DNA mismatch repair genes in renal cell carcinoma. J Urol. 2003;169:2365–2371. doi:10.1097/01.ju.0000065668.19267.b4
31. Stoehr C, Burger M, Stoehr R, et al. Mismatch repair proteins hMLH1 and hMSH2 are differently expressed in the three main subtypes of sporadic renal cell carcinoma. Pathobiology. 2012;79:162–168. doi:10.1159/000335642
32. Roslan NH, Makpol S, Mohd Yusof YA. A review on dietary intervention in obesity associated colon cancer. Asian Pac J Cancer Prev. 2019;20:1309–1319. doi:10.31557/APJCP.2019.20.5.1309
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.