")
Back to Journals » Patient Preference and Adherence » Volume 14
Factors Associated with Health-Seeking Preference Among People Who Were Supposed to Cough for More Than 2 Weeks: A Cross-Sectional Study in Southeast China
Authors Wang W, Wang F, Peng Y, Liu K , Chen X, Chai C, Wang X, Chen B
Received 10 April 2020
Accepted for publication 19 June 2020
Published 12 July 2020 Volume 2020:14 Pages 1173—1183
DOI https://doi.org/10.2147/PPA.S257722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Wei Wang,1 Fei Wang,1 Ying Peng,1 Kui Liu,1 Xinyi Chen,2 Chengliang Chai,1 Xiaomeng Wang,1 Bin Chen1,3
1Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou 310051, People’s Republic of China; 2Department of Preventive Medicine, Epidemiology and Health Statistics, School of Medicine, Ningbo University, Ningbo 315211, People’s Republic of China; 3Key Laboratory of Vaccine, Prevention and Control of Infectious Disease of Zhejiang Province, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou 310051, People’s Republic of China
Correspondence: Bin Chen; Xiaomeng Wang
Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, 3399, Binsheng Road, Binjiang District, Hangzhzou, Zhejiang Province 310051, People’s Republic of China
Tel/Fax +86 571 8711 5183
; Tel +86 571 8711 5181
Fax +86 571 8711 5189
Email [email protected]; [email protected]
Background: The health-seeking preference of people with a cough > 2 weeks had not been extensively researched in southeast China. The study aimed to explore factors associated with health-seeking preference, which could provide more evidence to improve individuals’ appropriate health-seeking behavior.
Materials and Methods: From October 2018 to December 2018, this cross-sectional study was conducted in Zhejiang, China. A questionnaire was used to collect information on sociodemographic characteristics, knowledge of tuberculosis (TB), and health-seeking preference. The chi-square test and multivariable logistic regression were performed to evaluate factors associated with health-seeking preference.
Results: Of the 7174 participants, 3321 (46.3%) were men, 6148 (85.7%) were married, and 6013 (83.8%) knew about TB. Appropriate health-seeking preference was reported by 6229 (86.8%) participants. Respondents knowing about TB were more likely to seek appropriate care than those did not (89.6% vs 72.4%, p< 0.001). Of the 6013 participants knowing about TB, respondents with higher scores on five key items of TB knowledge were more likely to get appropriate health-seeking preference. About 805 (96.6%) participants with 5 scores on TB knowledge had appropriate care preference. Only 97 (72.4%) participants with a score of 0 reported an appropriate preference. Multivariable logistic regression showed residence, marital status, education level, occupation, and awareness of TB knowledge were predictors of appropriate health-seeking preference. Compared to participants with a score of 0 on five TB key knowledge, participants with a score of 5 were 8.57 times more likely to have appropriate health-seeking preference (95% confidence interval [CI]: 4.97– 14.78), followed by a score of 4 (odds ratio [OR]=5.99, 95% CI, 3.23– 8.03); 3 (OR=3.74, 95% CI, 2.44– 5.74); 2 (OR=1.99, 95% CI, 1.30– 3.02) and 1 (OR=1.17, 95% CI, 0.76– 1.80).
Conclusion: Participants with little knowledge of TB had a low level of appropriate health-seeking preference. Appropriate health-seeking preference of the participants improved with increased key knowledge level of TB.
Keywords: tuberculosis, health care-seeking behavior, cough
Introduction
The global tuberculosis (TB)1 report revealed that TB remained the top infectious killer worldwide. The disease can affect anyone anywhere, and approximately 10 million people become ill with TB each year globally.1 To date, most TB patients can be cured with a 6-month regimen of four first-line drugs and further transmission of infection is curtailed when patients are detected and treated in a timely manner. No new vaccine is licensed to prevent TB disease effectively, except for the Bacillus Calmette-Guérin vaccine. The preventive efficiency of this vaccine in adults is limited. The early detection of people with suspected symptoms and the standardized treatment of TB patients is crucial for the control and prevention of TB.
Previous studies demonstrated that the early detection of TB cases is affected by health-seeking delay and diagnosis delay.2,4 Rapid molecular detection technology has been endorsed by the World Health Organization (WHO) for TB detection.5 Compared to conventional methods, rapid molecular detection technology can greatly shorten the diagnosis delay time6,7 (ie, the duration from the first visit to a healthcare facility to when TB is bacteriologically confirmed). Thus, measures are also necessary to conduct to promote people with suspected TB symptoms to seek appropriate health care in a timely manner. Compared to other symptoms, the relative importance of a cough persisting >14 days as a predominant symptom of TB has been demonstrated in previous studies.8,9 The WHO refer to TB suspects as individuals with a cough persisting >2 weeks, if they are uninfected with the human immunodeficiency virus.10 However, the time from symptom onset to the first visit to a doctor was reported as 2–5 weeks in many districts.11,14 The health-seeking delay was affected by an individual’s awareness of TB knowledge, the national TB control policy, health-seeking factors such as the first health-seeking facilities, and socio-demographic features.15,18
China is in the WHO’s list of 30 countries with a high TB burden, and accounts for 9% of the global total new TB cases. Drug-resistant TB is also a public health threat in China with 14% share of the global burden of new cases of rifampicin-resistant TB in 2018.1 However, new TB case detection in the National Tuberculosis Protocol in China follows the WHO recommended passive case-finding guidelines. People with TB-related symptoms are identified when they seek care at a general health facility and are referred to a local TB dispensary for diagnosis and treatment.19 This passive case-finding strategy primarily depends on the individual’s health-seeking behavior,20 which is influenced by a multitude of factors, including socio-demographic characteristics and knowledge about the disease.21,22 Zhejiang Province is a relatively developed district in southeast China. The TB incidence in Zhejiang is in the low level in the country. However, based on the results of an investigation conducted in Zhejiang, 2018, the awareness rate of key knowledge on TB was only 48%.23 The median of health-seeking delay of primary TB patients in Zhejiang Province is approximately 17 days, which is significantly longer than the diagnosis delay time.24 Moreover, the health-seeking preference of people with suspected symptoms had not been extensively researched in southeast China. This study aimed to investigate health-seeking preference in the scenario of a cough lasting >2 weeks and associated factors that might provide evidence-based recommendation to promote people with suspected TB symptoms to seek appropriate health care in a timely manner.
Materials and Methods
Study Setting
From October 2018 to December 2018, a cross-sectional study was conducted in Zhejiang Province. Zhejiang Province is a relatively developed province in southeast China and consists of 11 prefectures. In 2018, it had a population of approximately 57 million residents and had an estimated landmass area of 105,500 square kilometers. The registered incident rate was reported to be 45.3/100,000 in 2018 by the Health Commission of Zhejiang Province.
Design and Sampling
The study included all 11 prefectures of Zhejiang Province. The sample size was calculated, based on the following formula:  in which n is the required sample size in one prefecture and p is the estimated awareness rate of key knowledge about TB. The symbol δ is the allowed margin of error. Previous study showed the awareness rate of key knowledge about TB was 44.5% in Zhejiang, 2014.25 We regarded 50% as the knowledge level of TB among participants in study area, which could get larger sample size. With an estimated awareness rate of 50% at a 95% confidence level, a sample size of 600 individuals was needed to achieve a 5% margin of error at one prefecture. The total estimated sample size was 6600 individuals among all 11 cities. Stratified cluster sampling method was applied to choose the survey objects. First, one county was randomly selected from one prefecture. Second, two townships were selected based on the socioeconomic status of the sampled county. In each selected township, three villages or communities were randomly selected. Thus, at least 100 participants from each sampled villages or communities needed to be investigated. If a selected respondent did not agree to participate in the study, another nonsampled neighborhood resident was selected.
in which n is the required sample size in one prefecture and p is the estimated awareness rate of key knowledge about TB. The symbol δ is the allowed margin of error. Previous study showed the awareness rate of key knowledge about TB was 44.5% in Zhejiang, 2014.25 We regarded 50% as the knowledge level of TB among participants in study area, which could get larger sample size. With an estimated awareness rate of 50% at a 95% confidence level, a sample size of 600 individuals was needed to achieve a 5% margin of error at one prefecture. The total estimated sample size was 6600 individuals among all 11 cities. Stratified cluster sampling method was applied to choose the survey objects. First, one county was randomly selected from one prefecture. Second, two townships were selected based on the socioeconomic status of the sampled county. In each selected township, three villages or communities were randomly selected. Thus, at least 100 participants from each sampled villages or communities needed to be investigated. If a selected respondent did not agree to participate in the study, another nonsampled neighborhood resident was selected.
Eligibility
Eligible participants needed to meet all of the following inclusion criteria: (1) was 12–75 years old, (2) was a resident or had lived locally for >6 months at the time of the investigation, and (3) had no communication barriers or mental disorders.
Questionnaire Survey and Quality Control
All investigators got provincial unified training. Qualified field investigators visited the participants face to face and conducted the survey. Electronic questionnaire, administered in the study, was developed based on previous research.25 The electronic questionnaire could control the quality of the responses, prevent the occurrence of missing items and logistical problems. The information collected by the e-questionnaire included socio-demographic characteristics, whether knew of TB or not, and health-seeking behavior. If respondents knew of TB, key information about TB was interviewed further, otherwise not. Socio-demographic characteristics information included gender, age, education level, marital status, occupation and type of residence. There were five items on key information about TB based on the National Guideline for TB Prevention and Control: “Do you believe TB is infectious?” “Should we suspect TB if we have coughed for more than two weeks?” “Did you know whether TB should be treated in designated TB hospital?” “Do you know about the free policy about TB diagnosis and first-line drugs?” “Do you believe TB can be cured?”. The information collected by the e-questionnaire was exported into Microsoft Excel, in which the database was set up.
Data Analysis
Statistical analysis was conducted by using IBM SPSS Statistics for Windows, version 19.0 (2010; IBM Corporation, Armonk, NY, USA). Participants’ TB key knowledge score, ranging 0–5 points, was calculated, based on the number of correct answers to five items on key information about TB. One point was awarded for each correctly answered item of key TB information.25 Among individuals who were supposed to have a cough for at least 2 weeks, those who sought help from doctor in hospitals or other community medical institutions were categorized as having “appropriate” health-seeking preference, and those who did nothing or visited a pharmacy themselves were categorized as having “inappropriate” health-seeking preference.
Frequency and percentages were used to describe characteristics and knowledge about TB. The Chi-square test was used to assess differences in health-seeking preference between different social demographic characteristics, awareness of knowledge on TB. Multivariable logistic regression was conducted to evaluate the predictors of appropriate health-seeking preference, for which the adjusted odds ratios and their corresponding 95% confidence intervals were calculated. Another multivariable logistic regression was conducted to evaluate the effect of participants’ TB key knowledge scores on health-seeking preference for which demographic characteristics were adjusted (eg, marital status, occupation, education level and type of residence). Stepwise logistic regression analysis was conducted in the multivariable logistic regression model. Analysis with a p-value < 0.05 (two-tailed test) was statistically significant.
Ethical Consideration
Respondents were informed of the study procedure and that their participation was voluntary. Informed consent was acquired at the beginning of the interview and recorded digitally. Informed consent from one of parents or legal guardians was also acquired for any participant under the age of 18 years. The study was approved by the Ethics Committee of the Zhejiang Provincial Center for Disease Prevention and Control (Hangzhou, China; approval number: 2018–035).
Results
Social-Demographic Characteristics of the Participants
A total of 7260 respondents were invited to participate in the study and 7174 agreed to participate. The response rate was 98.8%. Among the 7174 participants, 3323 (46.3%) were male, 4077 (56.8%) lived in rural areas, 6151 (85.7%) were married. Two thousand three hundred twenty-eight (32.5%) individuals were educated at the junior middle school level, followed by 1786 (24.9%) at primary school, 999 (13.9%) at high school, and 817 (11.4%) illiterate individuals. More than one-half of the participants were over 50 years old. With respect to occupation, 2679 (37.3%) individuals were farmers, 2679 (37.3%) individuals were farmers, followed by 998 (13.8%) unemployed individuals, 960 (13.4%) industrial workers, and 933 (12.9%) business/service personnel (Table 1).
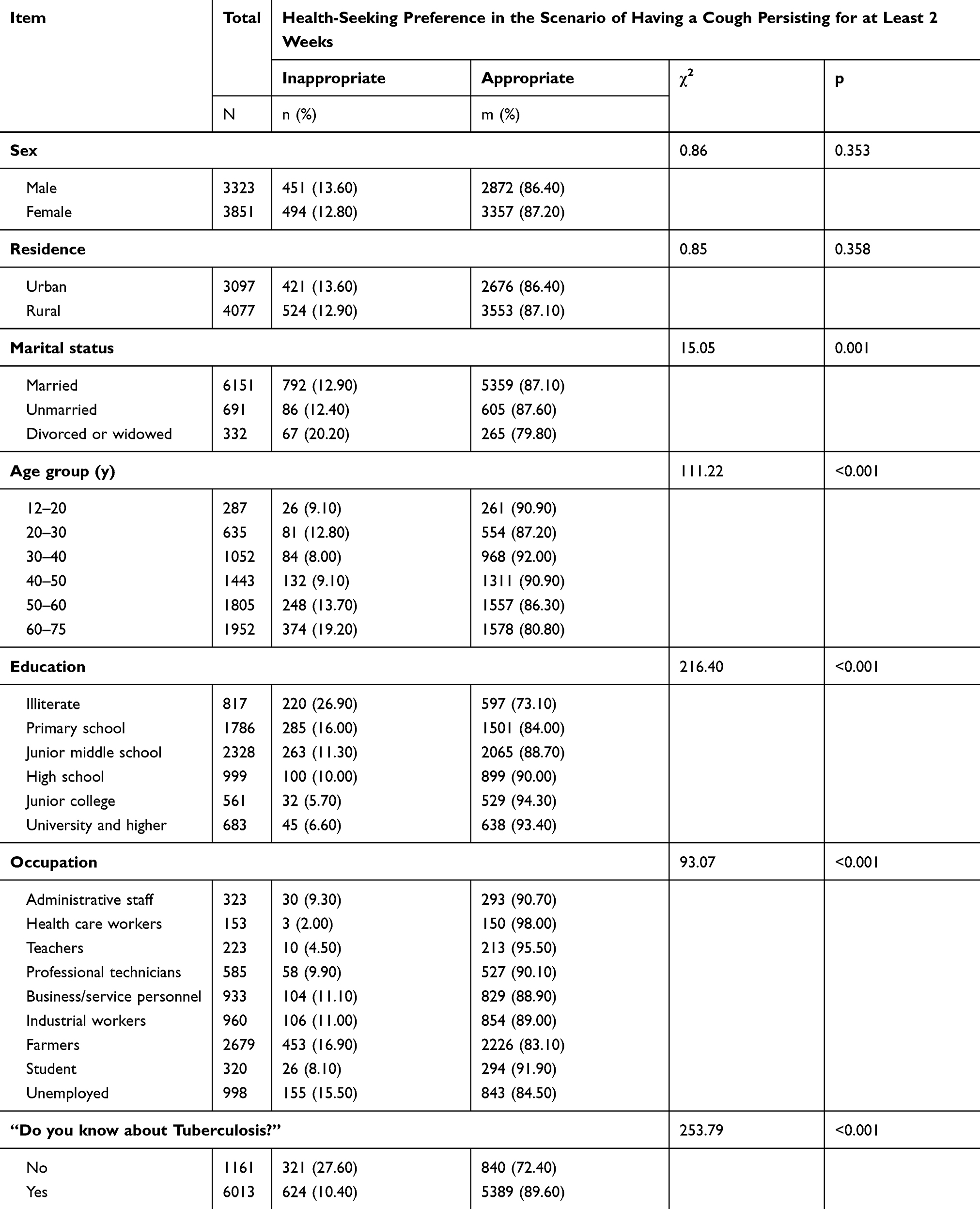 |
Table 1 Sociodemographic Characteristics and Differences in Health-Seeking Preference of Participants in Zhejiang, China (n=7174) |
Differences in the Health-Seeking Preference of Participants
Of the 7174 participants, appropriate health-seeking preference was reported by 6229 (86.8%) of them if they had a cough for at least 2 weeks. Significant statistical differences in health-seeking preference were observed for different marital statuses, age groups, education levels, and occupations. Divorced and widowed participants had a higher rate (20.2%) of inappropriate health-seeking preference.
More participants aged 60–75 years, 50–60 years, and 20–30 years, reported inappropriate health-seeking preference, compared to other age groups. Approximately 73.1% illiterate respondents expressed an appropriate health-seeking preference, which was a lower rate than that of participants in primary school (84%), junior middle school (88.7%), high school (90%), junior college (94.3%), and university and higher (93.4%). A higher proportion of farmers (16.9%) and unemployed respondents (15.6%) reported inappropriate preference than did individuals in other occupations. A significant statistical difference in health-seeking preference also existed between participants who did and did not know about TB (89.6% vs 72.4%, p<0.001) (Table 1).
The Association Between Knowledge of TB and Health-Seeking Preference Among Participants Who Knew of TB
Table 2 shows the association between knowledge of TB and health-seeking preference among 6013 participants who knew of TB. Approximately 90% of participants had appropriate health-seeking preference if they believed TB was infectious. In addition, 94% believed TB should be suspected if cough persists for more than 2 weeks, 93.6% knew TB should be treated in a designated hospital, 93% knew of the free policy on TB diagnosis and first-line drugs, and 91.9% believed TB could be cured. A significant statistical difference in health-seeking preference existed between participants who had knowledge of TB and participants who did not. The TB key knowledge scores of the 6013 participants who knew of TB was calculated, based on correct answers on five items of key information. The number of participants who had a score of 3 or a score of 4 was 1654 (for both), followed by 1127 participants with a score of 2; 611 participants with a score of 1; 833 participants with a score of 5; and 134 participants with a score of 0. More participants with higher scores had appropriate health-seeking preference: 96.6% of participants had a score of 5; 94%, a score of 4; 91.6%, a score of 3; 84.7%, a score of 2; and 75.6%, a score of 1. Only 72.4% of participants who had a score of 0 reported an appropriate preference, which was the same rate as that of participants who did not know about TB.
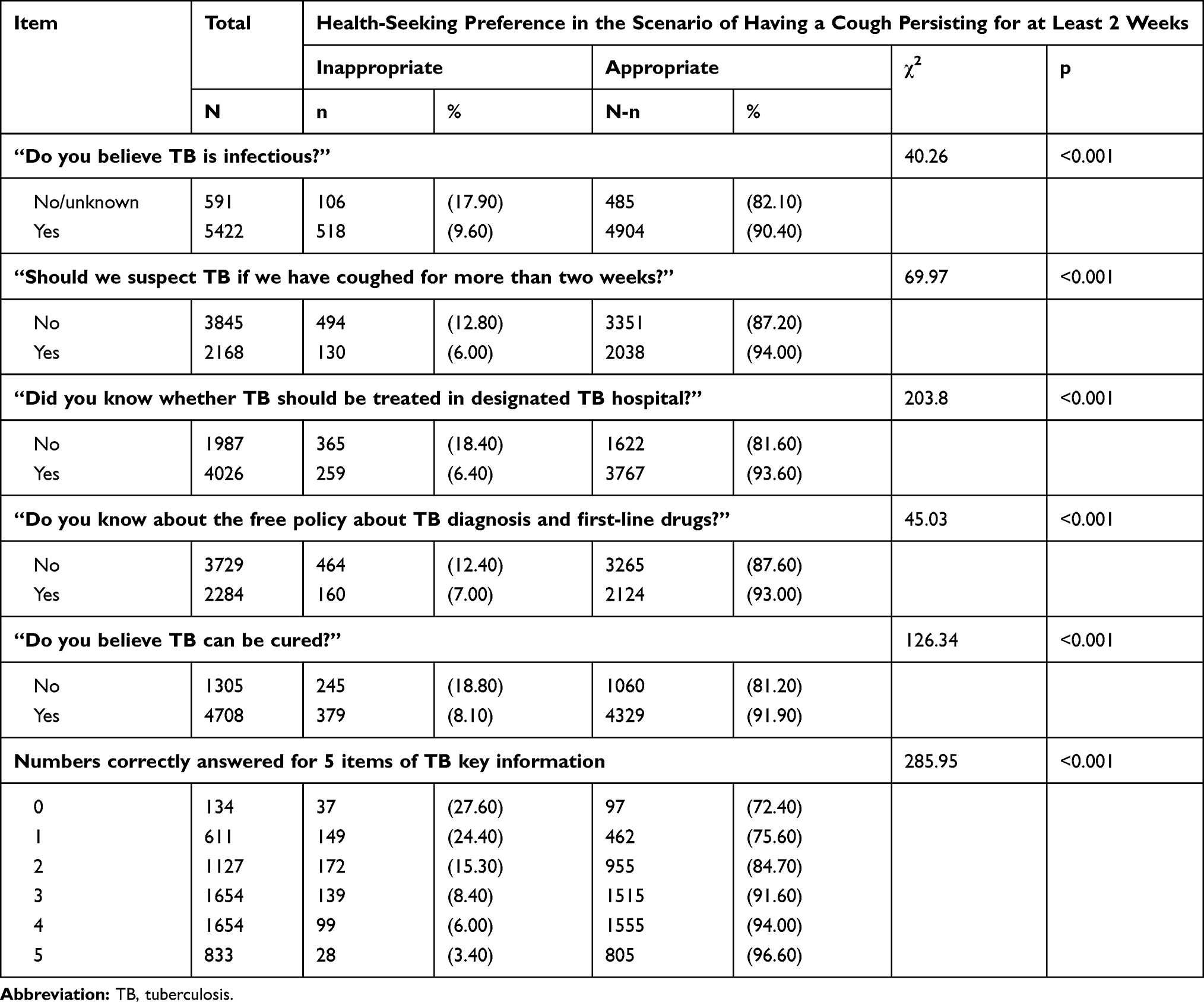 |
Table 2 The Association Between Knowledge of TB and Health-Seeking Preference Among Participants Who Knew About TB in Zhejiang, China (n=6013) |
Predictors of Health-Seeking Preference Among Participants Who Knew of TB
As presented in Table 3, multivariable logistic regression was conducted to detect the predictors of appropriate health-seeking preference if participants had a cough for >2 weeks. Participants who resided in a rural area were 1.54 times more likely (95% CI, 1.26–1.88) to have appropriate health-seeking preference than were urban residents. Unmarried participants were less likely than married participants to get appropriate health-seeking preference. Compared to illiterate participants, participants with an education level of primary school (OR=1.60; 95% CI, 1.21–2.11), junior middle school (OR=1.66; 95% CI,1.26–2.20), high school (OR=1.92; 95% CI,1.35–2.74), junior college (OR=4.02; 95% CI, 2.36–2.45), university and higher (OR=2.45; 95% CI,1.49–4.02) were more likely to have appropriate health-seeking preference. No significant statistical difference existed in administrative staff (OR=1.04; 95% CI, 0.62–1.75) or professional technicians (OR=1.27; 95% CI, 0.86–1.86) versus farmers. Participants who believed TB should be suspected if a cough persisted for >2 weeks (OR=1.52; 95% CI, 1.23–1.88), had knowledge that TB should be treated in a designated hospital (OR=2.24; 95% CI, 1.85–2.70), had knowledge of the free policy on TB diagnosis and first-line drugs (OR=1.23; 95% CI, 1.01–1.51), and believed TB could be cured (OR=1.84; 95% CI, 1.53–2.22) were more likely to have an appropriate health-seeking preference.
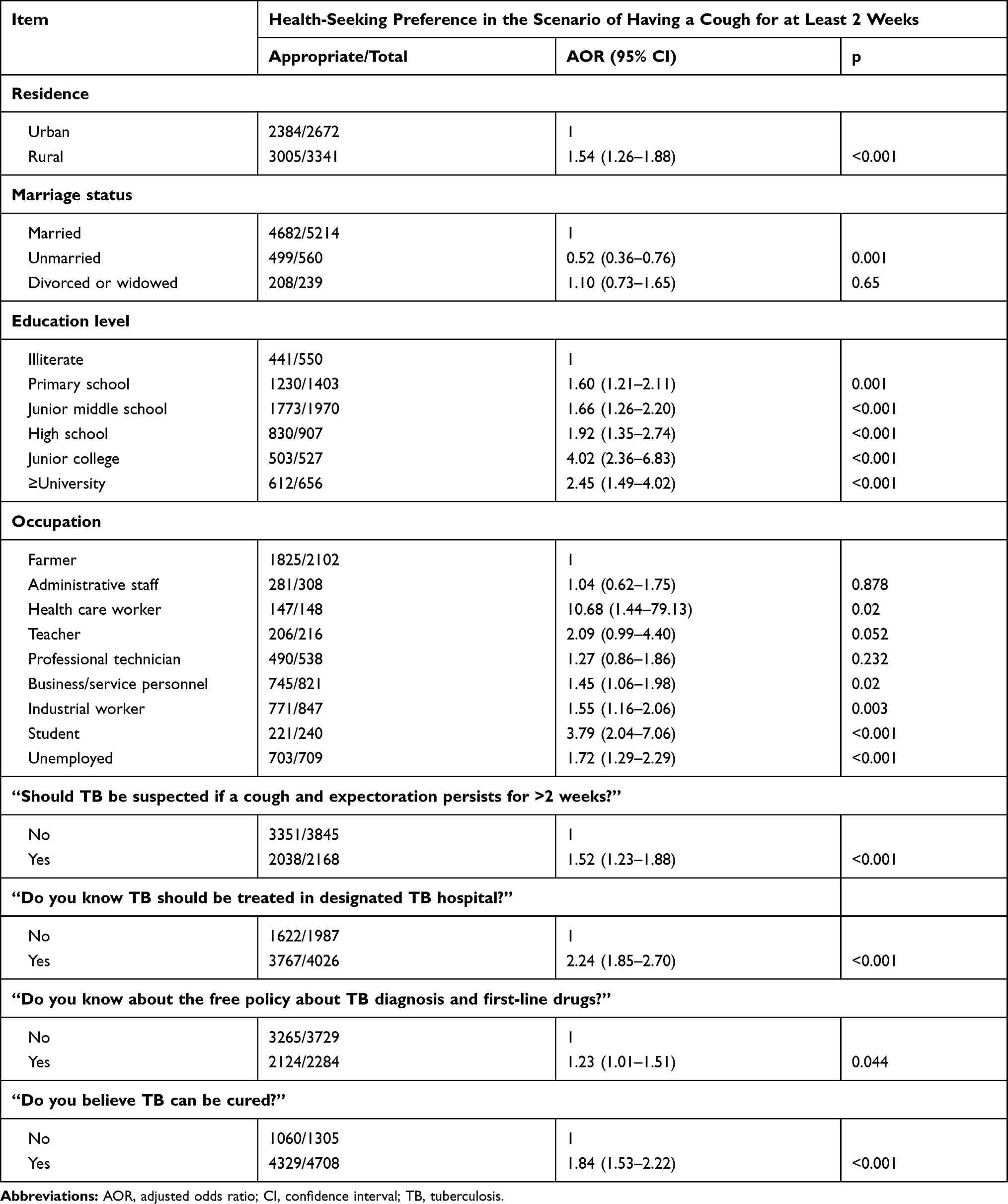 |
Table 3 Predictors of Health-Seeking Preference Among Participants Who Knew About TB in Zhejiang, China (n=6013) |
In addition, when residence, education, marriage, and occupation were adjusted for (Figure 1), participants with higher scores based on correct answers on five items of key information were more likely to get appropriate health-seeking preference. Compared to participants with a score of 0, participants with a score of 5 were 8.57 times more likely (95% CI, 4.97–14.78) to have appropriate health-seeking preference, followed by participants with a score of 4 (OR=5.99; 95% CI, 3.23–8.03), a score of 3 (OR=3.74; 95% CI, 2.44–5.74); a score of 2 (OR=1.99; 95% CI, 1.30–3.02); and a score of 1 (OR=1.17; 95% CI, 0.76–1.80).
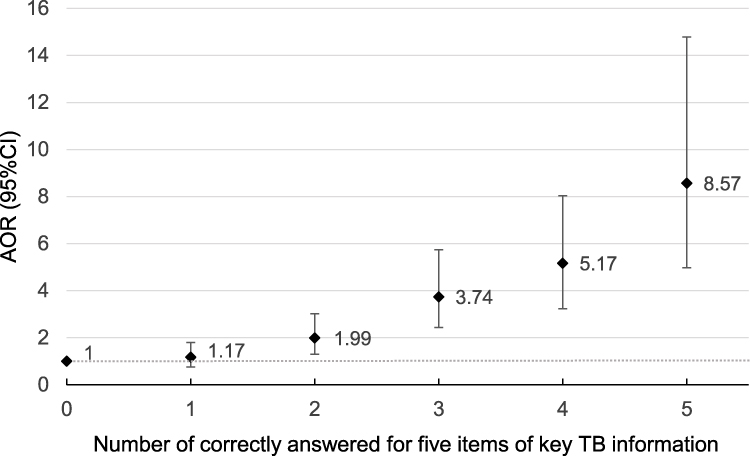 |
Figure 1 The association between knowledge of TB and health-seeking behavior among participants who knew about TB in Zhejiang, China (n=6013). Notes: 1) When residence, education, marriage, and occupation were adjusted for, participants with higher scores based on correct answers on five items of key information were more likely to get appropriate health-seeking preference. 2) Compared to participants with a score of 0, participants with a score of 5 were 8.57 times more likely (95% CI, 4.97–14.78) to have appropriate health-seeking preference, followed by participants with a score of 4 (OR=5.99; 95% CI, 3.23–8.03), a score of 3 (OR=3.74; 95% CI, 2.44–5.74); a score of 2 (OR=1.99; 95% CI, 1.30–3.02); and a score of 1 (OR=1.17; 95% CI, 0.76–1.80). 3) Appropriate health-seeking preference of the participants increased as the key knowledge scores increased. |
Discussion
This study investigated the health-seeking preference and associated factors of people in Zhejiang Province. We found that participants with little knowledge of TB had a low level of appropriate health-seeking preference. At present, a pulmonary TB detection strategy is primarily based on passive case-finding in health facilities in China. The appropriate health care-seeking choice of people with TB symptoms could improve access to TB diagnostic services and contribute to the early detection of cases.26 The study results also indicated that participants with higher knowledge scores about TB were more likely to report an appropriate health-seeking preference.
The proportion of participants with appropriate health-seeking preference was 86.8% if having a cough for at least two weeks in Zhejiang province, which was higher than that in the Western Cape of South Africa,27 Ethiopia,28 India,29 and Vietnam.30 A relatively low proportion of appropriate health-seeking preference was observed in two types of participants in our study: (1) participants who did not know about TB and (2) participants who knew of TB but had a score of 1 or less in five key areas of information about TB. Several studies have demonstrated that a delay in health-seeking behavior is influenced by the lack of knowledge of TB.31,33 Similar reasons such as wrong concepts were also mentioned in Vietnam34 and China.35 The inappropriate health-seeking behavior like self-medication could also contribute to the delay in the diagnosis and treatment by tuberculosis patients.36 Compared to participants with a score of 0 on TB knowledge, participants with a score of 2 or more were more likely to have appropriate health-seeking preference. However, the awareness rate of key information on TB was only about 50% in Zhejiang Province.25 Thus, more effective efforts such as community-based interventions,37 educational programs in schools,38 or multiple sources of information39 are necessary to conduct to convey more specific knowledge. These efforts could contribute to appropriate health-seeking behavior by people with suspected TB symptoms.
As stated in several studies,22,40 women are less likely than men to visit a medical health provider. A similar finding was also reported in a western province of China.32 This finding was associated with their poor knowledge of TB, and affected by their relatively lower position in a family and heavy housework, which led to their having fewer opportunities to learn information about TB. However, our findings suggested that no significant difference in appropriate health-seeking preference existed between women and men. Two kinds of factors may contribute to the result. First, no significant difference was reported between women and men on their awareness of TB and key information on TB in Zhejiang Province.23 Second, Zhejiang is a relatively prosperous and developed province in China. It has a more convenient transportation network, higher per-capita income levels. Thus, both women and men having more accessibility to health care facilities when they do not feel well. Despite these factors, their knowledge of TB and appropriate health-seeking preference were not very high. Measures should be taken to promote earlier appropriate health-seeking choice of people with symptoms of suspected TB.
The appropriate health-seeking choice was affected by knowledge level, and determined by education level, occupation, economic factors, social support, availability of adequate health services, and so on.41,42 More participants with a higher education level reported appropriate health-seeking choices than did illiterate individuals, which was confirmed in our study and other research studies.43 Compared to the married, the unmarried were less likely to have an appropriate health-seeking preference among participants who knew about TB, which might not only associate with their low awareness of TB knowledge, but also associate with their less social support from family. In our study, no significant difference was observed between rural and urban residents. However, when they knew about TB, rural residents were more likely than urban citizens to acquire an appropriate health-seeking choice. In Zhejiang Province, the detection, diagnosis, and treatment of TB was primarily based on a hierarchical medical system. Community health service institutions are convenient. Patients could get a higher reimbursement ratio of the national basic medical insurance in community health services. Patients with suspected TB identified by community health service workers would be transferred to the local TB-designated hospital. Some urban citizens with mild symptoms but without sufficient knowledge of TB may first select inappropriate health-seeking. In addition, the sensitivity of only the symptom of a cough persisting >2 weeks for detecting individuals with TB was not very high.8 This fact could also confuse people with other respiratory diseases. This may also affect the choice of farmers, whose knowledge about TB was relatively poorer than other occupation participants. However, although students’ knowledge on TB was also in low, their health-seeking choice was more likely to be appropriate than farmers. Students could get more support from school and family when they did not feel well. Thus, different policies based on different population groups should be considered to strengthen accurate information dissemination on TB. Education program on promoting awareness of TB and appropriate health-seeking choice was conducted, especially for farmers.
Some limitations of our research exist. First, all information obtained in the survey depended on the participants’ recalled history. Second, the health-seeking preference reported by participants, which was based on what they usually did, assumed that they had experienced a cough for 2 weeks or longer. The results reported may have a bias with their actual behavior. Third, causal conclusions cannot be drawn because of the nature of the cross-sectional study method employed in the study. In addition, the survey results reflected the present situation in Zhejiang Province, and could only apply to areas with similar demographic characteristics and economical status.
Conclusion
Our study results indicated participants with little knowledge of TB had a low level of appropriate health-seeking choice. An inappropriate health-seeking choice occurred more frequently among farmers, individuals with a low education level. Appropriate health-seeking preference of the participants increased as the key knowledge scores increased. Hence, public health education on the knowledge of TB and appropriate health-seeking choice would be important. A change in policy to focus on high-risk group of inappropriate health-seeking behavior should also be necessary. In the future research, it is necessary to evaluate the role of health interventions and policy in improving health-seeking behavior and the prevention and control of TB.
Acknowledgments
We would like to thank the staff from the local CDC and community health service workers for their help with the field survey. We would like to thank Editage for English language editing.
Author Contributions
W.W., B.C., X.W., C.C involved in the design of the study. W.W., B.C., F.W., Y.P., K.L., X.C. involved in data collection and analysis. W.W., B.C. wrote the initial draft and reviewed the manuscript. All authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2019. Geneva: World Health Organization;2019. Licence: CC BY-NC-SA 3.0 IGO.
2. Long R. Making a timely diagnosis of pulmonary tuberculosis. Can Respir J. 2015;22(6):
3. Chanda-Kapata P, Kapata N, Masiye F, et al. Health seeking behaviour among individuals with presumptive tuberculosis in Zambia. PLoS One. 2016;11(10):e0163975. doi:10.1371/journal.pone.0163975
4. Getnet F, Demissie M, Assefa N, Mengistie B, Worku A. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and meta-analysis. BMC Pulm Med. 2017;17(1):202. doi:10.1186/s12890-017-0551-y
5. World Health Organization. The use of molecular line probe assays for the detection of resistance to isoniazid and rifampicin policy update. 2016.
6. Pai M, Schito M. Tuberculosis diagnostics in 2015: landscape, priorities, needs, and prospects. J Infect Dis. 2015;211(Suppl 2):S21–28. doi:10.1093/infdis/jiu803
7. Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005–1015. doi:10.1056/NEJMoa0907847
8. den Boon S, White NW, van Lill SW, et al. An evaluation of symptom and chest radiographic screening in tuberculosis prevalence surveys. Int J Tuberc Lung Dis. 2006;10(8):876–882.
9. Gopi PG, Subramani R, Narayanan PR. Evaluation of different types of chest symptoms for diagnosing pulmonary tuberculosis cases in community surveys. Indian J Tuberc. 2008;55(3):116–121.
10. World Health Organization. Guidelines for treatment of tuberculosis. 2010.
11. Qureshi SA, Morkve O, Mustafa T. Patient and health system delays: health-care seeking behaviour among pulmonary tuberculosis patients in Pakistan. J Pak Med Assoc. 2008;58(6):318–321.
12. Auer C, Kiefer S, Zuske M, et al. Health-seeking behaviour and treatment delay in patients with pulmonary tuberculosis in Switzerland: some slip through the net. Swiss Med Wkly. 2018;148:w14659. doi:10.4414/smw.2018.14575
13. Segagni Lusignani L, Quaglio G, Atzori A, et al. Factors associated with patient and health care system delay in diagnosis for tuberculosis in the province of Luanda, Angola. BMC Infect Dis. 2013;13(1):168. doi:10.1186/1471-2334-13-168
14. Tattevin P, Che D, Fraisse P, et al. Factors associated with patient and health care system delay in the diagnosis of tuberculosis in France. Int J Tuberc Lung Dis. 2012;16(4):510–515. doi:10.5588/ijtld.11.0420
15. Yirgu R, Lemessa F, Hirpa S, Alemayehu A, Klinkenberg E. Determinants of delayed care seeking for TB suggestive symptoms in Seru district, Oromiya region, Ethiopia: a community based unmatched case-control study. BMC Infect Dis. 2017;17(1):292. doi:10.1186/s12879-017-2407-8
16. Zhao X, Yang P, Gai R, Mei L, Wang X, Xu L. Determinants of health care-seeking delay among tuberculosis patients in Shandong Province, China. Eur J Public Health. 2014;24(5):757–761. doi:10.1093/eurpub/ckt113
17. Tong Y, Guan X, Hou S, et al. Determinants of health care-seeking delay among tuberculosis patients in rural area of central China. Int J Environ Res Public Health. 2018;15(9):9. doi:10.3390/ijerph15091998
18. Ukwaja KN, Alobu I, Nweke CO, Onyenwe EC. Healthcare-seeking behavior, treatment delays and its determinants among pulmonary tuberculosis patients in rural Nigeria: a cross-sectional study. BMC Health Serv Res. 2013;13(1):25. doi:10.1186/1472-6963-13-25
19. Wei X, Zou G, Walley J, et al. China tuberculosis policy at crucial crossroads: comparing the practice of different hospital and tuberculosis control collaboration models using survey data. PLoS One. 2014;9(3):e90596. doi:10.1371/journal.pone.0090596
20. Luis SF, Kamp N, Mitchell EM, Henriksen K, van Leth F. Health-seeking norms for tuberculosis symptoms in southern Angola: implications for behaviour change communications. Int J Tuberc Lung Dis. 2011;15(7):943–948. doi:10.5588/ijtld.10.0588
21. Alema HB, Hailemariam SA, Misgina KH, et al. Health care seeking delay among pulmonary tuberculosis patients in North West zone of Tigrai region, North Ethiopia. BMC Infect Dis. 2019;19(1):309. doi:10.1186/s12879-019-3893-7
22. Yimer S, Holm-Hansen C, Yimaldu T, Bjune G. Health care seeking among pulmonary tuberculosis suspects and patients in rural Ethiopia: a community-based study. BMC Public Health. 2009;9(1):454. doi:10.1186/1471-2458-9-454
23. Chen X, Wang W, Wang X, et al. Public awareness of tuberculosis in Southeast China: a population-based study. Int J Environ Res Public Health. 2019;16(21):21. doi:10.3390/ijerph16214290
24. Chen SH, Wang XM, Zhong JM, Chen B, Huang Y. Factors associated with diagnostic delay for primary pulmonary tuberculosis patients in Zhejiang province. Chin J Public Health. 29(4):481–484.
25. Zhang MW, Chen SH, Zhong JM, et al. Awareness of key knowledge about tuberculosis and its major influencing factors among general population in Zhejiang province. Chin J Public Health. 2017;33(11):1607–1611.
26. Rudolf F, Haraldsdottir TL, Mendes MS, et al. Can tuberculosis case finding among health-care seeking adults be improved? Observations from Bissau. Int J Tuberc Lung Dis. 2014;18(3):277–285. doi:10.5588/ijtld.13.0517
27. Christian C, Burger C, Claassens M, Bond V, Burger R. Patient predictors of health-seeking behaviour for persons coughing for more than two weeks in high-burden tuberculosis communities: the case of the Western Cape, South Africa. BMC Health Serv Res. 2019;19(1):160. doi:10.1186/s12913-019-3992-6
28. Abebe G, Deribew A, Apers L, et al. Knowledge, health seeking behavior and perceived stigma towards tuberculosis among tuberculosis suspects in a rural community in southwest Ethiopia. PLoS One. 2010;5(10):e13339. doi:10.1371/journal.pone.0013339
29. Satyanarayana S, Nair SA, Chadha SS, et al. Health-care seeking among people with cough of 2 weeks or more in India. Is Passive TB Case Finding Sufficient? Public Health Action. 2012;2(4):157–161. doi:10.5588/pha.12.0019
30. Hoa NB, Tiemersma EW, Sy DN, et al. Health-seeking behaviour among adults with prolonged cough in Vietnam. Trop Med Int Health. 2011;16(10):1260–1267. doi:10.1111/j.1365-3156.2011.02823.x
31. Long Q, Li Y, Wang Y, et al. Barriers to accessing TB diagnosis for rural-to-urban migrants with chronic cough in Chongqing, China: a mixed methods study. BMC Health Serv Res. 2008;8:202. doi:10.1186/1472-6963-8-202
32. Wang J, Fei Y, Shen H, Xu B. Gender difference in knowledge of tuberculosis and associated health-care seeking behaviors: a cross-sectional study in a rural area of China. BMC Public Health. 2008;8(1):354. doi:10.1186/1471-2458-8-354
33. Senkoro M, Hinderaker SG, Mfinanga SG, et al. Health care-seeking behaviour among people with cough in Tanzania: findings from a tuberculosis prevalence survey. Int J Tuberc Lung Dis. 2015;19(6):640–646. doi:10.5588/ijtld.14.0499
34. Hoa NP, Thorson AE, Long NH, Diwan VK. Knowledge of tuberculosis and associated health-seeking behaviour among rural Vietnamese adults with a cough for at least three weeks. Scand J Public Health. 2003;31(Suppl. 62):59–65. doi:10.1080/14034950310015121
35. Wang Y, Long Q, Liu Q, Tolhurst R, Tang S. Treatment seeking for symptoms suggestive of TB: comparison between migrants and permanent urban residents in Chongqing, China. Trop Med Int Health. 2008;13(7):927–933. doi:10.1111/j.1365-3156.2008.02093.x
36. Dantas DNA, Enders BC, Oliveira DRC, Vieira C, Queiroz AAR, Arcencio RA. Factors associated with delay in seeking care by tuberculosis patients. Rev Bras Enferm. 2018;71(suppl 1):646–651. doi:10.1590/0034-7167-2016-0680
37. Dewi C, Barclay L, Passey M, Wilson S. Improving knowledge and behaviours related to the cause, transmission and prevention of Tuberculosis and early case detection: a descriptive study of community led Tuberculosis program in Flores, Indonesia. BMC Public Health. 2016;16:740. doi:10.1186/s12889-016-3448-4
38. Haasnoot PJ, Boeting TE, Kuney MO, van Roosmalen J. Knowledge, attitudes, and practice of tuberculosis among Maasai in Simanjiro district, Tanzania. Am J Trop Med Hyg. 2010;83(4):902–905. doi:10.4269/ajtmh.2010.10-0061
39. Chizimba R, Christofides N, Chirwa T, et al. The association between multiple sources of information and risk perceptions of tuberculosis, Ntcheu district, Malawi. PLoS One. 2015;10(4):e0122998. doi:10.1371/journal.pone.0122998
40. Bati J, Legesse M, Medhin G. Community’s knowledge, attitudes and practices about tuberculosis in Itang Special District, Gambella Region, South Western Ethiopia. BMC Public Health. 2013;13:734. doi:10.1186/1471-2458-13-734
41. Wieland ML, Weis JA, Yawn BP, et al. Perceptions of tuberculosis among immigrants and refugees at an adult education center: a community-based participatory research approach. J Immigr Minor Health. 2012;14(1):
42. Lienhardt C, Glaziou P, Uplekar M, Lonnroth K, Getahun H, Raviglione M. Global tuberculosis control: lessons learnt and future prospects. Nat Rev Microbiol. 2012;10(6):
43. Tolossa D, Medhin G, Legesse M. Community knowledge, attitude, and practices towards tuberculosis in Shinile town, Somali regional state, eastern Ethiopia: a cross-sectional study. BMC Public Health. 2014;14:804. doi:10.1186/1471-2458-14-804
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.