")
Back to Journals » Patient Preference and Adherence » Volume 14
Factors Affecting Adherence to Co-Trimoxazole Preventive Therapy in HIV/AIDS Patients Attending an Antiretroviral Therapy Clinic in Ethiopia University Hospital: A Cross-Sectional Study
Authors Mekonnen GB , Addis SA
Received 6 March 2020
Accepted for publication 12 May 2020
Published 22 May 2020 Volume 2020:14 Pages 881—890
DOI https://doi.org/10.2147/PPA.S252805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Gashaw Binega Mekonnen,1 Surafel Ashenafi Addis2
1Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2University of Gondar Compressive Specialized Teaching Hospital, Hospital Pharmacy, Gondar, Ethiopia
Correspondence: Gashaw Binega Mekonnen Tel +251 938735983
Email [email protected]
Purpose: This study aimed to assess the factors that affect adherence to co-trimoxazole preventive therapy (CPT) among human immunodeficiency virus (HIV)-positive adults in an antiretroviral therapy (ART) clinic at the University of Gondar Compressive Specialized Teaching Hospital (UOGCSTH).
Methods: A hospital-based cross-sectional study was conducted from March 1 to April 30, 2018, at the ART clinic at UOGCSTH. Data were collected using face-to-face interviews with pretested and standard questionnaires. Binary and multivariable logistic regression analyses were used to assess the association between different variables. P< 0.05 was used to declare the association.
Results: The prevalence of adherence to CPT by self-reporting measurement was 205 (67.8%). Factors such as level of education, taking street drugs (alcohol and khat), spouse knowledge about clients on CPT, knowledge of the benefit of CPT, duration of CPT, missed dose, got proper information on how to take CPT, and counseling done on refill were found to be significantly associated with adherence to CPT.
Conclusion and Recommendations: The overall adherence to CPT was fair in our study. To improve the adherence, continuous education and counseling, giving group service support for clients and having a separate counseling room are some of the possible solutions.
Keywords: factors, adherence, co-trimoxazole preventive therapy, HIV/AIDS, Ethiopia, University of Gondar
Introduction
HIV is one of the most common health crises ever faced by humankind.1,2 HIV destroys and impairs the immune cells and causes a depletion of CD4 T cells, resulting in conditions called opportunistic infections (OIs), and more than 90% of these are responsible for acquired immune deficiency syndrome (AIDS) morbidity and mortalities.3 High early morbidity and mortality have been observed in a number of ART programs in Sub-Saharan Africa.4,5
In Ethiopia, the total prevalence rate of HIV in 2017 among adults was 1%, and the estimated total people living with HIV/AIDS (PLWHA) accounted for 722 248 and 15,600 people died from AIDS-related illness.6
Early diagnosis, prophylaxis, and treatment of opportunistic infections evidently indicated that improving the quality and length of life of people living with HIV, even before the start of highly active antiretroviral treatment. However, OI continues to cause mortality and morbidity in HIV/AIDS patients still after ART. Most patients do not have a constant response to ART for several reasons, such as less adherence, drug side effects, drug interactions, or initial gaining of a drug-resistant of HIV.3,5
Co-trimoxazole is a fixed-dose combination of two antimicrobial drugs (sulfamethoxazole and trimethoprim) offers a synergistic effect with a broad spectrum of antimicrobial action that covers a variety of bacterial, fungal, and protozoan infections. CPT is a feasible, well-tolerated, widely available, cost-effective intervention to reduce HIV-related morbidity and mortalities related to OIs.5–8
Adherence to CPT has been found to reduce the incidence of OIs and other AIDS-related illnesses. As a result, there is an improvement in the quality of life and increased life expectancy of people infected with HIV. Many studies on CPT revealed that reductions in mortality of between 25% and 46%, reduced OIs as well as rates of hospitalization, weight loss, diarrhea, and malaria, have been reported in low - and middle-income countries.4,9 Therefore, adherence affects the outcome, but achieving and maintaining good adherence is a considerable challenge. This has been a remarkable challenge in HIV/AIDS patients, among whom suboptimal adherence has been reported in a study.9 CPT is self-administered, and therefore, adherence cannot be insured. Adherence to CPT has been low and opportunistic infections continue to be the major cause of mortality and morbidity in HIV, accounting for 47% of AIDS-related deaths.10,11 Adequate initial and ongoing counseling is critical to achieving good adherence. Initial counseling can help patients to identify factors that may interfere with adherence while ongoing counseling both reinforce positive trends and allow for the detection of an emerging issue.10
Several factors affect the level of adherence to CPT like personal related factors such as lack of means of transport, level of education, knowledge of couple, poor knowledge on the benefit of CPT, alcohol or illicit substances, and stress.,12–14 drug-related perceiving medicines as toxic to the body, duration of CPT, missed dose, and added drugs;12–15 and health-center-related factors such as clinics were too far to attend monthly to pick up the tablets, counseling system, and stock out.12,14,15
Identification of a cause that affects adherence to CPT may help for improve adherence. Hence, to the best of our search done, no prior study has been conducted on the factor that affecting of adherence to CPT among HIV/AIDS patients on treatment in UoGCSTH. Thus, adherence to CPT in adult HIV patients in this region is poorly understood, and the most crucial factors for improving adherence are not yet fully investigated. The aim of the present investigation was to assess factors that influence adherence to CPT among HIV-positive adult individuals in the ART clinic at UoGCSTH. Therefore, the findings will be used by the hospital health team and other program implementers to enhance adherence to CPT among HIV/AIDS patients.
Methods
Study Setting and Design
A hospital-based prospective cross-sectional study was conducted at the UoGCSTH ART clinic from March 1 to April 30, 2018. The hospital serves 7 million people in its catchment area of northwest Ethiopia, and it is the largest tertiary hospital in the region. UoGCSTH is located 750 km northwest of the national capital, Addis Ababa. It has both inpatient and outpatient departments.
ART clinics is the one among these outpatient clinics and provide health care services for 8681 adult HIV/AIDS patients, of which 5100 are currently on ART and 1000 HIV/AIDS patients on CPT. The UoGCSTH serves more than five million people in the North Gondar zone and people of neighboring zones.
Sample Size Calculation and Sampling Technique
The sample size was calculated based on a single population proportion formula by considering the proportion 50% with 95% confidence interval and with a 5% margin of error, and the sample size drawn was n=384.
Since the sample was taken from the total population of 1000 PLWHA who had been taking CPT, that is, less than 10,000, the sample size was adjusted to n=274.
Finally, with the addition of 10% non-response, a total of 302 participants were included. During the introduction survey, 5100 PLWHA medical records were screened. Of these, 1000 patients were on CPT. Of 1000 eligible patients for the study, we selected 302 participants using a systematic random sampling technique with an interval (k-value) 3. Randomly, one number was selected from 1 to 3 by the lottery method, and the unique medical registration number of patients was selected in every 3rdunit of registered HIV patients from the ART logbook registration. We invited every three patients attending the ART Clinic to participate in an interview until the required sample was recruited. The next patient registration number was taken to avoid repetition if the medical registration number was redundant; the patient did not meet the inclusion criteria or did not have scheduled follow-up during the study period.
Inclusion and Exclusion Criteria
Those randomly selected HIV patients aged ≥18 years, on CPT, who willing gave informed consent and visited the clinic from March 1 to April 30, 2018, for follow-up were included. However, those patients who were difficult to communicate were excluded from the study.
Study Variables
The dependent variable was adherence to CPT. Independent variables included socioeconomic and demographic (age, sex, occupation, marital status, level of education), patient-related factors (level of education, knowledge of couple, poor knowledge on the benefit of CPT, alcohol or illicit substances, and stress), drug-related factors (availability, adverse drug reactions, duration of CPT, missed dose, and additional drugs), and health service factors (clinics were too far to attend monthly to pick up the tablets, counseling system, and stock out).
Data Collection Method
Data on participants’ socio-demographic characteristics, patient-related factors, drug-related factors, and health-facility-related factors were collected through face-to-face interviews using a structured questionnaire. The magnitude of adherence to CPT was measured using self-reported measurements.17 Two data collectors who are 2 B.Sc nurses and one supervisor, B. Pharmacy, were recruited from ART clinics. Data collectors and supervisors were trained intensively for two days by the principal investigator on the contents of the questionnaire, data collection methods, and ethical concerns.
Data Quality Assurance
The data collection tool was developed from different kinds of literatures.11,12,15 The questions were translated into Amharic with modifications and back-translated to English to retain its original meaning and so as to maintain an unbiased response. The filled questionnaire was checked daily for completeness by the principal investigator. A pretest was done on some of the patients approximately 5% (15) of the sample to make ensure that the study was feasible in this way and to see if the data collection format was appropriate and consistent when gathering the intended information.
Operational Definitions
CPT- is a feasible, inexpensive, and well-tolerated method of using co-trimoxazole intervention in people living with HIV/AIDS to reduce HIV/AIDS-related morbidities and mortalities caused by various bacteria, fungi, and protozoa.15,16
Good adherence: taking greater than 95% prescribed dose of co-trimoxazole.17
Poor adherence: less than 95% missed greater than 3 doses per 30 doses of co-trimoxazole.17
Data Processing and Analysis
The collected data were coded, cleared, and checked for completeness, entered into a computer using Epi Info 7 software and analyzed using statistical packages for social sciences Version 21 statistical software computer program. Statistical analyses were performed using SPSS v.21 (SPSS Inc., Chicago, IL, USA). Frequencies, percentages, mean, and standard deviations were used to describe the variables. Binary logistic regression was used to see the association between independent and dependent variables. Odds ratios were used to see the strength of the association. In this research, there are many potential variables that might have a relation to the outcome and among each other. So, if we included all these variables in the multivariable regression model, confounding, and interaction effect might highly bias our estimate and hence we preferred to use the recommended variable selection method. That is, variables that had a p-value of less than 0.25 at the bivariate analysis were considered for multivariate regression analysis, and those variables with a P-value less than 0.05 were as cut-off points for determining statistical significance.
Ethical Considerations
The study was conducted after ethical clearance and informed verbal consent was acceptable and approved by the Institutional Review Board of the School of Pharmacy, University of Gondar. Informed consent was also obtained from each respondent after the purpose of the study had been explained. They were also informed that participation was voluntary and they could withdraw from the study at any stage if they desired. Participant’s confidentiality was guaranteed by not recording their personal identifiers on the questionnaire. And that this study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of the Respondents
A total of 302 patients were included in this study. The mean age of the study participants was 37.3 years with SD of ± 11.8 years. One hundred eighty-three (60.6%) participants were female. 146 (48.3%) participants were married, and the majority 284 (94%) were Amhara in ethnicity and Orthodox Christians 259 (85.8%). 149 (49.3%) respondents were primary schools. The majority of 212 (70.2 %) of the participants were employed. All of these are shown in Table 1.
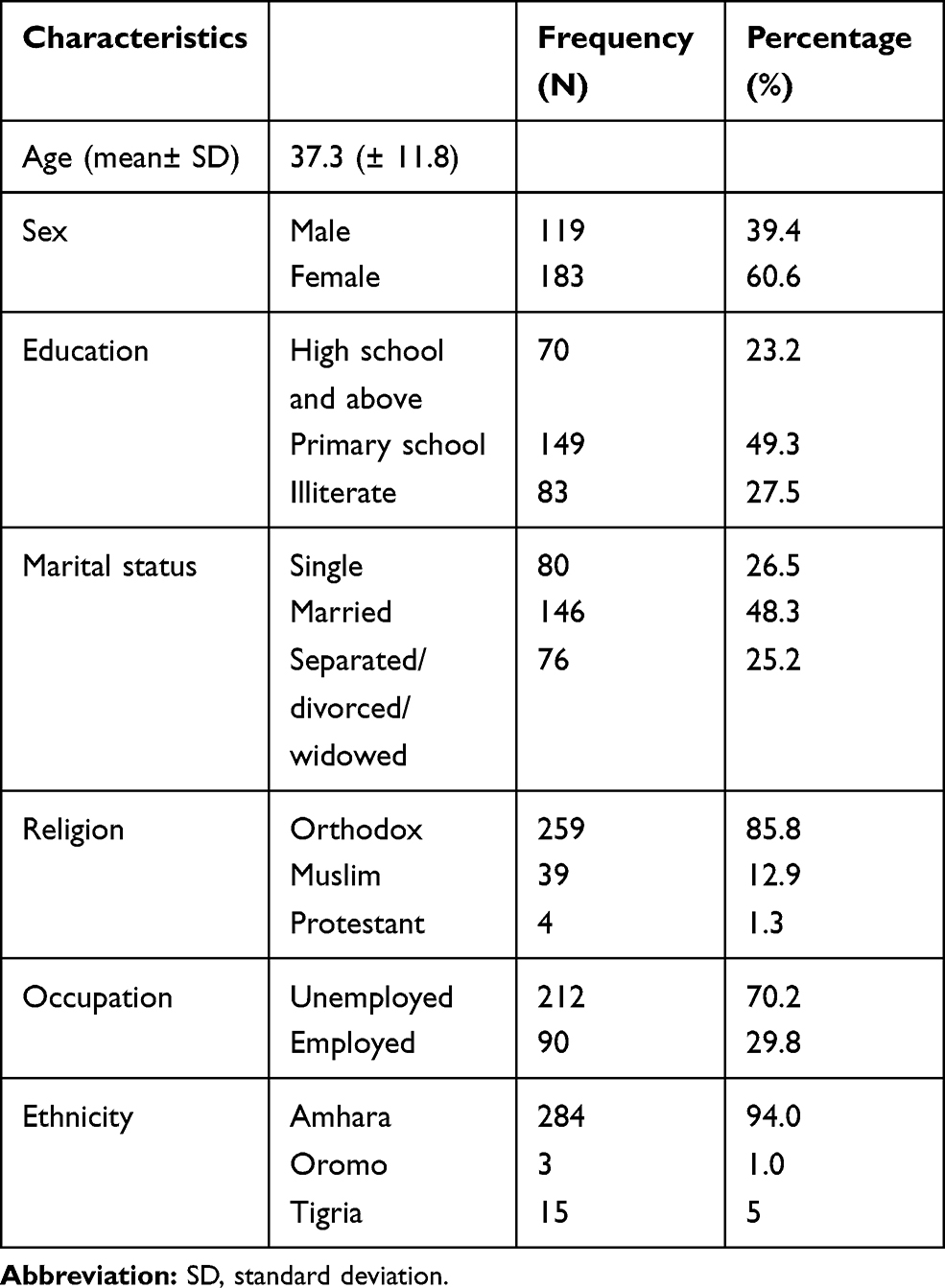 |
Table 1 Socio-Demographic Characteristics of the Participants |
Prevalence of Adherence
The magnitude of adherence to CPT was measured using self-reported measurements. Our results showed that 205 (67.8%) participants were adhering to CPT over the past 30 days. 205 of respondents had missed only one dose and 97 (32.2%) reported missing more than three doses within the past one month. Of these, 62 (63.9%) of the respondents reported that they had missed pills due to forgot to take the pill, development of side effect 15 (15.5), lack of transport 12 (12.4%), and perceived or actual lack of effect (8.2%).
Factors Affecting Adherence to CPT
Association Between Socio-Demographic Factors with Adherence to CPT
The identified socio-demographic factors that contributed to the adherence to CPT were the level of education. However, the other variables were not statistically significant. The level of education of the participants at P= value 0.002 significantly affected the adherence to CPT. Participants high school and above were 2.4 times more likely to adhere to CPT than primary school, and illiterate participants are presented in Table 2.
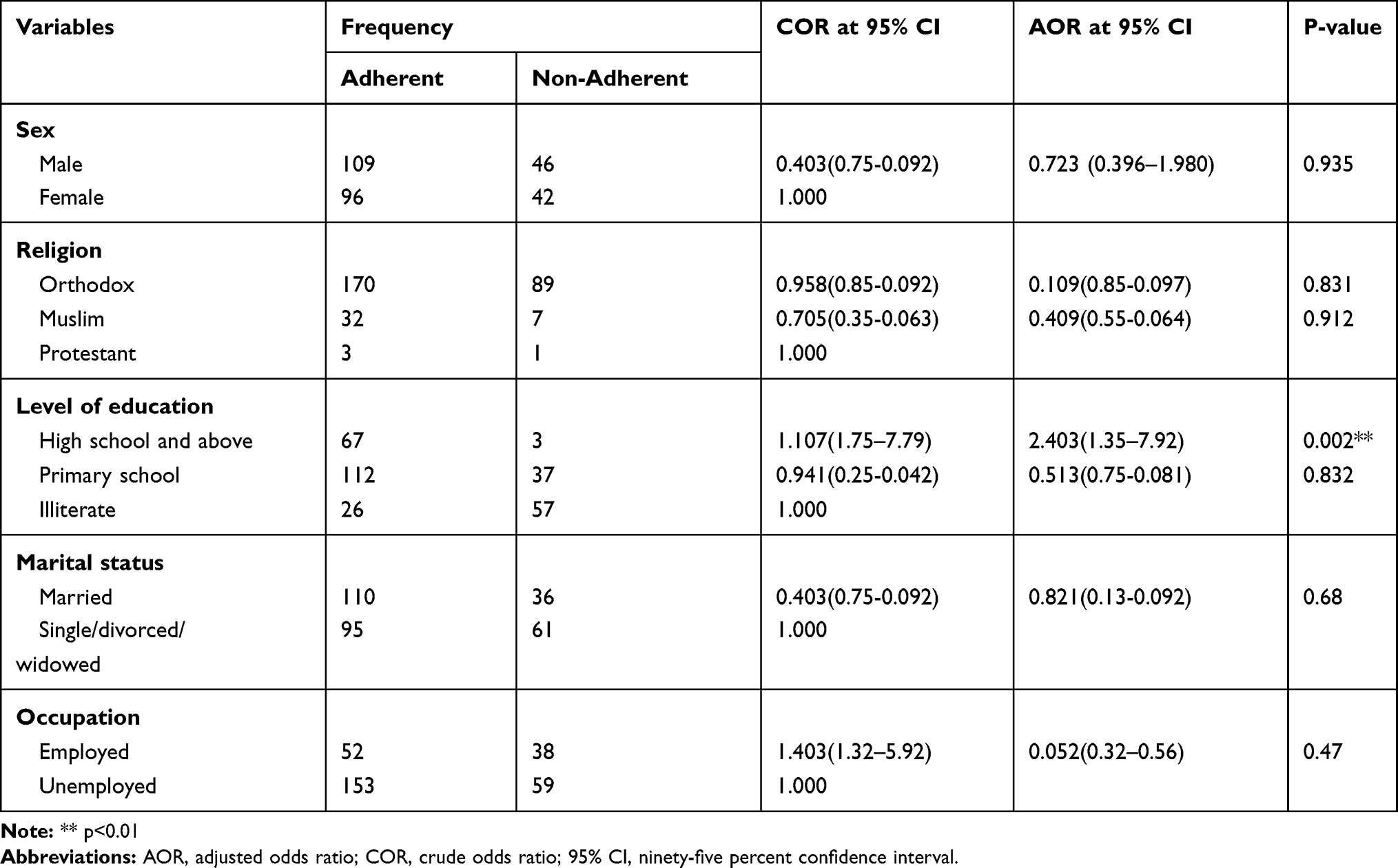 |
Table 2 Socio-Demographic Factors of Participants with Adherence to CPT |
Patient-Related Factors
Patients’ adherence to prescribed drug regimens has been shown to be greatly influenced by individual behavior patterns that have a direct attitude on how well the patient sticks to their medication.
Thirty-four (11.3%) of the participants reported appealing to drugs and other substance abuse. The results of this study revealed that alcohol was the most widely used substance among the respondents at 30 (88.2%), followed by Khat 4 (11.8%), and when asked why they engaged in drug use, 25 (73.5%) of the respondents who reported using drugs gave psychosocial stress as their main reason for doing so, 6 (17.7%) of them reported habit development over time even before infection with HIV/AIDS, as shown in Figure 1.
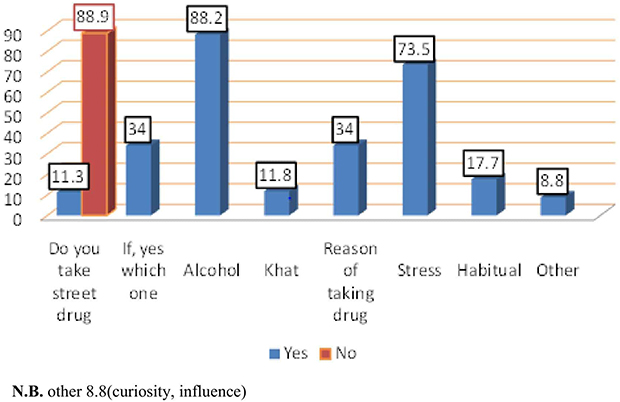 |
Figure 1 Frequencies of street drug intakes and reasons by participants. |
Out of 146 married participants, 130 (68.5%) were aware of their partner’s HIV status. And 110 (84.6%) spouse knew they were taking co-trimoxazole pills, whereas 20 (13.4%) did not know that their spouse was taking CPT. Among 302 participants, 268 (88.7%) participants had another member of their family knew about their HIV status. 116 (38.4%) respondents had another family member on CPT. Of these, 102 (87.9%) of the respondents reported that they had taken co-trimoxazole pills for opportunistic infection related to HIV, 8 (6.9%) for treatment of urinary tract infection, and 6 (5.2%) for respiratory disease treatment.
Association Between Person-Related Factors with Adherence to CPT
Participants who took street drugs were such as alcohol and khat 1.3 times less likely to adhere to CPT than those who did not. Having a spouse aware of the participants being on CPT was 1.2 times to adhere to CPT than the spouse not aware of CPT [Table 3]
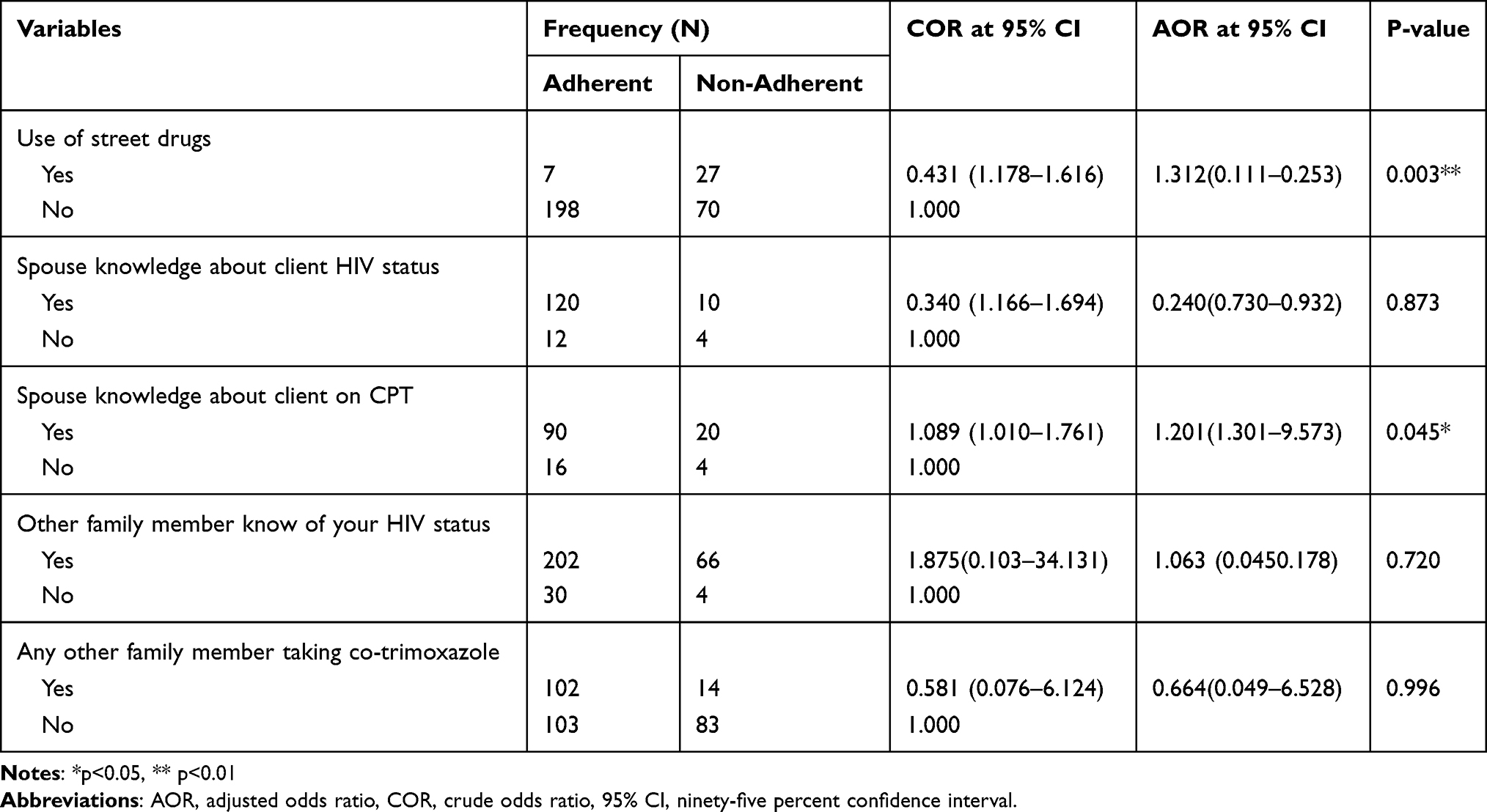 |
Table 3 Patient-Related Factors of Participants with Adherence to CPT |
Drug-Related Factors
The majority of participants 268 (88.7%) knew taking CPT as beneficial, of which 223 (83.2%) knew they were taking the medication to alleviate signs and symptoms are presented in Figure 2.
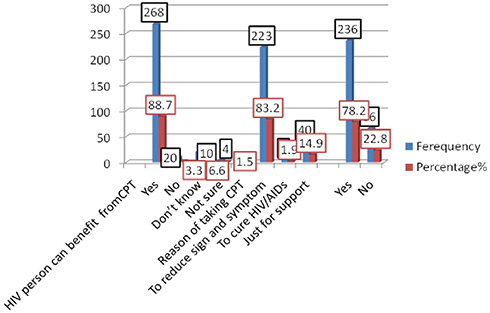 |
Figure 2 Participant’s knowledge of the benefits of CPT. |
Duration of CPT
Of the total participants, 103 (34%) had been on CPT for less than 6months, 65 (21.5) had CPT 6–12months, and 134 (44.4%) had been on CPT for more than two years. The mean duration of the program was 1.7 years ± 0.83year.
Other Drugs Taken by the Participants
Two hundred and seventy-two (90.15) of 302 participants were concurrently taking other drugs. Of these, two hundred forty-two (88.9%) were taking ARTs and 30 (11.2%) participants were on other drugs, and ARTs are summarized in Figure 3.
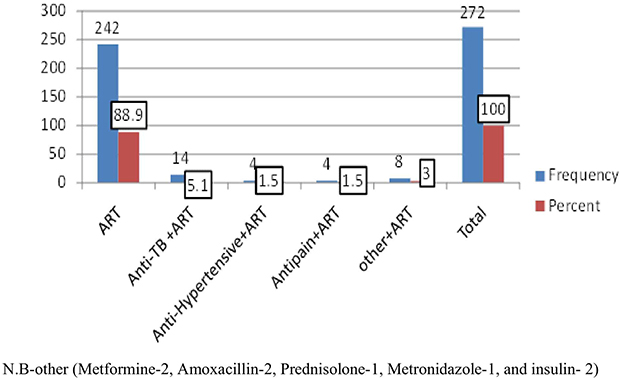 |
Figure 3 Other drugs taken by participants. |
Drug-Related Factors of Participants with Adherence to CPT
Participants perceived CPT to be beneficial were 1.36 times more likely to adhere to CPT than those who did not. Participants who had been on CPT for less than six months, 1.12 times more likely to adhere to CPT than those who had been more than six months. Participants who missed CPT were 1.2 times less likely to adhere to CPT. However, other variables were not statistically significant, as shown Table 4.
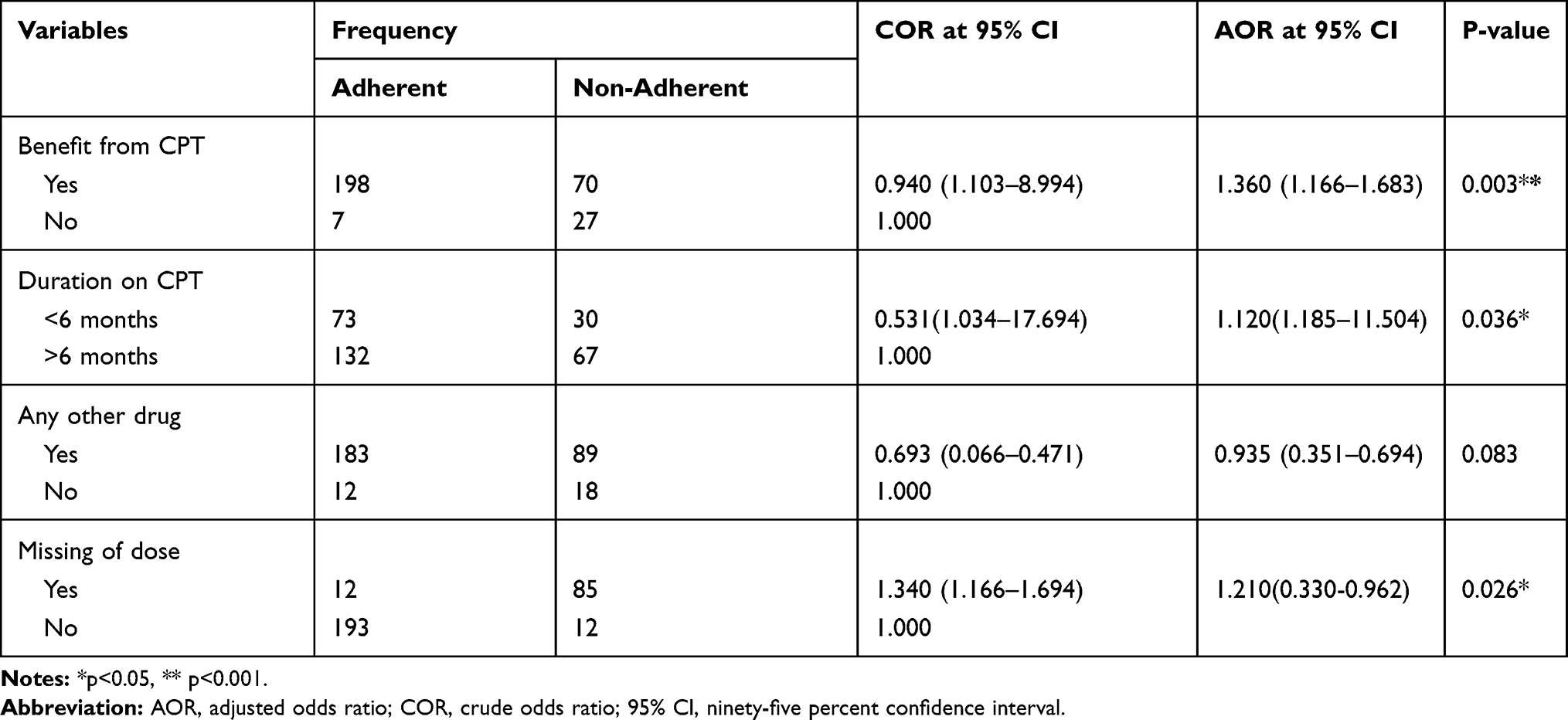 |
Table 4 Drug-Related Factors of Participants with Adherence to CPT |
Health-Facility-Related Factors
One hundred thirty-one (43.4%) participants lived over 5 kilometers from the hospital. The majority of the participants 278 (92.1%) said received a regular supply of CPT and did not encounter any difficulties accessing the drug from the facility. One hundred twenty-two (40.4%) participants considered the time taken to see the doctor as long. Moreover, 95 (31.5%) of the participants considered the information given by the health care provider during the clinical visit not adequate, and again 142 (47.1%) participants said they were not given counseling during refill are presented in Table 5.
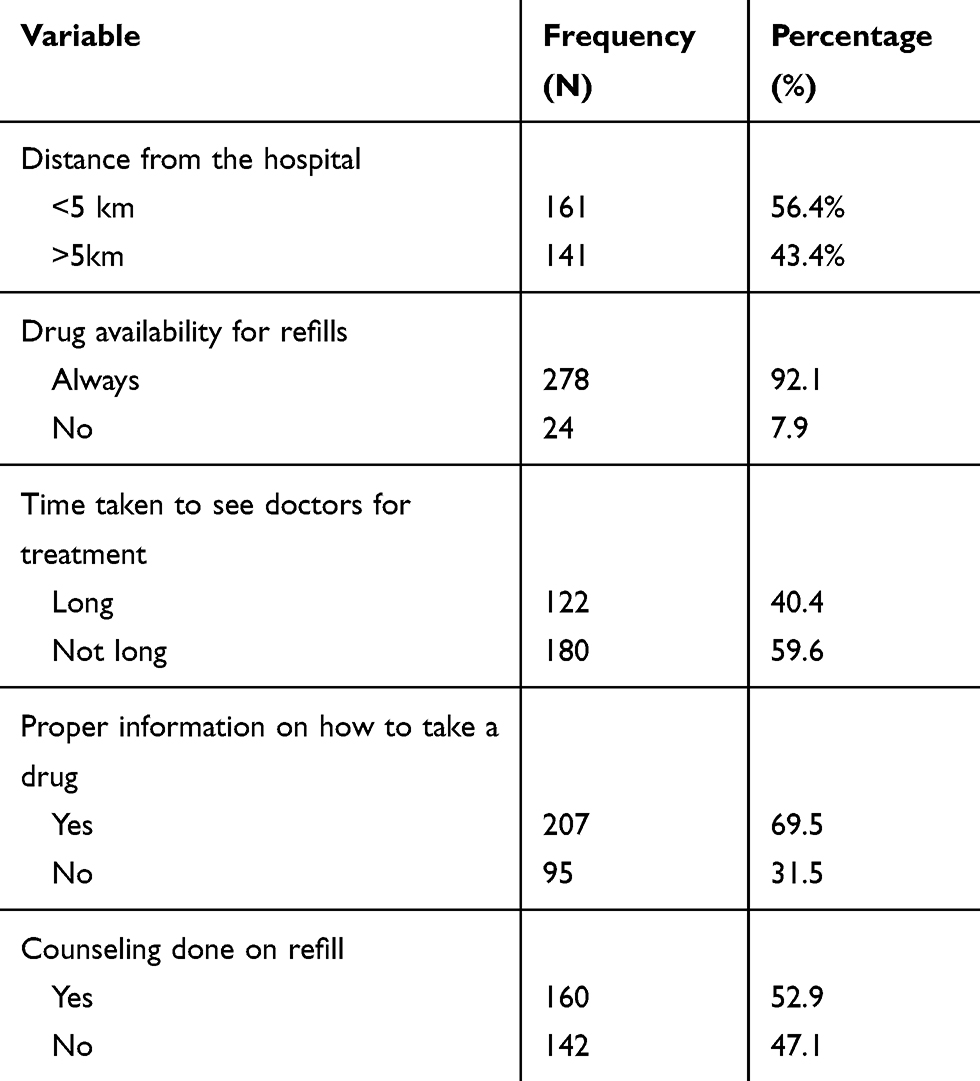 |
Table 5 Health-Facility-Related Factors in CPT |
Association Between Health-Center-Related Factors with Adherence to CPT
Participants got proper information by the health care provider during the clinical visit 2.3 times more likely to adhere to CPT than those participants not got proper information. Participants got counseling during refill 1.6 times more likely to adhere to CPT than those who did not. However, other variables were not statistically significant are presented with Table 6.
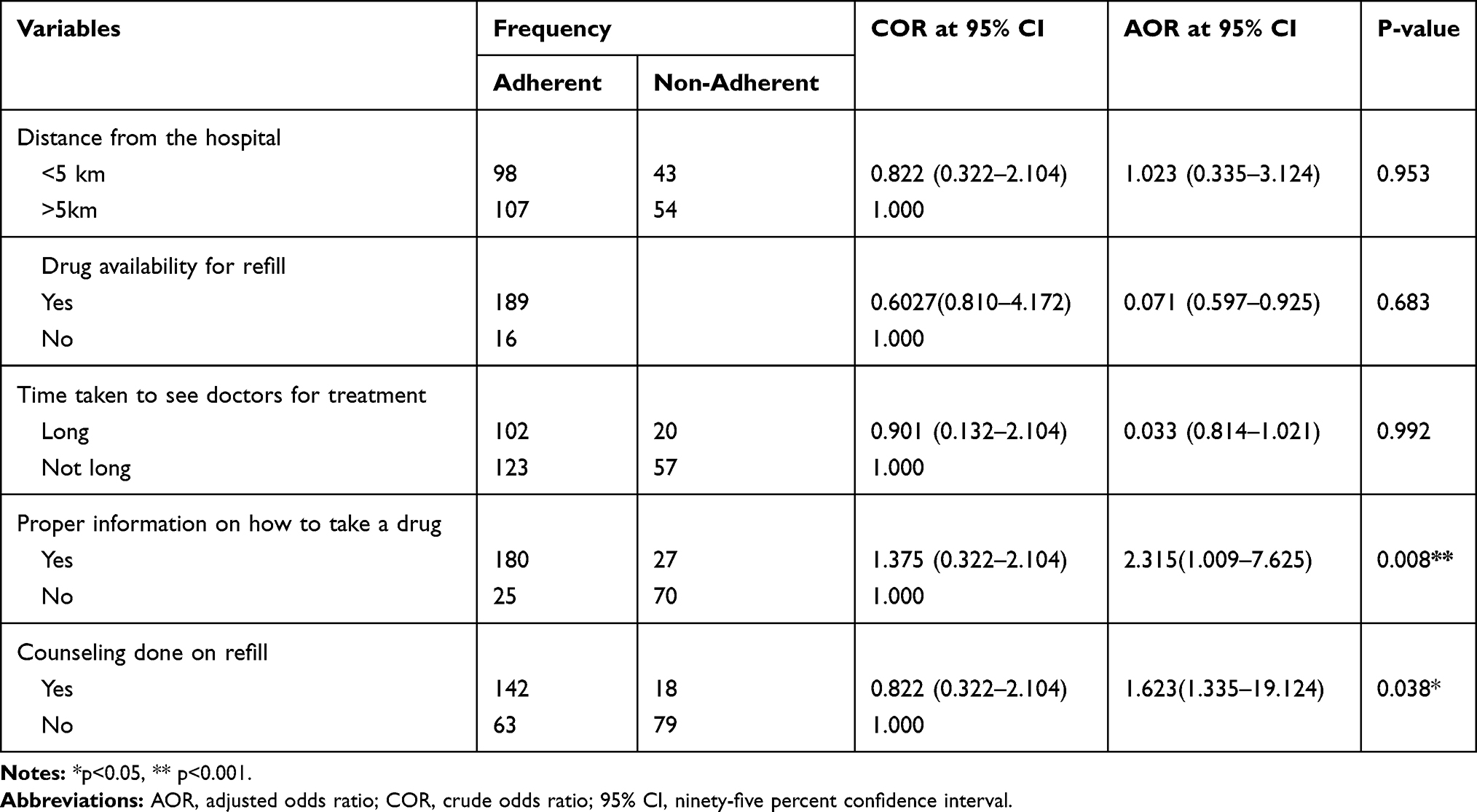 |
Table 6 Health-Facility-Related Factors of Participants with Adherence to CPT |
Discussion
Medication adherence is an emergent concern in healthcare systems, health care providers, and others because of the facts that low adherence to the course of therapy is a major problem, mostly in patients with chronic diseases like HIV/AIDS. It is common and associated with compromised treatment effectiveness, adverse effects, mortality, and higher expenses on the health care system.18–20
Adherence is defined as taking medications or interventions correctly according to prescription. With any drug use, drug effectiveness is directly proportional to the patient’s level of adherence. Strict adherence is vital for successful CPT. Event exposing patients to CPT for a longer period is more likely to influence adherence to CPT.21–23
There are different methods for evaluating the prevalence of adherence.23 These include direct methods such as biologic markers and body fluid assays, or indirect methods such as self-report, interview, pill counts, and pharmacy records, or a combination of these methods may be employed. Of these alternatives, self-report is the most widely used for adults in developing countries.24 Given its ease of implementation and use of already existing resources.24–26 At this time, there are no gold standard methods for assessing adherence.25
In the present study, the adherence of CPT by self-reported measurement was 205 (67.8%). This finding was consistent with those similar studies done in Uganda 65.7%12 and the University of Gondar.16 However, this finding is lower than that of a study conducted in the MUJHU AIDS clinic at Mulago hospital 77.6%.14 This may to differences in study settings and the majority of the participants’ caregivers in the MUJHU AIDS clinic at Mulago hospital lives in the city.
Adherence to CPT is influenced by several factors. They range from socio-demographic factors, patient-related factors, drug-related and health-related factors. Among the socio-demographic characteristics, such as high school and above education, participants had 2.4 times more likely to adhere to CPT than primary and illiterate participants [AOR 95% CI 2.403 (1.35–7.92) (P=0.002)]. This may be due to the fact that the more educated patients are good knowledge about their CPT.
Participants who took street drugs like alcohol and khat were 1.3 times less likely to adhere to CPT than those who did not take. This result was consistent with the study done in Uganda.12 This may be a street drug like alcohol and khat consumption resulting in poor memory, high forgot, and little attention given to adherence to CPT. Having a spouse aware of the participants being on CPT was 1.2 times to adhere to CPT than the spouse not aware of CPT. This result was consistent with the study done in Uganda.12 This might be the spouse’s support for their clients to enhance adherence to CPT. Those patients who had knowledge of the benefit of CPT were 1.36 times more likely to adhere to CPT than those who did not. This finding was in agreement with those similar studies done in Uganda.12
Participants who had been on CPT for less than 6 months were 1.12 times more likely to adhere to CPT than those who had been more than six months. However, this finding was not in agreement with the study done in Uganda.12 This may be because exposing patients to CPT for a longer period is more likely to affect adherence to CPT.
Participants got proper information by the health care provider during the clinical visit 2.3 times more likely to adhere to CPT than those participants not get proper information. Clients who took counseling during refill were1.6 times more likely to adhere to CPT than those who did not take counseling. This finding was in agreement with those similar studies done in Uganda.12 This may be due to patients getting adequate counseling, and clear information on CPT is a greater chance of adherence to CPT. However, distance from the hospital, drug availability for refill, and time taken to see doctors for treatment was not significantly associated with adherence to CPT.
To our knowledge, this is the first study to assess factors that affect adherence to CPT in adult HIV-infected patients in Ethiopia university hospitals, so this study can provide baseline information. However, there were some limitations to the present study that has to be considered. The possible limitations of the present study were: this is a cross-sectional study design, whereby claims about the directionality of a causal relationship between the dependent and independent variables cannot be verified. The questionnaire was administered through face-to-face interviews by trained nurses in ART clinics, which may increase the respondents’ inclination to give socially acceptable answers. Moreover, in this study, adherence was measured using self-report, which can potentially lead to recall bias by the respondents, which should be taken into consideration while interpreting the results. Moreover, the study was assessed using only a quantitative method.
Conclusion
The findings of this study found that the prevalence of adherence by self-report was relatively good. The level of education, spouse knowledge on CPT, knowledge of the benefit of CPT, takes street drugs, duration of CPT, proper information on how to take a drug, and counseling during refill, independently affected CPT adherence. To improve the adherence, continuous education and counseling, giving group service support for clients and having a separate counseling room are some of the possible solutions.
Abbreviations
AIDS, acquired immune deficiency syndrome; ART, antiretroviral therapy; ADR, adverse drug reaction; CPT, co-trimoxazole preventive therapy; HIV, human immunodeficiency virus; OIs, opportunistic infections; UOGCSTH, University of Gondar Compressive Specialized Teaching Hospital.
Data Sharing Statement
All available data can be obtained by contacting the corresponding author.
Acknowledgments
We would like to thank the data collectors and supervisors involved in data collection and the clients for their participation.
Author Contributions
Both authors of this manuscript made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work, including ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
Financial support was provided only by the authors. The authors declare that they have no conflicts of interest.
References
1. Gayle HD, Hill GL. Global impact of immunodeficiency virus and AIDS. Clini Microbiol Rev. 2001;14(2):327–335. doi:10.1128/CMR.14.2.327-335.2001
2. Federal Democratic Republic of Ethiopia. Country progress report on the HIV response. September, 2014.
3. Federal HIV/AIDS Prevention and Control Office Federal Ministry of Health; Guidelines for management of opportunistic infections and antiretroviral treatment in adolescents and adults in Ethiopia. 2008.
4. Lowrance D, Makombe S, Harries A, et al. Lower early mortality rates among patients receiving antiretroviral treatment at clinics offering cotrimoxazole prophylaxis in Malawi. J Acquir Immune Defic Syndr. 2007;46:56–61.
5. Suthar AB, Granich R, Mermin J, et al. Effect of cotrimoxazole on mortality in HIV-infected adults on antiretroviral therapy: a systematic review and meta-analysis. Bull World Health Organ. 2012;90:128C–138C. doi:10.2471/BLT.11.093260
6. HAPCO.HIV prevention in Ethiopia National Road map; 2018. Available from: https://ethiopia.unfpa.org/en//hiv-prevention-Ethiopia-national-road-map.
7. World health organization guideline on Post-Exposure Prophylaxis for HIV and Use of co-trimoxazole prophylaxis for HIV-related infections among adults, adolescents and children: recommendations for a public health approach: december 2014 supplement of the 2013 consolidate ARV guidelines. Available from: https://www.who.int/hiv/pub/guidelines/arv2013/arvs2013upplement_dec2014/en/.
8. Mermin J, Lule J, Ekwure JP, et al. Effect of co-trimoxazole prophylaxis on morbidity, mortality,CD4cell count and viral load in HIV in rural Uganda. Lancet. 2004;364(9443):1428–1434. doi:10.1016/S0140-6736(04)17225-5
9. Grimwade K, Sturm A, Nunn A, Mbatha D, Zungu D, Gilks C. Effectiveness of cotrimoxazole prophylaxis on mortality in adults with tuberculosis in rural South Africa. AIDS. 2005;19:163–168. doi:10.1097/00002030-200501280-00008
10. Gallant JE, Moore RD, Chaisson RE. Prophylaxis for opportunistic infections in patients with HIV infection. Ann Intern Med. 1994;120:932. doi:10.7326/0003-4819-120-11-199406010-00006
11. Musembi J, Determinants of adherence to cotrimoxazole preventive therapy among hiv infected persons on treatment in Machakos District Hospital, Machakos County, Kenya 2014. Available from: https://ir-library.ku.ac.ke/handle/123456789/13745.
12. Simon M. Factors Affecting Adherence to Cotrimoxazole Prophylaxis Among HIV/AIDS Patients in Rukungiri District. Uganda; 2009. Available from: http://makir.mak.ac.ug/handle/10570/992.
13. Denue BA. Knowledge regarding co-trimoxazole preventive therapy among patients who are HIV positive in a tertiary health facility, northwestern Nigeria. Sub-Sharan Afr J Med. 2017;4:31–36. doi:10.4103/ssajm.ssajm_22_16
14. Eldred LJ, Wu AW, Chaisson RE, Moorev RD. Adherence to antiretroviral and Pneumocystis prophylaxis in HIV disease. J Acquir Immune Defic Syndr. 1998;18:117–125. doi:10.1097/00042560-199806010-00003
15. Kasirye G, factors affecting adherence to cotrimoxazole prophylaxis in HIV infected exposed children attending MUJHU AIDS clinic at Mulago hospital. [dissertation]. Makere medical school. 2006:
16. Gebresillassie BM, Gebeyehu MB, Abegaz TM, et al. Evaluation of cotrimoxazole use as a preventive therapy among patients living with HIV/AIDS in Gondar University Referral Hospital, northwestern Ethiopia: a retrospective cross-sectional study. HIV AIDS. 2016;8:125. doi:10.2147/HIV.S103081
17. WHO. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach; 2013. Available from: https://www.who.int/hiv/pub/guidelines/arv2013/en/.
18. Napolitano F, Napolitano P, Angelillo IF. Medication adherence among patients with chronic conditions in Italy. Eur J Public Health. 2016;26(1):48–52. doi:10.1093/eurpub/ckv147
19. Sahm. L, MacCurtain A, Hayden J, Roche C, Richards HL. Electronic reminders to improve medication adherence—are they acceptable to the patient? Pharm World Sci. 2009;31:627–629. doi:10.1007/s11096-009-9327-7
20. Ahmed R, Aslani P. What is patient adherence? A terminology overview. Int J Clin Pharm. 2014;36:4–7.
21. Bardfield J, Agins B, Palumbo M, Wei AL, Morris J, Marston B. Improving rates of cotrimoxazole prophylaxis in resource-limited settings: implementation of a quality improvement approach. Int J Qual Health Care. 2014;26(6):613–622. doi:10.1093/intqhc/mzu085
22. Moodley D, Reddy L, Mahungo W, Masha R. Factors associated with coverage of cotrimoxazole prophylaxis in HIV- exposed children in South Africa. PLoS One. 2013;8(5):e63273. doi:10.1371/journal.pone.0063273
23. Landovitz RJ. What’s the best way to measure ART adherence? J Watch. 2011;23(3).
24. Vreeman RC, Wiehe SE, Pearce EC, Nyandiko WM. A systematic review of pediatric adherence to antiretroviral therapy in low- and middle-income countries. Ped Infect Dis J. 2008;27(8):686–691. doi:10.1097/INF.0b013e31816dd325
25. Nachega JB, Mills EJ, Schechter M. Antiretroviral therapy adherence and retention in care in middle-income and low-income countries: current status of knowledge and research priorities. Curr Opin HIV AIDS. 2010;5(1):70–77. doi:10.1097/COH.0b013e328333ad61
26. Chesney MA. The elusive gold standard: future perspectives for HIV adherence assessment and intervention. J Acquir Immune DeF Syndr. 2006;43(1):S149–S155. doi:10.1097/01.qai.0000243112.91293.26
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.