")
Back to Journals » Journal of Inflammation Research » Volume 15
Factors Influencing the Withdrawal of Antiepileptic Drugs in Adult Patients with Symptomatic Seizures Secondary to Neuronal Surface Antibodies-Associated Autoimmune Encephalitis
Authors Huang F, Wu Y, Nong W , Mao F, Cao X, Huang W, Zheng J
Received 4 November 2021
Accepted for publication 16 January 2022
Published 9 February 2022 Volume 2022:15 Pages 927—937
DOI https://doi.org/10.2147/JIR.S347893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Fang Huang, Yu Wu, Weidong Nong, Fengping Mao, Xiaoli Cao, Wen Huang, Jinou Zheng
Department of Neurology, The First Affiliated Hospital of Guangxi Medical University, Guangxi, People’s Republic of China
Correspondence: Wen Huang; Jinou Zheng, Department of Neurology, The First Affiliated Hospital of Guangxi Medical University, No. 6 shuangyong Road, Qingxiu District, Nanning, 530021, Guangxi, People’s Republic of China, Tel +86-18277197957; 86-13977166059, Email [email protected]; [email protected]
Purpose: This retrospective study aimed to investigate the relationship between clinical characteristics, seizure outcomes, and the potential factors influencing the withdrawal of antiepileptic drugs (AEDs) in adult patients with symptomatic seizures secondary to neuronal surface antibody (NSAb)-associated autoimmune encephalitis (AE).
Patients and Methods: Eighty-one patients (age ≥ 18 years) diagnosed with NSAb-associated AE were included in this retrospective study. After at least 1 year of follow-up, clinical details, magnetic resonance imaging (MRI) findings, electroencephalography (EEG) data, cerebrospinal fluid parameters, and the therapeutic outcomes were analyzed. Patients who needed long-term AEDs to control seizures were divided into two groups (withdrawal ≤ 1 year and withdrawal > 1 year). Multivariable logistic regression analysis was performed to identify the risk factors affecting the AEDs’ withdrawal in patients with seizures secondary to NSAb-associated AE.
Results: During the 12-month follow-up after AEDs’ withdrawal, 28 (44.4%) patients among the 63 patients who needed long-term AEDs stopped AEDs within 1 year, while 35 (55.6%) patients continued AEDs treatment. Multivariable logistic regression analysis showed that delayed immunotherapy, status epilepticus (SE), and elevated intrathecal Immunoglobulin G synthesis rate of 24 hours (24-h intrathecal IgG) were independent risk factors for delayed withdrawal in patients with seizure secondary to NSAb-associated AE (odds ratios: 1.129, 6.497, 3.415, P< 0.05). The receiver operating characteristics (ROC) curve analysis showed that the area under the curve (AUC) of delayed immunotherapy, SE, and elevated 24-h intrathecal IgG was 0.816 (95% CI=0.711– 0.921, P< 0.001).
Conclusion: Delayed immunotherapy, status epilepticus and elevated 24-hour intrathecal IgG synthesis rate are the factors that may influence the decision to delay AEDs’ withdrawal.
Keywords: autoimmune encephalitis, GABA(BR), LGI1, NMDAR, prognosis, seizure
Introduction
Autoimmune encephalitis (AE) is a new group of neurological diseases mediated by specific antibodies against neuronal antigens. Its common clinical manifestations include changes in behavior, psychosis, seizures, memory and cognitive deficits, abnormal movements, dysautonomia, and a decreased level of consciousness.1 According to the location of the antigen targeted by the antibody, it is further divided into three subtypes, different in treatment and outcomes: associated with antibody against the intracellular target, associated with antibody against the cell surface antigen, and without recognizable antibody association.2 The most common types of neuronal surface antibodies (NSAb) associated with AE are N-methyl-
Seizures usually occur as the only major symptom in patients with AE in the acute stage or with disease progression.6 Compared to other forms of epilepsy caused by intraneuronal antibodies, most patients with NSAb-associated AE rarely develop epilepsy from seizures. Seizure symptoms of most patients are effectively controlled after initial immunotherapy and/or antiepileptic therapy.7,8 However, in many cases, the short-term curative effect known as “honeymoon period” led to confusion and omissions in the AEDs’ management. Recent follow-up study by Yao et al found that the seizure control rate reached the peak in the first 12 months, but decreased in the following 6 months. Combined with previous clinical experience, it is proposed that 1 year after the onset of AEDs is the key period for AEDs’ withdrawal.9 Geis et al also proposed that patients with seizures secondary to AE should have an appropriate follow-up (1 year) before the diagnosis of epilepsy is considered in those who continue having seizures or need sustained AEDs.10 At present, more studies focus on the risk prediction of seizure secondary to NSAb-associated AE, as a kind of epilepsy that can be treated or even cured. Many studies also investigate pathogenic factors that may affect the incidence of epilepsy in AE patients. However, there is still a lack of guidance on the treatment of subsequent AEDs, and the timing of discontinuation of AEDs depends more on the personal experience of clinicians. Although it has been agreed that in the majority of cases there is no need for a long AEDs treatment, the lack of attention to the late prevention measures and premature discontinuation of treatment might become an important reason for the recurrence of epilepsy in such patients. This retrospective study analyzed the clinical characteristics of seizures secondary to NSAb-associated AE and potential factors influencing AEDs’ withdrawal. We hypothesized that it is possible to find some relatively objective indicators rather than subjective experience, to aid decision-making regarding which patients can withdraw drugs as soon as possible or need to prolong the medication time to reduce the probability of epilepsy recurrence.
Materials and Methods
Patients
Sixty-seven adult (age ≥18 years) patients with symptomatic seizures secondary to NSAb-associated AE and diagnosed at the Neurology Department of the First Affiliated Hospital of Guangxi Medical University between January 2015 and December 2019 were included. The inclusion criteria were 1) rapid onset (<3 months) of symptoms of encephalitis, 2) seizures in the acute or subacute phase of the disease, 3) positive detection of NMDAR, LGI1, or GABA(BR) antibody in the cerebrospinal fluid (CSF), and 4) immunotherapy as initial treatment.
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University, Guangxi, China. Due to the retrospective design, the requirement for individual consent was waived by the committee.
Clinical Data Collection
The following information was retrieved from medical records: demographic information, seizure semiology, associated tumor, CSF tests, and magnetic resonance imaging (MRI) and electroencephalogram (EEG) findings. According to the 2017 guidelines of the International League Against Epilepsy (ILAE), seizures were classified based on clinical symptoms.11 Status epilepticus (SE) was defined as persistent or recurrent seizures that lasted more than 5 min without complete recovery of consciousness.12 Baseline seizure frequency was categorized into two groups: single seizure and recurrent seizure.
CSF examinations included total cell count, total protein content, albumin, and IgG content in both CSF and serum. Pleocytosis was defined as CSF white blood cell count >5×106/L. Protein concentration exceeding 450 mg/L was defined as abnormal elevation. Detection of antibodies in the CSF was performed by specific staining against NMDAR, LGI1, or GABA(BR) isolated from rat hippocampus and cerebellum, and positive cell-based assay with HEK293 cells transfected with respective target proteins.
The evaluation of blood-CSF barrier function was performed using QAlb (albumin-CSF/serum-quotient), IgG index (IgG CSF/IgG serum)/(Alb CSF/Alb serum), and 24-h intrathecal IgG synthesis rate ([(IgG CSF-IgG serum/369)-(Alb CSF-Alb serum/230)×(IgG serum/Alb serum)×0.43]×5), which are considered reliable parameters for monitoring the synthesis of intrathecal immunoglobulin.13,14 Dysfunction was defined as QALB >7.00, 24-h intrathecal IgG synthesis rate >3.3 mg/dL, and IgG index >0.7.
Evaluation of Outcomes
All patients were followed up for at least 1 year after AED withdrawal. Data on seizure outcomes and medications were collected every 3 months during follow-up at the outpatient clinic or via telephone interviews after discharge. The modified Rankin scale (mRS) was used to evaluate the functional status before immunotherapy.15 Seizure remission was defined as no seizures for at least 1 year after AED withdrawal. Effective seizure control referred to ≥50% reduction in seizure frequency. The patients taking AEDs were divided into two groups: drug withdrawal ≤1 year and drug withdrawal group >1.
Statistical Analysis
IBM SPSS 22.0 was used for data analysis. Descriptive statistics were performed for each variable, including means, medians, and interquartile range. Student’s t-test was used to analyze the continuous variables with a normal distribution. Non-parametric tests were used to analyze continuous data with a non-normal distribution. The categorical data were presented as n (%) and analyzed using the χ2 test. Multivariable Logistic regression analysis was used to explore the independent risk factors affecting delayed withdrawal of patients with seizures secondary to AE. The prediction of delayed withdrawal factors was analyzed by receiver operating characteristics (ROC) analysis. P<0.05 was considered statistically significant.
Results
Clinical Characteristics of Study Patients
We identified a total of 81 adult patients with NSAb-associated AE. Of these, 73 patients had seizures during the acute or subacute phase of AE. The incidence of seizures in NSAb-associated AE was 90.1%. Six patients were lost during follow-up. Therefore, 67 eligible patients were included in the present study: 54 with anti-NMDAR encephalitis, six with LGI1 antibody encephalitis, and seven with GABA(BR) encephalitis. The demographic and clinical characteristics of the patients are shown in Table 1. The median age at onset was 26 (range, 18–72) years. The patients with anti-NMDAR encephalitis (median, 21.5 years) were younger than those with anti-LGI1 encephalitis (median, 40 years) and patients with anti-GABA (BA) encephalitis (median, 48.3 years). Thirty (44.8%) patients were women. The median baseline of mRS was 4 (range, 2–5). The median delay to the initiation of immunotherapy was 12 (range, 3–121) days. The median hospital length of stay was 20 (range, 5–135) days. Eight patients had associated tumors [five women with anti-NMDAR encephalitis had ovarian teratoma, and three men with anti-GABA(BR) encephalitis had lung cancer]. Paired serum and CSF samples were available from 67 patients; all patients had antibodies in the CSF, and 49 (73.1%) patients were serum antibody-positive. All 67 patients underwent brain MRI and EEG; 31 (46.3%) had abnormal MRI, and 48 (71.6%) had abnormal EEG. The CSF cell count was elevated in 35 (52.2%) patients. Only six (9.0%) patients had elevation of CSF total protein. Seven (10.4%) patients showed the disruption of the blood–brain barrier (BBB) (QALB >7). An elevated IgG index was observed in 18 (26.9%) patients, and 41 (61.2%) patients showed elevated 24-h intrathecal IgG.
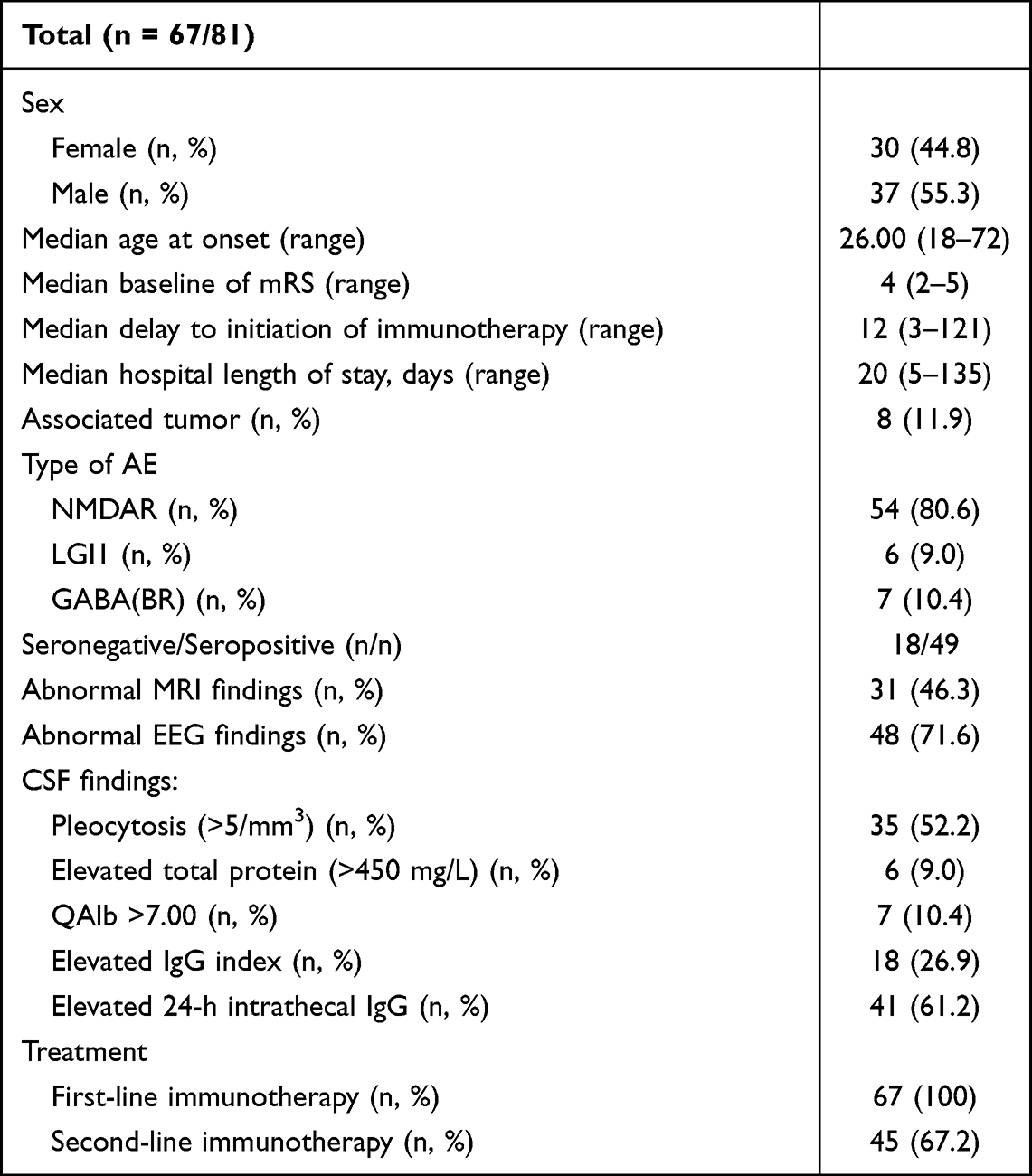 |
Table 1 Summary of the Clinical Characteristics of 67 Adult Patients with Symptomatic Seizures Secondary to AE |
The overview of medications for all patients is shown in Figure 1. All 67 patients were treated with first-line immunotherapy (combination of methylprednisolone and/or intravenous immunoglobulin (IVIG) and/or therapeutic plasma exchange) and 67.2% with additional second-line immunotherapy (azathioprine, mycophenolate mofetil, cyclophosphamide, or tacrolimus).
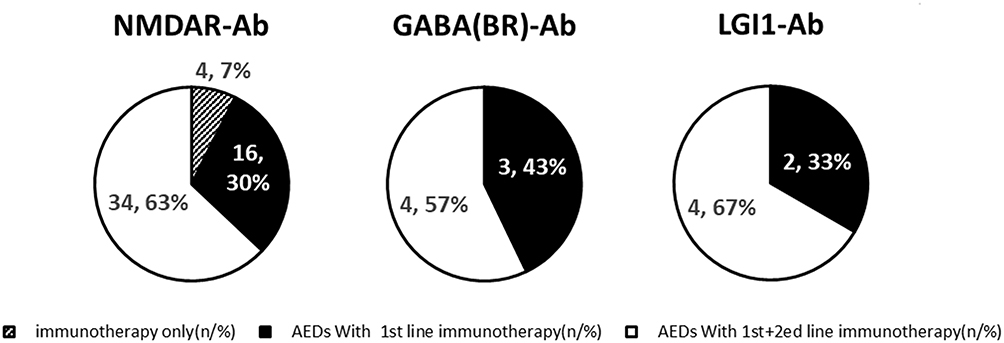 |
Figure 1 Overview of medication in 67 adult patients with symptomatic seizures secondary to neuronal surface antibody-associated autoimmune encephalitis, according to different antibody types. |
Seizure Semiology of Different AE Types
The seizure semiology of the different AE types is shown in Table 2. The most common type of seizure in all patients was generalized tonic-clonic seizure (GTCS) (53.7%, 36/67). The second most common seizure type was focal to bilateral tonic-clonic seizure (FBTCS) (16.4%). Most patients with anti-NMDAR encephalitis (92.6%, 50/54) experienced recurrent seizures, while only four patients suffered from single seizures. In the other two types of AE, 100% of the patients had recurrent seizures. SE was observed in 19.4% (13/67) patients; 92.3% (12/13) of these were patients with anti-NMDAR encephalitis.
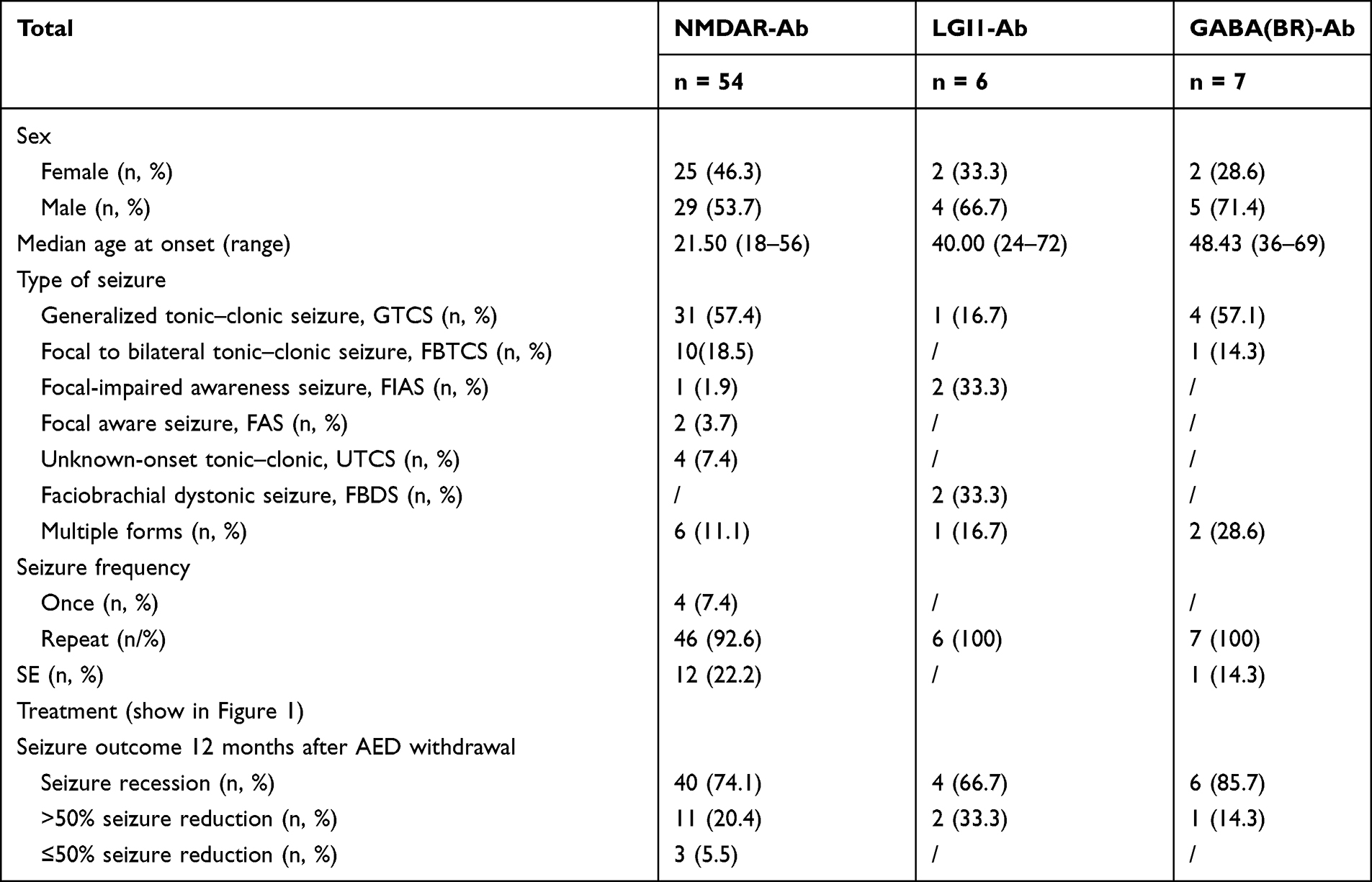 |
Table 2 Seizure Semiology of Different Antibody Types |
The prognosis of seizures in different AE groups was slightly different at 12 months after discharge. Overall, 95.5% of the patients could become seizure-free or achieve reduction after adequate immunotherapy and/or AED treatment. The discharged patients were followed up every 3 months for at least 1 year. The withdrawal distribution of patients taking AEDs every 3 months is shown in Figure 2. Among the 63 patients who took AEDs and immunotherapy, nearly half of them withdrew AEDs within the first 12 months of follow-up.
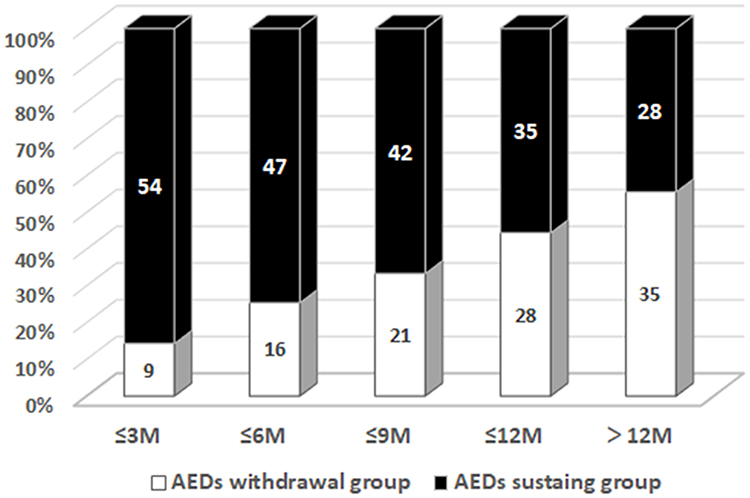 |
Figure 2 The proportion of patients underwent antiepileptic drugs (AEDs) withdrawal (white) compared to still receiving AEDs (black) among patients with seizure secondary to autoimmune encephalitis, from 3 to 13 months of follow-up. |
Prognostic Factors of Seizures Secondary to NSAb-Associated AE
Of the 67 patients, four had single seizures and took immunotherapy alone. Furthermore, 94% (63/67) were treated with immunotherapy and one or more AEDs. The patients taking AEDs (63 patients) were divided into two groups to analyze the influencing factors for the withdrawal from AEDs (Table 3): AEDs’ withdrawal ≤1 year and AEDs’ withdrawal >1 year. The clinical characteristics, seizure semiology, and auxiliary examination were compared between the two groups. No significant differences were observed between the two groups in terms of sex (P=0.775), age at seizure onset (P=0.258), associated tumor (P>0.99), abnormal MRI findings (P=0.091), and abnormal EEG findings (P=0.409). No significant difference was found in the course of treatment between different antibody types. The statistical analysis revealed that the related factors included time to initiating immunotherapy, SE, and elevated 24-h intrathecal IgG rate (P<0.05). Delayed immunotherapy, SE, and elevated 24-h intrathecal IgG were included in the multivariable logistic regression analysis. The results were analyzed by regression coefficient (β), odds ratios (OR), standard error, Z-test, 95% confidence intervals (CI), and P-value (Table 4). The results showed that delayed immunotherapy, SE, and 24-h intrathecal IgG were independent risk factors for delayed withdrawal in patients with seizures secondary to AE (all P<0.05). In order to evaluate the predictive effect of the above three parameters on the timing of the withdrawal of AEDs, a ROC curve analysis was performed. The results showed that the area under the curve (AUC) was 0.816 (95% CI=0.711–0.921, P<0.001) (Figure 3).
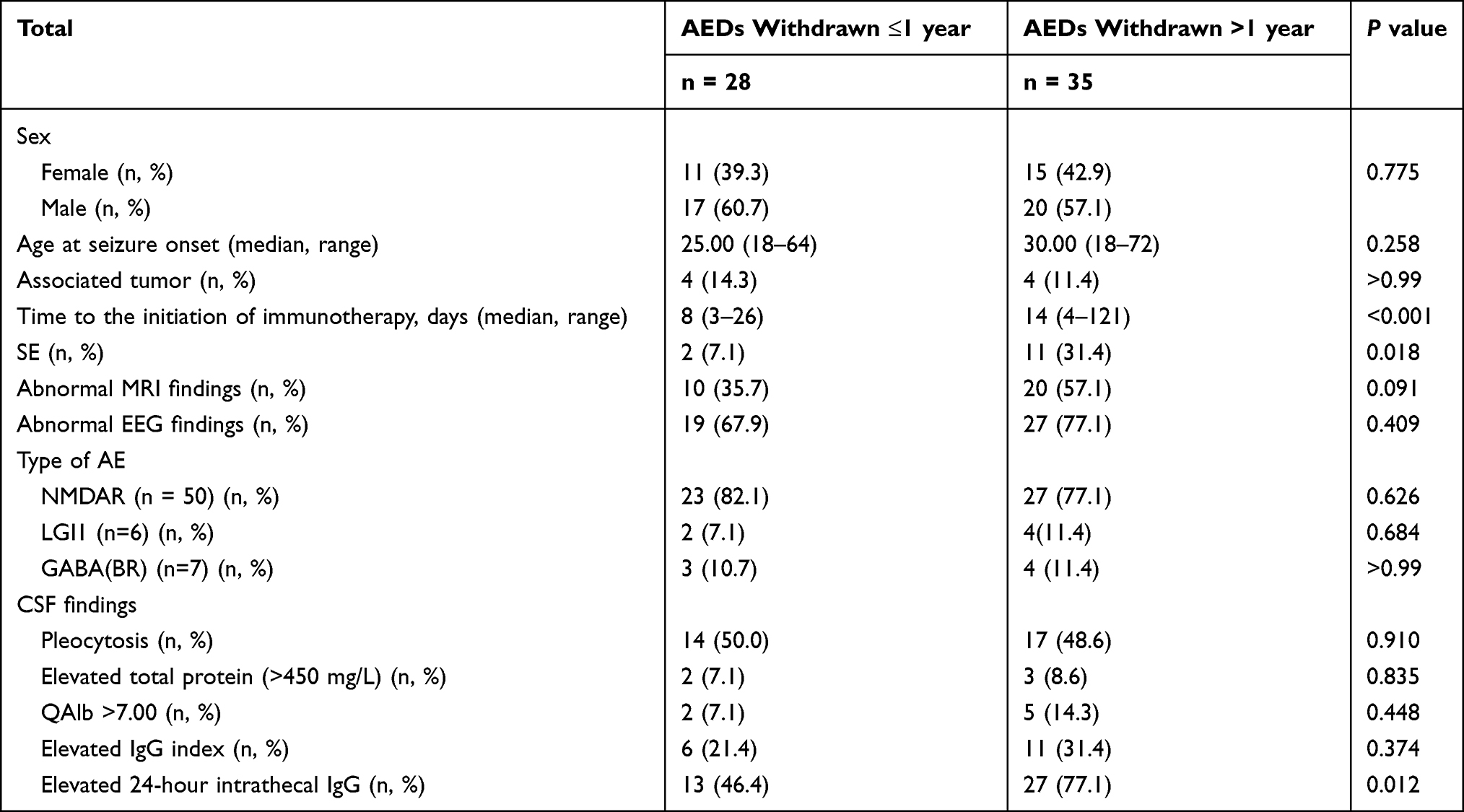 |
Table 3 Predictors for Delayed Withdrawal of AEDs |
 |
Table 4 Multivariable Logistic Regression Analysis of Predictors for Delayed Withdrawal of AEDs |
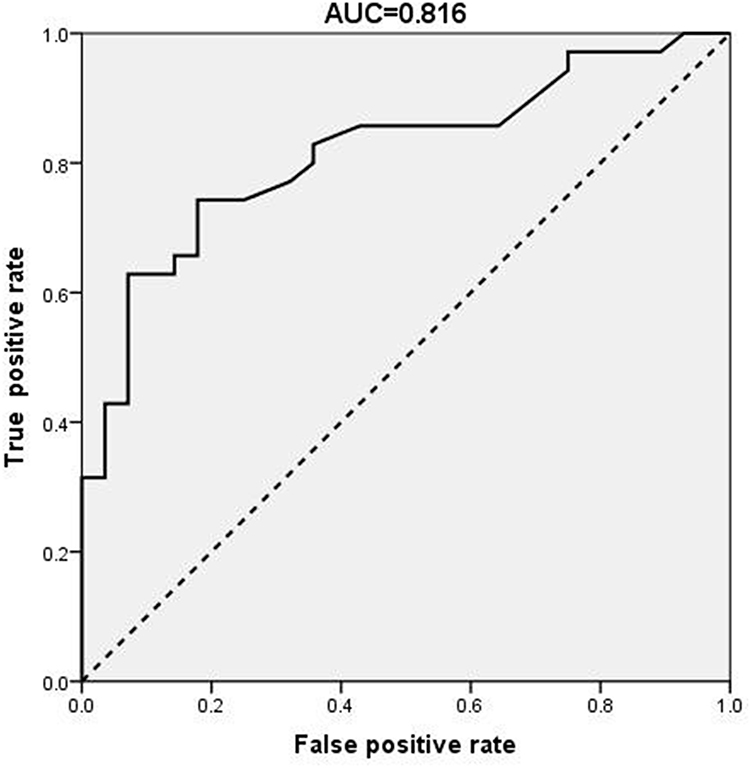 |
Figure 3 Receiver operating characteristic (ROC) curve for predicting value of the timing of immunotherapy initiation, status epilepticus and 24-h intrathecal Immunoglobulin G synthesis for the decision of antiepileptic drugs withdrawal in patients with seizure secondary to autoimmune encephalitis. |
Discussion
Approximately 45.9 million adults worldwide suffer from epilepsy16 and it is estimated that one-third of all cases of epilepsy in adults have an unknown etiology.17 Recent studies suggested that AE might explain at least 20% of adult-onset cases of epilepsy with unknown etiology.18,19 The incidence rate of secondary seizures is probably underestimated, as the expansion of the autoimmune antibody spectrum of the central nervous system (CNS). Different from T cell-mediated irreversible neuronal damage induced by antibodies to intracellular antigens (anti-Hu and Yo), cell membrane surface antigens [NMDAR antibody, LGI1 antibody, and GABA(BR) antibody] have direct effects on neural function.20 Most patients with NSAb-associated AE can finally achieve a complete seizure-free state and stop taking AEDs in a relatively short time. Therefore, referring to the current ILAE terminology, seizures in the context of AE at initial or relapsing presentations are best conceptualized as acute symptomatic seizures instead of epilepsy.21 This study examined the clinical characteristics of seizures secondary to the three most common NSAb-associated AE [NMDAR antibody, LGI1 antibody, and GABA(BR)] and the factors that may influence the decision to delay AEDs’ withdrawal.
Despite High Frequency of Seizures, Majority of Patients Successfully Withdrew AEDs Within 1 Year and Did Not Relapse at Least 12 More Months
In this study, 90.1% of the patients developed seizures, which is consistent with previous findings (ranging from 57% to 100%).22,23 The proportion of male patients with seizures was higher than female (37 male/30 female). This partially confirms the findings of some previous studies, reporting that seizure is more likely to appear as the first symptom in male AE patients.24 This gender difference suggests that sex hormone may be one of the factors of epilepsy susceptibility.25 Although the incidence of seizures was high and the conditions of the patients were relatively serious at the time of admission with the average mRS score of 4, more than half of the patients successfully withdrew AEDs' treatment within 1 year and did not relapse during the follow-up for at least 12 months. These findings are also in line with the conclusions of other studies, such as a few patients with NMDAR, LGI1, or GABA(BR) encephalitis have developed clinical “epilepsy”.26 The risk factors of epilepsy that were considered in this study, according to the existing literature,27–29 included delayed immunotherapy, hippocampal atrophy in neuroimaging, interictal epileptiform discharges, IED on EEG during follow-up, first occurrence of status epilepticus. Consistent with the literature, we also found that seizures secondary to AE had the characteristics of AED resistance:10 among the 63 patients treated with AEDs, 26 patients experienced a failure of AED therapy alone before initiating immunotherapy. Previous animal model studies of anti-NMDA antibody encephalitis revealed its possible underlying mechanism was related to the production of specific cytokines (IL-1β, HMGB1, and TNF-α) that induce neuronal hyperactivity, dysfunction of the BBB, and damage to neurons.30 These pathological changes lead to the maintenance of the inflammation due to seizures and chronic decrease of seizure threshold, thus promoting seizures.
Seizure Forms of Different Antibody Types Demonstrated Their Own Characteristics, but are Comparable in Response to Treatment
In this study, GTCS (57.4%), FBTCS (18.5%) and multiple forms (11.1%) were the three most common forms of seizures in patients with anti-NMDAR encephalitis. This data confirmed the EEG findings of previous study that focal abnormalities are rare for this form.31 In patients with GABA-BR encephalitis, seizures was the first and prominent symptom with the main types of seizures being GTCS (57.1%) and multiple forms (28.6%). In contrast, two of the six (33.3%) patients with LGI1 antibodies had faciobrachial dystonic seizure (FBDS), the most characteristic seizure type in patients with LGI1 encephalitis. Due to the poor response of FBDS to AEDs, whether it should be classified as autoimmune seizures or dystonia is still controversial. Previous studies found that the ictal EEG of FBDS showed a decrease of 1s in amplitude in all the electrodes before onset, indicating that it was epileptic. Combined with imaging findings (basal ganglia lesions were found in brain MRI), it was considered that FBDS was essentially epileptic seizure and originated from subcortical basal ganglia.22,32 Despite differences in form, 74.1% of the patients with anti-NMDAR encephalitis, 66.7% of the patients with LGI1 encephalitis and 85.7'% of the patients with GABA-BR encephalitis demonstrated successful seizure recession 12 months after AED withdrawal, without statistically significant differences in treatment response. Two elderly male patients had lung cancer: one had small-cell lung cancer, and the other one had alveolar cell carcinoma and invasive adenocarcinoma. In those cases, seizures were still not completely controlled until the removal of the tumors and radiotherapy, even after the combined use of multiple AEDs and immunotherapy. Those results suggest that antiepileptic treatment itself needs to be individualized, and some more objective indicators in addition to clinical experience may be needed to provide more guidance on withdrawal.
Delayed Immunotherapy, SE and 24-Hour Intrathecal IgG Synthesis Rate are the Factors That May Influence the Decision to Delay AEDs’ Withdrawal
Some of the previous studies have found no difference between early and late withdrawal of AEDs in the short term,29,33 therefore little research is published on the factors that may influence the decision to delay AEDs’ withdrawal in AE. In this study, patients were divided into two groups (≤1-year withdrawal and >1-year withdrawal) and logistic regression analysis showed that some of the factors were independently linked to the prolonged use of AEDs, namely delayed immunotherapy, SE and 24-hour intrathecal IgG synthesis rate. Using ROC analysis, it was found that the AUC for predicting withdrawal using the above three parameters was 0.848, indicating a good reference value. Some patients in our study had drug resistance when using AEDs alone at the beginning of the disease and then showed rapid improvement when combining immunotherapy. The phenomenon indicated that the lack of immunotherapy might be the reason why they had AED resistance. Therefore, delayed initiation of immunotherapy can cause inability to break this vicious circle, failing to control the seizures quickly. After that prolonged seizure duration, the duration of cerebral ischemia and hypoxia, and the cascading effects of various inflammatory factors produced by seizures might lead to a higher probability of irreversible structural damage to the brain. Admittedly, among the 13 patients with SE in this study, 11 patients needed to take AEDs for more than 1 year, suggesting that they were more likely to transform from seizures to chronic epilepsy.Furthermore, 24-h intrathecal IgG synthesis rate is an index for quantitative monitoring of intrathecal immunoglobulin synthesis. Tourtellotte formula fully considers and excludes the effects of two factors: increased serum IgG and increased blood–brain barrier permeability on intrathecal synthesis rate.34 Therefore, it is a more reliable index for evaluating intrathecal synthesis of intrathecal immunoglobulin. At present, there are few studies on the correlation between the 24-h intrathecal IgG synthesis rate and clinical features in patients with AE. Previous similar reports demonstrated QALB association with poor short-term prognosis, along with a significant correlation between the increase of 24-hour intrathecal IgG synthesis rate and the change of QALB.2,35 In this study, some patients had abnormal BBB function (QAlb >7.00), but the proportion was low (7/63, 11.1%), and it was not related to the withdrawal of AEDs (P=0.448). Therefore, this study shows that the 24-hour intrathecal synthesis rate can objectively reflect the degree of inflammatory response of CNS, and may be used as a reference index for clinicians to consider the withdrawal time of AEDs. Due to the small sample size and low proportion of increased QALB in this study, the correlation between abnormal QALB and abnormal 24-hour intrathecal IgG synthesis rate still needs to be confirmed by further research.
The novelty of this study is identifing three factors that can affect the withdrawal of AEDs in patients with seizures secondary to AE. It can provide clinicians with some reference for the withdrawal of AEDs. However, this study has several limitations. The disease is relatively rare, the sample size is small, and patients with seizures secondary to AE are rarer. The long follow-up time range increases the difficulty of expanding the sample. Although the sample size was sufficient for multivariable logistic regression for risk factor analysis, a larger multicenter sample is still needed.
Conclusion
The frequency of seizures secondary to NSAb-associated AE was abnormally high, and the seizure forms of different antibody types have their own characteristics, but tend to have good response to treatment. While paying attention to the management of immunotherapy, the corresponding adjustment of AEDs’ strategy after the acute phase of the disease should not be ignored. In addition to the personal experience of clinicians, delayed immunotherapy, status epilepticus and 24-hour intrathecal IgG synthesis rate are the factors that may influence the decision to delay AEDs’ withdrawal.
Abbreviations
AE, autoimmune encephalitis; AEDs, antiepileptic drugs; APE, antibody prevalence in epilepsy; APE, faciobrachial dystonic seizure; BBB, blood–brain barrier; CNS, central nervous system; FBTCS, focal to bilateral tonic–clonic seizure; GABA(BR), anti-gamma-aminobutyric acid-B receptor; GTCS, generalized tonic–clonic seizure; ILAE, International League Against Epilepsy; LGI, leucine-rich glioma-inactivated; mRS, modified Rankin scale; NMDAR, N-methyl-
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University, Guangxi, China. Due to the retrospective design, the requirement for individual consent was waived by the committee. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The authors confirmed that all patient data were confidential.
Acknowledgments
The authors cordially thank the participants and their families.
Author Contributions
FH, YW, NWD, FPM, XLC, WH, and JOZ were all directly involved in clinical management. FH and YW were major contributors in writing the manuscript under the guidance of WH and JOZ. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82060236) and the Natural Science Foundation of Guangxi Province (CN) (2019GXNSFDA245032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dalmau J, Graus F. Antibody-mediated encephalitis. N Engl J Med. 2018;378:840–851. doi:10.1056/NEJMra1708712
2. Wesselingh R, Butzkueven H, Buzzard K, et al. Seizures in autoimmune encephalitis: kindling the fire. Epilepsia. 2020;61(6):1033–1044. doi:10.1111/epi.16515
3. Dalmau J, Tuzun E, Wu HY, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61:25–36. doi:10.1002/ana.21050
4. Granerod J, Ambrose HE, Davies NWS, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10(12):835–844. doi:10.1016/S1473-3099(10)70222-X
5. Lancaster E, Lai M, Peng X, et al. Antibodies to the GABAB receptor in limbic encephalitis with seizures: case series and characterisation of the antigen. Lancet Neurol. 2010;9(1):67–76. doi:10.1016/S1474-4422(09)70324-2
6. Bien CG, Bauer J. Autoimmune epilepsies. Neurotherapeutics. 2014;11(2):311–318. doi:10.1007/s13311-014-0264-3
7. Liu X, Yan B, Wang R, et al. Seizure outcomes in patients with anti-NMDAR encephalitis: a follow-up study. Epilepsia. 2017;58(12):2104–2111. doi:10.1111/epi.13929
8. Feyissa AM, López Chiriboga AS, Britton JW. Antiepileptic drug therapy in patients with autoimmune epilepsy. Neurol Neuroimmunol Neuroinflamm. 2017;4:e353.
9. Yao L, Yue W, Xunyi W, et al. Clinical features and long-term outcomes of seizures associated with autoimmune encephalitis: a follow-up study in East China. J Clin Neurosci. 2019;68:73–79. doi:10.1016/j.jocn.2019.07.049
10. Geis C, Planaguma J, Carreno M, et al. Autoimmune seizures and epilepsy. J Clin Invest. 2019;129(3):926–940. doi:10.1172/JCI125178
11. Fisher RS, Cross JH, D’Souza C, et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia. 2017;58(4):531–542. doi:10.1111/epi.13671
12. Leitinger M, Beniczky S, Rohracher A, et al. Salzburg consensus criteria for non-convulsive status epilepticus–approach to clinical application. Epilepsy Behav. 2015;49:158–163. doi:10.1016/j.yebeh.2015.05.007
13. Sindic CJ, Van Antwerpen MP, Goffette S. The intrathecal humoral immune response: laboratory analysis and clinical relevance. Clin Chem Lab Med. 2001;39:333–340. doi:10.1515/CCLM.2001.052
14. Deisenhammer F, Bartos A, Egg R, et al. Guidelines on routine cerebrospinal fluid analysis. Report from an EFNS task force. Eur J Neurol. 2006;13(9):913–922. doi:10.1111/j.1468-1331.2006.01493.x
15. van Swieten JC, Koudstaal PJ, Visser MC, et al. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19(5):604–607. doi:10.1161/01.STR.19.5.604
16. Feigin VL, Nichols E, Alam T, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
17. Ramanathan S, Bleasel A, Parratt J, et al. Characterisation of a syndrome of autoimmune adult onset focal epilepsy and encephalitis. J Clin Neurosci. 2014;21(7):1169–1175. doi:10.1016/j.jocn.2013.09.024
18. Dubey D, Alqallaf A, Hays R, et al. Neurological autoantibody prevalence in epilepsy of unknown etiology. JAMA Neurol. 2017;74(4):397–402. doi:10.1001/jamaneurol.2016.5429
19. Brenner T, Sills GJ, Hart Y, et al. Prevalence of neurologic autoantibodies in cohorts of patients with new and established epilepsy. Epilepsia. 2013;54(6):1028–1035. doi:10.1111/epi.12127
20. Dalmau J, Geis C, Graus F. Autoantibodies to synaptic receptors and neuronal cell surface proteins in autoimmune diseases of the central nervous system. Physiol Rev. 2017;97(2):839–887. doi:10.1152/physrev.00010.2016
21. Steriade C, Britton J, Dale RC, et al. Acute symptomatic seizures secondary to autoimmune encephalitis and autoimmune-associated epilepsy: conceptual definitions. Epilepsia. 2020;61(7):1341–1351. doi:10.1111/epi.16571
22. Wang Y, Yu Y, Hu Y, et al. Clinical and electroencephalographic features of the seizures in neuronal surface antibody-associated autoimmune encephalitis. Front Neurol. 2020;11:280. doi:10.3389/fneur.2020.00280
23. de Bruijn M, van Sonderen A, van Coevorden-hameete MH, et al. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABABR encephalitis. Neurology. 2019;92:e2185–e2196. doi:10.1212/WNL.0000000000007475
24. Viaccoz A, Desestret V, Ducray F, et al. Clinical specificities of adult male patients with NMDA receptor antibodies encephalitis. Neurology. 2014;82(7):556–563. doi:10.1212/WNL.0000000000000126
25. Rhodes ME, Frye CA. Androgens in the hippocampus can alter, and be altered by, ictal activity. Pharmacol Biochem Behav. 2004;78(3):483–493. doi:10.1016/j.pbb.2004.04.020
26. Britton JW, Dalmau J. Recognizing autoimmune encephalitis as a cause of seizures: treating cause and not effect. Neurology. 2019;92(19):877–878. doi:10.1212/WNL.0000000000007444
27. Gifreu A, Falip M, Sala-Padro J, et al. Risk of developing epilepsy after autoimmune encephalitis. Brain Sci. 2021;11:1182.
28. Spatola M, Dalmau J. Seizures and risk of epilepsy in autoimmune and other inflammatory encephalitis. Curr Opin Neurol. 2017;30(3):345–353. doi:10.1097/WCO.0000000000000449
29. Shen CH, Fang GL, Yang F, et al. Seizures and risk of epilepsy in anti-NMDAR, anti-LGI1, and anti-GABAB R encephalitis. Ann Clin Transl Neurol. 2020;7:1392–1399. doi:10.1002/acn3.51137
30. Vezzani A, Lang B, Aronica E. Immunity and inflammation in epilepsy. Cold Spring Harb Perspect Med. 2015;6:a022699. doi:10.1101/cshperspect.a022699
31. Gillinder L, Warren N, Hartel G, et al. EEG findings in NMDA encephalitis – a systematic review. Seizure. 2019;65:20–24. doi:10.1016/j.seizure.2018.12.015
32. Flanagan EP, Kotsenas AL, Britton JW, et al. Basal ganglia T1 hyperintensity in LGI1-autoantibody faciobrachial dystonic seizures. Neurol Neuroimmunol Neuroinflamm. 2015;2(6):e161. doi:10.1212/NXI.0000000000000161
33. Huang Q, Ma M, Wei X, et al. Characteristics of seizure and antiepileptic drug utilization in outpatients with autoimmune encephalitis. Front Neurol. 2018;9:1136. doi:10.3389/fneur.2018.01136
34. Reiber H, Peter JB. Cerebrospinal fluid analysis: disease-related data patterns and evaluation programs. J Neurol Sci. 2001;184(2):101–122. doi:10.1016/S0022-510X(00)00501-3
35. Yu Y, Wu Y, Cao X, et al. The clinical features and prognosis of anti-NMDAR encephalitis depends on blood brain barrier integrity. Mult Scler Relat Disord. 2021;47:102604. doi:10.1016/j.msard.2020.102604
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.