")
Back to Journals » Patient Preference and Adherence » Volume 16
Factors Related to Complying with Anti-TB Medications Among Drug-Resistant Tuberculosis Patients in Indonesia
Authors Yani DI , Juniarti N , Lukman M
Received 28 September 2022
Accepted for publication 13 December 2022
Published 17 December 2022 Volume 2022:16 Pages 3319—3327
DOI https://doi.org/10.2147/PPA.S388989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Desy Indra Yani, Neti Juniarti, Mamat Lukman
Lecturer, Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jatinangor, West Java, Indonesia
Correspondence: Desy Indra Yani, Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jatinangor, 45363, West Java Province, Indonesia, Tel +6222-7796647, Fax +6222-7796647, Email [email protected]
Background: A variety of factors influenced the decision of tuberculosis (TB) drug-resistant patients to continue treatment. The study aimed to analyze factors that influence complying with anti-TB medications in patients with TB drug resistance in Indonesia.
Patients and Methods: The study employed a cross-sectional approach and was conducted in various community health centers and polyclinics offering TB drug-resistant services in Bandung city, Indonesia. Participants were 79 patients with TB drug resistance who met the criteria during their treatment for TB drug resistance, were willing to be involved in the research, and accessed TB services in Bandung. Complying with anti-TB medications scale, TB Health Behaviors questionnaire, the family support questionnaire, the TB-Related Stigma Scale, and TB knowledge were used in this study. Data were analyzed using Spearman’s Rho.
Results: Health behavior (r = 0.36) was positively associated with complying with anti-TB medications, while family support, TB stigma, and knowledge were not related to treatment compliance.
Conclusion: Information on these factors will inform the development of models and modules for the prevention and control of TB drug resistance in Indonesia, which can later be used widely in Indonesia.
Keywords: compliance, drug resistance, health behaviors, pulmonary tuberculosis, treatment
Introduction
Mismanaged tuberculosis (TB) treatment and person-to-person transfer enhance multi-drug resistance. Multidrug-Resistant Tuberculosis (MDR-TB) is resistant to isoniazid and rifampin, the two most effective first-line medicines.1 Globally in 2020, 71% (2.1/3.0 million) of TB patients were tested for rifampicin resistance, representing a rise from 61% (2.2/3.6 million) in 2019 and 50% (1.7/3.4 million) in 2018.1 In addition, 132,222 cases of MDR/ Rifampicin-Resistant Tuberculosis (RR-TB) RR-TB and 25,681 cases of pre- Extensively Drug-Resistant TB (XDR-TB) or XDR-TB were identified, for a total of 157,903 patients.1 Ten countries, including Indonesia, accounted for 70% of the global disparity between MDR/RR-TB incidence and treatment in 2020.2 TB is treatable, but is ranked thirteenth in 2019’s leading causes of mortality worldwide.1 In 2018, 482,683 MDR/RR-TB patients were engaged in treatment, 32% of the five-year goal of 1.5 million (2018–2022) from the UN high-level meeting on TB for treatment targets. In 2018, the MDR/RR-TB treatment success rate was 60%, up from 50% in 2012.2 People diagnosed and started on treatment with drug-resistant TB in Indonesia in 2021 were 8268 and 5234, and both increased from last year by 4.4% and 0.038%, respectively. In addition, TB treatment success rate in Indonesia was 47% of those who started drug-resistant TB treatment in 2019.1 Compliance with anti-TB medications is essential for each patient’s recovery, preventing the spread of illness and reducing the emergence of extreme drug resistance.3
Patients’ decision to continue receiving MDR/RR TB treatment was affected by a variety of circumstances. Successful therapy was aided by self-motivation, knowledge of the illness and available treatments, counseling assistance, family support, nutritional support, and social support.4 According to service providers, nutritional support, family support, and social support all helped patients persevere with their treatments. The qualitative study revealed five themes related to the patients’ experience and conduct during therapy, namely, patients’ perceptions of the illness, patients’ perceived barriers, the variables that assist treatment adherence, patients’ desires regarding healing, and patients’ health-promoting behavior.5
Complying with anti-TB medications is associated with several characteristics, which have been classified into five factors, namely, patient factors, condition-related factors, treatment, socioeconomic, and health system factors. Side effects, social support, demography, education, and self-report of health are the primary determinants of medication use among latent TB patients.6 Poor treatment compliance of TB has been linked to younger age, lower BMI, and prior TB history.7
In studies on compliance with treatment in Indonesia, family support for MDR-TB8 and demanding access to healthcare, lack of TB knowledge, and treatment experience for drug-sensitive TB9 were associated with non-adherence during TB treatment. Studies on complying with anti-TB medications in patients taking sensitive medications and those with latent TB have been well publicized; however, studies on drug-resistant TB are scarce, particularly in Indonesia. Hence, efforts must be made to ensure effective compliance to the treatment because the optimal MDR-TB/RR-TB medication alone is insufficient. Therefore, this study aimed to analyze the factors that influence complying with anti-TB medications in patients with TB drug resistance in the city of Bandung, Indonesia. Knowledge of these factors can help health professionals and policymakers address what hinders medication compliance and improve the health outcomes of MDR-TB/RR-TB patients.
Materials and Methods
Study Design
The research method was correlation research with a cross-sectional approach.
Setting
The study was conducted in various settings including a Hospital in Bandung, the Lung Health Center in Bandung, 15 community health centers (Puskesmas) in the city of Bandung, and and three Puskesmas in Garut Regency. In Indonesia, Puskesmas are government-mandated community health centers. The term “Puskesmas” will be used throughout this paper. Puskesmas are administered by the Indonesian Ministry of Health and provide sub-district-level healthcare for the populace.
Participants
Drug-resistant TB patients from Bandung and Garut, Indonesia, were recruited using a convenience sampling technique. A nurse in each setting approached the potential subjects who met the inclusion criteria to ascertain their interest in this study. The study consisted of 76 drug-resistant TB patients who completed their clinical history. The inclusion criteria to identify eligible subjects were: must be older than 15 years of age, have confirmed diagnosis of drug-resistant TB, received drug-resistant TB medication and can write and read the Indonesian language.
Variables
Respondents and health characteristics of drug-resistant patients were assessed. In addition, Complying with anti-TB medications and its associated factors, which included health behaviors, family support, stigma, and TB knowledge, were measured in this study.
Measurement
This study used five instruments, namely, the Complying with anti-TB medications, the Tuberculosis health behaviors questionnaire, the family support questionnaire, The Tuberculosis-Related Stigma Scale, TB knowledge. Various participants’ demographic characteristics also included in the instrument.
Complying with anti-TB medications measure of medication-taking behavior consisting of five items.10 The response format was yes and no, ranging from 5 to 20.
A modified version of the tuberculosis health behaviors questionnaire created by Biswas (2010) based on related literature was utilized. Internal consistency of this questionnaire in Biswas’s study showed a Cronbach’s alpha coefficient of 0.76. There are 26 items and six sub-scales, including healthy food, physical activity, environmental hygiene, disease transmission prevention, and avoiding TB risk factors. The response format was a four-point Likert scale (never [1], occasionally [2], frequently [3], and always [4]). The range for the total score was 31 to 124. Higher ratings were indicative of greater adherence to healthy behaviors.10
The family support questionnaire was measured to evaluate perceived family support for pulmonary TB patients, comprising 41 questions. This questionnaire is composed of emotional anxiety, aid, and affirmation domains. Emotional anxiety included expressions of care (questions 1–5), encouragement (questions 6–10), and empathy (questions 11–15). The aid domain covered service (questions 16–20), money (questions 21–25), and information (questions 26–31). Affirmation included constructive feedback (questions 32–36) and acknowledgment (questions 37–41). On a four-point Likert scale, the received statements of family support were ranked according to their level of support: 1 = never; 2 = sometimes; 3 = most of the time; and 4 = at all times. Based on the mean score of each question, 1–2 equated to low level of perceived family support, 2.01–3 equated to moderate level of perceived family support, and 3.01–4 equated to high level of perceived family support.11
The Tuberculosis-Related Stigma Scale quantified the stigma associated with TB that patients faced. Community perceptions of TB and patient perspectives on TB were its two elements. Community perspectives on TB included 11 items about the community’s behavior toward TB patients. In contrast, patients’ perspectives on TB comprised 12 items about emotions, such as dread, guilt, and sadness related to living with the disease. The scale was rated on a four-point Likert scale, from strongly disagree (1), disagree (2), agree (3), to firmly agree (4). The item scores varied from 11 to 44 for community perspectives and 12 to 48 for patient perspectives on TB, with 11 indicating no stigma and 44 or 48, depending on the dimension, representing the maximum level of TB stigma.12
TB knowledge consisted of 14 statements about TB cause, transmission, signs, and treatment. The responses were yes and no, with scores ranged from 0–14.
Data Analysis
IBM SPSS statistics V21.0 was used for data analysis. Frequency and percentage were used for categorical data, while mean and SD were used for continuous data. Each domain score was counted using calculations from the computing domain from each instrument-scoring guideline. Since the data do not follow a normal distribution for complying with anti-TB medications, Spearman’s Rho was used to investigate the relationships between variables. We set the significance level at p < 0.05.
Ethical Clearance
Ethical approval number 770/UN6.KEP/EC/2018 was received from the Research Ethics Commission of the Faculty of Medicine at Universitas Padjadjaran, which adheres to the Declaration of Helsinki. The community health centers nurses introduced the researchers to the patients who could participate in the study. All respondents were provided with verbal and written explanations, and interested respondents were given a consent form. The researcher reassured the participants that their participation in the study was voluntary and that they might withdraw at any time. All information was confidential, and aggregated data were published for academic purposes only. In addition, there was no risk involved in filling out the questionnaires.
Results
The average age of the respondents was 36.78 years (SD = 11.76). The number of male (n = 40) and female (n = 39) respondents was almost the same. More than half of the respondents were Muslim (92.4%), were married (65.8%), were Sundanese (75.9%), were unemployed (69.6%), had health insurance (65.8%), and received an income above the minimum wage (59.5%) (Table 1).
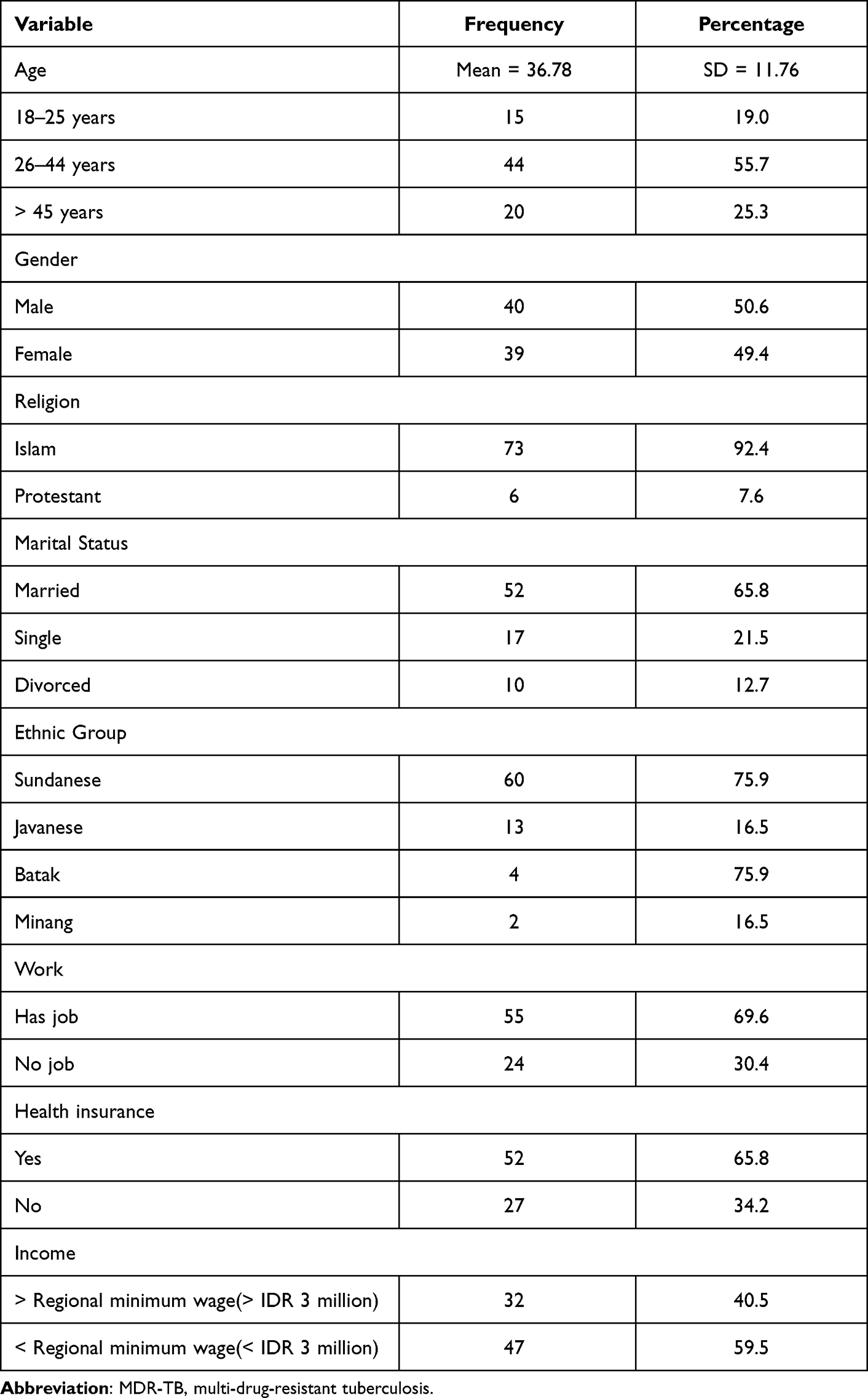 |
Table 1 Frequency and Percentage of Demographic Data in Drug-Resistant TB Patients (N = 79) |
Chronic obstructive pulmonary disease (COPD) was a comorbid disease experienced by 22 respondents. More than half of the respondents had no history of contact with MDR/RR-TB (78.5%), had had TB multiple times (57%), did not smoke (84.8%), and were in the advanced phase of MDR-TB treatment (68.4%). The side effects of treatment most experienced were dizziness (81%), nausea (80.6%), and headache (70.9%) (Table 2).
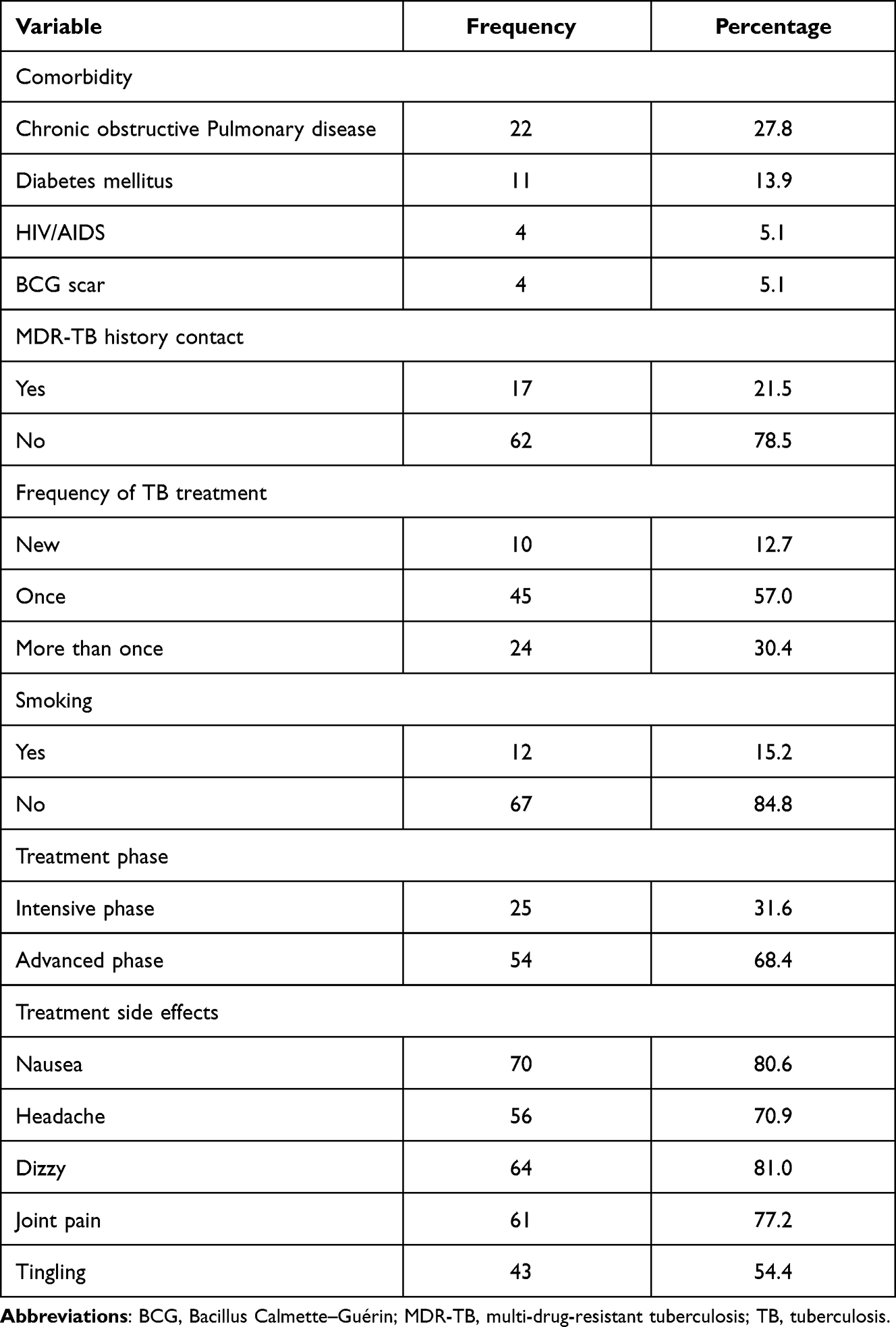 |
Table 2 Frequency and Percentage of Health Data on Drug-Resistant TB Patients (N = 79) |
The median score of treatment adherence was 20 (IQR = 2.00; 18–20), and the average score of health behavior adherence was 74.32 (SD = 12.26). The average values of family support and TB stigma were 88.05 (SD = 21.94) and 57.41 (SD = 6.35), respectively, and TB knowledge had a mean score of 7.14 (SD = 1.93) (Table 3).
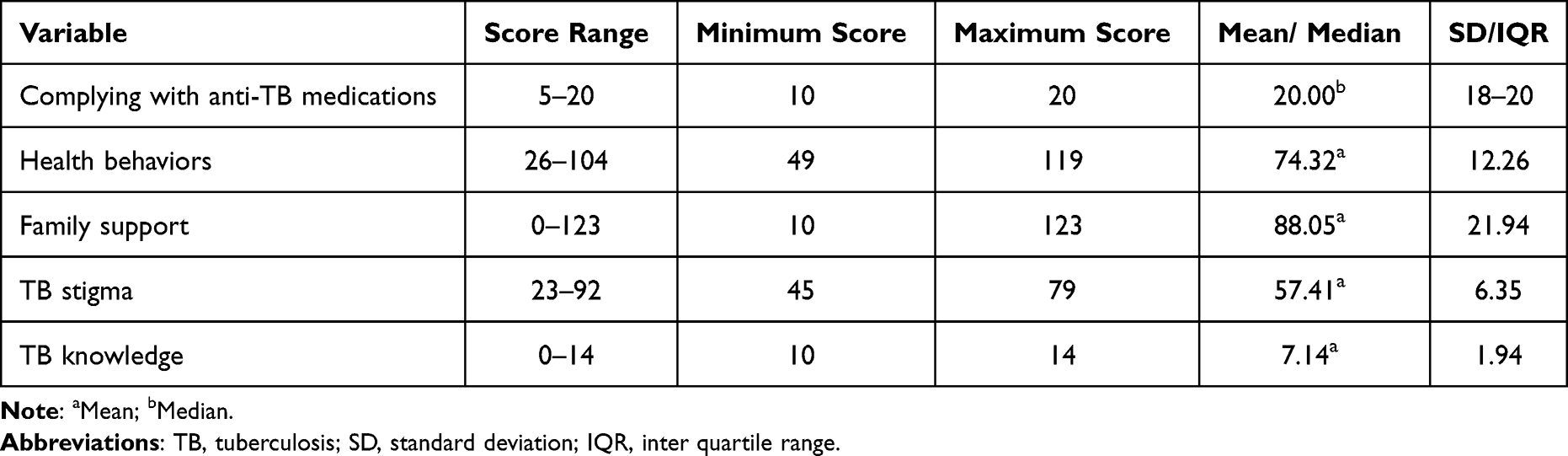 |
Table 3 Score Range, Minimum and Maximum Scores, Mean/ Median, and SD/ IQR of Complying with Anti-TB Medications, Health Behaviors, Family Support, TB Stigma, and TB Knowledge in Drug-Resistant TB Patients (N = 79) |
Health behavior (r = 0.36) was positively associated with complying with anti-TB medications, while TB stigma, knowledge, and family support were not related to medication adherence (Table 4).
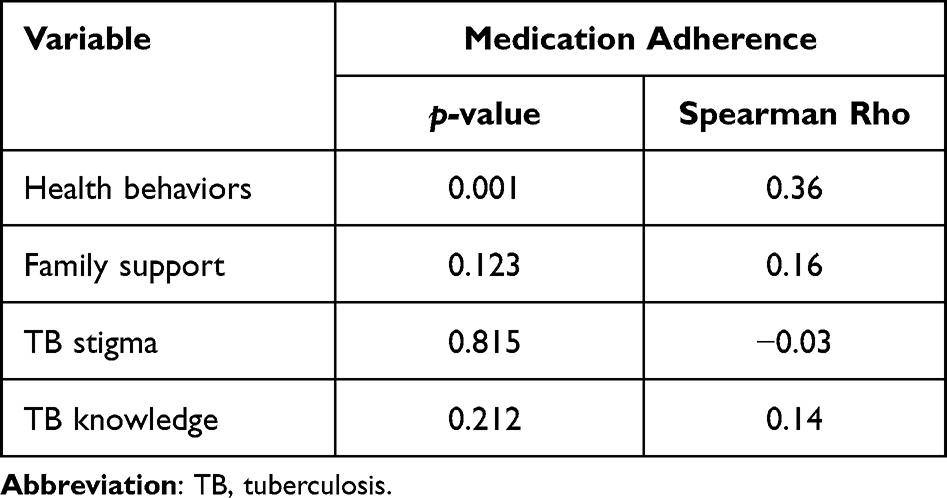 |
Table 4 Factors Related to Complying with Anti-TB Medications Among Drug-Resistant TB Patients (N = 79) |
Discussion
As measured by complying with anti-TB medications Scale, 91.1% of respondents had complying with anti-TB medications. A previous study demonstrated that 78.56% of TB patients had adherence,13 and the predicted rate of MDR-TB treatment adherence was 71%.14 During the continuation phase, 64.2% of 307 patients adhered to TB therapy.15 Complying with anti-TB medications is influenced by patient-related factors, condition-related factors, medication-related factors, socioeconomic factors, and healthcare system factors.16 Family support related to TB compliance among MDR-TB patients in Surabaya, Indonesia.8 In addition for tuberculosis patients in Bengkulu, Indonesia, age, gender, education, income, knowledge, the function of the drug-taking supervisor, drug accessibility, and family support have direct and beneficial effects on adherence to anti-tuberculosis treatment. It is negatively affected by the drug’s side effects, the distance to the nearest medical facility, and tenure.17
Health behaviors were a positive predictor of medication adherence. Health behaviors such as smoking, alcohol consumption, diet, exercise, and others contribute to patient-related factors. It is generally established that the efficient management of TB necessitates a change of habits in relation to smoking, drinking alcohol, physical exercise, and healthy diet, in addition to good drug adherence.18 The majority of treatment results were determined by patient characteristics.19 In addition, alcohol consumption and smoking significantly correlated to TB treatment.20 Higher complying with anti-TB medications was seen in TB patients who did not consume alcohol.21 Medication non-compliance of pulmonary TB patients was found to be influenced by patients’ inability to self-manage and self-regulate in a qualitative study.22 Few studies explored the association between health behaviors and medication compliance among TB patients. However, linkages between these variables had significant positive correlations with other chronic diseases, such as hypertension,23 acute myocardial infarction,24 and diabetes mellitus, and in the elderly.25 Conversely, self-reported health maintenance behavior cannot predict non-adherence to medications in people with ulcerative colitis.26 Few studies have investigated the association between health habits and medication compliance. Patients who exercise fundamental self-care behaviors are more likely to exhibit good medication compliance according to the majority of studies.
Another patient-related factor is patients’ knowledge. TB knowledge showed no correlation with medication adherence in the current study. Patients who had greater TB knowledge demonstrated greater treatment adherence.21 Medication compliance is influenced by education, knowledge, the kind of medicament, and mode of transportation.27 Higher medication adherence is seen in TB patients with greater tuberculosis awareness (OR: 1.34, p = 0.001) and who did not consume alcohol (OR: 1.84, p = 0.032).21
Demographic characteristics are part of patient-related factors. The number of male and female respondents in the current study was almost the same. However, a previous retrospective study was conducted in Bandung with different characteristics of respondents from those found in the current study in the form of a median age of 36 years (range 15–71 years) and 57% being male.28 The characteristics of respondents in research conducted in China were in the form of a median age of 41 years, 70% being male.29
Family support and TB stigma represent socioeconomic factors. Family support was significantly related with a missed dose, although there was no difference between interrupted therapy, lack of follow-up examination, and family support.30 TB patients who received psychological support from their family throughout TB therapy were less likely to skip doses than patients of other ethnicities and those who received no help.30 Patients with satisfactory medication adherence had family members who frequently supervised medication, family members who frequently provided spiritual encouragement, and more TB-related knowledge.31 Through medication adherence, directly observed therapy had an indirect, favorable effect on treatment success.32 Of all the respondents, 54.4% had low family support. The study’s results on family support in MDR/RR-TB patients found that participants were single, widowed or divorced, retired, and had fewer family members. Lower family incomes were found to have lower social support scores. Participants who did not disclose their illness tended to have less social support (31.59 < 34.23, p = 0.010). Participants who received good support from healthcare workers reported higher scores on the social support rating scale than those who did not feel supported (35.36 > 29.89, p = 0.014) (Chen et al). Of all respondents, 96.2% had good knowledge. This figure is higher than in other studies, where only 63.27% of respondents were found to have good knowledge.10 TB stigma had no association with medication adherence. However, there was a correlation between lack of provider support and societal stigma and non-adherence to therapy.33 In addition, stigma, discrimination, and lack of family and social support were found to have a substantial link with the number of loss to follow-up patients in drug-resistant TB patients. In terms of social support, the duty of nurses is to provide incentive, supervision, comfort, empathy, and information.34 This is critical for tuberculosis patients throughout treatment.
Condition-related factors represent comorbidities and contact history of MDR/RR-TB. The comorbidities in this study were COPD, Diabetes Mellitus (DM), cancer, and HIV. Another study conducted in Bandung found the highest comorbidity rates were DM, that being as much as 5%; while HIV, lupus, pregnancy, and chronic hepatitis were each as much as 1%.28 Regarding contact history, 21.5% of respondents had a contact history of MDR/RR-TB. This figure was more significant than noted in a previous study, which found only 1% had a contact history of MDR/RR-TB.28 In addition, treatment-related factors included side effects of treatment. All respondents complained of the side effects of treatment. The side effects of treatment most experienced were dizziness (81%), nausea (80.6%), and headache (70.9%). These results are similar to those found in other studies, where the side effects most often complained of were gastroenteropathy, rheumatism, and headaches.28 Patients who reported adverse drug effects had a greater likelihood of treatment interruption compared with those who did not report any drug side effects. There was no significant connection between symptoms and self-report adherence behaviors.30 Health-system-related factors included health insurance, and 65.8% of patients had taken out health insurance. Health insurance influences medication adherence positively.35 TB patients with high medication adherence have a favorable quality of life.36 Treatment compliance among MDR-TB patients will increase with stronger MDR-TB case management by healthcare workers in public health center sectors.37 Older age, vomiting, and TB treatment failure have the highest ORs for each category characteristic, respectively.38 Stigma of TB also correlates with non-adherence to medication because patients felt shamed, isolated, and fearful, which occurred at three levels—the individual level, the family level, and the societal level.39
The 2021–2024 National Strategy includes a program to provide integrated quality MDR-TB care and accelerate universal access. This policy has not yet explained the importance of health behaviors (following a healthy diet; doing physical exercise; keeping the environment clean; preventing disease transmission, and avoiding risk factors) that enhance medication adherence and increase treatment success. Thus, it is important to incorporate the strategy to improve health behavior of patients with MDR-TB in the national strategy. Further research is needed to examine the impact of health behavior interventions on MDR-TB treatment adherence and success. The present study covers the expected factors of compliance of anti-TB medications and all instruments were valid and reliable. However, this study restricts the applicability of the findings to a larger population, as the selection of settings for the sample is frequently influenced by accessibility, and sampling bias is typical.
Conclusion
Most patients demonstrated medication compliance. Health behaviors were positively correlated to medication compliance. Involvement and support from families, healthcare providers, and community leaders may assist in resolving the complicated issues of medication compliance in drug-resistant TB patients. Therefore, the government needs to incorporate strategies to improve health behaviors of MDR TB patients. Further research is needed to examine the effectiveness of various health behavior interventions on MDR-TB treatment adherence and success.
Acknowledgments
We thank all respondents, hospital, the Lung Health Center, and the community health centers for their cooperation. This study was funded by Universitas Padjadjaran, grant number 1113/UN6.L/PL/2018.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO Global Tuberculosis Report 2021. World Health Organization; 2022.
2. World Health Organization. Global Tuberculosis Report, 2022. Geneva: World Health Organization; 2022.
3. World Health Organization. Guidelines for Treatment of Drug-Susceptible Tuberculosis and Patient Care 2017. Geneva: World Health Organization; 2017.
4. Deshmukh RD, Dhande DJ, Sachdeva KS, Sreenivas AN, Kumar AMV, Parmar M. Social support a key factor for adherence to multidrug-resistant tuberculosis treatment. Indian J Tuberc. 2018;65(1):41–47. doi:10.1016/j.ijtb.2017.05.003
5. Sari YS, Kamil H. The patient with multi-drug resistant – pulmonary tuberculosis adherence to treatment: a qualitative study. Enfermería Clínica. 2022;32:S58–S61. doi:10.1016/j.enfcli.2022.03.019
6. Zuñiga JA. Medication adherence in Hispanics to latent tuberculosis treatment: a literature review. J Immigr Minor Heal. 2012;14(1):23–29. doi:10.1007/s10903-010-9393-x
7. Koo H-K, Min J, Kim HW, et al. Prediction of treatment failure and compliance in patients with tuberculosis. BMC Infect Dis. 2020;20(1):622. doi:10.1186/s12879-020-05350-7
8. Ainiyah SN, Soedarsono S, Umiastuti P. The relationship between family’s assessment support and MDR TB patient’s adherence on treatment in RSUD. JUXTA J Ilm Mhs Kedokt Univ Airlangga. 2019;10(2SE):75–77. doi:10.20473/juxta.V10I22019.75-78
9. Ruru Y, Matasik M, Oktavian A, et al. Factors associated with non-adherence during tuberculosis treatment among patients treated with DOTS strategy in Jayapura, Papua Province, Indonesia. Glob Health Action. 2018;11(1):1510592. doi:10.1080/16549716.2018.1510592
10. Biswas BR, Thaniwattananon P, Nilmanat K. The relationship between family support and health behaviors among patients with pulmonary TB.
11. Nasution SZ. Family Support perceived by pulmonary TB patients in complying with the DOTS program in Medan, Indonesia; 2007.
12. de Almeida Crispim J, da Silva LMC, Yamamura M, et al. Validity and reliability of the tuberculosis-related stigma scale version for Brazilian Portuguese. BMC Infect Dis. 2017;17(1):510. doi:10.1186/s12879-017-2615-2
13. Fagundez G, Perez-Freixo H, Eyene J, et al. Treatment adherence of tuberculosis patients attending two reference units in Equatorial Guinea. PLoS One. 2016;11(9):e0161995–e0161995. doi:10.1371/journal.pone.0161995
14. Nellums LB, Rustage K, Hargreaves S, Friedland JS. Multidrug-resistant tuberculosis treatment adherence in migrants: a systematic review and meta-analysis. BMC Med. 2018;16:1. doi:10.1186/s12916-017-1001-7
15. Gashu KD, Gelaye KA, Tilahun B. Adherence to TB treatment remains low during continuation phase among adult patients in Northwest Ethiopia. BMC Infect Dis. 2021;21(1):725. doi:10.1186/s12879-021-06428-6
16. Peh KQE, Kwan YH, Goh H, et al. An adaptable framework for factors contributing to medication adherence: results from a systematic review of 102 conceptual frameworks. J Gen Intern Med. 2021;36(9):2784–2795. doi:10.1007/s11606-021-06648-1
17. Hamidi S, Raharjo SS, Wijaya M. Path analysis on the determinants of adherence to anti tuberculosis drug treatment in Kaur District, Bengkulu, Indonesia. J Epidemiol Public Heal. 2019;4(3):205–214. doi:10.26911/jepublichealth.2019.04.03.08
18. Nezenega ZS, Perimal-Lewis L, Maeder AJ. Factors influencing patient adherence to tuberculosis treatment in Ethiopia: a literature review. Int J Environ Res Public Health. 2020;17(15):5626. doi:10.3390/ijerph17155626
19. Ali MK, Karanja S, Karama M. Factors associated with tuberculosis treatment outcomes among tuberculosis patients attending tuberculosis treatment centres in 2016–2017 in Mogadishu, Somalia. Pan Afr Med J. 2017;28:1.
20. Chaves Torres NM, Quijano Rodriguez JJ, Porras Andrade PS, Arriaga MB, Netto EM. Factors predictive of the success of tuberculosis treatment: a systematic review with meta-analysis. PLoS One. 2019;14(12):e0226507. doi:10.1371/journal.pone.0226507
21. Du L, Chen X, Zhu X, et al. Determinants of medication adherence for pulmonary tuberculosis patients during continuation phase in Dalian, Northeast China. Patient Prefer Adherence. 2020;14:1119–1128. doi:10.2147/PPA.S243734
22. Zhang J, Yang Y, Qiao X, et al. Factors influencing medication nonadherence to pulmonary tuberculosis treatment in Tibet, china: a qualitative study from the patient perspective. Patient Prefer Adherence. 2020;14:1149–1158. doi:10.2147/PPA.S252448
23. Wiarsih W, Jannah NM, Sahar J. Health behavior and medication adherence in hypertensive client. Indones J Glob Heal Res. 2020;2(2):103–110. doi:10.37287/ijghr.v2i2.75
24. Lee Y-M, Kim RB, Lee HJ, et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):100. doi:10.1186/s12955-018-0921-z
25. Han E, Sohn HS, Lee J-Y, Jang S. Health behaviors and medication adherence in elderly patients. Am J Heal Promot. 2016;31(4):278–286. doi:10.4278/ajhp.150205-QUAN-709
26. Lillis Y, Vaughn B, Gifford A, Cheifetz A. P-084 self-reported health maintenance behaviors in a population of patients with ulcerative colitis: correlation with medication adherence. Inflamm Bowel Dis. 2013;19(suppl_1):S58–S59. doi:10.1097/01.MIB.0000438763.60296.50
27. Ratnasari NY, Husna PH, Marni M, Nurtanti S, Susanto T. Adherence to medication behavior among tuberculosis patients and their affecting factors: a cross-sectional study at Public Health Center of Wonogiri District, Indonesia. Front Nurs. 2020;7(3):279–285. doi:10.2478/fon-2020-0024
28. Rahmawati RN, Pranggono EH, Ruslami R. Clinical characteristics and side effects of multidrug resistant tuberculosis therapy at top referral hospital West Java Indonesia. Althea Med J. 2016;3(4):526–532. doi:10.15850/amj.v3n4.934
29. Liu CH, Li L, Chen Z, et al. Characteristics and treatment outcomes of patients with MDR and XDR tuberculosis in a TB referral Hospital in Beijing: a 13-year experience. PLoS One. 2011;6(4):e19399. doi:10.1371/journal.pone.0019399
30. Zhang R, Pu J, Zhou J, et al. Factors predicting self-report adherence (SRA) behaviours among DS-TB patients under the “Integrated model”: a survey in Southwest China. BMC Infect Dis. 2022;22(1):201. doi:10.1186/s12879-022-07208-6
31. Chen X, Du L, Wu R, et al. The effects of family, society and national policy support on treatment adherence among newly diagnosed tuberculosis patients: a cross-sectional study. BMC Infect Dis. 2020;20(1):623. doi:10.1186/s12879-020-05354-3
32. Yin J, Wang X, Zhou L, Wei X. The relationship between social support, treatment interruption and treatment outcome in patients with multidrug-resistant tuberculosis in China: a mixed-methods study. Trop Med Int Heal. 2018;23(6):668–677. doi:10.1111/tmi.13066
33. Soedarsono S, Mertaniasih NM, Kusmiati T, et al. Determinant factors for loss to follow-up in drug-resistant tuberculosis patients: the importance of psycho-social and economic aspects. BMC Pulm Med. 2021;21(1):360. doi:10.1186/s12890-021-01735-9
34. Elfiyunai NN, Pandin MGR. The role of nurses in providing social support in tuberculosis treatment: Literature Review; 2021.
35. Ajibola SS, Timothy FO. The influence of national health insurance on medication adherence among outpatient type 2 diabetics in Southwest Nigeria. J Patient Exp. 2018;5(2):114–119. doi:10.1177/2374373517732384
36. Yadav RK, Kaphle HP, Yadav DK, et al. Health related quality of life and associated factors with medication adherence among tuberculosis patients in selected districts of Gandaki Province of Nepal. J Clin Tuberc Other Mycobact Dis. 2021;23:100235. doi:10.1016/j.jctube.2021.100235
37. Xing W, Zhang R, Jiang W, et al. Adherence to multidrug resistant tuberculosis treatment and case management in Chongqing, China - A mixed method research study. Infect Drug Resist. 2021;14:999–1012. doi:10.2147/IDR.S293583
38. Yani DI, Juniarti N, Lukman M. Characteristics of multidrug-resistant tuberculosis and smear-positive pulmonary tuberculosis: a case–referent study; 2022.
39. Juniarti N, Evans D. A qualitative review: the stigma of tuberculosis. J Clin Nurs. 2011;20(13‐14):1961–1970. doi:10.1111/j.1365-2702.2010.03516.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.