")
Back to Journals » International Journal of Women's Health » Volume 12
Factors Associated with Timely Antenatal Care Booking Among Pregnant Women in Remote Area of Bule Hora District, Southern Ethiopia
Authors Tufa G, Tsegaye R , Seyoum D
Received 22 March 2020
Accepted for publication 4 August 2020
Published 24 August 2020 Volume 2020:12 Pages 657—666
DOI https://doi.org/10.2147/IJWH.S255009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Girma Tufa,1 Reta Tsegaye,2 Dejene Seyoum3
1Department of Nursing, College of Health and Medical Sciences, Bule Hora University, Bule Hora, Ethiopia; 2Department of Nursing, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 3Department of Public Health, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia
Correspondence: Reta Tsegaye
Department of Nursing, Institute of Health Sciences, Wollega University, P.O.Box 395, Nekemte, Ethiopia
Tel +251-912272612
Email [email protected]
Background: Antenatal care (ANC) is one of the most cost-effective and crucial components of maternal health care services. In developing countries where access to care, empowerment, and decision making power of women is low, ANC service is vital. The time at which first ANC visit was done has the utmost importance to ensure optimal health effects for both women and children. This study aimed to assess the proportion and factors associated with early antenatal care booking among pregnant women who were attending public health institutions in a remote area of Bule Hora district, Southern Ethiopia, from May to July, 2019.
Methods: Institutional-based cross-sectional study design was conducted at Bule Hora district public health facilities. Data were collected on systematically selected 377 pregnant women from 1st May to 30th July 2019. The sample size was determined by single population proportion formula and data were collected by using a standardized and pretested questionnaire and entered into Epidata 3.1 version, and then exported to Statistical Package for Social Science (SPSS) version 25 for analysis. The strength of association was measured by odds ratios with 95% confidence interval (CI) at a p-value of < 0.05 and finally obtained results were presented by using simple frequency tables, bar graph, and texts.
Results: The proportion of early antenatal care booking among pregnant women attending antenatal care in the study area was 57.8%. Factors contributing to early antenatal care booking were husband’s education (Adjusted odds ratio (AOR), 2.5; 95% CI: 1.2, 4.9), knowledge on antenatal care service (AOR,1.99; 95% CI:1.2,3.3), means of approving current pregnancy (AOR,1.8; 95% CI:1.1,2.8), and being advised before starting antenatal care visit (AOR,2.1; 95% CI:1.2,3.6).
Conclusion: Generally, the timely initiation of ANC among pregnant mothers is not ideal. Modifiable factors like husband’s education, knowledge on antenatal care service, means of recognizing current pregnancy, and access to pre-ANC advice were found determinants for the timely initiation of ANC. Thus, it is advisable to provide proper information about antenatal care services by health care providers and enhancement of health extension program to increase community awareness before and during pregnancy at all levels of health care provision is very important.
Keywords: antenatal care, pregnant women, timely booking, Ethiopia
Background
Worldwide, more than half million maternal deaths and about 2.6 million stillbirths occur every year. Every day, 830 mothers die of which 99% happens in developing countries as a result of pregnancy-related complications. Majority of these deaths occur among pregnant women who did not receive ANC.1–5 Despite good progress in access and utilization of ANC visits globally, studies have shown that only 17% of women ever received any ANC and the proportion of women who are receiving the recommended focused ANC minimum of four visits still low.6–8
Timely antenatal care is the period in which pregnant women visited ANC at less than four months of pregnancy, while late antenatal care is the period in which women start attending ANC at greater than or equal to four months of pregnancy.9
According to Ethiopian Demographic and Health Survey (EDHS), 62% of pregnant women attended ANC at least once and only 32% of them attended four times. Among those who attended, only 20% of them had booked their first antenatal care visit in the first trimester of pregnancy. The rest attended during their fourth to the fifth month of pregnancy or later.10
The time at which first ANC visit was started has the utmost importance to insure optimal health effects for both women and children. According to the new World Health Organization (WHO) antenatal care model, it is advisable for pregnant women to visit first ANC visit within the first trimester of pregnancy. The first visit offers an opportunity to establish baseline information on the general wellbeing of the mother, accurate gestational age ascertainment, identifying multiple pregnancies, and fetal anomalies. It also helps the mothers to consider the services provided in the facility and build up their impression and trust in these facilities to seek health care.11 It is also an appropriate time to create awareness on signs and symptoms of pregnancy complications which may lead to timely access to appropriate emergency obstetric care.9
Early initiation of ANC during the first three months of gestation plays a key role in detecting and treating complications of pregnancy and forms a descent basis for appropriate management during delivery and postpartum. Late attendance of ANC results in the potential for complications during pregnancy, delivery, and puerperium. Hence, the first ANC visit should be as early as possible in pregnancy, preferably in the first trimester.9,12 Delay in booking of ANC results in the potential for complications during pregnancy, childbirth, and post-partum. Pregnant women who are late booked for antenatal care visit or those who missed these opportunities are at high risk of developing pregnancy danger signs such as convulsions, respiratory distress, vaginal bleeding, acute abdominal pain, severe headaches, blurred vision, vomiting, fever, leaking of liquor, and increased risk of fetal death.9,13
Generally, early ANC booking is recommended to prevent adverse outcomes of pregnancy which subsequently results in unmanaged complications among pregnant women. Due to this high burden and its grave consequences, maternal health is one of the top priorities in the national health agenda, which needs due attention. Ethiopia is implementing the primary health care model to improve access to basic maternal health services guided by global health initiatives and support from different international communities.14 However, utilization of maternal health services along the full cascade of maternity care (family planning, safe abortion, antenatal care, institutional delivery, and postnatal care) is low due to socio-economic, cultural, and structural barriers.1
Bule Hora district is one of the remotest areas in Ethiopia which is found near the Ethio-Kenya border where accesses to services like early antenatal care are generally low. To improve this, the investigation of factors contributing to late antenatal care booking is very important. Besides this, the finding of this study would add significant input to literature assessing factors affecting early initiation of ANC. Thus, this study was aimed to assess the proportion and associated factors of timely antenatal care booking in a remote area of Bule Hora district, Southern Ethiopia.
Materials and Methods
Study Area
The study was conducted in Bule Hora district, West Guji Zone, Oromia regional state, Southern Ethiopia. The district is one of the remotest areas located at a distance of 467 Km away from the country’s capital, Addis Ababa. According to the 2018 report of zonal statistics office, the district has a total population of 263, 780 among which 49% (130 703) males, 51% (133 077) females. Bule Hora district has one general hospital and 6 health centers with 183 and 286 health care workers respectively.
Study Design and Period
Institution-based cross-sectional study design was employed to assess the proportion of early antenatal care booking and associated factors among pregnant women. The study was conducted from May to July 2019.
Population
The source population was all pregnant women who were attending ANC clinic in public health institutions of Bule Hora district while the study populations were randomly selected pregnant women who were following ANC service at public health institutions of Bule Hora district during the data collection period and fulfills inclusion criteria.
Inclusion and Exclusion Criteria
Pregnant women who were attending antenatal care clinics for ANC services were included whereas pregnant women who came after attending ANC service at another health facility were excluded. These women were excluded because; their gestational age at their first visit might not be known.
Sample Size Determination
The sample size was calculated for each specific objective and the optimal sample size was selected. For the proportion of early ANC booking, the sample size was determined using a single population proportion formula n= (Zα/2)2 p (1-p)/d2 with the following assumptions: the proportion of early ANC booking was taken from the previous study done in Dilla town which was 35.4%.15 The significant level at α= 0.05, with 95% CI, a maximum acceptable marginal error of 5%, and a non-response rate of 10% was used to obtain a final sample size of 386.
Sampling Procedures and Technique
All public health facilities found in Bule Hora districts that were providing ANC services during the study period namely, Bule Hora general hospital, Bule Hora Health Center, Kilenso Mokonisa Health Center, and Garba Health Center were included based on their client flow. The total sample size was proportionally allocated to these health facilities based on the previous average two-month flow of pregnant women for ANC in each health facility. The study respondents were recruited by using a systematic random sampling technique of every 2nd client after identification of the first study subject by lottery method.
Study Variables
Dependent Variable
Early ANC booking.
Independent Variables
Maternal age, educational status, Ethnicity, religion, monthly income, marital status, residence, husband education, husband occupation.
Parity, number of alive children, planned pregnancy/wanted pregnancy, medical complication in a previous pregnancy, previous birth outcome, previous use of ANC service, women decision on ANC, husband involvement on ANC, pregnancy approval by a spouse.
Perceived starting time, number of ANC visits, source of information.
Distance, cost of service, waiting time.
Operational Definitions
Timely ANC Booking
Booking for first ANC before 16 weeks of gestational age after pregnancy is confirmed either by missed period or urine test for the current pregnancy.16
Knowledge on Early ANC
Each knowledge question answered correctly was scored one mark while the question answered incorrectly was scored zero marks. The total score ranging from 0–7 obtained by each respondent was added up and was computed to categorize knowledge into:
Good Knowledge
Those pregnant women who answered knowledge-related questions of above 60%.17
Poor Knowledge
Those pregnant women who answered knowledge-related questions of below 60%.17
Data Collection Tools and Procedures
Data were collected using standardized and pretested questionnaires by interviewing pregnant mothers. The tool was adapted from Safe motherhood and modified from different literatures.15,18 The questionnaire had six parts which consist of socio-demographic characteristics, knowledge of ANC, current pregnancy and experience of health services utilization, obstetric history of the mother, health service-related, and women decision making and husband involvement.
The data collection tool was first prepared in English and then translated to regional working language, Afaan Oromo, by language experts. The tool was retranslated back into English by other language experts to check for consistency. The edited final version of Afaan Oromo questionnaire was used for data collection. Four degree holder professional nurses were recruited based on their experience of data collection and communication skills with pregnant mothers and two lecturers were assigned for supervision from Bule Hora University based on their language skills and experience.
Pregnant women were interviewed on exit after they completed their daily visits. Client card was also reviewed to extract important variables, like the gestational age of the mother for those women who were not sure of their gestational age.
Data Quality Controls
To control the quality of data, the questionnaire was pre-tested on 5% of the study population at Finchawa health center which was different from the selected health institutions. Data collectors along with the supervisors were trained for two days on the purpose of the study, study tools, data collection procedures, and data handling. Supervisors carried out their regular supervision, spot-checking, and reviewing the completed questionnaire daily to maintain data quality. The overall activity was coordinated by the principal investigator.
Data Processing and Analysis
Data were entered into Epidata 3.1 version and exported to SPSS version 25 statistical software for analysis. Cross tabulation was done among dependent and independent variables for data exploration and to compute descriptive summary statistics. The descriptive statistics result of numerical variables expressed by mean with standard deviation while categorical variables were presented using frequency with percentage, and displayed by tables, bar graph, line graph, and pie chart, whereas the normality of continuous variables was checked by histogram and Shapiro-Wilk test.
Bivariable logistic regression analysis was used to assess the association between the dependent and all the independent variables and to identify candidate variables for multivariable analysis with p-value <0.25 in order to control potential confounders and to predict the association of explanatory variables and outcome.19 The multivariable logistic regression model was applied by the backward elimination stepwise method. The crude and Adjusted OR results together with their corresponding 95% CI with computed a p-value less than 0.05 were considered to declare predictive candidate variables.
The Hosmer and Lemeshow model goodness of fit test was checked for the fitness of the variables fulfilled at p-value >0.05 and the value was 0.908.19 The variance inflation factors (VIF) was used to test multicollinearity among predictor variables.
Ethical Considerations
Ethical clearance was obtained from the Institutional Ethical approval Committee of Wollega University. A formal letter from the Institute of health sciences of Wollega University was written to the Bule Hora district, and then the permission and support letter was written to each health facility. Written consent was obtained from each study participants after explaining the purpose of the data collection and before the interview. Respondents’ names were not written on the questionnaire for anonymity and confidentiality of their information. Assent was obtained from participants under the age of 18 years, and was approved by Institutional Ethical approval Committee of Wollega University to provide informed consent on their own behalf. They were also informed that they were free to withdraw from the interview and study at any time. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
Out of a total of 386 eligible pregnant women, 377 respondents participated in this study with a 97.6% response rate. More than half of 206 (54.6%) of the respondents were in the age group of 25–34 years. Almost all respondents, 359 (95.2%) were married. One hundred sixty-one (42.7%) of the respondents were housewives and 160 (42.4%) attended primary school (1–8); and 213 (56.5%) were urban residents. Nearly half (181 (48%)) of the participants were protestants by religion. Two hundred forty-one (63.9%) of them were Oromo in ethnicity, and 105 (27.9%) of them had a monthly family income of less than 500 Ethiopian Birr (Table 1)
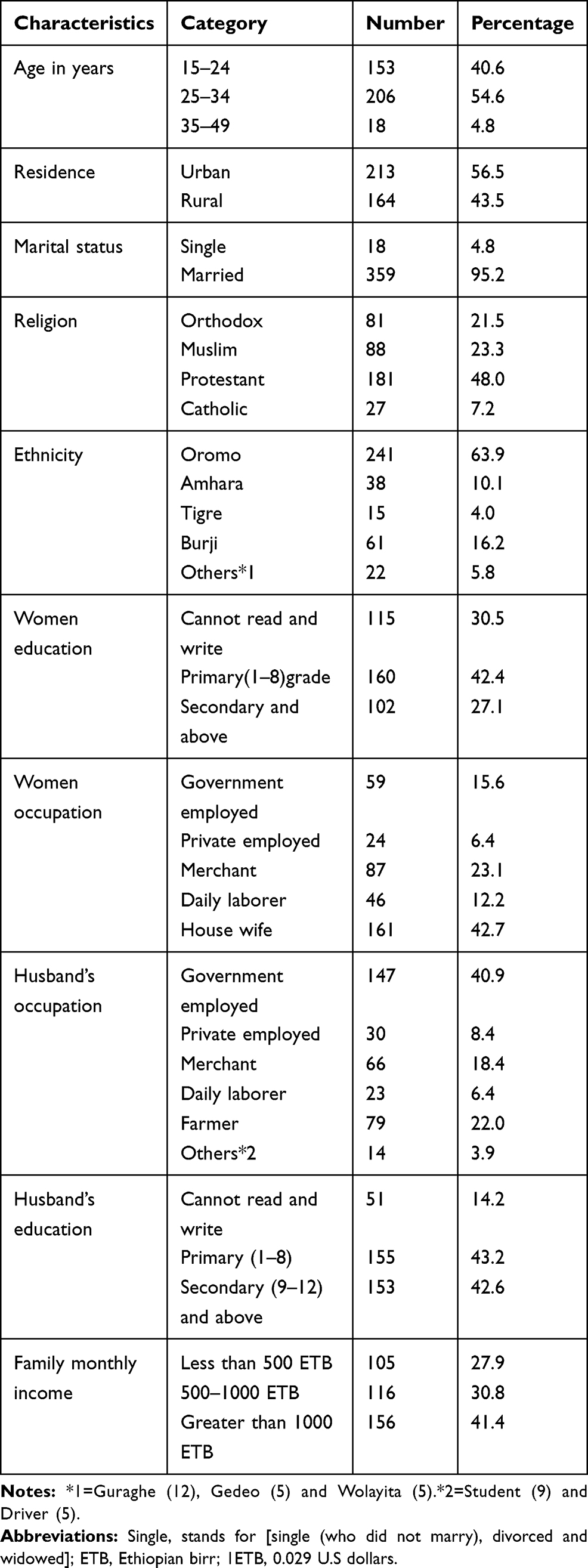 |
Table 1 Socio-Demographic Characteristics of Pregnant Women, Bule Hora District 2019 |
Knowledge of ANC Service
Three hundred forty-seven (92.0%) pregnant women knew the importance of ANC service while 229 (66.0%) of them reported that the appropriate time to begin ANC service after missed period was before four months. Nearly 95% of pregnant women knew that early ANC booking improves pregnancy outcome while 290 (76.9%) of women perceived that four and more ANC visits are necessary. Among the respondents, only 146 (38.7%) had information that all pregnant women are at risk of pregnancy complications while 166 (44%) of all respondents reported that there is a difference in time of booking early ANC between primiparous and multiparous. Of the total respondents, 279 (74%) of them had good knowledge of early ANC service, while 98 (26%) of them had poor knowledge of the service (Table 2)
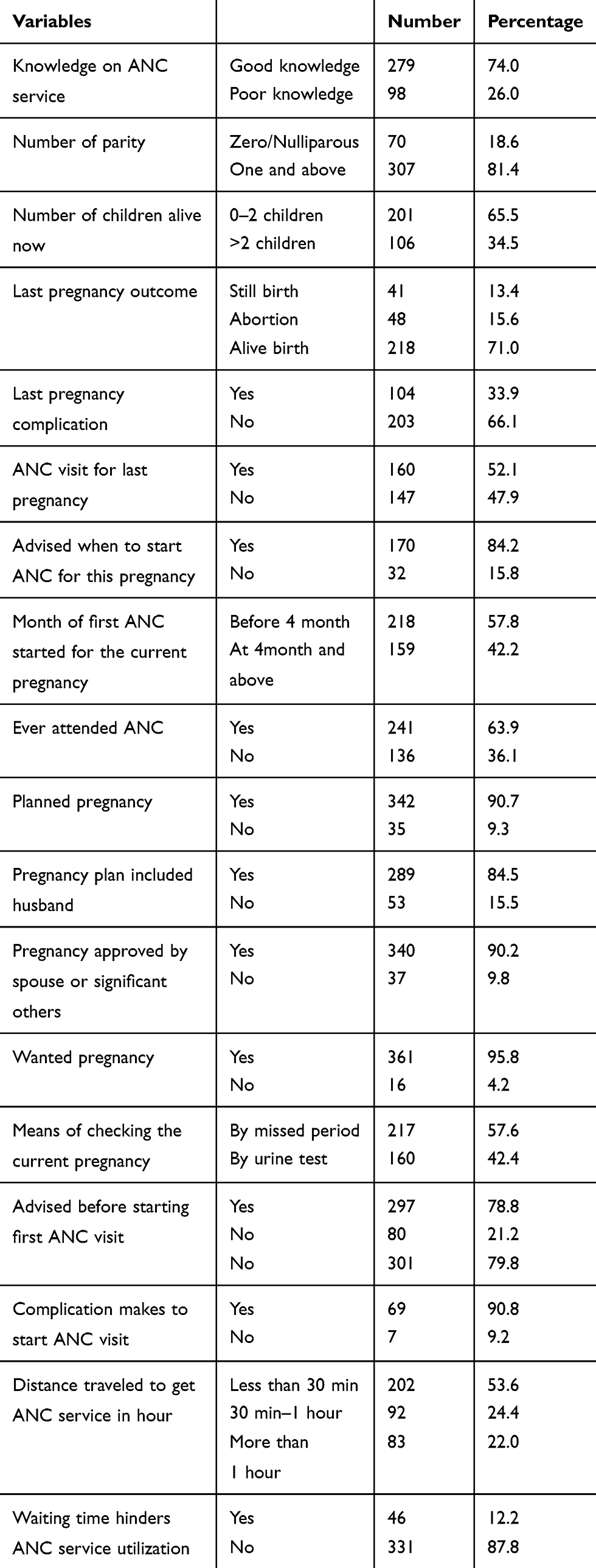 |
Table 2 Knowledge, Obstetric History, Husband Involvement and Experience of Service Utilization of Respondents, Bule Hora District, 2019 |
Obstetric History, Husband Involvement, and Decision Power
The majority (81.4%) of the respondents had parity of one and above, while 18.6% were nulliparous. Nearly two-thirds (65.5%) of respondents had 1–2 number of alive children, while 106 (34.5%) of them had more than two number of alive children. Two hundred eighteen (71.0%) of respondents had alive birth, while about 41 (13.4%) and 48 (15.6%) had stillbirth and abortion, respectively. One hundred four (33.9%) of pregnant women reported that they had a complication in their last pregnancy. Among respondents who had a pregnancy before, more than half (52.1%) of them had a history of ANC visit in their last pregnancy whereas the rest (47.9%) did not receive ANC at all. One hundred seventy (84.2%) of those who had ANC visit got counseling about the time of initiation for current pregnancy (Table 2)
Among respondents who attended ANC for the current pregnancy, 342 (90.7%) of them had planned pregnancy, and 217 (57.6%) and 160 (42.4%) of respondents confirmed their pregnancy by missed period and urine test, respectively. The primary source information for the respondents was their husbands (42.8%) followed by friends (20.5%) and media (12.8%). The distance from the health facility was collected from the respondents. Accordingly, 92 (24.4%) of them traveled 30 minutes to one hour while 83 (22%) of the respondents traveled more than one hour to reach the ANC services. The median time travel to reach the ANC service was 30 min (Table 2)
Information on early ANC booking was also collected from the respondents. Accordingly from the total respondents, 218 (57.8%) of them booked ANC early, while 159 (42.2%) booked lately. Booking of early ANC ranged from the third month to ninth months of pregnancy. The mean gestational age the respondents booked was 22 weeks (5.5 months) with SD±6.5weeks (1.63 months) (Figure 1)
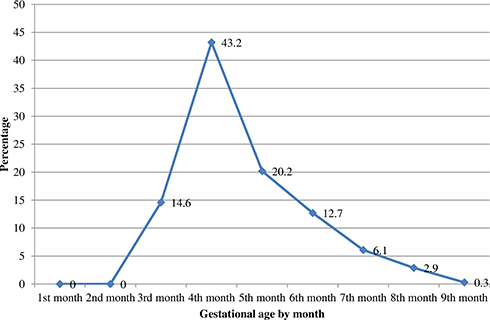 |
Figure 1 The percentage of respondents booked first ANC from 3rd to 9th month of pregnancy, Bule Hora district, 2019. Showing the percentage of pregnant women initiated first ANC. Large proportion of them had initiated during their fourth month of pregnancy. |
Factors Associated with Early ANC Booking
In the multivariable analysis of this study; husband education, knowledge on ANC service, means of approving (checking) current pregnancy, and getting advice before starting ANC visit was statistically significant variables for early antenatal care booking at the p-value <0.05.
Women who had educated husbands of secondary and above were 2.5 times more likely to book ANC early as compared to the counterparts (AOR, 2.5; 95% CI: 1.2, 4.9). Those pregnant women who had good knowledge of antenatal care service were 1.99 times more likely to book early ANC as compared to poor knowledge (AOR, 1.99; 95% CI:1.2, 3.3). Those respondents who had checked their current pregnancy by urine test were 1.8 times more likely to book early ANC compared to those who checked by missed menstrual period (AOR, 1.8; 95% CI: 1.1, 2.9). Respondents who were counseled before starting early ANC were twice more likely to book early ANC than who did not get the counseling (AOR, 2.1; 95% CI: 1.2, 3.7) (Table 3)
 |
Table 3 Factors Associated with ANC Booking Among Pregnant Women Attending ANC, Bule Hora District, 2019 |
Discussion
In this study, the proportion of early antenatal care booking among pregnant mothers was 57.8%. Despite good knowledge about the importance of ANC visits, the early initiation of ANC is comparably low. This finding was higher when compared to the results of other studies like developing region (48.1%), EDHS 2016 report (20%), Bahir Dar Zuria (46.7%), and Gondar (47.2%).2,10,11,20 The reason for the high proportion in this study could be the commitment of health extension workers who are engaged in tracing and further advising of pregnant mothers for early ANC booking, the effort of the health facilities and government on the improving women’s access to maternal and child health services, and improvement in women health care seeking might have played a major role.21 Though the figure looks better compared to other studies, late initiation of ANC service might have resulted in them developing complications as nearly one-third of pregnant women had reported that they had a complication in their last pregnancy. The mean gestational age at which the pregnant women booked their early ANC was 22 weeks despite more than half of respondents booked it early. This study finding is almost similar to studies done in Nigeria and Dilla Town, Southern region, Ethiopia.15,22 Despite having good knowledge of the importance of ANC service, many pregnant women had no behavior of seeking timely ANC initiation and only attend antenatal care when they are feeling sick.10
In this study, pregnant women whose husbands’ had the educational status of secondary and above were more likely to book early as compared to their counterparts. This finding is congruent with other studies conducted in Ethiopia.23–25 It could be because: those husbands who had no or less information on early antenatal care booking may discourage their wives from discussing their pregnancies regarding the health-seeking behavior for ANC visit and this may lead to delay pregnant women to visit of ANC early.
Having good knowledge about antenatal care services was another statistically significant predictor for early antenatal care booking in this study. Pregnant women who had good knowledge of antenatal care service were almost twice more likely to start ANC visits early compared to their counterparts. Similarly, pregnant mothers who have been advised before starting ANC visit were more likely to initiate ANC early compared to mothers who did not get any advice. This study finding is similar to a study conducted in Kham District, Debre Berhan, Dilla town, review study, and Southern Ethiopia.4,15,17,18,24 This indicates that previous knowledge, experience, and access to sources of information and access to counseling services might have helped them to utilize maternal health services like ANC. Though knowing only about maternal health services cannot be a guarantee for initiation of ANC early, it would enhance early utilization of ANC.
In this study, pregnant women whose pregnancy approved by urine tests were more likely to book early ANC than those by missed periods. This finding is consistent with studies conducted in Halaba Kulito which reported as pregnant mothers who recognize their pregnancy by urine test were more likely to book early ANC as compared to those mothers who approved their pregnancy by missed period.26 This showed that pregnant women who know pregnancy urine test would also opt for early initiation of ANC at the same time.
In the current study, the husband’s occupation was found to be factors associated with timely initiation of ANC visit. Those pregnant mothers whose husbands’ occupation daily laborers were less likely to start timely ANC booking compared to respondents who were government employed. This might be attributed to work-related pressure of husbands to accompany their wives to start ANC visits early.
Limitations
As the study used was a quantitative data collection method, it lacks the depth to identify the reasons behind associated factors for the inability to book antenatal care early. As the interview was conducted at health institutions, respondents may answer what is desirable and hence, the study was prone to socially desirable bias.
Conclusions
The study showed that 57.8% of pregnant mothers booked antenatal care early. Though this figure is better than the national EDHS 2016 estimate, still it is not satisfactory. Modifiable factors like husband’s education, knowledge on antenatal care service, means of recognizing current pregnancy, and being advised before starting antenatal care visits were factors significantly associated with early antenatal care booking. Thus, it is advisable to provide proper information about antenatal care services by health care providers and enhancement of health extension program to increase community awareness before and during pregnancy at all levels of health care provision is very important.
Acknowledgments
We are grateful to Bule Hora district health office for their cooperation during the data collection. We also thank data collectors, supervisors and study participants for their immense contribution for the successful accomplishment of this study.
Author Contributions
GT conceptualized the idea, and GT, RT, and DS analyzed the data. GT wrote the original draft. RT and DS supervised the overall study. RT prepared the manuscript and all authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. FMOH, Antenatal Care, Part 1. Blended Learning Module for the Health Extension Programme; 2017.
2. Alemu Y, Aragaw A. Early initiations of first antenatal care visit and associated factor among mothers who gave birth in the last six months preceding birth in Bahir Dar Zuria Woreda North West. Reprod Health. 2018;1–8.
3. WHO, Trends in Maternal Mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division; 2016.
4. Geta MB, Yallew WW. Early Initiation of Antenatal Care and Factors Associated with Early Antenatal Care Initiation at Health Facilities in Southern Ethiopia. Advances in Public Health. 2017:1624245.
5. WHO. Status of the health-related SDGs. World Health Stat. 2018;4–5.
6. Wado YD, Afework MF, Hindin MJ. Unintended pregnancies and the use of maternal health services in southwestern. Ethiopia BMC Int Health Human Rights. 2013;13:36. doi:10.1186/1472-698X-13-36
7. Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville, Maryland, USA: EPHI and ICF; 2019.
8. WHO. Provision of Effective Antenatal Care; Integrated Management of Pregnancy and Childbirth. 2006:3
9. Gidey G, et al. Timing of first focused antenatal care booking and associated factors among pregnant mothers who attend antenatal care in Central Zone, Tigray, Ethiopia. BMC Res Notes. 2017;10(1):608. doi:10.1186/s13104-017-2938-5
10. CSA. Ethiopia Demographic and Health Survey 2016. USA: CSA and ICF; 2016:134
11. Moller A-B. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. Lancet Glob Heal World Health Organization. 2013;5:10.
12. The Partnership for Maternal, Newborn and Child Health. Opportunities for Africa‘s Newborns Practical data, policy and programmatic support for newborn care in Africa. 2006. Available at https://www.who.int/pmnch/media/publications/africanewborns/en/.
13. USAID. National Guidelines for Antenatal Care For Service Providers. 2018. Available at http://themimu.info/sites/themimu.info/files/documents/Ref_Doc_National_Guidelines_for_Antenatal_Care_for_Service_Providers_May2018.pdf
14. Primary Health Care Systems (PRIMASYS): Case Study from Ethiopia, Abridged Version. Geneva:World Health Organization. License: CC BY-NC-SA 3.0 IGO. 2017.
15. Abukar T. Assessment of Timing of First Antenal Care Booking and Associated Factors Among Pregnant Women Who Attend Antenatal Care at Health Facilities in Dilla Town. Gedeo Zone, Southern Ethiopia,2014. Journal of Pregnancy and Child Health. 2016.
16. FMOH. Management Protocol on Selected Obstetrics Topics. Addis Ababa. 13. 2010.
17. Yang YE, Yoshitoku YOSHIDA. Factors Affecting the Utilization of Antenatal Care Services Among Women in Kham District. Xiengkhouang Province, LAO PDR. 2010. Nagoya journal of medical science.
18. Zegeye AM, Bitew BD, Koye DN. Proportion and Determinants of Early Antenatal Care Visit Among Pregnant Women Attending Antenatal Care in Debre Berhan Health Institutions, Central Ethiopia. African Journal of Reproductive Health. 2013; 1:130–136.
19. David W, Hosmer SL. Applied Logistic Regression Second Edition. Wiley-Interscience Publication. New York; 2000.
20. Belayneh T, Adefris M, Andargie G. Previous early antenatal service utilization improves timely booking: cross-sectional study at University of Gondar Hospital, northwest Ethiopia. J Pregnancy. 2014;2014.
21. Gebretsadik A, et al. Health extension workers involvement in the utilization of focused antenatal care service in rural sidama zone, Southern Ethiopia: a cross-sectional study. Health Serv Res Manag Epidemiol. 2019;6:2333392819835138.
22. Oladokun, Imran Morhason-Bello AFB, Departments BA. Proximate predictors of early antenatal registration among Nigerian pregnant women. Annals of African Medicine. 2010;9(4):9–12.
23. Gudu W. Factors influencing antenatal care utilization in Ethiopia. Systematic Rev Abstract. 2018;10(3):25–37.
24. Tesfaye G. Delayed initiation of antenatal care and associated factors in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2017;14. doi:10.1186/s12978-017-0412-4
25. Tekelab T, Chojenta C, Smith R, Lox Ton D. Factors affecting utilization of antenatal care in Ethiopia: a systematic review and meta-analysis. PLoS ONE. 2019;14(4):e0214848. doi:10.1371/journal.pone.0214848
26. Kondale M, Tumebo T, Gultie T, et al. Timing of first antenatal care visit and associated factors among pregnant women attending antenatal clinics in halaba kulito. J Women’s Health Care. 2016;5(2):8–11. doi:10.4172/2167-0420.1000308
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.