")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Factors Influencing Effectiveness of Peer Education Against Nonadherence to Antiretroviral Therapy Among Adult People Living with HIV/AIDS: A Pre-Post Intervention Study in Arsi Zone, Ethiopia
Authors Hussein M, Dibaba B , Wondu Y
Received 22 August 2019
Accepted for publication 20 December 2019
Published 9 January 2020 Volume 2020:12 Pages 1—7
DOI https://doi.org/10.2147/HIV.S228330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Mohammed Hussein,1 Bekele Dibaba,2 Yirga Wondu3
1Department of Pharmacy, College of Health Sciences, Arsi University, Asella, Oromia Regional State, Ethiopia; 2Department of Public Health, College of Health Sciences, Arsi University, Asella, Oromia Regional State, Ethiopia; 3Department of Midwifery, College of Health Sciences, Arsi University, Asella, Oromia Regional State, Ethiopia
Correspondence: Bekele Dibaba
Tel +2510910955032
Email [email protected]
Background: Nonadherence to antiretroviral therapy (ART) among people with HIV/AIDS can lead to drug resistance and death. Different studies have defined nonadherence, and it denotes at least one missed dose of ART within 28 days. One of the strategies to prevent nonadherence to ART could be peer education. However, published studies which test out whether or not peer education is effective for prevention of nonadherence to ART among adults living with HIV were not available. Moreover, published studies on factors discussing the success of peer education against nonadherence to ART were not available, so we conducted this study.
Objectives: To determine effectiveness of peer education against nonadherence to ART and identify factors influencing the effectiveness of peer education for prevention of nonadherence to ART among people living with HIV/AIDS in Arsi zone, Ethiopia.
Methods: An institution based pre-post intervention study was conducted. The intervention was giving peer education for three months. Frequencies and percentages were used to describe the data. Binary and multivariate logistic regressions were used to assess the variables.
Results: The data was collected from 355 and 319 people with HIV/AIDS at pre- and post-intervention stages, respectively. Experiencing an ART side effect, reminder to take ART, gender, marital status and monthly income were associated with nonadherence. More study participants who had not useda reminder to take ART service missed at least one dose of ART when compared to those who used a reminder to take ART service (adjusted odds ratio (AOR) =6.21; 95% CI=2.12–18.20).
Conclusion: Experiencing a side effect of ART influenced effectiveness of peer education negatively while using reminder to take ART influenced effectiveness positively. Peer education is effective for reduction of nonadherence to ART if it is used with reminder to take ART. This study can be a base for further studies that should be conducted in various areas, since peer education can be influenced by sociodemographic and economic factors.
Keywords: success, reduction, health, Oromia Regional State
Introduction
HIV/AIDS is a major problem in the world. In 2017 prevalence of HIV was 0.8% among adults. The new infections of HIV among adults in 2017 were 1.8 million. The majority of people living with HIV are located in low and middle income countries. In East and Southern Africa there were 800,000 new HIV infections in 2017.1
Treating HIV/AIDS with ART is needed against the prevalence of HIV to slow disease progression and reduce mortality. In 2018, an estimated 23.3 million people were receiving ART globally.2 However, there has been an inconsistency to ART. Nonadherence to ART among HIV infected adults in Mon State of Myanmar was 16% in 2016.3 Study in Brazil found that nonadherence to ART among patients initiating the therapy was 36.9% in 2005.4 A study conducted in Northwest Ethiopia indicated that nonadherence to ART among adult hospitalized patients was 19.1% in 2014.5
Nonadherence to ART is related to different factors. Study conducted in Northern Tanzania among HIV infected patients revealed that nonadherence was associated with younger age and unemployment.6 Study done in Yaoundé-Cameroon showed that change in ART regimen was significantly associated with increased likelihood of nonadherence.7 Study conducted in Dares Salaam, Tanzania indicated that nonadherence was high among patients on ART for long duration.8 Nonadherence to ART contributed to resistance of the virus to the ART.9
Since the consequence of nonadherence to ART is unpleasant, it has to be prevented or reduced. One of the strategies to reduce or prevent nonadherence to ART among adult people living with HIV/AIDS could be peer education, since peer education has been used with a number of target populations in developing countries. A systematic review and meta analysis on effectiveness of peer education in developing countries indicated that peer education is moderately effective at improving behavioral outcome, suggesting further research for success of peer education intervention.10 In contrast to the above meta analysis, a systematic review of European studies concluded that there is no clear evidence of the effectiveness of peer education concerning HIV prevention, adolescent pregnancy prevention and sexual health promotion in young people in the member of European Union countries suggesting further study.11
Peer education is teaching by members of similar age or health status. Peer education involves information sharing. Peer education attempts to influence knowledge, attitude and behavior.12 In our case peer education denotes peers with similar health status (people living with HIV and on ART).
Peer education interventions have been tried for different purposes. Study conducted in Khartoum, Sudan indicated that peer education intervention aiming at AIDS prevention among secondary school students found that the program improved participants' knowledge from 75.5–83.2%.13 Another study conducted in Osun State, Nigeria showed that peer education intervention significantly increased knowledge and attitude towards HIV/AIDS in school adolescent.14 Peer education intervention done in 2015 among secondary school students in Addis Ababa found that the students in intervention group demonstrated positive change in HIV related compressive knowledge.15
A systematic review conducted in 2015 indicated that peer education interventions are effective at reducing risk behavior among prisoners.16 Another systematic review performed in 2017 showed that peer education intervention among adults with type 2 diabetes is successful in improving clinical outcomes.17 Study conducted in Zimbabwe in 2014 indicated that at population level HIV incidence was not reduced by peer education intervention and concluded the program was disappointing.18
Even though effectiveness of peer education was established for different purposes as discussed above, published studies which relate the effectiveness of peer education for prevention or reduction of nonadherence to ART were not available. Moreover, published studies which identified factors influencing the effectiveness of peer education against nonadherence to ART were not available on the internet.
Materials and Methods
Study Area and Period
The study was conducted in six governmental health facilities found in Arsi zone, Oromia Regional State, Ethiopia. The capital town of Arsi zone is Asella which is 175 km from Addis Ababa, the capital city of the country. Twenty-five health facilities are giving ART service in Arsi zone at the time of data collection for this study. The data was collected from six health facilities found in the zone. These are Dhera health center, Bokojji health center, Kersa health center, Robe hospital, Bokojji hospital and Abomsa hospital.
The duration of the study was from January 1, 2018 to July 1, 2018.
Study Design and Measurement
Institution based pre-post intervention was carried out. The study had three stages. These were: pre-intervention, intervention and post intervention stages. At pre-intervention stage base line data was collected from study participants. At intervention stage peer education had been given to the study population by the peers with similar health status of study participants for three months. At the post-intervention stage the same questionnaire that was used at pre-intervention stage was administered to the same study population. The intervention was peer education and its effectiveness was measured by missed dose of ART within 28 days after the intervention had completed.
Target Population
Adults living with HIV/AIDS and on antiretroviral therapy follow-up in Arsi zone, Ethiopia.
Study Population
Adults living with HIV/AIDS and aged greater than 18 years on antiretroviral therapy follow-up in purposely selected Arsi zone health facilities.
Sample Size
The sample size was calculated to fulfill the needs of this study. We used EPI INFO version 7.0.2.1 stat calc setting error probability of 0.05, proportion of 0.35 and 10% nonresponse rate. With the above criteria the sample size was 384.
Sampling Procedure
In the study area (Arsi zone) there were 25 health facilities which give ART services. Out of these health facilities six were selected purposely to include health facilities which had peer educators and high number of clients who were on ART follow-up. Then equal numbers of adults on ART follow-up were randomly selected from each of the health facilities to include them in the study.
Data Collection Method
The data was collected by the nurse giving ART services in each of the health facilities. The data collectors were trained and oriented regarding the purpose of the study.
Data collection tool was a questionnaire. The questionnaire included questions on sociodemographics and side effect of ART. Baseline data was collected immediately before the intervention. Then three months after the intervention had completed post-intervention data was collected.
Data Analysis
SPSS version 21 (IBM Corporation, Armonk, NY, USA) was used for analysis. Data collected before intervention was compared to data collected at post-intervention. Binary and multivariate logistic regressions were used to see the association between variables.
Ethical Consideration
Ethical clearance was obtained from Arsi university ethical review board. Permission letter to conduct the study was obtained from Arsi zone health office. Consent was obtained from the study participants. The participants consent was written informed consent and this study was conducted in accordance with the Declaration of Helsinki.
Results
Sociodemographic Characteristics
The data was collected from 355 participants at pre-intervention stage and this gives a response rate of 92.4% since the sample size is 384. At post-intervention stage the numbers of studied participants have decreased to 319 giving the response rate of 83.1%.At pre-intervention 146 (41.1%) and at post-intervention 104 (32.6%) study participants missed at least one dose of ART within 28 days (nonadherent to ART).
At pre-intervention 39.1% and 43% males and females missed at least one dose of ART within 28 days. At post-intervention stage 34.1% and 30.8% females and males had missed at least one dose of ART within 28 days. This indicates that nonadherence to ART had reduced by 8.3% among males and 8.9% among females.
In individuals who had a secondary school education, 53.3% and 39.1% had missed at least one dose of ART within 28 days at pre- and post-intervention stages respectively. This indicates that nonadherence among this group was high. However, the decline in number of respondents who missed at least one dose of ART is great. That is (53.3–39.1%) = 14.2%. The reduction in number of study participants (whose monthly incomes were 510=1000EBR) who missed at least one dose of ART is also huge.
Major reduction in nonadherence to ART was seen among those greater than 50 or 18–19 years of age, never married, divorced, who had a secondary school education, and monthly income 501–1000 at post intervention stage (Table 1).
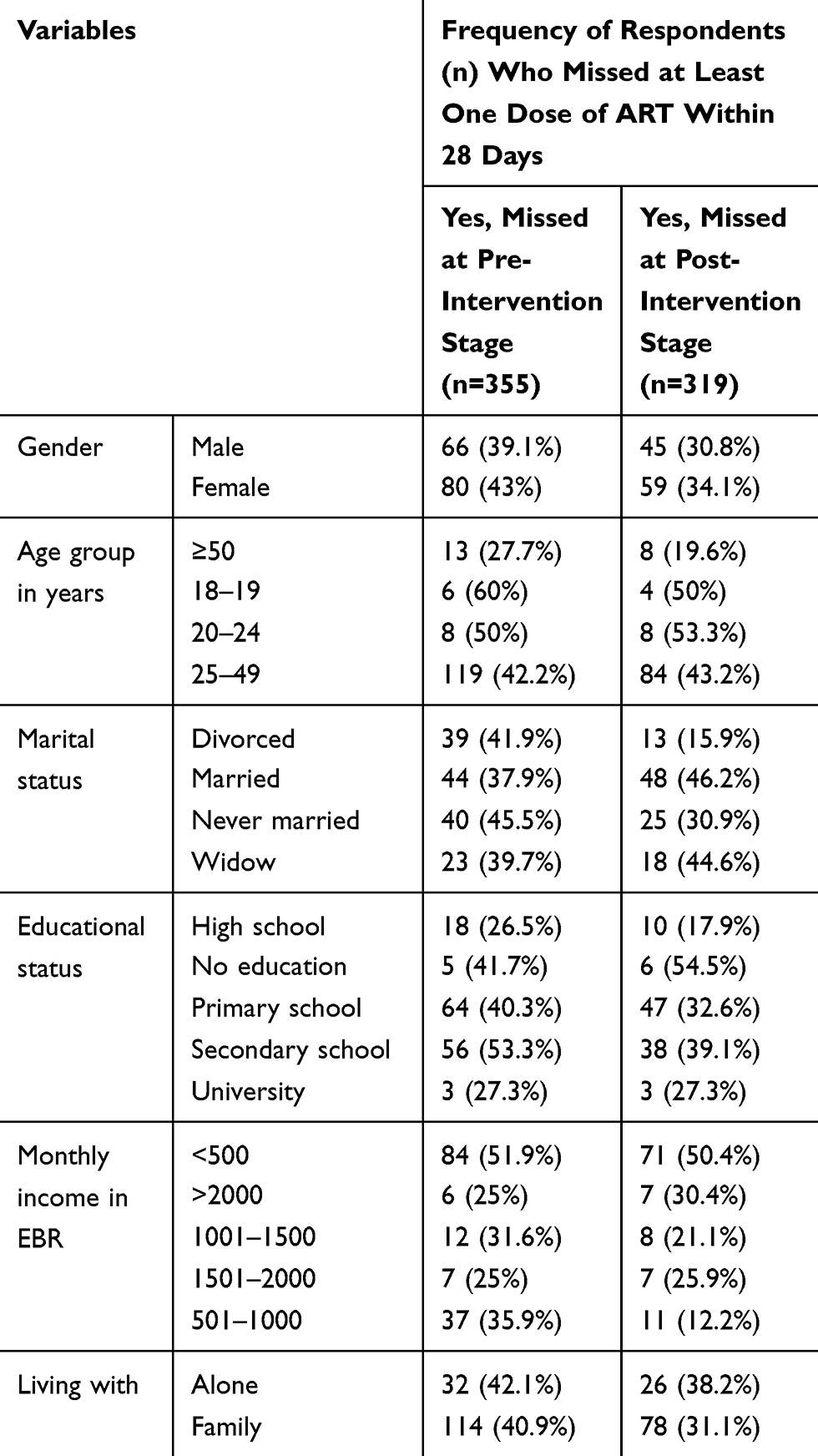 |
Table 1 Sociodemographic Characteristics with Their Corresponding Missed Doses of ART Among the Study Participants |
Factors Associated with Effectiveness of Peer Education Among Study Participants (Analysis of Post-Intervention Data)
The frequencies of all variables this study at post-intervention stage were entered into binary logistic regression one by one to see their significance at p-value of 0.05. Finally, all significant variables were entered into binary logistic regression at once to see the association between the variables having in mind that the intervention with peer education is constant for all respondents, the following result found:
- At post-intervention stage, a greater number of study participants who had not reported side effect of their ART had more likely missed at least one dose of ART in the last 28 days (AOR = 0.06) when compared to their counterparts (those who had not reported side effect of their ART).
- A greater number of respondents who had not used reminder had more likely missed at least one dose of ART within 28 days when compared to their counterparts at post-intervention stage (AOR = 6.21; 95%CI = 2.12–18.20).
At post-intervention stage it was more likely that a greater number of females missed at least one dose of ART within 28 days when compared to males (AOR=0.06) (Table 2).
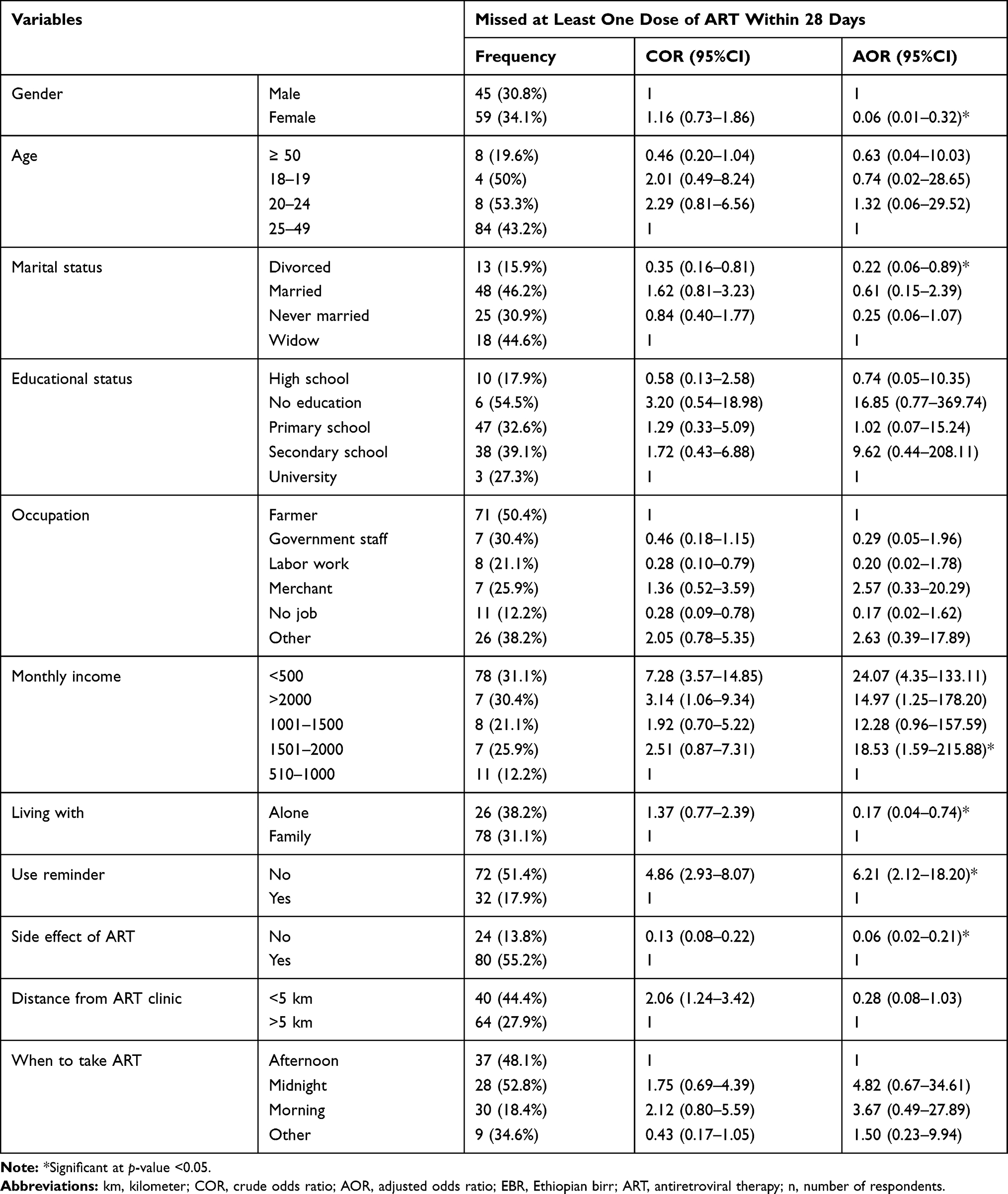 |
Table 2 Variables Associated with Effectiveness of Peer Education Among Respondents (Post-Intervention Data Analysis) (n=319) |
Discussion
Published studies which tested whether peer education is effective or not to reduce or prevent non- adherence to antiretroviral therapy were not available. Similarly studies on factors influencing effectiveness of peer education for prevention of nonadherence to ART were not available. So we could not able extensively compare the results of our study with other findings.
In our study at post intervention stage prevalence of nonadherence was 32.6% among the study participants. However, cross-sectional study conducted in Shiraz showed that prevalence of nonadherence was 30.4%.19 This small difference between our study and that of study conducted in Shiraz may be due to the fact that studies were done in different sociocultural areas. More over the difference could be due to differences in design of the studies that is in our study we used pre-post intervention study but the other study is cross sectional.
The result from our study revealed that after intervention 34.1% of females and 30.8% of males were nonadherent. This indicated that more improvement was among males than females. However, a critical review of peer education was beneficial creating some behavior change, specifically for women was effective.20 This difference could be because of among whole adult people living with HIV/AIDS and age greater than 18 years but the critical appraisal was reviewed effects of peer sexual education among college campuses.
At post intervention stage 42.6% of study participants who had monthly income of less than 500 Ethiopian birr missed at least one dose of ART within 28 days which means 42.6% of them were nonadherent to their medication (ART). Income can be correlated to nonadherence to ART since those with low monthly income work hard and for long hours leaving them short of time to take the medication from the ART clinic on schedule. At pre-intervention stage it was 51.9%. This indicates that there was improvement in adherence to the ART among this group of population after intervention with peer education. However, the published study that support or contrast this finding was not available.
In our study nonadherence was 0.17 times more likely to occur among those who live alone when compared to those who live with their family. This denotes that more people who live with their family were nonadherent to ART. Similarly, study conducted in Northern Ethiopia found that nonadherence were more likely to occur among those who live with their parents than those who live alone.21 Further research is needed to justify why more people who live with their family were nonadherent to ART.
In our study respondents who reported side effect of ART were more inconsistent to the ART despite the intervention with peer education. This indicates that side effect of the medication (ART) has the power to influence the effectiveness of peer education.22 Similarly nonadherence was associated with self-reported three or more adverse reactions.4
In our study fewer of those who use a reminder were nonadherent to ART after intervention with peer education. It is supported by study that forgetfulness was the major reported reason for nonadherence to ART.23 This indicates that even if peer education is given for the people on ART follow-up without using a reminder to take their medication (ART); the intervention with peer education may not be effective.
Conclusion
Peer education intervention was effective for reducing nonadherence to ART if it is used with reminder since at post-intervention stage prevalence of nonadherence decreased. Side effects of the therapy have influenced effectiveness of peer education negatively however using a reminder to take ART influenced the effectiveness of peer education positively. Other variables which were associated with nonadherence at post intervention stage include monthly income, gender marital status and with whom the ART user lives.
Published studies were not available regarding effectiveness of peer education against nonadherence to ART and factors disturbing its effectiveness among people living with HIV/AIDS. So we recommend more studies in different areas because peer education intervention were associated with sociodemographic factors (gender, marital status and with whom the ART user lives) and economic factors (monthly income).
Acknowledgments
The authors acknowledge Arsi University for financial support. The authors forward their deepest thanks to Arsi zone Health Office for cooperation and permission to conduct this study. The authors express appreciation to the study participants, data collectors and supervisors.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. UNAIDS [home page on the internet]. Global HIV and AIDS statistics. 2011. Available from: http://aidsinfo.unaids.org/.
2. World Health Organization [home page on the internet]. Global Health Observatory (GHO) data. 2018. Available from: https://www.who.int/gho/en.
3. Aye WL, Puckpinyo A, Peltzer K. Non adherence to antiretroviral therapy among HIV infected adults in Mon State of Myanmar. BMC Public Health. 2017;17(1):391. doi:10.1186/s12889-017-4309-5
4. Bonolo PF, Cesar CC, Acurcio FA, et al. Non –adherence among patients initiating antiretroviral therapy: a challenge for health professionals in Brazil. AIDS. 2005;19(4):S5–S13. doi:10.1097/01.aids.0000191484.84661.2b
5. Tsega B, Srikanth BA, Shewamene Z. Determinants of non-adherence to antiretroviral therapy in adult hospitalized patients, Northwest Ethiopia. Patient Prefer Adherence. 2015;9:373–380. doi:10.2147/PPA
6. Semvua SK, Orrell C, Mmbaga BT, Semvua HH, Bartlett JA, Boullee AA. Predictors of non-adherence to antiretroviral therapy among HIV infected patients in Northern Tanzania. PLoS One. 2017;12(12):e01894–e0189460. doi:10.1371/journal.pone.0189460
7. Fonsah JY, Njamnshi AK, Kouanfack C. Adherence to Antiretroviral Therapy(ART) in Yaounde-Cameroon: association with opportunistic infections, depression, ART regimen and side effects. PLoS One. 2017;12(1):e0170893–e0170893. doi:10.1371/journal.pone.0170893
8. Muya AN, Geldsetzer P, Hertzmark E, et al. Predictors of non-adherence to antiretroviral therapy among HIV infected adults in Dar es Salaam, Tanzania. J Int Assoc Provid AIDS Care. 2015;14(2):163–171. doi:10.1177/2325957414539193
9. Yuan Y, Xing H, Wang XY, et al. The prevalence of HIV-1 drug resistance and associated factors in AIDS patients receiving HAART in Zhecheng country, Henan province. Zhonghua Yu Fang Yi Xue Za Zhi. 2011;45(7):619–624.
10. Medley A, Kennedy C, O’Reilly K, Sweat M. Effectiveness of peer education interventions for HIV prevention in developing countries: a systematic review and meta-analysis. AIDS. 2009;21(3):181–206.
11. Tolli MV. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: a systematic review of European studies. Health Educ Res. 2012;27(5):904–913. doi:10.1093/her/cys055
12. Joanne M, Ann MR, Mitch D, Natalie S; for National Center for Education and Training on Addiction (NCETA) [home page on the Internet]. Australia: peer education: from evidence to practice. 2003. Available from: http://nceta.flinders.edu.au/files/7812/5548/1521/EN65.pdf.
13. Ali MHM, Osman OB, Ibrahim MAM, Ahmed WAM. The effect of AIDS peer health education on knowledge, attitude and practices of secondary school students in Khartoum, Sudan. AIMS Public Health. 2015;2(4):718–726. doi:10.3934/publichealth.2015.4.718
14. Adeomi AA, Adeoye OA, Asekun-Olarinmoye EO, Abodunrin OL, Olugbenga-Bello AL, Sabageh AO. Evaluation of the effectiveness of peer education in improving HIV knowledge, attitude and sexual behaviours among in school adolescents in Osun State, Nigeria. AIDS Res Treat. 2014;2014:131756.
15. Menna T, Ali A, Worku A. Effects of peer education intervention on HIV/AIDS related sexual behaviors of secondary school students in Addis Ababa, Ethiopia: a quasi-experimental study. Reprod Health. 2015;12:84. doi:10.1186/s12978-015-0077-9
16. Bagnall AM, South J, Hulme C, et al. A systematic review of the effectiveness and cost-effectiveness of peer education and peer support in prisons. BMC Public Health. 2015;15:290. doi:10.1186/s12889-015-1584-x
17. Gatlin TK, Serafica R, Johnson M. Systematic review of peer education intervention programmes among individuals with type 2 diabetes. J Clin Nurs. 2017;26(23–24):4212–4222. doi:10.1111/jocn.13991
18. Campbell C, Scott K, Mupambireyi Z, et al. Community resistance to peer education programme in Zimbabwe. BMC Health Serv Res. 2014;14:574. doi:10.1186/s12913-014-0574-5
19. Motazedian N, Sayadi M, Firoozbakhtian A. Non-adherence to antiretroviral medication in Shiraz, 2014: a cross- sectional study. Afr Health Sci. 2018;18(2):384–393.
20. Wong T, Pharr JR, Bungum T, Coughenour C, Lough NL. Effects of peer sexual health education on college campuses: a systematic review. Health Promot Pract. 2018:1524839918794632. Available from http://www.ncbi.nlm.nih.gov/pubmed/30141355. Accessed December 27, 2019.
21. Gebrezgabher BB, Kebede Y, Kindie M, Tetemke D, Abay M, Gelaw YA. Determinants to antiretroviral treatment non-adherence among adult HIV/AIDS patients in northern Ethiopia. AIDS Res Ther. 2017;14:16. doi:10.1186/s12981-017-0143-1
22. Trotta MP, Ammassari A, Cozzi-Lepri A, et al. Adherence to highly active antiretroviral therapy is better in patients receiving non-nucleoside reverse transcriptase inhibitor- containing regimens than in those receiving protease inhibitor-containing regimens. AIDS. 2003;17(7):1099–1102. doi:10.1097/00002030-200305020-00026
23. Sangeda RZ, Mosha F, Aboud S, et al. Predictors of non-adherence to antiretroviral therapy at an urban HIV care and treatment center in Tanzania. Drug Healthc Patient Saf. 2018;10:79–88. doi:10.2147/DHPS
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.