")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Factors Affecting the Knowledge and Motivation of Health Cadres in Stunting Prevention Among Children in Indonesia
Authors Mediani HS , Hendrawati S , Pahria T, Mediawati AS , Suryani M
Received 1 January 2022
Accepted for publication 20 April 2022
Published 11 May 2022 Volume 2022:15 Pages 1069—1082
DOI https://doi.org/10.2147/JMDH.S356736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Henny Suzana Mediani,1 Sri Hendrawati,1 Tuti Pahria,2 Ati Surya Mediawati,3 Mira Suryani4
1Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Medical and Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 3Department Fundamental of Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 4Department of Computer Science, Math and Science Faculty, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Henny Suzana Mediani, Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, 45363, Indonesia, Tel/Fax +62 22-7795596, Email [email protected]
Purpose: Stunting is a public health problem in Indonesia with a relatively high incidence, thereby making its prevention a priority for the Indonesian government. It potentially causes short and long effects on the quality of human resources as well as the productivity of stunted children when they grow up. Therefore, prevention and early detection efforts are needed by health professionals and cadres. Earlier studies have identified complexities associated with the determinant factors of stunting. This study aims to examine the association between sociodemographic factors as well as the knowledge and motivation of health cadres in stunting prevention in West Java.
Methods: A correlational study with a cross-sectional approach was conducted on health cadres samples from 8 districts/cities in West Java Province namely Karawang, Tasikmalaya, Garut, Bandung, Subang, Sukabumi, Cianjur, and West Bandung. A total of 363 health cadres participated and the sampling technique used is the stratified method. The data were collected using a questionnaire developed specifically for this study and were analyzed using a correlation with chi-square test and presented in the form of a frequency distribution.
Results: The results showed the majority of health cadres namely 81.27% had good knowledge, which was significantly influenced by education level and marital status with a P-value < 0.05. Meanwhile, approximately half of the respondents had moderate motivation with 47.66%, while one-third or 39.12% had high motivation. This motivation was significantly influenced by education level, marital status, and age with p < 0.05.
Conclusion: Based on the results, it was concluded that the roles and functions of health cadres need to be improved in the prevention and early detection of stunting in West Java by providing continuous guidance, stunting prevention training, and award presentations.
Keywords: children stunting, health cadres, knowledge, motivation, stunting prevention
Introduction
Stunting is one of the nutritional problems experienced by children under five globally with a high prevalence in developing countries including Indonesia, where up to 22.9% or 154.8 million children under five experienced stunting in 2016, while in 2017, the value was 22.2% or approximately 150.8 million.1–2 According to the 2014 Global Nutrition Report, Indonesia is one of the top 17 countries out of 117 that have three nutritional problems, one of which is stunting. Moreover, about 56% of stunted children live in Asia and 36% in Africa,2 while approximately 30% of under five years old children are stunted globally.4–6 Children with this condition are characterized by a Z-score for body length for age (PB/U), or height for age (TB/U), weight for age (W/U), and weight for height (W/TB) less than −2 SD.3–5
Indonesia is included in the top five countries with the highest prevalence of stunting in Asia-Africa2 with approximately 9 million affected children out of the 24.5 million population.7 The prevalence from 2007 to 2018 is still above the threshold set by WHO, which is 20%. In 2007, 2010, and 2013, it reached 36.8%, 35.6%, 37.2% respectively and in 2018, it was 30.8%.8 Meanwhile, West Java is the second province in Indonesia with the largest population and has a stunting prevalence rate of 29.2% or 2.7 million in under five years old children,9 this figure is in the medium level, while values above 30% indicate a high prevalence. Based on the non-public health problem limit set by the WHO for stunting, West Java is one of the provinces in Indonesia with a high prevalence.10
Stunting occurs due to lack of adequate nutrition or malnutrition, particularly in the First 1000 Days of Life.11–16 Malnutrition at an early age increases infant and child mortality, while stunting is estimated to cause approximately one million child deaths every year,15,16 due to the frequent illness and bad posture during adulthood in affected persons.17 The adverse effects in the short term can also cause disturbance of the brain, intelligence, impaired physical growth, and metabolic disorders in the body.15,16,18 Meanwhile, in the long term, the detrimental consequences caused are declined cognitive abilities and learning achievement, decreased immunity which increases susceptibility to sicknesses, high risk of diabetes, obesity, heart and blood vessel disease, cancer, stroke, disability in old age, as well as poor quality of work that leads to low economic productivity.8,11,12,16,19
Several studies reported that various factors contribute to the incidence of stunting in children, such as parenting, exclusive breastfeeding practices, psychosocial stimulation, poor hygiene and environmental sanitation, especially in densely populated areas, as well as remote and demographic factors.10,17,20,21 Other basic factors include economic influence, mother’s education, as well as intermediates such as the number of family members, mother’s height and age, as well as the number of children.17,22,23 This is followed by proximal factors such as exclusive breastfeeding, age, and infants with low birth weight (LBW).10,24
The Indonesian government has made regulations to reduce stunting rates by issuing Presidential Regulation Number 42 of 2013 concerning the National Movement for the Acceleration of Nutrition Improvement which focuses on the First 1000 Days of Life (1000 HPK). This movement aims to increase effectiveness and initiatives by increasing coordination and technical support, advocacy innovative, and participatory partnership in improving the nutritional status and health of people in Indonesia. However, the rate has not decreased because the various efforts have not been balanced with the knowledge, attitudes, and behavior of parents, as well as family supports and health cadres in preventing stunting within the first 1000 HPK.
Health cadres in integrated healthcare centers (Posyandu) play an important role in bridging the gap between healthcare providers and the community by providing information related to health, such as child growth and development.13 Stunting prevention in the community is implemented by involving health cadres in the respective working areas. This is consistent with the pillars of handling stunting in Indonesia at the 3rd point, namely convergence, coordination, as well as consolidation of national programs. As also mentioned in the Rural ministry regulations PDTT No.19 2017 at the 9th point, the implementation of community empowerment in the promotion of public health and healthy living includes health cadres’ sub-point involvement in monthly posyandu activities program.
The active role of health cadres in the early detection of stunting and stimulation of growth and development in children at the posyandu contributes to improving the quality of public health status. This is because early prevention is one of the best ways to reduce stunting prevalence. Posyandu cadres as community representatives have an important role in the implementation of interventions that are effective in reducing the stunting rate of children. Consequently, they need to have the basic requirements, including the knowledge and skills to maximize their respective roles which are expected to improve optimally with high motivation.25 Based on previous studies, the majority of the health cadres have fairly good knowledge of the development and early detection of malnutrition in children under five years.26,27 Meanwhile, the active role of the health cadres is based on age, education, occupation, and length of work, although age is an indirect contributing factor. There are still clear gaps on the effect of internal factors, including cadre knowledge and motivation on the efforts to prevent stunting in children. Therefore, this study aims to identify the associations between the sociodemographic characteristics with the knowledge and motivation of health cadres in stunting prevention in West Java.
Materials and Methods
Research Methods
This study was carried out based on a cross-sectional approach with a correlational analytic method to examine the relationship between the characteristics as well as the knowledge and motivation of health cadres in stunting prevention in West Java. Therefore, it determined the relationship between the independent and the dependent variable by making instantaneous measurements.28
Study Location
The study was conducted in 8 districts/cities in West Java namely Bandung, West Bandung, Garut, Tasikmalaya, Cianjur, Subang, Sukabumi, and Karawang between August and December 2020.
Sampling Design
The stratified simple random sampling technique was used by taking groups with simple randomness as respondents.29 A total of 363 health cadres from 8 districts/cities participated in this study.
Data Collection
The data were collected using a questionnaire consisting of the respondents’ demographics as well as their knowledge and motivation in stunting prevention. Meanwhile, it was initially analyzed through content and a constructed test on validity and reliability.
Statistical Analysis
A descriptive univariate analysis was used as the first section presenting the percentage of response to each variable. Bivariate analysis comprising a Chi-square score analysis was used to assess the relationship between health cadres’ characteristics such as occupation, education, marital status and age, with the knowledge and motivation of stunting prevention in West Java. All statistical analysis was performed using the SPSS Windows Version 19.0 and statistical significance was set α = 0.05.
Ethical Consideration
This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (IRB) of Universitas Padjadjaran Bandung, Indonesia with the ethical approval number: 594/UN6.KEP/EC/2020. Participants were enrolled in the study after providing informed consent which contains relevant information and it is conditional on participation in the study after signing the consent form. All participants agreed to participate and contribute to this study.
Results
Health Cadres’ Characteristics
The health cadres’ characteristics across the 8 districts/cities are depicted in Table 1. Among the 363 participants, a total of 270 or 74.38% have jobs while 93 or 25.62% are unemployed. In terms of education, there was a great variation with 139 or 38.29% having high school education, 124 or 34.16% were diploma/bachelor graduates, 57 or 15.70% had junior high school education, while 43 or 11, 85% were elementary school graduates. Regarding marital status, the majority of respondents namely 330 or 90.91% were married, 25 or 6.89% were single, while 8 or 20.20% were widowed. Moreover, in terms of the health cadres age, the mean was 39 years.
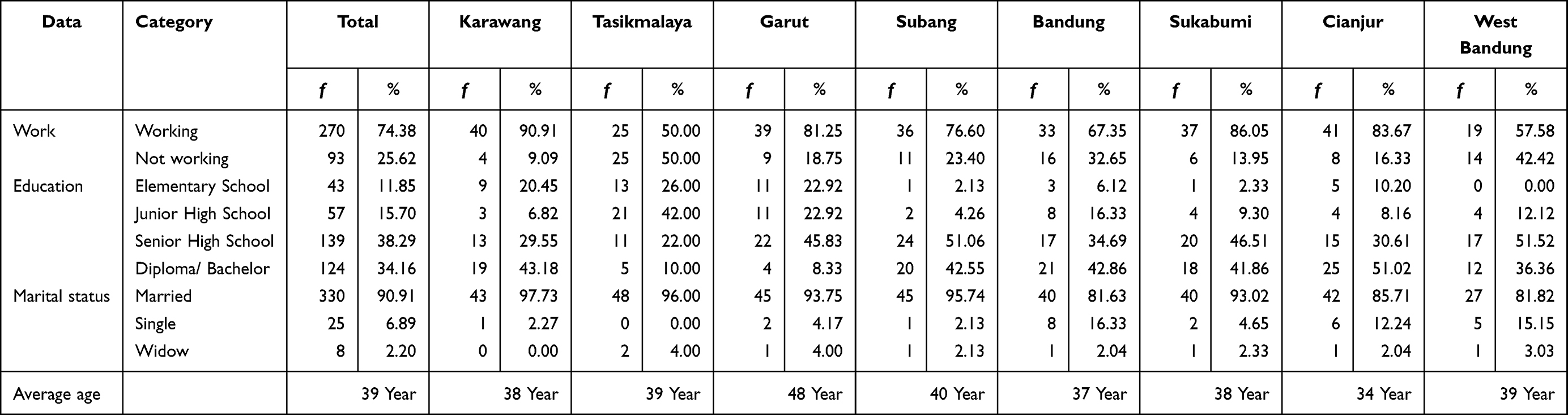 |
Table 1 Description of the Health Cadre Respondents Characteristics in West Java (n=363) |
Knowledge and Motivation of Health Cadres in Stunting Prevention
The health cadres’ knowledge and motivation on stunting prevention in children under five years in 8 districts/cities are illustrated in Table 2. Based on the results, the majority of respondents already have good knowledge, up to 295 or 81.27%, followed by 36 or 9.92% which had sufficient, and 32 or 8.82% that lack knowledge.
 |
Table 2 Knowledge and Motivation of Health Cadres in Integrated Stunting Prevention Efforts in West Java (n=363) |
The results also found that the majority of the health cadres have moderate motivation related to stunting prevention efforts while 142 or 39.12% have high motivation. Therefore, it was concluded from Table 2 that most of the health cadres have good knowledge as well as moderate to high motivation about stunting prevention efforts in each district/city.
Relationship Between Knowledge and Motivation with Occupation of Health Cadres in West Java
As presented in Table 3, the chi-square score analysis results show that there was no significant relationship between the knowledge and motivation of cadres with the work carried out in all districts/cities in West Java Province namely Bandung, West Bandung, Garut, Tasikmalaya, Cianjur, Subang, Sukabumi, and Karawang as indicated by the probability values generated which were all greater than an error rate of 0.05 or 5%.
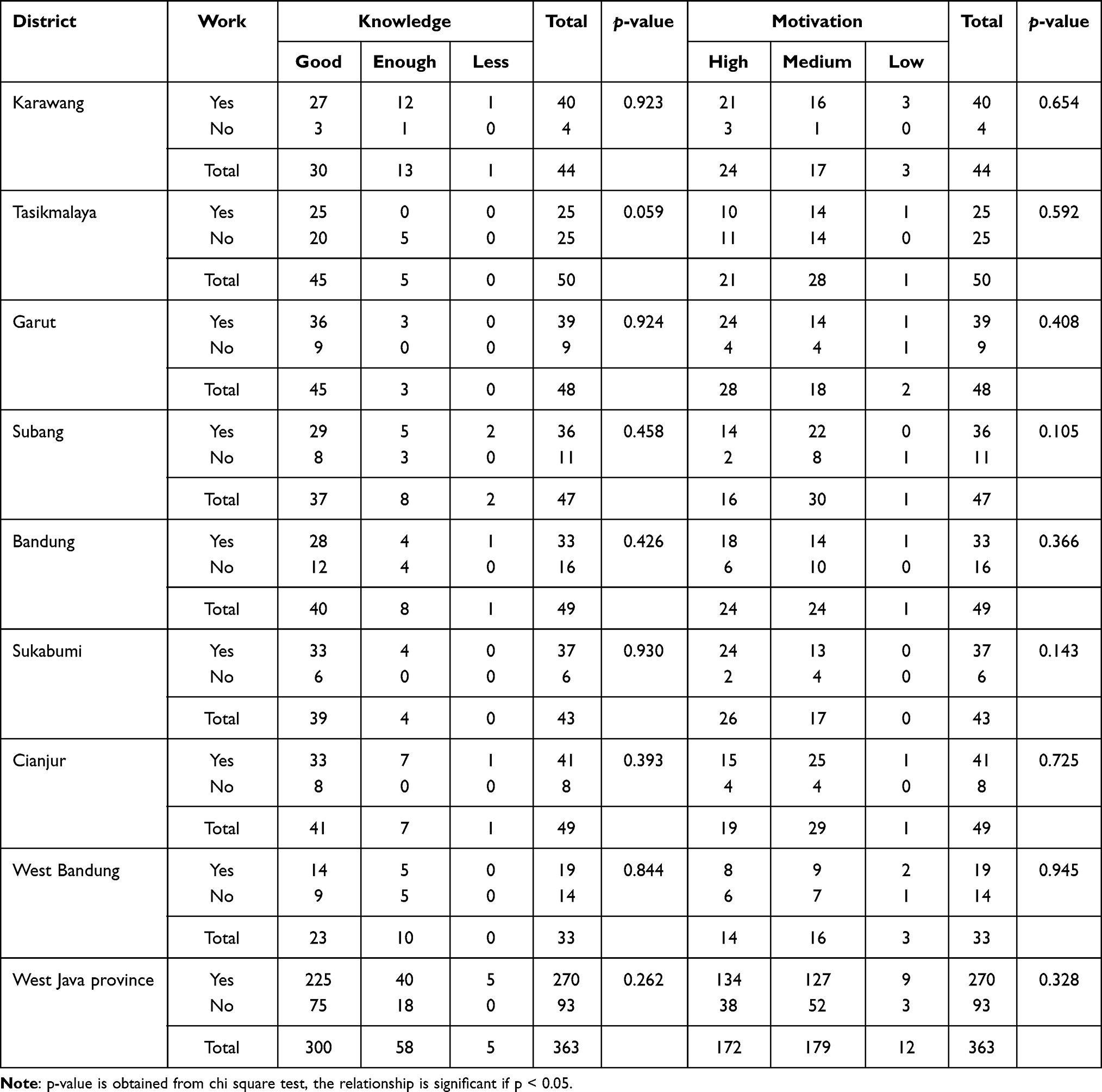 |
Table 3 Relationship of Knowledge and Motivation with Occupation of Health Cadres in West Java (n=363) |
Relationship Between Knowledge and Motivation with Health Cadre Education in West Java
The bivariate analysis results demonstrated in Table 4 show that there was no significant relationship between knowledge and the health cadres’ education as indicated by a probability value greater than an error rate of 0.05 or 5%. However, the value obtained generally in West Java Province was 0.017 which is <0.05, hence, it was concluded that the overall data had a significant relationship with education, indicating that good knowledge tends to be associated with higher education including Senior High School, and Diploma/Bachelor, while sufficient tends to be associated with low education including, Elementary School. Furthermore, Table 4 shows that there was no significant relationship between cadre motivation and education as indicated by a probability value greater than an error rate of 0.05 or 5%. A significant relationship was only found in Subang Regency with a p-value of 0.000 which is <0.05, hence, high motivation tends to be associated with fairly high education such as Senior High School and Diploma/Bachelor, while low tends to be associated with relatively low education, namely Junior High School.
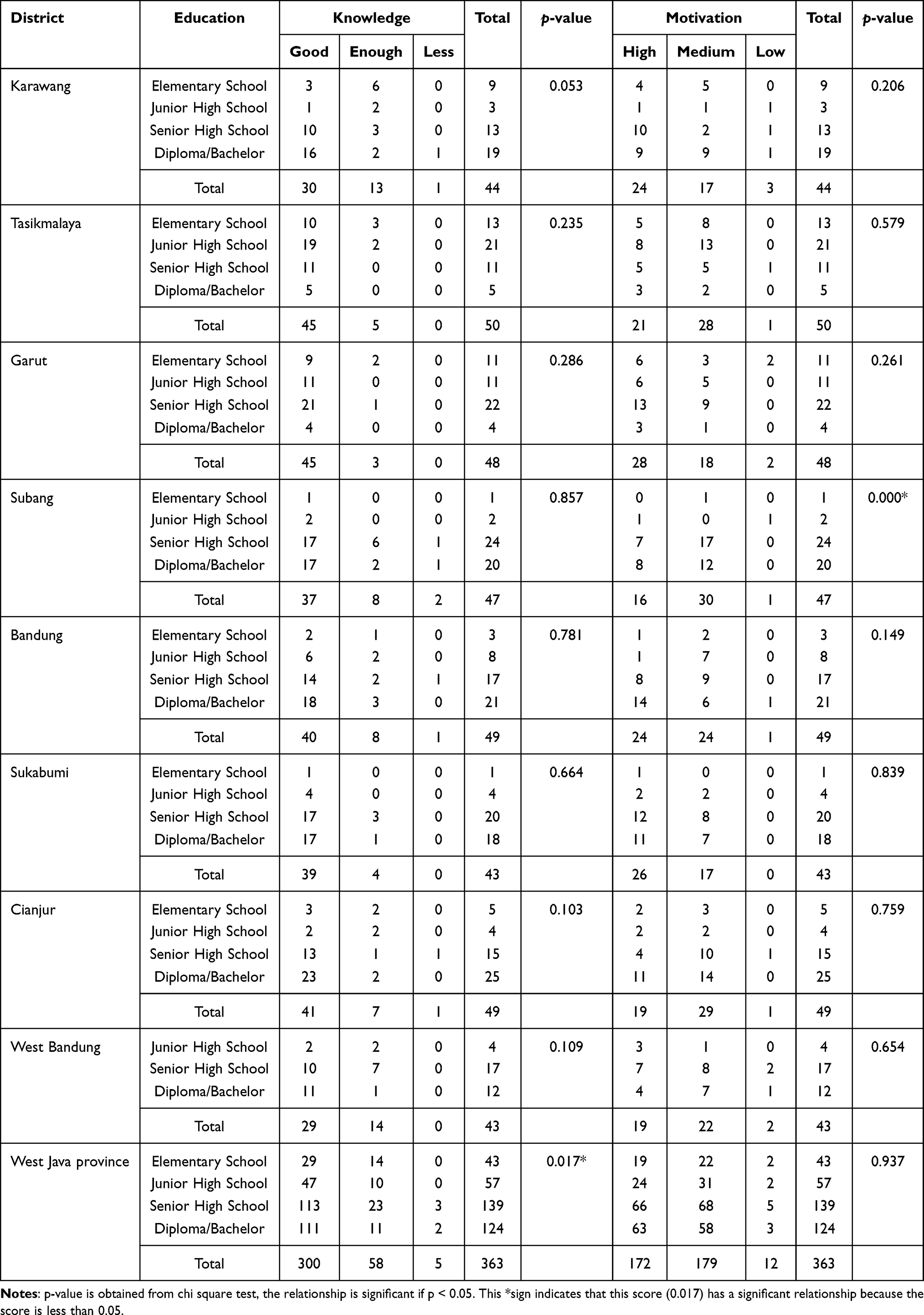 |
Table 4 Relationship of Knowledge and Motivation with Health Cadre Education in West Java (n=363) |
Relationship Between Knowledge and Motivation with Marital Status of Health Cadres in West Java
Based on the results in Table 5, there was no significant relationship between cadre knowledge and marital status in almost all districts/cities, as indicated by a probability value greater than an error rate of 0.05 or 5%. However, a significant relationship was found in Garut Regency with a p-value of 0.033 which is <0.05. There was also no significant relationship between motivation and marital status as indicated by a probability value greater than an error rate of 0.05 or 5%. Meanwhile, a significant relationship was found in Tasikmalaya Regency with a p-value of 0.000 <0.05, hence, it was concluded that the motivation of health cadres has a significant relationship with marital status, where high motivation tends to be associated with marital status, and low tends to be related to widow/widower status.
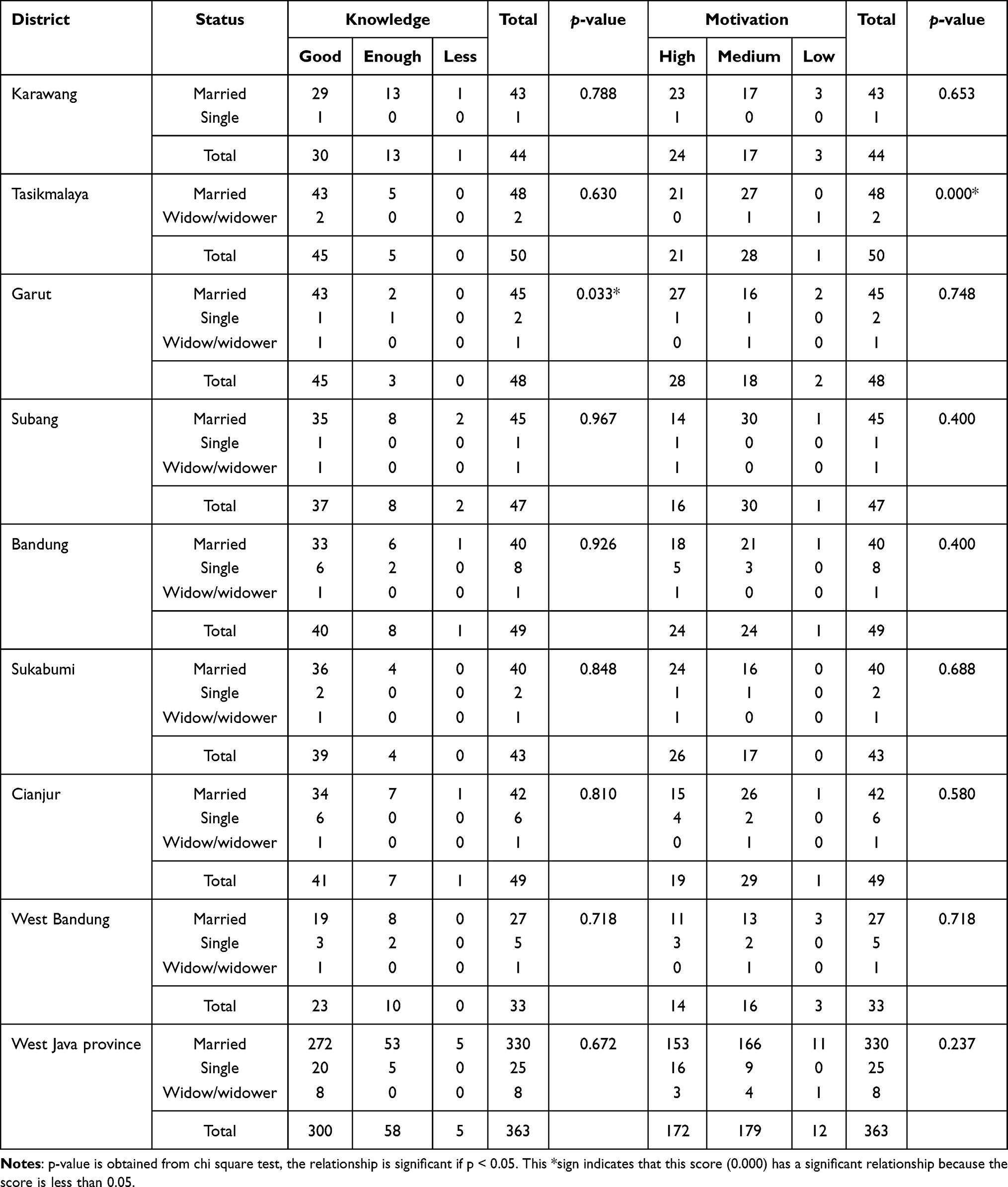 |
Table 5 Relationship of Knowledge and Motivation with Marital Status of Health Cadres in West Java (n=363) |
Relationship Between Knowledge and Motivation with Age of Health Cadre in West Java
Table 6 shows that there was no significant relationship between knowledge and the age of the cadres, both in each district/city and overall in West Java Province. There was also no significant relationship between motivation and age as indicated by a probability value greater than an error rate of 0.05 or 5% in all districts/cities studied. In contrast, there was a significant relationship in Subang Regency with p-value of 0.013 which is <0.05. It was concluded that cadre motivation has a significant relationship with age, where high motivation tends to be associated with relatively young age < 41 years, while low tends to be associated with old age namely >50 years.
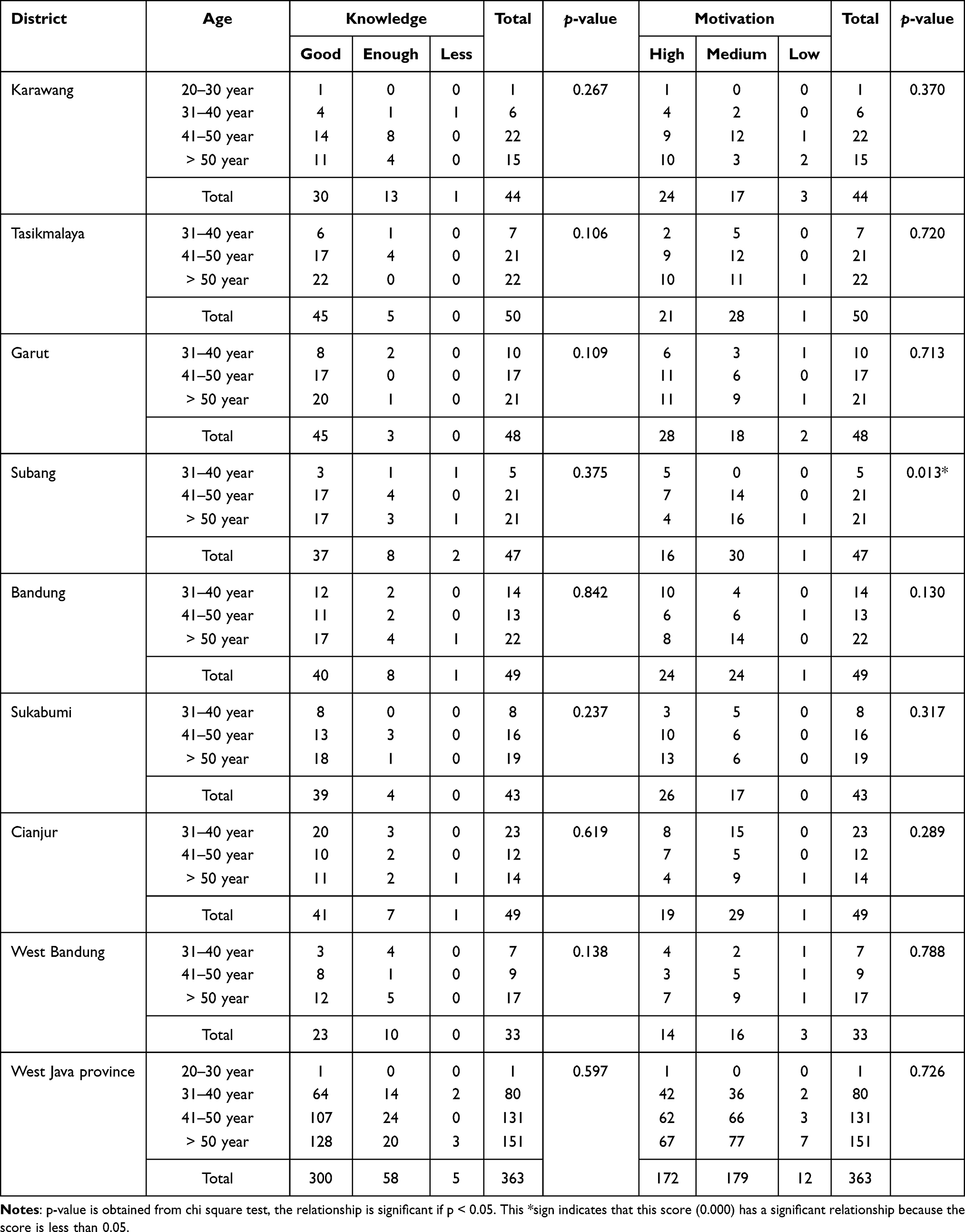 |
Table 6 Relationship of Knowledge and Motivation with Age of Health Cadre in West Java (n=363) |
Discussion
This study was conducted to identify the associations of sociodemographic characteristics with the knowledge and motivation of health cadres towards stunting prevention in West Java. There were no significant associations between occupation, education, marital status, and age with health cadre’s knowledge and motivation of stunting prevention.
Health cadres are community members involved by the public healthcare center for voluntary management. They are also the main pillar for improving the public health status, especially in the prevention of stunting. The results showed that the majority of health cadres have good knowledge as well as moderate to high motivation regarding stunting prevention efforts. This further is applicable as initial capital for the provision of health cadres to the community as part of the stunting prevention efforts. Furthermore, the data from the 8 districts/cities namely Karawang, Tasikmalaya, Garut, Bandung, Subang, Sukabumi, Cianjur, and West Bandung showed that the average age was 39 years and the majority have senior high school education/diplomas/graduates which tend to strengthen the role of health cadres. Based on the results, at a productive age supported by fairly high education, good knowledge, and high motivation, health cadres tend to carry out respective functions appropriately in collaboration with professional health workers in the work areas.
The knowledge on stunting and preventive measures is relatively good, possibly because the cadres have attended the training held in the district/city and are supported by health professionals such as midwives and public health center nurses. A study conducted in the public health center area of Bandung City found that health cadres attended stunting prevention training several times during the implementation of integrated healthcare centers and were always evaluated by the midwives and nurses. Cadres are also guided on how to find stunting cases in the community. Furthermore, a previous study found that a conducive support system with assistance from health workers tends to increase the knowledge of health cadres,30 while another study reported that training is an activity carried out to improve skills, knowledge, and attitudes for improved performance.31
A previous study reported that a person’s knowledge is influenced by age, education, occupation, sources of information, experience, social status, economy, culture, and the environment.32 This study indicates that there is a significant relationship between knowledge and education which indicates that good knowledge tends to be associated with fairly high to high education including Senior high school, Diploma/Bachelor, while sufficient tends to be associated with low education such as Elementary School. There was also a significant association between knowledge and marital status in Garut Regency with a p-value of 0.033 which is <0.05. The knowledge level is one of the factors that affect the performance of integrated healthcare centers, while notion is the first part of this level. Meanwhile, understanding generates knowledge, therefore, it constitutes a major part of the level.32
The results indicate that occupation and age have no significant effect on knowledge, this is not consistent with a previous study by Muthmainna which stated there is a significant relationship between occupation and knowledge.33 There was no relationship between the occupation and knowledge in relation to stunting prevention because the majority of health cadres do not work with sufficient knowledge. This is also possible because both health cadres with or without jobs have a similar experience and opportunity to obtain information, as well as participate in various training held by agencies or government for stunting prevention and control. This is in line with Wardani et al which stated that there is no significant relationship between work and knowledge of health cadres.34
The results are also not consistent with a previous study by Astuti which reported there is a relationship between age and knowledge level, as the respondents’ age ranged from 20–35 years.35 Meanwhile, the majority of respondents in this study were in the age group of > 35–50 years. This age range is associated with a good pattern of comprehension and thinking power, hence, the knowledge is also better32 as similarly stated by.34
The role of health cadres in relation to child nutrition problems, especially stunting, is to carry out early detection by weighing and measuring the length or height of children properly as well as regularly every month and record on the Health Monitoring Card (KMS) at integrated healthcare centers. Cadres also provide counseling to parents on the characteristics of stunting children as well as the preventive measures.36 Furthermore, they play an important role in conveying health information related to its dangers and impacts of stunting to reduce the risk in children under five years old in the community.
Improving the cognitive aspects of health cadres is very important, given that several studies reported that knowledge influences a person’s behavior.33,35 Knowledge is the outcome of understanding, and this occurs after people have sensed a certain object through the human senses, namely sight, hearing, smell, taste, and touch. The majority of human knowledge is obtained through the eyes and ears, while cognitive knowledge plays an important role in shaping overt behavior.32
Increased knowledge will change perceptions, habits, and beliefs,32 based on experience and several studies, a long-lasting behavior depends on knowledge, awareness, a positive attitude and vice versa.25,32,35 Therefore, increasing the cognitive aspect, in this case, the knowledge of health cadres is important to prevent stunting problems in the community.
External motivation is triggered from the outside, while the internal comes from an individual’s initiative. Motivation is a process of influencing or promoting a person or group to carry out a particular task, it is also a driving force or a natural urge to satisfy and sustain life.37
A person’s motivation is influenced by internal and external factors,38 the internal consists of inner desire, knowledge level, education, self-management, and age, while the external consists of family support, religion, and reinforcement/strength. Motivation is also influenced by needs, attitudes, and interests.39 Based on the results, there is a significant relationship with education, where high motivation tends to be associated with moderate to high education including Senior High School and Diploma/Bachelor, while low tends to be associated with relatively low education such as Junior High School. Additionally, there was a significant relationship with marital status, where high motivation tends to be associated with marital status, while low tends to be associated with the widow/widower status. This study also found a significant relationship with age, where high motivation tends to be associated with relatively young age < 41 years, while low tends to be associated with old age > 50 years. However, there is no significant relationship with occupation.
Motivation has a significant relationship with education which is related to knowledge, the higher the knowledge, the higher the motivation of health cadres in carrying out respective roles. Based on the results, the marital status in the form of husband/family support also increases motivation. Moreover, the majority of health cadres are in the age range of 36–50 years, hence, it was concluded that high motivation is associated with a relatively young age. This is supported by a previous study conducted by Haryani where awards, family support, environment, and knowledge were observed to influence the motivation of cadres in carrying out activities at Integrated Health Post.25
The roles of health cadres in community empowerment include health motivator, educator, and service provider.40 Meanwhile, community empowerment is formed from motivational factors to improve family and community health, the ability to identify needs and barriers to health services, as well as understand the available resources. Therefore, it was concluded that health cadres have an important role in improving health status, especially stunting prevention in the community. However, there are certain limitations in providing health services given that cadres are not health workers.
Health cadres’ efforts in preventing stunting among children include activities at the integrated health center or home visits. Meanwhile, age, attitude, motivation, knowledge, years of service, incentives, and training are factors that affect the performance of health cadres.41 Profita stated that knowledge, motivation, and support from various parties are needed to encourage activeness among health cadres in the Integrated Health Post.42 In addition, continuous coaching and reward increase their active participation.
To achieve the optimal stunting reduction target, health cadres need to improve respective roles and functions to empower families and communities in West Java. Moreover, healthcare providers such as nurses and midwives are recommended to review and design appropriate intervention strategies, particularly in children under five. This is expected to enhance the Healthy Indonesia program at the sub-district and district levels. Meanwhile, to empower family functions in preventing stunting and improving the life quality, parents and families need to provide adequate nutrition for the children and maintain good environmental sanitation. Furthermore, health cadres need to improve respective roles and functions to empower families and communities as well as to prevent and detect stunting in West Java.
This study did not explore how various factors including demographics, self-efficacy, and length of time, influence the actual performance of health cadres in stunting prevention efforts. Another aspect that needs to be studied in the future is the experience of cadres in stunting prevention efforts as well as the inhibiting and supporting factors in the community.
Conclusion
The results showed that the majority of health cadres respondents have good knowledge of stunting prevention efforts in each district/city of West Java Province. This is influenced by the education level and marital status, while occupation and age had no significant effect. Furthermore, the majority of the health cadres had high and moderate motivation which is influenced by education level, marital status, and age, while occupation had no significant effect.
These results are applicable as initial capital for the provision of health cadres to the community in preventing stunting. Furthermore, the average age of the respondents was 39 years and the majority have a fairly high level of education which strengthens their roles. At a productive age supported by higher education, good knowledge, and high motivation, health cadres effectively carry out respective functions in improving the health status of children through collaboration with healthcare professionals at integrated healthcare centers.
The study provides a basis for further studies to develop an integrated model of prevention and treatment of stunting in children based on community empowerment in West Java Province.
Acknowledgments
The authors are grateful to the participants of this study who had spent their time volunteering.
Funding
This study was funded by the Ministry of Education, Culture, Research, and Technology Republic of Indonesia under PTUPT Research Grant with the number: 1427/UN6.3.1/LT/2020.
Disclosure
The authors declare that there is no conflict of interest.
References
1. World Health Organization. Reducing stunting in children: equity considerations for achieving the Global Nutrition Targets 2025; 2018. Available from https://www.who.int/publication-detail-redirect/9789241513647
2. Ministry of Health Republic of Indonesia. Pusat data dan informasi Kementerian Kesehatan RI. Jakarta: Ministry of Health Republic of Indonesia; 2017.Available from https://pusdatin.kemkes.go.id/
3. World Health Organization. Prevalence of stunting. Geneva; 2019. Available from https://apps.who.int/iris/rest/bitstreams/1269729/retrieve
4. UNICEF/WHO/World Bank Group. Levels and trends in child malnutrition 2018. Joint Child Malnutrition Estimates 2018 Edition; 2018: 1–15.
5. Indonesian Ministry of Health. Decree of the Minister of Health of the Republic of Indonesia Number1995/Menkes/SK/XII/2010 Concerning Anthropometric Standards for Assessment of Child Nutritional StatusT. Jakarta: World Health Organization; 2011.
6. Okoh M. Socio-demographic correlates of overweight and obesity among women of reproductive age in Nigeria. Afr J Reprod Heal. 2013;17(4):66–76.
7. Rachmi CN, Agho KE, Li M, Baur LA. Stunting, underweight and overweight in children aged 2.0–4.9 years in Indonesia: prevalence trends and associated risk factors. PLoS One. 2016;11(5):1–17. doi:10.1371/journal.pone.0154756
8. Ministry of Health Republic of Indonesia. Basic health research [Riskesdas] [Internet]. Jakarta; 2018. Available from: http://wwwdepkesgoid/resources/download/info-terkini/materi_rakorpop_2018/Hasil20Riskesdas202018pdf.
9. West Java Regional Development Planning Agency. Prevent Stunting, West Java will hold a 2023 zero stunting campaign [Internet]; 2018. Available from: http://bappeda.jabarprov.go.id/cegah-stunting-jabar-akan-gelar-kampanye-zero-stunting-2023/.
10. Mediani HS. Predictors of stunting among children under five year of age in Indonesia: a scoping review. Glob J Health Sci. 2020;12(8):83. doi:10.5539/gjhs.v12n8p83
11. Bloem MW, de Pee S, Hop LT, et al. Key strategies to further reduce stunting in Southeast Asia: lessons from the ASEAN countries workshop. Food Nutr Bull. 2013;34(2 Suppl):8–16. doi:10.1177/15648265130342S103
12. Anugraheni HS, Kartasurya MI, Risk Factors for Stunting in Children Age 12-36 Months in Pati District, Pati Regency. J Nutr Coll. 2012;1(1):30–37. doi:10.14710/jnc.v1i1.725
13. Ministry of Health of the Republic of Indonesia. Prevent stunting, that’s important. Jakarta; 2019.
14. Purwandini K, Kartasurya MI, Effect of micronutrient sprinkle on the motor development of stunted children aged 12-36 months. J Nutr Coll. 2013;2(1):50–59. doi:10.14710/jnc.v2i1.2098
15. Crookston BT, Penny ME, Alder SC, et al. Children who recover from early stunting and children who are not stunted demonstrate similar levels of cognition. J Nutr. 2010;140(11):1996–2001. doi:10.3945/jn.109.118927
16. Aguayo M, Menon P. Introduction stop stunting: improving child feeding, women’s nutrition and household sanitation in South Asia. Matern Child Nutr. 2016;12(1):3–11. doi:10.1111/mcn.12283
17. Sutarto ST, Mayasari D, Indriyani R. Stunting, Risk Factors and Prevention. J Agromed. 2018;5(1):540–545.
18. Dewey KG, Begum K. Long-term consequences of stunting in early life. Matern Child Nutr. 2011;7(SUPPL. 3):5–18. doi:10.1111/j.1740-8709.2011.00349.x
19. Hossain M, Choudhury N, Abdullah KAB, et al. Evidence-based approaches to childhood stunting in low and middle income countries: a systematic review. Arch Dis Child. 2017;102(10):903–909. doi:10.1136/archdischild-2016-311050
20. Maywita E. Risk factors cause the stunting of age 12–59 Months in Kampung Baru Kec. Lubuk Begalung in 2015. J Ris Hesti Medan Akper Kesdam I/BB Medan. 2018;3(1):56. doi:10.34008/jurhesti.v3i1.24
21. Umeta M, West CE, Verhoef H, Haidar J, Hautvast JGAJ. Factors associated with stunting in infants aged 5–11 months in the Dodota-Sire District, Rural Ethiopia. J Nutr. 2003;133(4):1064–1069. doi:10.1093/jn/133.4.1064
22. Victora CG, Adair L, Fall C, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–357. doi:10.1016/S0140-6736(07)61692-4
23. Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M. Maternal and child undernutrition and overweight in low-income and middle-income countries. Matern Child Nutr. 2013;382(9890):427–451.doi:10.1016/S0140-6736(13)60937-X
24. Darteh EK, Acquah E, Kyereme AK. Correlates of stunting among children in Ghana. J BMC Public Health. 2014;14:504. doi:10.1186/1471-2458-14-504
25. Haryani D. Analysis of factors that influence the motivation of cadres in implementing the Posyandu for elderly in Ledug Village, Banyumas Regency in 2014 A. Universitas Muhammadiyah Purwokerto; 2014. Available from https://repository.ump.ac.id
26. Agustin A, Rakhmawati W, Nurlita L. Knowledge of Cadres at Posyandu in Cipacing Village on Toddler Development. Student e- Journal. 2012;1(1):169–172. Available from https//jurnal.unpad.ac.id/ejournal/
27. Adistie F, Maryam NNA, Lumbantobing VBM. Knowledge of Health Cadres About Early Detection of Malnutrition in Toddlers. J Apl Ipteks Untuk Masy. 2017;6(3):173–177. Available from https//jurnal.unpad.ac.id/dharmakarya/article
28. Sastroasmoro S, Ismael S. Fundamentals of Clinical Research Methodology. D
29. Creswell JW. Qualitative Inquiry & Research Design: Choosing Among Five Approaches.
30. Singh A, Upadhyay AK, Kumar K. Birth size, stunting and recovery from stunting in Andhra Pradesh, India: evidence from the young lives study. Matern Child Health J. 2016;21:21.
31. Permatasari ED, Nurika G, Damayanti NA. Capacity building in health worker as an alternative solution to solve stunting problem. Indian J Public Heal Res Dev. 2019;10(8):1409–1414. doi:10.5958/0976-5506.2019.02095.3
32. Notoatmodjo S. Behavioral Health Science. Jakarta: Rineka Cita; 2014.
33. Muthmainnah F. Factors related to mother's knowledge in providing complementary foods for breast milk at Pamulang Health Centre in 2010. Syarif Hidayatullah State Islamic University; 2010.Available from https://repository.uinjkt.ac.id
34. Wardani NI, Sarwani D, Masfiah S. Factors related with level of health volunteers knowledge about thalassaemia in sumbang district Banyumas regency. J Kesmasindo. 2014;6(3):194–206. Available from https://jos.unsoed.ac.id/index.php/kesmasindo
35. Astuti HP. The relationship between the characteristic of pregnant women and the level of knowledge about danger signs in pregnant in Sidoharjo Community Health Centre. Sragen Regency. J Kesehat Kusuma Husada. 2011.
36. Astuti S. Stunting Prevention Movement Through Community Empowerment in Jatinangor Distric, Sumedang Regency. Dharmakarya. 2018;7(3):185–188. Available from https://jurnal.unpad.ac.id/dharmakarya/article
37. Samsudin S. Human Resource Management. Bandung: Pustaka Setia; 2005.
38. Handoko TH. Personnel and human resource management. . Yogyakarta: BPFE; 2012. Available from https://lib.ui.ac.id
39. Purwanto N. Educational psychology Bandung: Remaja Rosdakarya; 2010. Available from htpps//repository
40. Susanto F, Claramita M, Handayani S. Role of posyandu cadres in empowering the community of Bintan. Ber Kedokt Masy. 2017;33(1):13. doi:10.22146/bkm.11911
41. Andira RA, Abdullah AZ, Sidik D. Factors associated with cadres performance in the posyandu activities in district bontobahari bulukumba in 2012. Hasanuddin Univ Repos. 2012;4:1–13.
42. Profita AC. Factors associated with the activeness of cadres in maternal and baby clinic of pengadegan Village Banyumas District. J Adm Kesehat Indones. 2018;6(2):68. Available from https://doi.org/10.20473/jkt.v62.218.68-74
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.