")
Back to Journals » Patient Preference and Adherence » Volume 10
Factors affecting medication adherence in elderly people
Authors Jin HK, Kim YH, Rhie SJ
Received 26 July 2016
Accepted for publication 14 September 2016
Published 19 October 2016 Volume 2016:10 Pages 2117—2125
DOI https://doi.org/10.2147/PPA.S118121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hyekyung Jin,1 Yeonhee Kim,2 Sandy Jeong Rhie1,3
1College of Pharmacy, 2Center for Excellence in Teaching & Learning, 3Division of Life and Pharmaceutical Sciences, Ewha Womans University, Seoul, Republic of Korea
Background: Little is known about the functional health literacy (FHL) associated with medication adherence in elderly patients. The aim of this study was to examine the FHL among older adults and identify influencing factors that can predict medication adherence.
Methods: This was a cross-sectional survey. Participants (n=160) aged 65 years and older were selected from outpatient clinics of 3 tertiary care hospitals, 6 community pharmacies, and 2 senior centers between November 1 and 30, 2014. The participants’ FHL was measured using the Korean Functional Health Literacy Test, which consists of 15 items including 8 numeracy and 7 reading comprehension items. Medication adherence was measured by the Adherence to Refills and Medication Scale. Descriptive statistics, chi-square or Fisher’s exact test, and multiple regression analyses were used to analyze the data.
Results: The mean score of the total FHL was 7.72±3.51 (range 0–15). The percentage of the total number of correct answers for the reading comprehension subtest and numeracy subtest were 48.1% and 54.4%, respectively. Among 160 participants, 52.5% showed low adherence to medication. The factors affecting medication adherence included the patient’s degree of satisfaction with the service (β=-0.215, P=0.022), sufficient explanation of medication counseling (β=-0.335, P=0.000), education level (β=-0.153, P=0.045), health-related problems (β=-0.239, P=0.004), and dosing frequency (β=0.189, P=0.018).
Conclusion: In this study, we found medication adherence of elderly patients was associated with education level, health-related problems, dosing frequency, satisfaction with patient counseling, and explanation of medication, but no association was found with FHL. Pharmacists should consider elderly patients’ individual characteristics such as educational background and specific patient-related health problems, provide sufficient information and explanation of medication, and ensure patient satisfaction with the counseling.
Keywords: ARMS, elderly, health literacy, medication adherence
Introduction
The number of elderly Korean patients aged 65 years and over continues to increase at unprecedented rates, and they comprised 13.1% (6.62 million people) of the total population of South Korea in 2015.1 Approximately 90% of older adults suffer from more than one chronic condition, and over 69.7% of those aged 65 years and older have multiple chronic diseases, which may result in complexity in the medication regimen.2 Also, among patients who are aged 65 years and above, 82.0% take more than one prescribed medication and 60.3% of these patients have prescriptions that contain three or more medications.2 It is a growing concern that these elderly people are the major consumers of medication in Korean society. Although appropriate drug therapy can contribute to alleviating symptoms and reduction of morbidity and mortality rates, the use of medications can also be a burden on health care costs, risk of side effects, and noncompliance in the elderly patients.3,4
According to the recent literature, there are various risk factors associated with nonadherence in the elderly. These include patient factors (eg, old age, male gender, low education level, physical and mental status, and health literacy [HL]), medication factors (eg, complexity of medication regimen, high medication costs, and poor labeling instructions), patient–provider relationship factors (dissatisfaction with health care providers, lack of trust, and lack of patient involvement), and health care system factors (eg, inability or difficulty in accessing pharmacy, lack of follow-up, and poor treatment by untrained staff).5,6 In particular, the relationship between HL and medication adherence among patient characteristics is an emerging clinical concept in pharmacy in Korea.
HL is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decision”.7 Early studies have indicated that patients with limited HL have more problems with understanding the indications for use and instructions.8,9 Therefore, it may contribute to medication errors or adverse drug events, which lead to medication nonadherence, increased hospitalizations, readmissions, and avoidable health care costs.10,11 However, recent studies have shown an inconsistent or contradictory relationship between HL and medication adherence.12–14
In Korea, remarkably little is known about elderly people’s HL and its relationship with medication adherence. The aim of this study was to assess the status of HL among 65- to 83-year-olds and to explore whether HL, among other factors, influences medication adherence.
Methods
Study design and participants
A cross-sectional questionnaire survey was conducted. One hundred and sixty participants were recruited for this study using the convenience sampling method from individuals visiting outpatient clinics of 3 tertiary care hospitals, 6 community pharmacies, and 2 senior centers between November 1 and November 30, 2014, in Seoul and Gyeonggi Province, which is in the vicinity of Seoul and located in the mid-western part of Korea. The selected 3 hospitals, 6 pharmacies, and 2 senior centers were located in an area having the largest proportion of people aged 65 years and older. Therefore, the sample increases the likelihood that the results are representative of the local area in the mid-western part of Korea. The inclusion criteria were people who were aged 65 years and above, were able to fill out the questionnaire, did not exhibit severe cognitive impairment and had not been diagnosed with dementia, and who consented. The exclusion criteria were individuals who had severe visual impairment, poor hearing, or were too ill to participate. A pilot study was conducted with a single pharmacy with 30 outpatients who were not included in the final study sample.
Ethical considerations
This study was approved by the Institutional Review Board (IRB) of Ewha Womans University (IRB number 82-1). We obtained written informed consent from all the participants before conducting the survey, and anonymity and confidentiality of responses were ensured.
Questionnaires
Study variables
The demographic information collected in the questionnaire included age, gender, marital status, level of education, monthly allowance, health-related problems, number of self-reported chronic diseases, chronic conditions, number of prescription drugs currently taken, frequency of doses, HL level, and Adherence to Refills and Medications Scale (ARMS) scores. The variables of adherence included patient factors (7 items: age, gender, education level, health-related problems, number of self-reported chronic diseases, expectancy of treatment, and HL level), medication factors (3 items: number of prescription drugs currently taken, pharmacy use patterns, and cost-related nonadherence), and health care provider factors (3 items: patient’s satisfaction with pharmacist’s patient counseling, patient–pharmacist relationship and communication, and explanation of medication). For patient factors, expectancy of treatment was assessed on a 3-point Likert scale: negative/neutral/positive. For medication factors, cost-related nonadherence was assessed by yes or no questions. For health care provider factors, satisfaction with patient counseling and patient–pharmacist relationship and communication were measured by a 3-point scale each: dissatisfaction/neutral/satisfaction, and poor/neutral/good, respectively. In addition, explanation of medication was measured on a 3-point scale: none/a little/enough.
Functional HL test
The participants’ functional HL (FHL) was measured using the Korean Functional Health Literacy Test (KFHLT).15 It was developed based on the Test of Functional Health Literacy in Adults (TOFHLA)16 and the US Department of Education.17 The KFHLT consists of two main parts: 1) eight items of the numeracy section and 2) seven items of the reading comprehension section; these items have total scores in a range of 0–15, with higher scores indicating better literacy. The correct response for each question in the reading and numeracy sections earns one point, and incorrect responses do not earn any points. The cutoff for appropriate HL is six or more correct answers. The KFHLT requires approximately 20 minutes to complete.
Measurement of medication adherence
The participants’ medication adherence was measured using ARMS, which was developed by Kripalani et al.18 The scale is known to be valid and reliable for minority populations in health care and patients with chronic disease or limited HL skills.18 The ARMS was translated into Korean and reverse translated to confirm its consistency with its original language and to reflect the Korean public health system. The ARMS was designed to include a twelve-item questionnaire consisting of the following two parts:18 1) eight items related to the medication taking subscale to assess the degree to which patients took their prescribed medication as directed; 2) four items related to the prescription refill subscale to assess the refill adherence.18 Each item was rated using a four-point Likert scale, ranging from 1 (none of the time) to 4 (all of the time). The overall adherence score may range from 12 to 48, with lower scores indicating better adherence.
Statistical analysis
The data were analyzed using the SPSS 21.0 statistical package (IBM Corporation, Armonk, NY, USA). The internal consistency reliability of the KFHLT was estimated by computing Cronbach’s α. The total ARMS score was dichotomized based on the median score using a cutoff value of 20 (low adherence ≥20 and high adherence <20). That is, in this study, the designated high adherence and low adherence are relative terms. Descriptive statistics for each variable were calculated as the percentage, mean ± standard deviation, and median. A chi-square or Fisher’s exact test was conducted to examine differences in subject characteristics by adherence level. We performed a multiple regression analysis to identify factors that affect the medication adherence. We considered the medication adherence score as a dependent variable, which is a continuous variable ranging from 12 to 48, and the significant variables among participants’ characteristics and the variables of adherence level were taken as independent variables. Although age and HL did not have a significant relationship with adherence in univariate analysis, we included them in our regression. Because both are known to be potentially related to the medication adherence among elderly people from previously literature, we sought to determine whether these variables could predict adherence. In all analyses, a 2-sided P-value <0.05 was considered to be statistically significant.
Results
General characteristics of participants
The participants’ characteristics are shown in Table 1. A total of 172 older adults were approached, and the 160 who consented were given the questionnaire (93.02%). The study participants were 70.0% female and had a mean age of 67.9 years, and 81.3% were married or cohabitating with someone. Approximately 67.0% of the participants had completed high school or a higher level of education. The mean monthly allowance was US$524. Approximately four out of five elderly people (81.3%) in this study had health-related problems, and the top five self-reported chronic conditions were hypertension (42.5%), hypercholesterolemia (27.5%), diabetes (20.0%), cardiovascular disease (6.3%), and bone fracture/osteoporosis (5.6%). The majority of participants (83.8%) were taking at least one prescription medication, and the most common dosing frequency was once daily (43.8%). Overall, 27.5% of participants (n=44) had inadequate HL and 72.5% (n=116) had adequate HL skills. The ARMS scores categorized participants into poor adherence (n=84; 52.5%) and good adherence (n=76; 47.5%).
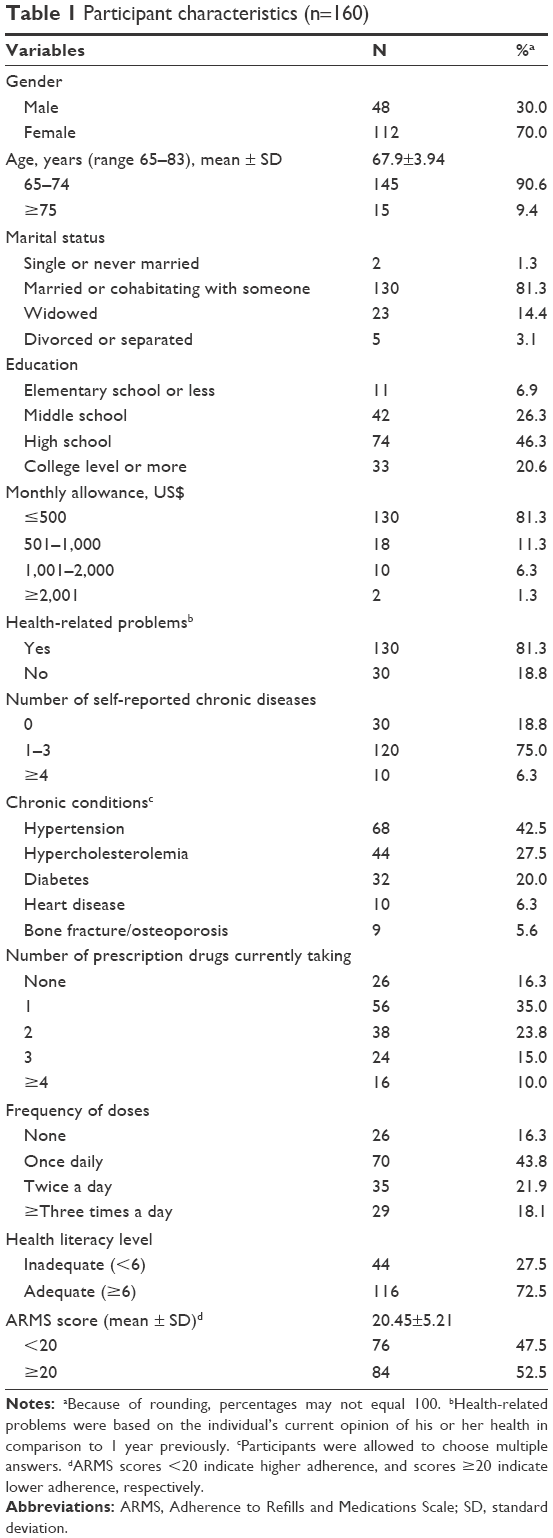 | Table 1 Participant characteristics (n=160) |
Proportion of participants correctly answering FHL test items
Table 2 presents the participants’ FHL. The mean KFHLT score was 7.72±3.51 (range: 0–15). Overall, the percentage of correct answers was 51.3%. The total average percentage of correct answers for the numeracy subtest and the reading comprehension subtest was 54.4% and 48.1%, respectively. Interestingly, only 14.4% of participants correctly answered the question regarding the last administration time for the four times-a-day dosing schedule. Furthermore, less than half of the participants were aware of the informed consent documentation, and only 12.5% of participants noticed the presence of the “procedure complications” section in the informed consent document. The instrument is reliable and has demonstrated internal consistency in a previous study (Cronbach’s α=0.796).15 In this study, the Cronbach’s α for the full 15-item scale was 0.821, which demonstrated good internal reliability (numeracy: Cronbach’s α=0.731; reading comprehension: Cronbach’s α=0.723).
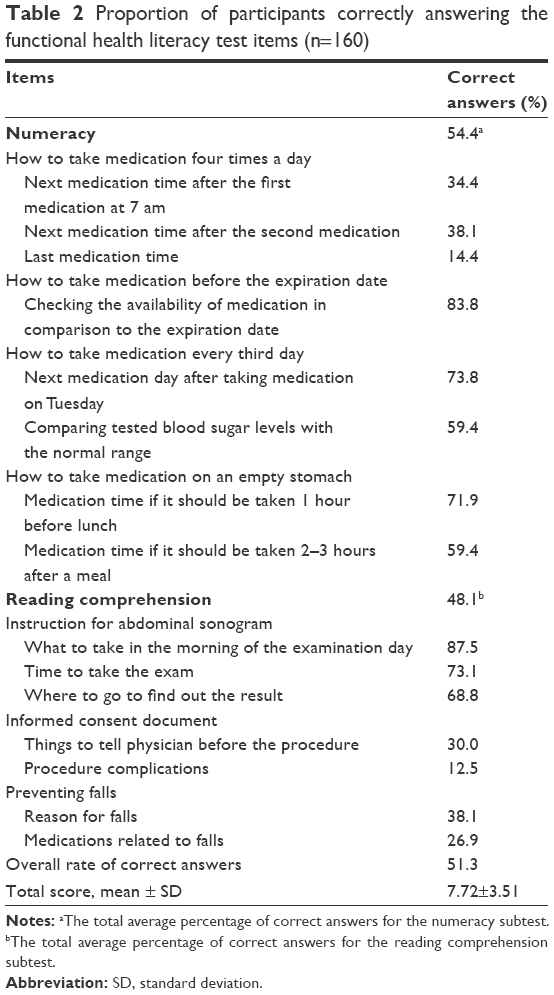 | Table 2 Proportion of participants correctly answering the functional health literacy test items (n=160) |
Patient factors, medication factors, and health care provider factors by medication adherence level
The prevalence of lower adherence was 52.5% (ARMS scores of ≥20). Compared to those with high adherence, participants with lower adherence were more frequently male, had not completed high school, had health-related problems, had fewer self-reported chronic diseases, had negative expectancy of treatment, had lower level of HL, reported more use of multiple pharmacies, had cost-related nonadherence, and ≥3 were currently taking a prescription drug, but these differences were not significant except expectancy of treatment. Also, participants with low adherence were less likely to be satisfied with a pharmacist’s patient counseling, received sufficient explanation of medication at a lower rate, and had a poorer or neutral patient–pharmacist relationship and communication, and these differences were statistically significant (P<0.05) (Table 3).
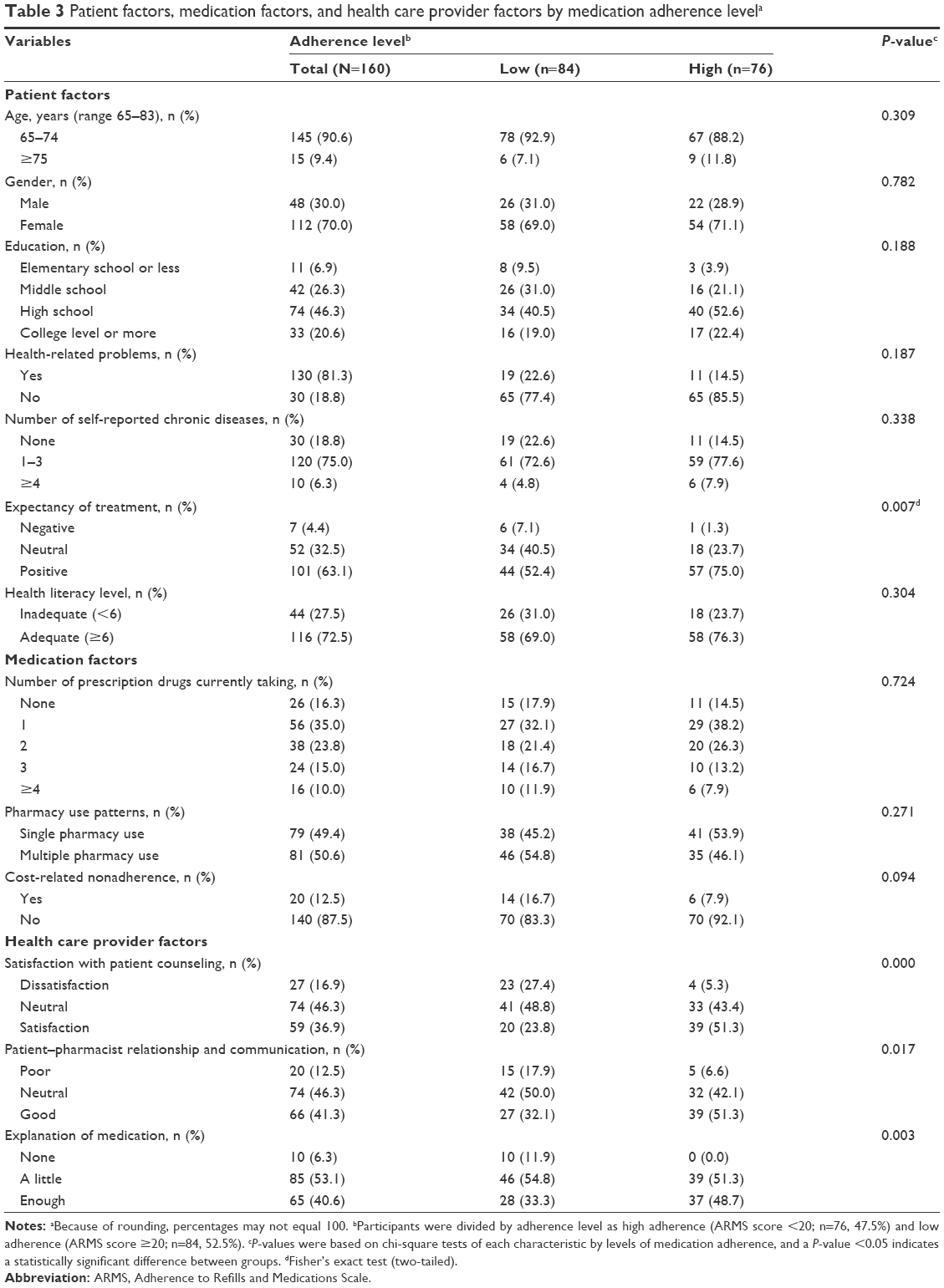 | Table 3 Patient factors, medication factors, and health care provider factors by medication adherence levela |
Influencing factors on medication adherence
We conducted multiple regression analyses using various factors as the independent variables and medication adherence as the dependent variable (Table 4). The four variables based on the patient factors (eg, age, level of education, health-related problems, and HL), the one variable based on the medication factors (eg, dosing frequency), and the three variables based on health care provider factors (eg, patient satisfaction, patient–pharmacist relationship and communication, and pharmacist’s explanation of medications) were entered simultaneously into the regression equation to predict the medication adherence. The results indicated that five of the variables were significantly associated with adherence. In particular, providing sufficient explanation and consultation about medication was the strongest predictor of adherence (β=−0.335, P=0.000). Furthermore, the participant’s satisfaction with counseling was also a strong predictor of adherence (β=−0.215, P=0.022). This analysis demonstrated that eight variables accounted for approximately 31% of the variance in adherence. In this study, age, HL, and patient–pharmacist relationship and communication did not have a significant influence on medication compliance.
 | Table 4 Factors influencing medication adherencea |
Discussion
This study examined the FHL of the elderly and the factors associated with medication adherence. The overall rate of correct answers on the KFHLT was 51.3%. In particular, elderly Koreans achieved the lowest score for items related to taking doses in the numeracy subtest (14.4%–38.1%) compared with the score of elderly Americans (78.0%).19 It is important to note that the elderly struggled with basic tasks, simple interpretations, and calculations of numbers. In addition, only 59.4% of answers were correct on interpreting blood sugar tests, which is lower than the result (74.7%) reported by Kim and Lee.20 The results demonstrated that many older adults had difficulty understanding health information and simple prescription instructions.
Only 12.5%–30.0% of the subjects in this study understood an informed consent document, and 26.9%–38.1% understood the information on preventing falls. An estimated 60% of elderly people in this study had difficulties in understanding the written information provided to them. Many of the elderly people reported that, in their daily lives, they were generally given counseling materials and informed consent documents that contained complex concepts, which exceeded their literacy abilities.21 Therefore, pharmacists should consider concise written information, appropriate levels of messages with familiar words, adherence monitoring or feedback, using pictorial aids, and audiovisual, oral, or written education.10,22 That is, patient counseling including combinations of behavioral and educational approach is necessary.22 A majority of studies showed that comprehension of drug information and adherence is lower in adults >75 years of age than those aged 66–74 years.23,24 Similarly, Barat et al25 demonstrated that only 21% of participants aged 75 years understood the consequences of nonadherence. The study also revealed that elderly people who knew about common side effects or all possible medication interactions amounted to less than 6%.25 Thus, pharmacists should emphasize the effects of adherence, adverse effects, and precautions repeatedly during the elderly patient counseling.
In this study, patient satisfaction, a detailed explanation of medication, patient–pharmacist relationship and communication, and expectancy of treatment had statistically significant differences in each characteristic by level of adherence. In this study, participants with lower adherence were more likely to use multiple pharmacies, and consistent with previous studies, using multiple pharmacies had higher likelihood of nonadherence and increased risks of potential drug–drug interactions compared to using only a single pharmacy.26,27 However, we found no statistically significant differences between pharmacy use patterns and adherence level.
Recently, several studies have demonstrated that developing trusting relationships and effective communication between health care providers and patients can improve older patients’ adherence to medications.3,28,29 Previous studies indicated that pharmacists were a highly trusted source of drug-related information, and a good relationship and proper counseling between patient and health care providers can affect adherence levels.30–32 Therefore, a better understanding of the patient–pharmacist relationship and communication factors may lead to improved medication adherence.
According to one study, an estimated one quarter of the elderly patients took less medication in order to avoid cost burdens.33 In particular, older adults with chronic conditions are more likely to experience financial difficulties.4,34 In this study, participants with lower adherence reported more cost-related nonadherence compared to the higher adherence group, but this difference was not significant (16.7% vs 7.9%; P=0.094).
In the multiple regression analyses, elderly patients were found to be more likely to adhere to a medication if they were highly educated, had diseases, were more satisfied with counseling, had received sufficient explanation of their medication, and were subject to lower frequency of dosing. These results are congruent with the findings of earlier studies that indicated that medication adherence and patients’ satisfaction increase when pharmacists provide ample instructions regarding taking medication.35,36 The participants noted that patient counseling might increase knowledge and skills for taking medication correctly;36 however, many participants complained that most pharmacists did not always fully explain the expected treatment outcomes and possible side effects or how to use medications properly.37,38 As a result, the majority of respondents were unaware of the potential side effects and consequences of taking medications incorrectly. Elderly patients have specific age-related problems for nonadherence, for example, physical inability (eg, poor eyesight or low manual dexterity) or psychosocial factors (eg, cognitive incapacity).39 Therefore, pharmacists should keep in mind the various risk factors in elderly patients.
In the present study, frequency of dosing was inversely related to medication adherence. This result was similar to that of a previous study, which showed that a more frequent dosing schedule was associated with a negative effect on adherence.40 In general, older adults would be more adherent to a simplified medication regimen (eg, once-daily regimens as compared to twice-daily regimens, monotherapy regimens as compared to polytherapy regimens), which can lead to effective medication management. In this study, patient–pharmacist relationship and communication did not have a significant effect on adherence. To our knowledge, this happens because, considering all other variables, the effect of the predictor declined, although there was a previously significant difference by adherence level.
In this study, HL was not found to be a predictor of adherence. Nevertheless, this finding is similar to the results of other studies, which support our observations.13,41,42 Mosher et al41 showed that low HL patients have less medication knowledge, but this does not imply poor adherence to medication or increased risk of adverse outcomes. However, based on multiregression analyses in the present study, having information on the patients’ educational background and specific patient-related information would be helpful for pharmaceutical care. Thus, to enhance patient adherence, the pharmacist should give special attention to elderly patients with low levels of education and should provide tailored professional advice to offer understandable information regarding medications.
Limitations
This study had several limitations. First, the study data were only collected from the mid-western metropolitan area, which may not be generalizable to the rural and lower income elderly in Korea, and it had a limited number of participants. Second, the medication adherence was measured through self-reporting, which is liable to recall bias and social desirability response bias. Nonetheless, the present approach is uncomplicated, inexpensive, and can feasibly be applied in various clinical settings. Third, future research is necessary to consider other variables associated with adherence, such as ethnicity or health beliefs (eg, belief in self-efficacy for taking medication, belief in control over one’s health). Finally, our study included people aged 65–83 years. Future studies should investigate adherence according to different age groups, such as young-old (65–74 years), middle-old (75–84 years), and oldest-old (≥85 years).
Conclusion
The findings of this study demonstrate that HL is not associated with medication adherence, but pharmacists should consider older adults’ educational background and specific patient-related health problems. The results of this study indicate that full explanation of medication management by pharmacists and patients’ satisfaction of patient counseling influence medication adherence in the elderly. Moreover, the development of pharmacist communication skills for patient-centered pharmaceutical care should focus on establishing a rapport with older patients, which can lead to improvement in patients’ adherence to medical treatment. In this light, pharmacists should consider multifaceted and customized strategies to enhance medication adherence.
Disclosure
The authors report no conflicts of interest in this work.
References
Statistics Korea. Statistics on Elderly People 2015. Available from: http://kostat.go.kr/portal/korea/kor_nw/2/1/index.board?bmode=read&aSeq=348565/. Accessed January 30, 2016. | ||
Ministry of Health and Welfare. The Status of Older Koreans 2014. Available from: http://www.mohw.go.kr/front_new/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=0328&CONT_SEQ=318518&page=1/. Accessed August 11, 2016. | ||
Holt E, Joyce C, Dornelles A, et al. Sex differences in barriers to antihypertensive medication adherence: findings from the cohort study of medication adherence among older adults. J Am Geriatr Soc. 2013;61(4):558–564. | ||
Piette JD, Heisler M, Wagner TH. Cost-related medication underuse among chronically ill adults: the treatments people forgo, how often, and who is at risk. Am J Public Health. 2004;94(10):1782–1787. | ||
Osterberg L, Blaschke T. Drug therapy – adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003. | ||
Institute of Medicine. Health literacy: a prescription to end confusion. In: Nielsen-Bohlman L, Panzer A, Kindig DA, editors. Washington, DC: The National Academies press; 2004. | ||
Pignone M, DeWalt DA, Sheridan S, et al. Interventions to improve health outcomes for patients with low literacy. J Gen Intern Med. 2005;20(2):185–192. | ||
Kalichman SC, Ramachandran B, Catz S. Adherence to combination antiretroviral therapies in HIV patients of low health literacy. J Gen Intern Med. 1999;14(5):267–273. | ||
Davis TC, Wolf MS, Bass PF III, et al. Low literacy impairs comprehension of prescription drug warning labels. J Gen Intern Med. 2006;21(8):847–851. | ||
Baker DW, Gazmararian JA, Williams MV, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–1283. | ||
Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. | ||
Loke YK, Hinz I, Wang X, et al. Systematic review of consistency between adherence to cardiovascular or diabetes medication and health literacy in older adults. Ann Pharmacother. 2012;46(6):863–872. | ||
Noureldin M, Plake KS, Morrow DG, et al. Effect of health literacy on drug adherence in patients with heart failure. Pharmacotheraphy. 2012;32(9):819–826. | ||
Park JY, June KJ. Influencing factors on functional health literacy among the rural elderly. J Korean Acad Community Health Nurs. 2011;22(1):75–85. | ||
Parker RM, Baker DW, Williams MV, et al. The test of functional health literacy in adults: a new instrument for measuring patients’ literacy skills. J Gen Intern Med. 1995;10(10):537–541. | ||
U.S. Department of Education. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adults Literacy. Available from: http://nces.ed.gov/pubs2006/2006483.pdf/. Accessed January 30, 2015. | ||
Kripalani S, Risser J, Gatti ME, et al. Development and evaluation of the adherence to refills and medications scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118–123. | ||
Gazmararian JA, Baker DW, Williams MV, et al. Health literacy among Medicare enrollees in a managed care organization. JAMA. 1999;281(6):545–551. | ||
Kim SH, Lee EJ. The influence of functional literacy on perceived health status in Korean older adults. J Korean Acad Nurs. 2008;38(2):195–203. | ||
Weintraub D, Maliski SL, Fink A, et al. Suitability of prostate cancer education materials: applying a standardized assessment tool to currently available materials. Patient Educ Couns. 2004;55(2):275–280. | ||
George J, Elliott RA, Stewart DC. A systematic review of interventions to improve medication taking in elderly patients prescribed multiple medications. Drugs Aging. 2008;25(4):307–324. | ||
Raji MA, Kuo YF, Salazar JA, et al. Ethnic differences in antihypertensive medication use in the elderly. Ann Pharmacother. 2004;38(2):209–214. | ||
Kuo YF, Raji MA, Markides KS, et al. Inconsistent use of diabetes medications, diabetes complications, and mortality in older Mexican Americans over a 7-year period: data from the Hispanic established population for the epidemiologic study of the elderly. Diabetes Care. 2003;26(11):3054–3060. | ||
Barat I, Andreasen F, Damsgaard EMS. Drug therapy in the elderly: what doctors believe and patients actually do. Br J Clin Pharmacol. 2001;51(6):615–622. | ||
Monane M, Bohn RL, Gurwitz JH, et al. The effects of initial drug choice and comorbidity on antihypertensive therapy compliance: results from a population-based study in the elderly. Am J Hypertens. 1997;10(7 Pt 1):697–704. | ||
Marcum ZA, Driessen J, Thorpe CT, et al. Impact of multiple pharmacy use on medication adherence and drug-drug interactions in older adults with Medicare Part D. Am Geriatr Soc. 2014;62(2):244–252. | ||
Murray E, Lo B, Pollack L, et al. The impact of health information on the internet on the physician-patient relationship: patient perceptions. Arch Int Med. 2003;163(14):1727–1734. | ||
Cooper C, Carpenter I, Katona C, et al. The AdHOC Study of older adults’ adherence to medication in 11 countries. Am J Geriatr Psychiatry. 2005;13(12):1067–1076. | ||
Donohue JM, Huskamp HA, Wilson IB, et al. Whom do older adults trust most to provide information about prescription drugs? Am J Geriatr Pharmacother. 2009;7(2):105–116. | ||
Morisky DE, Ang A, Krousel-Wood M, et al. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). 2008;10(5):348–354. | ||
Hyre AD, Krousel-Wood MA, Muntner P, et al. Prevalence and predictors of poor antihypertensive medication adherence in an urban health clinic setting. J Clin Hypertens (Greenwich). 2007;9(3):179–186. | ||
Safran DG, Neuman P, Schoen C, et al. Prescription drug coverage and seniors: findings from a 2003 national survey. Health Aff (Millwood). 2005;Suppl web exclusives:w152–w166. | ||
Heisler M, Wagner TH, Piette JD. Clinician identification of chronically ill patients who have problems paying for prescription medications. Am J Med. 2004;116(11):753–758. | ||
Kim SO. Medication adherence of elderly with hypertension and/or diabetes-mellitus and its’ influencing factors. Korean J Clin Pharm. 2011;21(2):81–89. | ||
Choi SY, Kang CY. A study on the determinants of out-patients’ satisfaction with medication counseling. Korean Public Health Res. 2007;33(2):147–161. | ||
Mohan AV, Riley MB, Boyington DR, et al. Illustrated medication instructions as a strategy to improve medication management among Latinos: a qualitative analysis. J Health Psychol. 2013;18(2):187–197. | ||
van Geffen EC, Philbert D, van Boheemen C, et al. Patients’ satisfaction with information and experiences with counseling on cardiovascular medication received at the pharmacy. Patient Educ Couns. 2011;83(3):303–309. | ||
Nikolaus T, Kruse W, Bach M, et al. Elderly patients’ problems with medication an in-hospital and follow-up study. Eur J Clin Pharmacol. 1996;49(4):255–259. | ||
Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. | ||
Mosher HJ, Lund BC, Kripalani S, et al. Association of health literacy with medication knowledge, adherence, and adverse drug events among elderly veterans. J Health Commun. 2012;17(Suppl 3):241–251. | ||
Bains SS, Egede LE. Associations between health literacy, diabetes knowledge, self-care behaviors, and glycemic control in a low income population with type 2 diabetes. Diabetes Technol Ther. 2011;13(3):335–341. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.