")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Factors Correlated with Practices Regarding Care of Dengue Patients Among Nurses from 94 Primary Care Units in a High- Risk Province in Southern Thailand
Authors Suwanbamrung C , Le CN , Phetphrom P, Kamneatdee P, Nontapet O, Kaewket N
Received 15 October 2020
Accepted for publication 23 November 2020
Published 31 December 2020 Volume 2020:13 Pages 2043—2056
DOI https://doi.org/10.2147/JMDH.S286737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Charuai Suwanbamrung,1 Cua Ngoc Le,1 Phatcharaphon Phetphrom,2 Penpanee Kamneatdee,2 Orratai Nontapet,3 Nattavadee Kaewket2
1Excellent Center for Dengue and Community Public Health (EC for DACH), School of Public Health, Walailak University, Thailand; 2School of Public Health, Walailak University, Thailand; 3Excellent Center for Dengue and Community Public Health (EC for DACH), School of Nursing, Walailak University, Thailand
Correspondence: Charuai Suwanbamrung
Excellent Center for Dengue and Community Public Health (EC for DACH), School of Public Health, Walailak University, Thailand
Email [email protected]
Background: In Thailand, primary care units (PCUs) play a part in the health assessment, diagnosis, care, basic treatment and referral of patients suffering from dengue.
Methods: In Nakhon Si Thammarat province in Thailand, we (i) undertook assessment of the personal information, experience, knowledge, attitudes, preparation of equipment and use of medical supplies of nurses in PCUs with regard to dengue patient care (DPC); (ii) analyzed the factors and practices of nurses regarding DPC; (iii) explored nurses’ opinions regarding DPC in PCUs. A cross-sectional mixed methods of collecting data consisted of quantitative and qualitative methods. The study cohort was 94 nurses from 94 PCUs in an area of high risk of dengue outbreaks. The quantitative component involved questionnaires. The qualitative component consisted of nurses’ discussions in focus groups. Spearman’s test was employed to analyze quantitative data, and thematic analyses were employed for qualitative data.
Results: Of 94 nurses from 94 PCUs, 77.7% (n = 73) had a poor knowledge level of DPC and negative attitude, preparation of equipment was carried out by 60.6% (n = 58), and 1 to 6 aspects of DPC were at good practice level: 88.3% (n = 83), 87.2% (n = 82), 85.1% (n = 80), 50.0% (n = 47), 51.1% (n = 48) and 77.7% (n = 73). There was no significant correlation (i) between the knowledge, attitudes and practices with regard to DPC (P > 0.05); (ii) with practice guidelines for dengue prevention (P > 0.05). The quantitative results were related to the four main themes of the qualitative study.
Conclusion: There was a few who had good knowledge and positive attitude levels among participants, and > 90% of all nurses had good practices regarding DPC. PCU nurses need training and supporting equipment to carry out a DPC program.
Keywords: dengue patient care, nurse, primary care unit, mixed methods, high risk of dengue
Background
“Dengue” is a viral infection caused by the mosquito Aedes aegypti. The virus responsible for causing dengue is called the dengue virus (DENV). There are four DENV serotypes, so it is possible to be infected four times.1 There have been outbreaks of dengue in tropical and subtropical zones in many countries. It has been estimated that 2.5 billion people worldwide are at risk of infection by the DENV, and signs and symptoms have been found in 50–100 million people. A total of 20,000 deaths have been reported for every 100,000 dengue cases.2,3 Dengue can lead to death because only nonspecific treatment is available. Dengue can manifest as dengue fever (DF), dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS).2
In Thailand, the dengue epidemic has persisted for >60 years. Dengue was first identified in 1958.4 The trend in the dengue outbreak has followed an ambiguous pattern. For example, there were fewer cases in 1999–2000 due to dengue-prevention campaigns, but there was increased mortality. Guidelines on dengue management in Thailand are issued by the Thai Ministry of Public Health, and these guidelines incorporate the guidelines for dengue management published in 1997 and 2009 by the World Health Organization.2,3,5
Nakhon Si Thammarat province (NSTP) is in the southern part of Thailand. It consists of 23 districts, 165 sub districts, 1551 villages and has a population of 1,580,687. It is associated with a high risk of dengue outbreaks. In 2013, 2014, 2015, 2016, 2017 and 2018, it exhibited morbidity cases per 100,000 people of 297.69, 199.11, 126.42, 147.33, 185.65 and 242.29, and mortality of 0.18, 0.20, 0.10, 0.00, 0.10 and 0.08%, respectively.4,6 NSTP has a prevention and control program for dengue which is in accordance with the dengue-control program set up by the Thai government. The severity of dengue is related to all stakeholders in the community: patients, villagers, healthcare staff and governmental officials who come from other districts to NSTP. In NSTP, there are ~235 nurses working at 235 primary care units (PCUs) in 165 sub districts. They play a part in the health assessment, diagnosis, care, basic treatment and referral of dengue patients.6
Providers of primary care are involved in dengue management for the community.7,8 Thus, nurses play an important part in providing healthcare services in both the community and in hospitals. Adequate knowledge can help a nurse provide health education to the general public and patients. In Thailand, the nurses’ roles in primary healthcare settings involve five components: (i) health assessments and basic treatment; (ii) health promotion; (iii) disease prevention; (iv) care for patients with chronic ailments and older patients; (v) self-care assessments.9,10 In particular, nurses working in communities help people improve their health status and prevent disease. Research is focused on nurses in PCUs who believe that health is affected by several factors, including genetics, lifestyle and environment. Instead of waiting for patients to visit hospitals with illnesses, the nurses visit communities to help people improve their health and prevent diseases.
In several studies, the concept of knowledge, attitude and practice–outcome has been used. One study showed that changes in a person’s behavior are based on his/her knowledge and attitude.11–13 The outcome measures of dengue management are mortality and morbidity rates, which must improve upon implementation of educational programs. The knowledge, attitudes and sociodemographic factors of nurses in PCUs in relation to dengue-patient care (DPC) in Thailand are not clearly understood. Moreover, educational programs for dengue are needed in hospitals.14 However, Ang and colleagues showed that 51.9% (n = 94) of primary care practitioners in two public hospitals did not provide information on dengue prevention to patients.7 Mohammed and colleagues showed that 348 healthcare professionals needed to attend training programs because their knowledge, attitudes and practices did not satisfy the requirements for care of dengue patients.15 Therefore, whether factors such as knowledge (causes, signs, symptoms, treatments) and attitudes affect nurses’ practices of DPC (eg, initial assessment, basic care, diagnosis for patients in shock, intravascular infusion, patient referral, counseling on dengue prevention) has yet to be studied.
If PCU nurses do not have sufficient knowledge regarding DPC, this means that they cannot have a good attitude and practice care for such patients. According to relevant studies, the DPC practices of nurses are important for the prevention, control and treatment of dengue in the community and in hospitals.16
Studies on the factors affecting DPC provided by nurses in NSTP are lacking. Hence, we conducted research on the risk factors (eg, demographic and social factors, knowledge and attitudes) affecting DPC practices by nurses. In this way, we wished to explain (at least in part) the high mortality and mortality rates of dengue. Our methodology involved: (i) assessing the personal information, experience, knowledge, attitude, preparation of equipment and use of medical supplies of nurses in PCUs regarding DPC; (ii) analyzing the factors and practices of nurses regarding DPC; (iii) exploring nurses’ opinions regarding DPC in PCUs.
Methods
Study Design
A cross-sectional mixed-methods study17,18 was chosen for the quantitative component of this research. We assessed factors such as personal information, experience, knowledge, attitude and practices regarding DPC among nurses in PCUs. Also, we analyzed the correlation between factors and practices regarding DPC among nurses in PCUs. The qualitative component of our study involved collecting data from focus groups to explore nurses’ opinions regarding DPC. The synthesis of these two components of our study was undertaken at the time of interpretation of results.
Research Setting
The PCU is the first level of primary care in Thailand. Provision of primary care in the community is through a multisectoral approach involving implementation of district health systems. This system allows alignment of health services for effective and efficient processes through introduction of service plans, and establishes multidisciplinary care teams at the community level.19
The PCU consists of the director of the PCU, a public health officer, a nurse, an office administrator and a general assistant. In NSTP, there are 235 PCUs in 165 sub districts, and a PCU has 3–4 health providers.6 The role of nurses in primary care has evolved markedly in the last 50 years. Nurses provide clinical and management skills which, if used to their fullest potential, can enhance the primary care team and improve patient care.20 Hence, the role of nurses in DPC involves health assessment, diagnostics, treatment and referral to a district hospital or tertiary hospital.
Quantitative Study
Study Design and Sample Size
The total sample size of nurses was calculated using the G*Power 3.1 calculus program (www.gpower.hhu.de/en.html.3.11.61).21 The parameters were: test family = exact; statistical test was correlation; a bivariate normal model was used; α = 0.05; power = 0.95. The sample size suggested was 83 nurses, which was increased by 10% to account for lost samples. A simple random-sampling method was used to select 94 PCUs. One nurse from each PCU was employed to answer questionnaires.
Research Instruments
The content validity was assessed by three experts. The measure of reliability was conducted on a sample of 30 nurses. The Content Validity Index and measure of reliability (Cronbach’s alpha) were 0.93 and 0.87, respectively. The components of quantitative questionnaires were: (i) personal factors; (ii) knowledge; (iii) attitudes; (iv) practices regarding dengue patient care; (v) preparation of equipment and use of medical supplies.
The components of knowledge consisted of 14 questions about dengue, including the causes, signs and symptoms. Each correct answer corresponded to 1 point, and each wrong answer corresponded to 0 points. The knowledge level was classified into two sublevels based on Bloom’s cutoff point.15,22 That is, “good” knowledge corresponded to a percentage of correct answers ≥80% (≥11 points), and “poor” knowledge corresponded to a percentage of correct answers <80% (<11 points).
The components of attitude consisted of 10 questions about viewpoints on the severity, prevention and primary care of dengue. The classification of the attitude level about dengue patient care had a cutoff point of 80%.15,16 A positive attitude and negative attitude to DPC corresponded to a mean score ≥8 points and <8 points, respectively.
The section on the practices of DPC comprised 47 questions that were divided into six aspects. The rating scale for practice consisted of five levels with the corresponding scores: “every time”, “almost”, “sometime”, “no action”, and “non-appearance” corresponded to 5, 4, 3, 2 and 1 points, respectively. Practice levels in each aspect were classified according to Bloom’s cutoff point of 60% 80%.22 For health practices, “good practice” involved a cutoff point of 90% of the total score in each of following: (i) initial assessment of primary care (five items), 22 out of a total of 25 points; (ii) practice in the first 2 days of fever (seven items), 31 out of 35 points; (iii) practice in diagnosing DFS (12 items), 54 out of 60 points; (iv) practice of intravenous infusion (four items), 18 out of 20 points; (v) practice of referring patients (13 items), 58 out of 65 points; (vi) guiding practice to prevent DF (six items), 27 out of 30 points.
The section on preparation of equipment and use of medical supplies provided the answers “yes”, “no”, and “not sure”, but remarks could also be given. We looked at eight aspects: (i) mercury sphygmomanometer and cuff of sizes small, medium and large; (ii) blood glucometer; (iii) hematocrit centrifuge; (iv) 5% dextrose in normal saline solution, 5% dextrose in lactated Ringer’s solution, or 5% dextrose acetar Ringer capacity 500 mL; (v) oral resuscitation solution and nasogastric tube of sizes 8, 14, 16 and 18; (vi) use of intravenous fluids, and use of cannula sizes 18, 20, 21, 22 and 23; (vii) manual on management of dengue patients; (viii) training of healthcare providers for dengue and guidelines for clinical practice. Practice levels in each aspect were classified according to Bloom’s cutoff point of 80%.
Collection and Analyses of Data
The PCU sent the self-administered questionnaire by post. Data were collected from October 2018 to August 2019. Differences in personal factors, knowledge, attitudes, preparation of equipment and use of medical supplies, and DPC practices were determined by Spearman’s test; p < 0.05 was considered significant.
Qualitative Study
Participants for Focus-Group Discussions
The qualitative component of our study was based on discussions from focus groups. Nurses’ experiences regarding DPC were documented. A purposive sampling method was used for 23 of 94 nurses who answered the questionnaires and who provided quantitative data. There were 23 nurses from 23 PCUs in 23 districts of NSTP. There were two focus groups, with 11 and 12 nurses in each group. The moderator of the group discussion was a researcher (Charuai Suwanbamrung) who took notes regarding nonverbal communication. A second researcher (Orratai Nontapet) took notes related to verbal communication. The two researchers wrote up the notes after the focus-group discussion.
Questions
The two groups discussed five open-ended questions regarding DPC: (i) What are your suggestions for dengue prevention based on the PCU? (ii) What do you think of the assessment and diagnosis of dengue in your PCU? (iii) What do you recommend for the care of dengue patients during infection, such as during critical illness and recovery periods? (iv) What do you advise dengue patients to do to look after themselves upon hospital discharge? (v) How do you prepare equipment and use medical supplies for dengue patients in the PCU?
Analyses of Qualitative Data
Next, we used a simple randomization and purposive method for inviting nurses representative of their PCU for group discussion. Qualitative data were analyzed based on themes. Analyses of qualitative data involved: (i) reading and re-reading the responses to understand the data; (ii) coding key words; (iii) assigning categories to key words; (iv) interpreting the meaning regarding the quotes from nurses; (v) determining the themes.23 Themes were returned to three nurses (who were randomized) to recheck the interpretations made by the researchers.
Results
Quantitative Study
Personal Factors
Among the 94 participants, 85.1% were senior clinical nurses (n = 80), and 91 females (96.8%). Also, 57 nurses (60.6%) were aged ≤45 years, and 76 nurses (80.9%) had ≥10 years of working experience (mean ± SD = 20.8 ± 8.9 years). A total of 71 nurses (75.5%) had worked in their current PCU for ≤10 years (7.8 ± 6.8 years). During a 5-year period, the number of nurses who had experience of caring for dengue patients in the fever phase, shock phase and recovery phase was 70 (74.5%), 11 (11.7%) and 43 (45.7%), respectively. The number of nurses who could carry out the tourniquet test, administer intravenous fluids for patients, refer patients in shock to a tertiary hospital, care for dengue patients who died subsequently and travel to prevent diseases was 71 (75.5%), 14 (14.9%), 11 (11.7%), 1 (1.1%) and 69 (73.4%), respectively (Table 1).
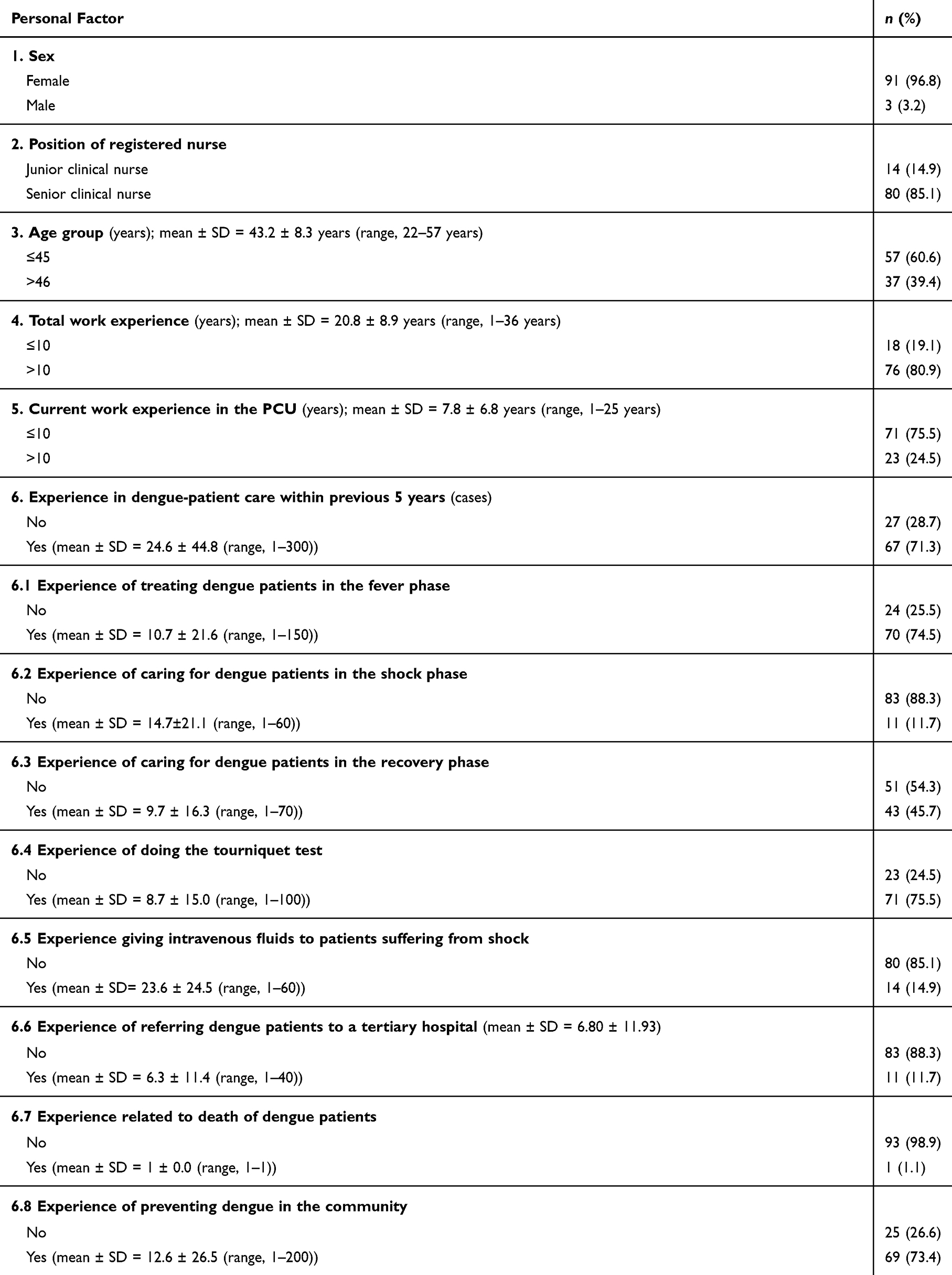 |
Table 1 Personal Factor of Nurses in 94 PCUs |
Knowledge Regarding DPC
The total knowledge regarding DPC in general as well as the causes and symptoms of dengue in particular were classified into two levels (cutoff point = 80%): 22.3% (n = 21) had a good knowledge level, and 77.7% (n = 73) had a poor knowledge level. Three of the 14 items (numbers 2, 4 and 7) had negative questions and had low percentages of correct answers: 31.9% (n = 30), 35.1% (n = 33) and 26.6% (n = 50), respectively. The highest percentage of correct answers (96.8%) corresponded to the knowledge that the four serotypes of the DENV can lead a patient to acquire DF more than once (item 3). Also, 95.7% of nurses knew that A. aegypti is a dengue-transmission vector that lives in small houses and has black and white stripes (item 10) and that a patient can be infected with the DENV several times (item 14). Finally, 94.7% of nurses recognized that the signs and symptoms of DHF include plasma leakage and a decrease in the platelet count (item 1) (Table 2).
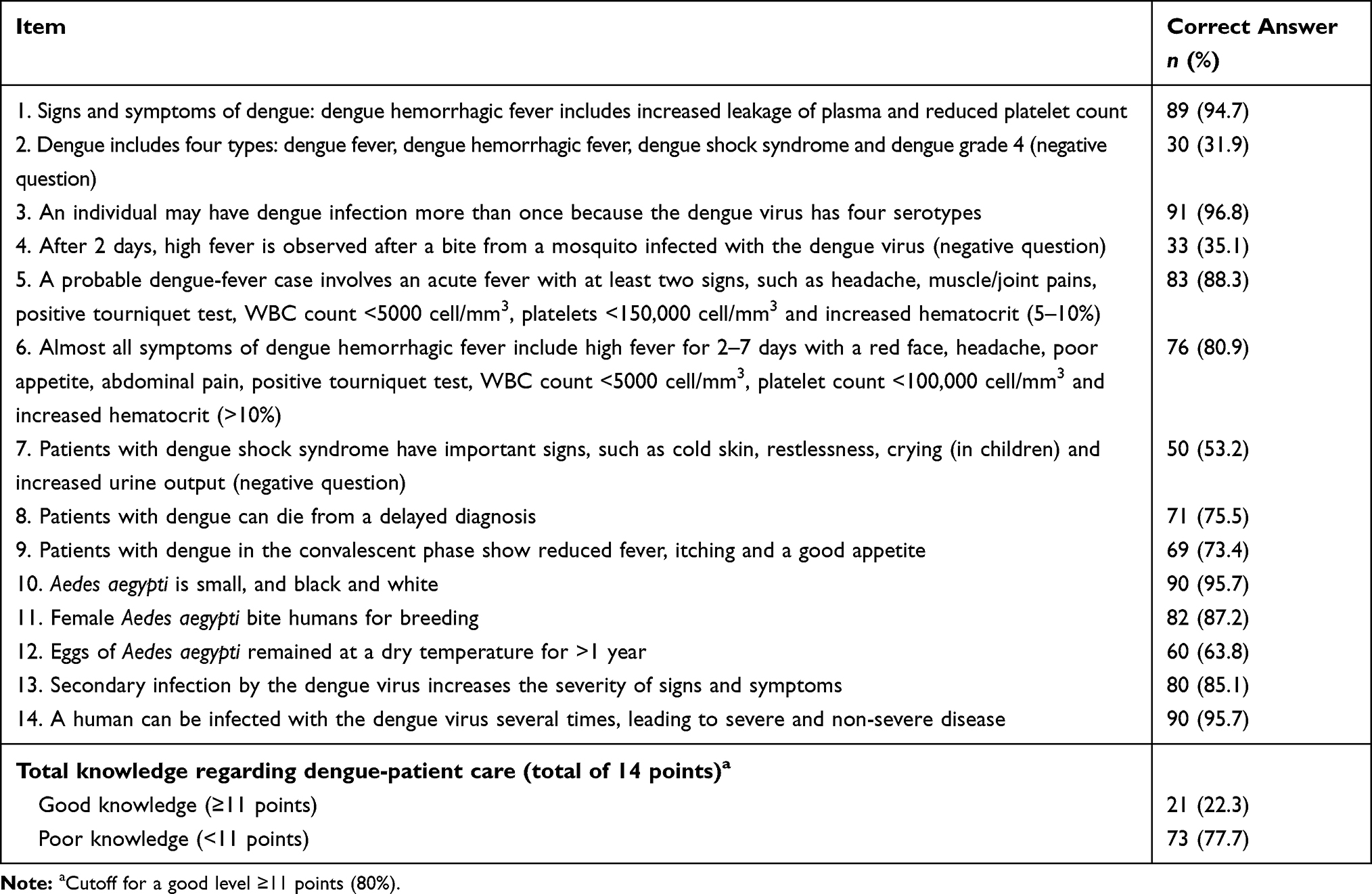 |
Table 2 Number and Percentage of Correct Answers of Knowledge Regarding Dengue-Patient Care |
Attitudes Regarding DPC
The total attitude regarding DPC was classified into two levels (cutoff point = 80%). Only 21 nurses had a positive attitude (22.3%), and 73 nurses (77.7%) had a negative attitude towards DPC. The percentage of positive attitudes in 10 items was 25.5%–100%. Three items corresponded to <80% with regard to the following statements: “All stakeholders are important in participating in the prevention and control of dengue” (25.5%); “Quick notification of a health official (within 72 h) after a dengue case is found should be done” (31.9%); “A probable dengue case needs investigation if the patient has a high fever and red face for >2 days” (69.1%) (Table 3).
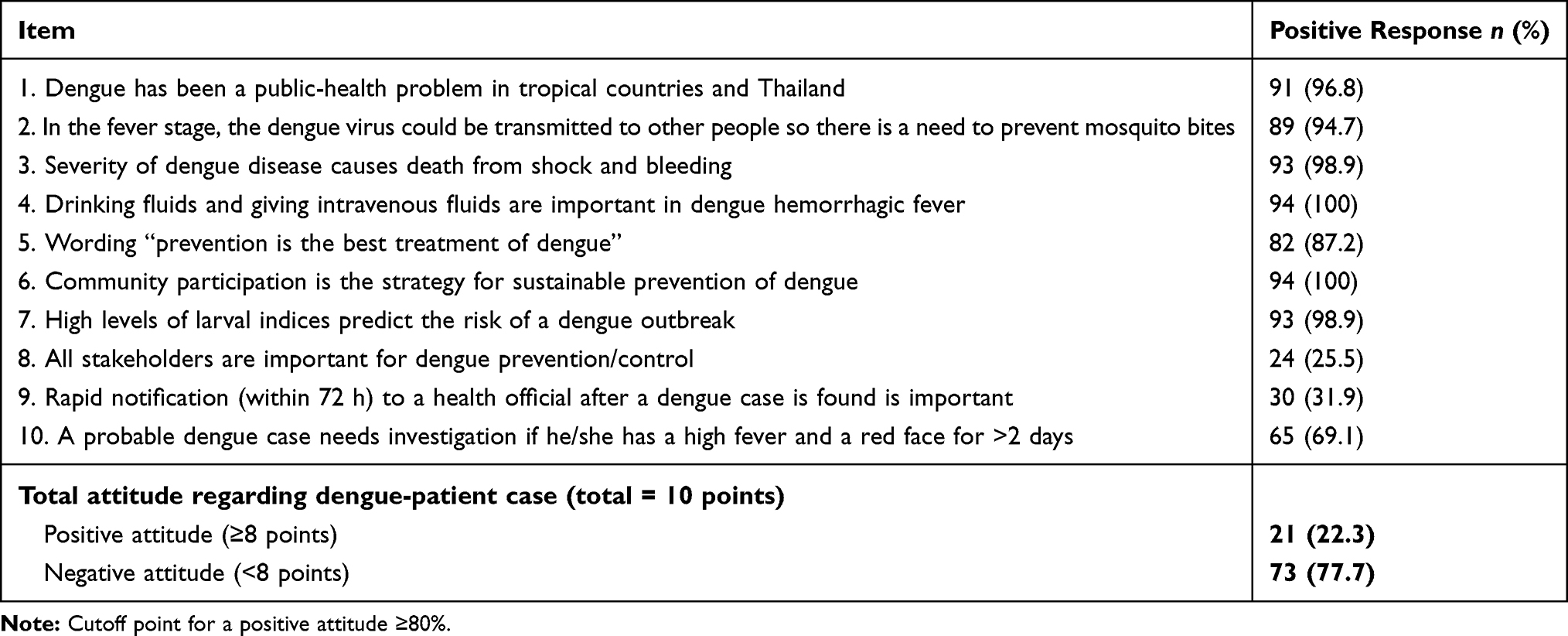 |
Table 3 Number and Percentage of Positive-Attitude Responses to Items Regarding Dengue-Patient Care |
Preparation of Equipment and Use of Medical Supplies in PCUs
Ninety-four nurses from 94 PCUs distributed in 23 districts provided information. Nurses in 58 PCUs (60.6%) prepared equipment and used medical supplies in PCUs at a cutoff of >80%; the other 36 PCUs (39.4%) had a cutoff of <80%. The highest prevalence for preparation of equipment, and use of medical supplies was item number 2 (blood glucometer), which was used by nurses in 91 PCUs (96.8%). In 32 PCUs (34%), nurses could carry out aspect number 1 (mercury sphygmomanometer and cuff of sizes small, medium and large) (Table 4).
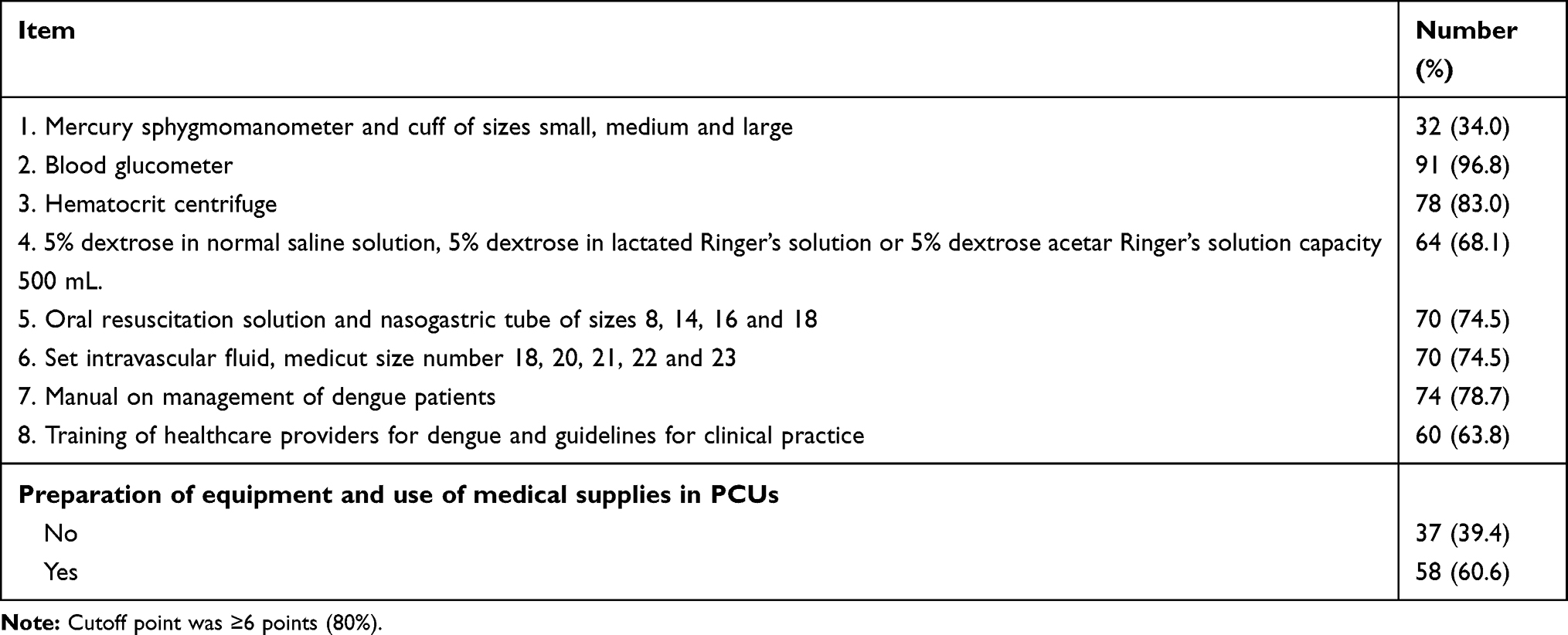 |
Table 4 Number and Percentage for Nurses Preparing Equipment and Using Medical Supplies in PCUs |
DPC Practices
With respect to DPC practices, we focused on six aspects, as shown below. The first aspect was initial assessment of a patient visiting the PCU/hospital for screening of dengue infection (five items). We found that 88.3% (n = 83) of nurses could practice screening for suspected cases of dengue well. Nearly all nurses could measure blood pressure, body temperature and respiratory rate.
The second aspect was basic practices after meeting dengue patients within the first 2 days of the fever phase (seven items). We found that 87.2% (n = 82) of nurses could provide primary care for patients. For example, they always recommended patients to use paracetamol to reduce fever instead of aspirin, and encouraged patients to drink liquids such as fruit juice or mineral water.
The third aspect was the practice guideline for the dengue diagnosis (12 items). We discovered that 85.1% (n = 80) of nurses had good levels of general practices. In all items, almost all nurses could regularly assess body temperature, abnormal bleeding (eg, vomiting blood, defecating blood), rapid, mild, unresponsive wrist pulses and depressive symptoms.
The fourth aspect was the practice guideline for using intravenous fluids to manage initial shock (four items). We discovered that 50% (n = 47) of nurses could resolve shock with treatments, such as intravascular infusion of 5% dextrose/normal saline solution at a drip rate suitable for adults and children in shock before referral to a tertiary hospital.
The fifth aspect was the practice guideline for referral to a tertiary hospital (13 items). We found that 51.1% (n = 48) of nurses were classified as achieving good practice in this regard. They could make hospital referrals when they recognized signs of shock (eg, not drinking, excessive thirst, little/no urination for 4–6 h, restlessness, abnormal bleeding, cold feet and sweating, fever and no improvement in symptoms), and they could refer patients suffering from shock to a tertiary hospital.
The final aspect was the practice guideline for dengue prevention (six items). We discovered that 77.7% (n = 73) of nurses could offer great advice. Most of the nurses could provide advice regarding prevention of mosquito bites; encouraged the destruction of Aedes species breeding sites every week in communities; communicated information to the PCU to undertake fogging in the patient’s home and over a radius of 100 m; monitored the Breteau Index, House Index and Container Index to assess the risk of dengue outbreak in communities (Table 5, Supplementary 1).
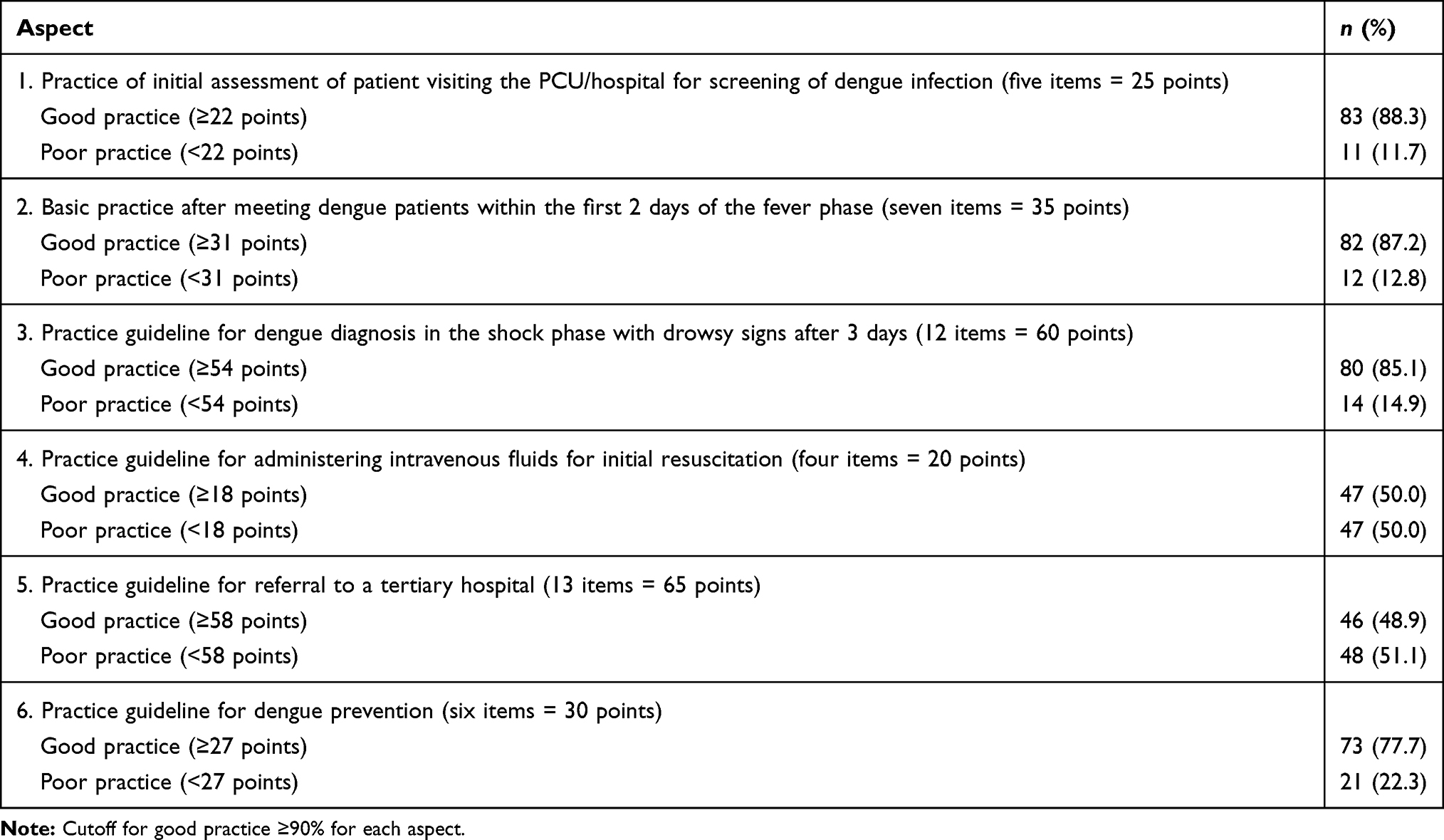 |
Table 5 Number and Percentage for Nurse Practices Regarding Dengue-Patient Care |
Correlation Among Personal Factors, Experience, Knowledge, Attitudes and Practices with Regard to DPC
Sex, age, employment grade, total work experience and current work experience in the PCU were significantly correlated with the ability to provide intravenous fluids to patients in the critical phase of dengue (p < 0.05 for all).
There was no significant correlation between the overall level of knowledge, attitudes or six aspects of practice regarding DPC (p > 0.05 for all). Almost all factors were not correlated significantly with the knowledge, attitude or practice components regarding DPC (p > 0.05 for all). Current work experience in the PCU was correlated significantly with attitudes regarding DPC (p < 0.05).
Experiences (ie, experience in caring for dengue patients with fever, in shock, in the recovery phase, requirement for administration of intravenous fluids and referral to a tertiary hospital) were correlated significantly with DPC (p < 0.05 for all). The employment grade, total work experience, experience in caring for patients in shock and ability to administer intravenous fluids were correlated with death of dengue patients (p < 0.05 for all).
Preparation of equipment and use of medical supplies for DPC showed a significant correlation with age, employment grade between ward nurses and senior nurses and ability to carry out the tourniquet test (p < 0.05 for all). Whereas practice regarding DPC aspect number 1, 2 and 5 were statistically significantly correlated with preparation of equipment factor (p < 0.01, p < 0.01 and p < 0.05), respectively.
Nurses’ experience with DPC within the previous 5 years, experience in undertaking the tourniquet test and in administering intravenous fluids to patients in the critical phase were correlated significantly with the practice guideline for dengue prevention (p < 0.05 for all) (Figure 1 and Supplementary 1).
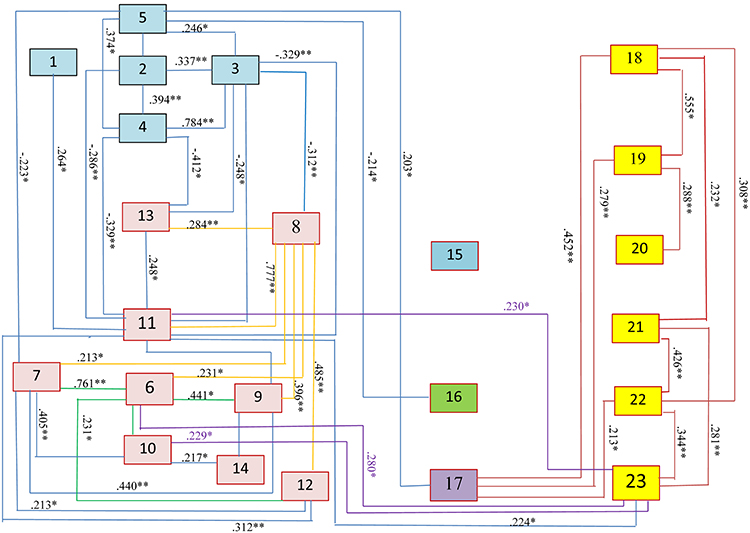 |
Figure 1 Correlation among personal factors (numbers 1–5), experience (numbers 6–14), knowledge (number 15), attitude (number 16), equipment (number 17) and practice regarding dengue patient care (numbers 18–24) Spearman’s test statistics: - Not statistically significant; *p < 0.05; **p < 0.01. Remarks, 1 Sex. 2 Age group (Cutoff point 45 years). 3 Position level (Practical/expert level). 4 Working experience up to the present (Cutoff point 10 years). 5 Working experience in the current duty at PCU (Cutoff point 10 years). 6 Have experience in treating dengue patients in previous 5 years (Yes/no). 7 Have experience in treating dengue patients in fever phase (Yes/no). 8 Have experience in caring for dengue patients in the shock phase (Yes/no). 9 Have experience in caring for dengue patients in the recovery phase (Yes/no). 10 Have experience in doing tourniquet test (Yes/no). 11 Experience giving intravascular fluid to patients in the critical phase (Yes/no). 12 Experience in referring dengue patients to hospital. 13 Experience related to dengue patient death (Yes/no). 14 Experience in prevention of dengue diseases in community (Yes/no). 15 Knowledge regarding DPC (Cutoff point for good knowledge level at ≥80%). 16 Attitude regarding DPC (Cutoff point for positive attitude level at ≥80%). 17 Preparation of equipment (Cutoff point for preparation level at ≥80%). 18 Practice regarding DPCA1: Practice to initial assessment of patient visiting the PCU/hospital for screening dengue infection (Cutoff point for good practice level at ≥90%). 19 Practice regarding DPCA2: Basic practice after meeting dengue patients within the first 2 days of the fever phase (Cutoff point for good practice level at ≥90%). 20 Practice regarding DPCA3: Practice guideline for dengue diagnosis with dengue shock phase with drowsy sign after 3 days (Cutoff point for good practice level at ≥90%). 21 Practice regarding DPCA4: Practice guideline for taking intravascular fluid for initial resuscitated shock (Cutoff point for good practice level at ≥90%). 22 Practice regarding DPCA5: Practice guideline for referral to province hospital (Cutoff point for good practice level at ≥90%). 23 Practice regarding DPCA6: Practice guideline for dengue prevention (Cutoff point for good practice level at ≥90%). |
Qualitative Study
Twenty-three nurses from 23 PCUs in 23 districts in NSTP participated in group discussions. They were 22 females and one male. The mean age was 44 ± 6.1 years. Twenty-two nurses had a senior rank, with total work experience of 21.1 ± 6.1 years, and current work experience in the PCU of 8.4 ± 6.2 years. Also, 65.2% (n = 15) had experience in DPC in the previous 5 years. DPC was analyzed according to four themes, as discussed below.
The first theme was “Several problems and obstacles in dengue management in the PCU”. This theme suggests that people in the community in NSTP mostly lacked awareness, lacked participation, had delayed information about dengue and did not have a budget supported by the local government. In forested communities, there were no cases of dengue tracking. Quotes from nurses included: “people in the community lack management of households and areas around the house” (Nurse #22); “ … people are not aware of dengue severity … ” (Nurse #5); “a delayed diagnosis means that it takes a long time to send a dengue patient from a sub district hospital to a district hospital” (Nurse #14).
The second theme was “Unpreparedness of equipment and medical supplies, and ambulances for hospital referral”. This theme suggested that the district and sub district governments lacked budgetary support for standard equipment for the prevention and control of dengue, and lacked medical supplies for the assessment, screening and initial treatment of dengue. The quotes from participants included: “lack of provision of children’s cuffs for a sphygmomanometer” (Nurse #5)”; “lack of sharing the medical equipment and supplies from provincial hospitals, and district hospitals to the PCU” (Nurse #5). Moreover, there was a lack of policy for initial treatment, such as “intravenous infusion in the physician’s presence” (Nurse #13) and “ … the PCU had no ambulances, sometimes the PCU must use the nurse’s car for referring a dengue patient if there is a severe case” (Nurse #15).
The third theme was “Delayed diagnosis and treatment because the PCU focuses only on the referral, not treatment”. This theme suggested that PCU nurses focused only on referring patients who had the signs and symptoms of dengue. Only the attending physician can make the dengue diagnosis, but PCUs contain only nurses. Nurses reported the limitations of their role: they could not make diagnoses but could refer patients. They stated: “The dengue diagnosis is the role of physicians, nurses only provide health assessments and referrals” (Nurse #1); “If I suspect a dengue case, it will be followed up” (Nurse #23); “ … if the patient’s symptoms indicate dengue, he/she will be referred as soon as possible” (Nurse #23); “ … the dengue diagnosis is the role of the physician … ” (Nurse #23).
The final theme was “Practice of dengue patient care will be better if all stakeholders are involved”. This theme suggested that to decrease the morbidity and mortality rates of dengue, the community must take action. Such action includes: making people in the community aware of dengue; organizing training programs for dengue prevention/control for all stakeholders; providing household management; revising clinical-practice guidelines for dengue and applying them to all PCUs in the province; developing a policy and budget for equipment and medical supplies. Quotes from participants included: “ … have the obvious guidelines, explanation and application cover all PCUs in the province” (Nurse #18); “PCUs, district hospitals, provincial hospitals and public-health officials in the province must support all equipment and medical supplies” (Nurse #3).
Discussion
First, we wished to assess the factors and practices of DPC. The risk factors were personal factors, experience, knowledge, attitudes, preparation of equipment and use of medical supplies, and practices with regard to DPC. We found that 77.7% (n = 73) of nurses had a poor knowledge level, and only 22% (n = 21) had a good knowledge level. Three of the 14 items (numbers 2, 4 and 7) were negative questions and had a low percentage of correct responses: 31.9%, 35.1% and 53.2%, respectively. The reason might be that nurses may not know the reporting procedures or may not have experience in reporting, such as classifying dengue into DF, DHF or DSS.3 This result is in accordance with that of a study of the knowledge, attitudes and practice towards DF of 348 healthcare professionals that demonstrated a low-to-moderate level.15 Moreover, the theme “Practice of dengue patient care will be better if all stakeholders are involved” and the quotes from nurses showed the unpreparedness of the PCU regarding preparation of equipment and use of medical supplies: “Unpreparedness of intravascular infusion sets in the PCU” (Nurse #6); “Lack of sharing of medical equipment and supplies from provincial hospitals, and district hospitals to PCUs” (Nurse #13); “ … lack of policy on initial treatment, such as intravascular infusion in the physician’s presence” (Nurse #13). These results are consistent with a study on 196 healthcare staff.23 The percentage of correct answers from healthcare staff regarding their knowledge, attitudes and practice was <50%, and the authors suggested that a training program for the prevention of dengue was necessary for healthcare staff.24 In another study, supporting data from patients (96–98%) revealed that the primary care practitioners had not given information on dengue prevention/control to them.7 In the present study, the highest percentage of correct answers (96.8% of nurses) corresponded to knowledge that the four serotypes of the DENV can lead a patient to acquire DF more than once. Also, 95.7% of nurses knew that A. aegypti is a dengue-transmission vector that lives in small houses and has black and white stripes, and that a patient can be infected by the DENV several times. Moreover, 94.4% of nurses knew that the signs and symptoms of DHF include plasma leakage and a decrease in the platelet count. These findings are consistent with those in a study on the knowledge, attitudes and practices regarding dengue infection among public-sector healthcare providers in Machala (Ecuador). That study showed that participants had a high level of knowledge on symptoms and treatment of dengue.25 However, our results are not consistent with observations in a study that found that healthcare professionals lacked clinical knowledge of dengue.26
Almost all nurses had a negative attitude towards DPC. This finding is related to the nurses’ opinion that the nurse in the PCU focuses only on referring patients who have the signs and symptoms of dengue. The dengue diagnosis can be made only by physicians, but PCUs contain only nurses. It showed an attitude that misunderstanding of the guidelines on the reporting of dengue cases within 24 hours which nursing care were covering the role of report case as the guideline disease control.4,9
The practice of DPC was divided into six aspects. More than 90% of nurses achieved good practice in these four aspects. This finding is consistent with that in a research study showing that 96.3% of doctors, physicians and nurses have a high level of basic practice of dengue patient care.27 According to one aspect (the practice guideline for administering intravenous fluids for initial resuscitation of patients in the critical phase), the low score was corrected to 44.7% because of the disorders related to dengue. The critical phase is where plasma leakage outside blood vessels occurs in individuals with DHF. Screening tests must begin to rapidly identify individuals who are sick and who are at risk. The practice of initial assessment, primary care and administration of intravenous fluids includes monitoring and assessment of shock, and care to prevent shock by providing intravascular infusions and blood transfusions. After the passing of the shock period, the patient enters the recovery phase, in which the nurse in the district hospital carefully takes intravascular fluids for the initially resuscitated patient in the critical phase.1,2 Our results were inconsistent with those in a study on the knowledge, attitudes and practices for dengue among healthcare professionals in southern Taiwan.26 That study showed that healthcare professionals lacked education in the important clinical features of dengue. Moreover, a limitation of practice in PCUs corresponded to a particular theme: “Delayed diagnosis and treatment is because PCUs focus only on referral, not treatment”. This theme indicates that nurses in PCUs focus only on referring patients who have the signs and symptoms of dengue disease. As stated above, this is because PCU nurses cannot diagnose dengue: only physicians can.
We analyzed the correlation among factors and practices of DPC. We found that almost all personal factors were not significantly correlated with DPC. This finding is not consistent with observations in a study on the knowledge, attitudes and practices towards DF prevention and associated factors among 348 public healthcare professionals.15 That study concluded that the sex, age, type of profession and experience of a healthcare professional were associated with the knowledge level of that healthcare professional.15 We found that current experience in the PCU was correlated significantly with practices involving the guidelines for administering intravenous fluids for initially resuscitated patients in the critical phase, and that experience in DPC within the previous 5 years was associated significantly with practices involving the guidelines for dengue prevention/control in the community. Both of these factors are important for nurses’ roles in dengue management in PCUs and for their career development.9,10 These findings are consistent with those from a study that reported that primary care practitioners do not give advice on disease prevention,7 and that public-health professionals rather than nurse practitioners participated in surveillance systems for dengue prevention/control in the community.28 One study reported that knowledge about DF and its complications among 100 nursing practitioners in a hospital did not have an association with the demographic variables of nurses.29
Two factors had a significant relationship with attitudes regarding DPC, namely the experience in: (i) caring for dengue patients in the critical phase; (ii) referring dengue patients. This finding shows that nurses’ attitudes are dependent upon their experience with dengue patients. This result is in accordance with that in the study on the knowledge, attitudes and practices among communities which found that people who live in outbreak areas showed better knowledge, attitudes and practices compared with those who did not.30 It is also believed that nurses who have experience will have more positive attitudes. This concept was indicated by a quasi-experimental study that assessed the effect of educational sessions about DF on the knowledge and attitudes of 71 nurses in El Zagazig Fever Hospital in Egypt. That study showed an increasingly positive attitude after participation in an education-and-implementation program.14
The correlation among the knowledge, attitudes and practices of DPC was not significant. Our result is not in accordance with that in a study on the knowledge of nurses regarding DF in a tertiary care teaching hospital in Nepal. That study demonstrated low levels of knowledge on DF and its complications among nursing practitioners, and did not reveal an association between their knowledge and demographic variables.29 Moreover, the results of a study involving 247 nurses and 348 healthcare professionals in Ethiopia showed that their knowledge, attitudes and practices regarding DF were not satisfactory.15 Another study between January and September 2019 demonstrated no relationship between knowledge, attitudes or practices because there was a high incidence of dengue: the morbidity incidence was 188.24 cases/100,000 people, and the mortality incidence was 0.27 cases/100,000 people.6 The reasons for such results might be a lack of training on DPC, which focuses on knowledge of treatments, so nurses in PCUs provided imperfect advice on dengue. Those results were consistent with data in a study that found that knowledge of DF had no significant relationship with practices.29,31 However, those results were inconsistent with data from a study on the knowledge, attitudes and practices regarding DF prevention in nursing students at a tertiary hospital which showed that the relationship between knowledge about DF spread and practices in dengue prevention was significant.27 Moreover, the results from our study were not consistent with the data from a systematic review of 17 studies conducted in Malaysia which showed that a high level of knowledge led to a good attitude and high level of preventive practices of dengue.32
In the present study, the four themes of qualitative data supported the quantitative data of knowledge, attitudes and practices of DPC. In particular, preparation of equipment and use of medical supplies in the PCU did not reach the cutoff point of ≥80%, which is important for the assessment and diagnosis of dengue.1,5 The tourniquet test is important for DPC in PCUs in Thailand.33 If a PCU lacks equipment and medical supplies, the healthcare provider will not be able to provide optimal DPC. Training is especially important for medical and non-medical personnel involved in the clinical management of dengue at the primary, secondary and tertiary levels of care.34 Moreover, community participation is needed to improve DPC by developing and using the appropriate guidelines.16
Our study had two main limitations. First, the study cohort (94 nurses) was small. Second, almost all participants were women. For these reasons, our results may not be representative of other PCUs in other provinces in Thailand.
Conclusions
Nurses in PCUs have important roles in providing DPC in Thailand. There was a few good knowledge and positive attitudes among participants, but >90% of all nurses had good practices regarding DPC. There was no significant relationship among knowledge, attitudes or practices regarding DPC. The nurses’ experience in caring for dengue patients in the critical phase and experience in referring dengue patients were related significantly to the attitudes regarding DPC. Current experience in the PCU was associated significantly with the dengue practice of administering intravenous fluids for initially resuscitated patients in the critical phase. Nurses’ experience of DPC in the previous 5 years was related to practices for dengue prevention/control in the community. Our study demonstrated the need for PCUs to provide equipment, medical supplies and guidelines for clinical management of dengue to support care of patients with dengue in PCUs. Moreover, dengue practice workshop programs are needed for PCU nurses as a bridge between knowledge, attitude and practice.
Abbreviations
BP, Blood pressure; BT, Body temperature; BI, Breteau Index; CI, Container Index; DENV, Dengue virus; DF, Dengue fever; DHF, Dengue hemorrhagic fever; DPC, Dengue patient care; DSS, Dengue shock syndrome; NSTP, Nakhon Si Thammarat province (NSTP); PCU, Primary care unit.
Data Sharing Statement
Additional data are not available.
Ethical Approval and Consent to Participate
Ethical approval and consent to participate were approved by the research board and research ethics committee of Walailak University (WUEC-18-065-01) on 12 December 2018. All participants provided written informed consent. Study data were stored safely, personal data were coded and the identities of participants remained confidential.
Consent to Publish
Not applicable.
Acknowledgments
We gratefully acknowledge all the nurses in all PCUs in Nakhon Si Thammarat Province. We thank the Excellent Center for Dengue and Community Public Health (EC for DACH), the Institute of Research and Development, School of Public Health and Walailak University. We also thank Supreecha Kaewsawat, Chuthamat Nopparat, Papassara Changklang, Paleeratana Wongrith, Jiraporn Jaroenpool and Nirachon Chutipattana for participating in collecting the data. We proffer special thanks to Charlesworth Author Services (Paper #: 72815) who edited the manuscript.
Author Contributions
Charuai Suwanbamrung participated in the five main criteria of authorship; Cua Ngoc Le, Phatcharaphon Phetphrom, Penpanee Kamneatdee, Nattavadee Kaewket and Orratai Nontapet participated in the following five criteria: 1) Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, 2) Have drafted or written, or substantially revised or critically reviewed the article, 3) Have agreed on the journal to which the article will be submitted, 4) Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and 5) Agree to take responsibility and be accountable for the contents of the article.
Funding
This work was supported financially by the Excellent Center for Dengue and Community Public Health (EC for DACH) and Walailak University (WU-COE-63-004).
Disclosure
The authors report no conflicts of interest for this work.
References
1. WHO. Dengue Hemorrhagic Fever: Diagnosis, Treatment, Prevention and Control. Geneva: WHO; 1997.
2. WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. Geneva, Swilzerland: WHO Library Cataloguing-in-Publication data; 2009.
3. WHO. Handbook for Clinical Management of Dengue. Genewa, Switzerland: WHO Library Catagologulng-in-Publication Data; 2012.
4. Vector Borne Diseases Division Diseases Control Department Thai Ministry of Public Health. Dengue situation. In: Vector Borne Diseases Division, Diseases Control Department. Thai Ministry of Public Health; 2019.
5. Hadinegoro S. The revised WHO dengue case classification: does the system need to be modified? Paediatr Int Child Health. 2012;32(Suppl 1):33–38. doi:10.1179/2046904712Z.00000000052
6. Public Health Official Nakhon Si Thammarat Province. Epidemiology surveillance report. Public Health Official Nakhon Si Thammarat Province Nakhon Si Thammarat Province 2018.
7. Ang KT, Rohani I, Look CH. Role of primary care provider in dengue prevention and control in the community. Med J Malasia. 2010;65:1.
8. Lum L, Ng CJ, Khoo EM. Managing dengue fever in primary care: A practical approach. Malays Fam Physician. 2014;9(2):2–10.
9. Boontong T, Athaseri S, Sirikul N. Nurse practitioners role towards primary medical care in primary health care setting. Thai J Nursing Council. 2007;22(4):24–37.
10. Siripukdeekan C. Nursing career ladder development. J Royal Thai Army Nurses. 2014;15(3):74–80.
11. Rav-Marathe K, Wan TTH, Marathe S. A systematic review on the kap-o framework for diabetes education and research. Medical Research Archives. 2016;4(1):1–21.
12. Wan TTH, Transdisciplinary A. Approach to health policy research and evaluation. Int J Public Pol. 2014;10(4–5):161–177. doi:10.1504/IJPP.2014.063094
13. Wan TTH, Terry A, McKee B, Kattan W. KMAP-O framework for care management research of patients with type 2 diabetes. World J Diabetes. 2017;8(4):165–171. doi:10.4239/wjd.v8.i4.165
14. Abd El-Ghany G, Mahmoud S. Effect of educational sessions about dengue fever on nurse’s knowledge and attitude at Zagazig Fever Hospital. Egyptian Nursing J. 2018;15(3):281–291. doi:10.4103/ENJ.ENJ_18_18
15. Mohammed Yusuf A, Abdurashid Ibrahim N. Knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals: in Dire Dawa, eastern Ethiopia. Risk Manag Healthc Policy. 2019;12:91–104. doi:10.2147/RMHP.S195214
16. Suwanbamrung C, Le CN, Maneerattanasak S, et al. Developing and using a dengue patient care guideline for patients admitted from households to primary care units and the district hospital: A community participatory approach in Southern Thailand. One Health. 2020;10:100168. doi:10.1016/j.onehlt.2020.100168
17. Wisdom JP, Cavaleri MA, Onwuegbuzie AJ, Green CA. Methodological reporting in qualitative, quantitative, and mixed methods health services research articles. Health Serv Res. 2012;47(2):721–745. doi:10.1111/j.1475-6773.2011.01344.x
18. Kaur N, Vedel I, El Sherif R, Pluye P. Practical mixed methods strategies used to integrate qualitative and quantitative methods in community-based primary health care research. Fam Pract. 2019;36(5):666–671. doi:10.1093/fampra/cmz010
19. Tejativaddhana P, Briggs D, Singhadej O, Hinoguin R. Developing primary health care in Thailand innovation in the use of socio-economic determinants, sustainable development goals and the district health strategy. Public Administration Policy. 2018;21(1):36–42. doi:10.1108/PAP-06-2018-005
20. Smolowitz J, Speakman E, Wojnar D, et al. Role of the registered nurse in primary health care: meeting health care needs in the 21st century. Nurs Outlook. 2015;63(2):130–136. doi:10.1016/j.outlook.2014.08.004
21. Cohen J. Statistical Power Analysis for the Behavioral Sciences. USA: Lawrence Erlbaum Associates; 1988.
22. Harvey K, Horton L. Bloom’s human characteristics and school learning. Phi Delta Kappa Int. 1977;59:3.
23. Suwanbamrung C. Reflections of health leaders’ experiences related dengue solutions from transmitting a technology of larval indices surveillance system in Southern Thailand. Trends Med. 2019;19.
24. Ruberto I, Yaglom H, Erhart LM, et al. Dengue knowledge attitude and practice among Arizona health worker, 2014–2015. Vector-Borne Zoonotic Diseases. 2019;19:434–440. doi:10.1089/vbz.2018.2370
25. Handel AS, Ayala EB, Borbor-Cordova MJ, et al. Knowledge, attitudes, and practices regarding dengue infection among public sector healthcare providers in Machala, Ecuador. Tropical Diseases, Travel Medicine Vaccines. 2016;2(1):8. doi:10.1186/s40794-016-0024-y
26. Ho T-S, Huang M-C, Wang S-M. Hsian-ChouHsu, Ching-ChuanLiu. Knowledge, attitude, and practice of dengue disease among healthcare professionals in southern Taiwan. J Formosan Med Association. 2013;112:18–23. doi:10.1016/j.jfma.2012.11.004
27. Jain S, Mishra MK, Gupta SK, Agrawal SS, Shukla US. Knowledge, attitude and preventive practices about dengue fever among nursing student of tertiary care hospital. J Evolution Med Dental Sci. 2014;3(6):1481–1488. doi:10.14260/jemds/2014/2011
28. Suwanbamrung C, Thoutong C, Eksirinimit T, Tongjan S, Thongkew K. The use of the “Lansaka Model” as the larval indices surveillance system for a sustainable solution to the dengue problem in southern Thailand. PLoS One. 2018;13(8):e0201107–e0201107. doi:10.1371/journal.pone.0201107
29. Valarmathi S, Parajulee S. Knowledge of nurses towards dengue fever in a tertiary care teaching hospital in Nepal. J College Med Sciences-Nepal. 2013;9(1):7–13. doi:10.3126/jcmsn.v9i1.9667
30. Ghani NA, Shohaimi S, Hee AK-W, Chee H-Y, Emmanuel O, Alaba Ajibola LS. Comparison of knowledge, attitude, and practice among communities living in hotspot and non-hotspot areas of dengue in selangor, Malaysia. Trop Med Infect Dis. 2019;4(1):37. doi:10.3390/tropicalmed4010037
31. Shuaib F, Todd D, Campbell-Stennett D, Ehiri J, Jolly PE. Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med J. 2010;59(2):139–146.
32. Ajibola L-SA, Shohaimi S, Adam MB, Nadzir MNHM, Segun OE. Systematic review of knowledge, attitude, and practices regarding dengue in Malaysia. J Applied Pharmaceutical Science. 2018;8(12):080–091.
33. Kanlayanarooj SVM, Vatcharasaevee V. Clinical Practice Guidelines of Dengue/Dengue Hemorrhagic Fever Management for Asian Economic Community WHO Collaborating Centre for Case Management of Dengue/DHF/DSS. Nonthaburi. Thailand: Department of Medicine Services, Department of Diseases Control; 2014.
34. Pan American Health Organization. Integrated management strategy for dengue prevention and control in the region of the americas the communications department through the PAHO website; 2018. Available from: www.paho.org/permissions.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.