")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Facial Herpetic Folliculitis Should Be Concerned in the Clinic: A Retrospective Case Series
Authors Cao Z , Zhang C , Wei J , Wei G
Received 3 September 2022
Accepted for publication 2 November 2022
Published 16 November 2022 Volume 2022:15 Pages 2487—2494
DOI https://doi.org/10.2147/CCID.S388588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Zhiqiang Cao, Chunhong Zhang, Jingjing Wei, Guo Wei
Department of Dermato-venereology, the Second Hospital of Shandong University, Jinan, People’s Republic of China
Correspondence: Guo Wei, Department of Dermato-venereology, the Second Hospital of Shandong University, 247 Beiyuan Street, Tianqiao District, Jinan, 250033, People’s Republic of China, Tel +86-531-85875027, Fax +86-531-88962544, Email [email protected]
Background: Herpetic folliculitis (HF) is a rare manifestation of herpes virus infection of the skin, which has different presentations causing frequent misdiagnosis. Previous literature has reported follicular infections caused by herpes simplex virus (HSV) in the beard area, called herpetic sycosis, but only a few cases presented facial extensive folliculitis.
Purpose: This case series aimed to describe the clinical features of facial generalized herpetic folliculitis.
Methods: We retrospectively collected a case series of 20 patients with facial diffused herpetic folliculitis diagnosed clinically or experimentally from outpatients between 2012 and 2022. The reported cases similar to HF of literature were concluded.
Results: There were 19 females and 1 male in this study. Disease duration varied from 1 to 10 days, and lesion manifestations were predominantly papules and maculopapules. Most patients suffered spontaneous pain or pruritus and recovered with antiviral treatment. All cases achieved great improvements in lesions after antiviral and topical medication therapy.
Conclusion: This case series suggests that in patients with infectious folliculitis of the face when the lesions develop acutely and diffusely, dermatologists should take into account the possibility of herpetic folliculitis, especially in cases where antibacterial or antifungal therapy is resistant, and actively administer antiviral therapy after diagnosis.
Keywords: clinical presentations, face, herpetic folliculitis, herpes simplex virus, diagnosis
Introduction
Herpetic folliculitis (HF) is a rare disease involving hair follicles and sebaceous epithelium, which is caused by varicella zoster virus (VZV) or herpes simplex virus (HSV). These viruses can cause skin or mucosal infections, and thus produce primary and recurrent infections. However, HF is uncommon in the literature and is present in a variety of forms in the clinic. Follicular involvement of HSV in the beard area has been reported in the literature and is referred to as herpetic sycosis.1,2 We report 20 patients with facial follicular damage due to herpes virus in the past 10 years, and also review the reported cases with similar clinical features.
Patients and Methods
We retrospectively collected a case series of 20 patients with HF diagnosed clinically or experimentally in the outpatient clinic of the Department of Dermato-venerology, the Second Hospital of Shandong University, from January 2012 to August 2022. In all cases, two patients got tested for HSV. We only included cases involving facial lesions as discrete distributions. Exclusion criteria included herpetic sycosis and Kaposi varicella rash. Clinical information was obtained from medical records and clinical follow-ups. We termed this kind of folliculitis due to herpes virus as facial HF, and similar cases reported in the previous literature were summarized.
This study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practices, and local regulatory requirements. Ethics Committee approval from the Institutional Review Board of the Second Hospital of Shandong University (Ethics No. KYLL-2022LW137) was obtained. Data collection included the patient’s gender, age, duration of disease prior to visiting, lesion types, subjective symptoms, HSV history, underlying conditions, and treatments. The clinical impression was established by the provider based on their assessment and patient’s report at each visit. Patients gave consent to the inclusion of material pertaining to themselves in this article, they acknowledged that they cannot be identified via the article; the Authors fully anonymized patients’ material. All clinical features of our cases were analyzed. Descriptive statistics were used to characterize the collected data using SPSS version 25.0.
Results
We summarize the results of this study and reported cases in Table 1. The analysis of clinical features of 20 cases is shown in Table 2.
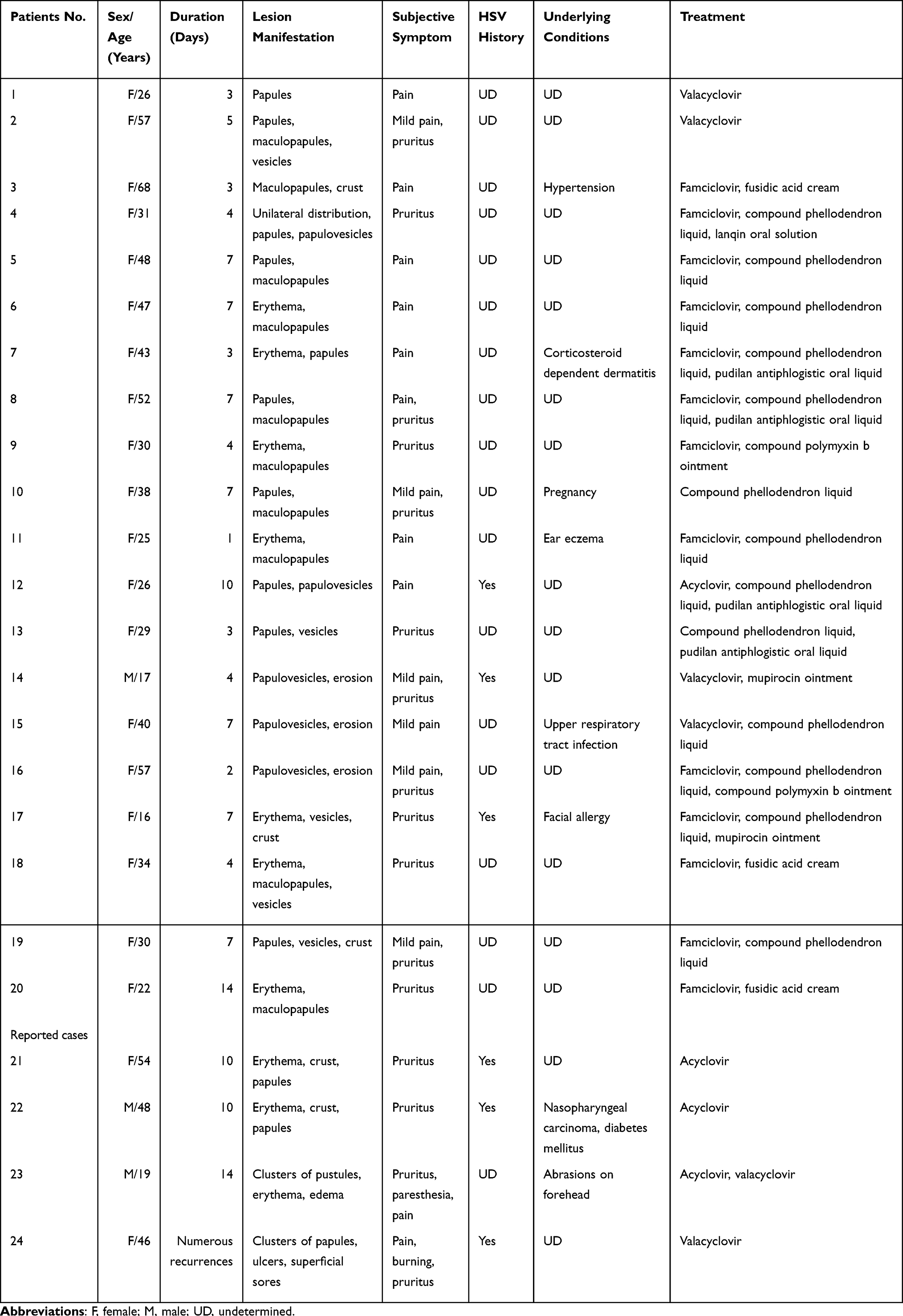 |
Table 1 Clinical Datas of Patients with Herpetic Folliculitis on the Face |
 |
Table 2 Analysis of Clinical Features of 20 Cases of Facial Herpetic Folliculitis (n = 20) |
A total of 20 patients were included, except for one male, the rest of whom were females. The mean age of patients was 36.8±14.35 years, which varied from 16 to 68 years. The duration differed from 1 to 14 days. The median value was 4.5 days. The clinical lesions presented mainly papules, maculopapules, and erythema (Figure 1). Only a few cases showed crust and erosion. most were distributed bilaterally on the face. Patients usually suffered pain or pruritus when folliculitis appeared. Patients 2 and 4 performed polymerase-chain reaction (PCR) tests and the results showed HSV-2 and HSV-1 infection, respectively. Three patients had a clear history of herpes simplex before folliculitis. One patient who had a pregnancy was advised to use Compound Phellodendron Liquid through wet compressing and lesions improved after ten days. The other 19 patients’ lesions improved with antiviral drugs within seven days. Our patients did not report underlying immunodeficiency, autoimmune diseases, or tumors. In the reported four cases, lesions were mostly presented as erythema and papules. They felt pruritus or pain and all cases were diagnosed by pathology or PCR. Three cases had a history of HSV infection, and Patients 23 and 24 PCR revealed HSV-1. Textural changes, such as scars, were absent in all 24 cases after treatments.
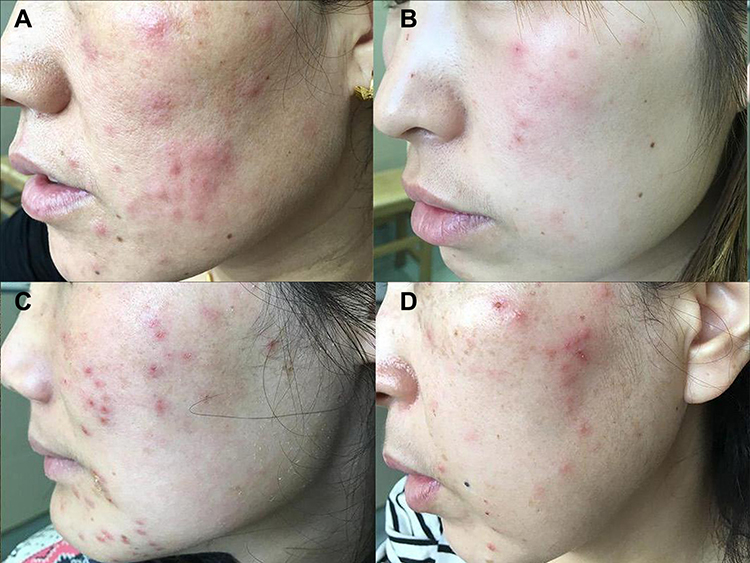 |
Figure 1 Various presentations of lesions (A–D). |
As Figure 2 shows, the patient was seen with painful multiple maculopapules and papules on her face for one week (Figure 2A and B). She mainly received oral famciclovir capsules 250mg three times a day and the lesions cleared out after 6 days without recurrence two months follow-up (Figure 2C and D).
 |
Figure 2 The change of lesions before and after treatments. (A and B) Herpetic folliculitis: multiple discrete red papules and maculopapules on the face. (C and D) Lesions disappeared after the six-day antiviral treatment. |
Discussion
HSV is a very common cause of skin infections. HSV-1 is usually associated with oral and facial infections and encephalitis, while HSV-2 usually causes genital infections.3 Nevertheless, only a few cases of HSV-related HF have been reported in the literature. In 1972, Izumi et al2 reported HSV-induced folliculitis of the whiskers, called herpetic sycosis, characterized by acute and rapid developing grouped painful erythema and papulovesicules, and discrete, satellite, and umbilicated vesiculofolliculers, preceded by burning or pruritus. Each case had a history of shaving with a razor. The duration of folliculitis lasted two to three weeks and the lesions tended to heal spontaneously with punctate follicular scars. Weinberg et al4 described two cases of herpetic sycosis where their diagnosis was made on clinical features and the Tzanck tests were positive. No biopsy or virus culture was performed. Both cases responded well to acyclovir treatment and healed without scar formation. The patients had previously been misdiagnosed with bacterial folliculitis and were treated with antibiotics for several days.
HF has been identified outside the beard area. Milioskas and Leong5 reported a case of occipital HSV-induced lymphadenopathy, with HF localized to the occiput which was confirmed by biopsy. In addition, Sexton6 reported two cases of occult herpesvirus infection, clinically similar to pseudolymphoma, involving the face and scalp but limited to a unilateral extent.
Skin biopsies usually showed viral-induced changes limited to hair follicles or follicular sebaceous glands without the involvement of the interfollicular epidermis, thus explaining the atypical clinical presentations.7 Recognition of the typical histological features of herpetic folliculitis can contribute to an accurate diagnosis.4 Böer et al8 analyzed the clinical and histopathological presentations of 21 patients with herpetic folliculitis, and they found that the PCR results were positive for VZV or HSV-1 in all patients. Cutaneous manifestations included erythema, erythematous papules, or plaques, but lacked vesicles or pustules. Early in the course of the disease, herpesvirus folliculitis presents as lymphocytic folliculitis without epidermal surface change, while complete involvement of hair follicles is typical of herpes zoster.8 The typical pathology of HSV infection shows ballooning, intranuclear viral inclusion, acantholysis, and multinucleated giant cells.9 Dense lymphocytic infiltration around blood vessels and appendages was seen throughout the dermis.9
Our patients, predominant middle-aged women, had an acute onset of folliculitis with a short course, and no fever or physical discomfort. We assumed women had a large proportion that may be associated with abuse of cosmetics resulting in impairment of skin barrier function. Lesions primarily presented as papules, maculopapules, and erythema, lacked vesicles or pustules. All lesions healed without scarring after short-term antiviral therapy. In all cases, there was no underlying immunocompromise or immunodeficiency, and only a few patients underwent PCR to confirm the diagnosis of HSV infection. Typical lesions of HSV infection, such as blisters and pustules, may not occur and even cause misdiagnosis. We emphasize that in patients with acute generalized facial folliculitis, it is necessary to consider the HSV infections at diagnosis. Though we could not conclude that all cases of HF were caused by HSV, the clinical presentations did not comply with herpes zoster infections. Sometimes PCR can confirm the presence of HSV. However, PCR is not yet applicable in parts of the world, where the diagnosis can only be made through clinical presentations and histopathology.10
The major clinical differential diagnosis for HF is bacterial folliculitis, with Staphylococcus aureus as the most common culprit. In addition, eczema herpeticum, also known as Kaposi varicelliform eruption, usually with fever and physical discomfort, should be considered when patients with underlying skin conditions, such as atopic dermatitis secondary to HSV infection. The lesions are characterized by clustered umbilicated blisters or pustules, small punctate seepage or crust.11 HF always develops acutely and diffusely, most in middle-aged women with lesions easy to rupture, and has short-term duration. However, different from HF, acne often appears in teenagers or youngsters with various kinds of lesions, including comedos, papules, pustules, cysts, and nodules, and reoccurs frequently. Excoriated acne usually has a clear history of using certain tools to pick on the acne. This may also be due to behavioral disorders of an individual. Due to the limitation of skin biopsy, PCR was recommended to distinguish similar diseases from HF. In patients with acne-like lesions that have failed to respond to conventional treatment, HF also should be raised.12 When lesions present unilaterally, herpes zoster must be considered.
In our cases, only three patients had a clear history of HSV infection before HF. Most occur in healthy patients with primary virus infections, who may lack pre-existing immunity to HSV, thus resulting in the facial inflammatory response. Whether it may be related to the abnormal immune system still requires further studies to elucidate the pathogenesis of viral folliculitis. When patients had acute pruritic or painful folliculitis with the absence of response to antibiotic or antifungal therapy, it is necessary to consider the possibility of facial HF and early antiviral therapy, even without signs of immunosuppression or pre-existing herpes infection.13
The diagnosis of HF is based on clinical and/or histologic findings, and also includes serologic testing (HSV-specific antibodies), Tzanck smears or viral cultures, and PCR from tissue sections or blisters. PCR may be helpful when herpetic folliculitis on the face is clinically suspected but cannot be confirmed by histology.14
Conclusion
In conclusion, HF is a rare skin infection disease and is uncommon in the literature, especially on the face. We summarize only about 24 cases and more are needed to better understand this disease. Dermatologists should be aware that HSV infections in patients with facial generalized folliculitis even if they have no underlying condition or history of HSV infection, especially if they show resistance to antibacterial and antifungal treatments.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent Statements
All patients signed informed consent forms that included consent for publication of all case details and accompanying images.
Funding
This work was supported by the Natural Science Foundation of Shandong Province (2014ZRE27077).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Al-Dhafiri SA, Molinari R. Herpetic folliculitis. J Cutan Med Surg. 2002;6(1):19–22. doi:10.1177/120347540200600104
2. Izumi AK, Kim R, Arnold H. Herpetic sycosis. Report of two cases. Arch Dermatol. 1972;106(3):372–374. doi:10.1001/archderm.1972.01620120056012
3. Whitley RJ, Roizman B. Herpes simplex virus infections. Lancet. 2001;357(9267):1513–1518. doi:10.1016/S0140-6736(00)04638-9
4. Weinberg JM. Viral folliculitis. Atypical presentations of herpes simplex, herpes zoster, and molluscum contagiosum. Arch Dermatol. 1997;133(8):983–986. doi:10.1001/archderm.1997.03890440053009
5. Miliauskas JR, Leong AS. Localized herpes simplex lymphadenitis: report of three cases and review of the literature. Histopathology. 1991;19(4):355–360. doi:10.1111/j.1365-2559.1991.tb00051.x
6. Sexton M. Occult herpesvirus folliculitis clinically simulating pseudolymphoma. Am J Dermatopathol. 1991;13(3):234–240. doi:10.1097/00000372-199106000-00004
7. McSorley J, Shapiro L, Brownstein MH, Hsu KC. Herpes simplex and varicella-zoster: comparative histopathology of 77 cases. Int J Dermatol. 1974;13(2):69–75. doi:10.1111/j.1365-4362.1974.tb01769.x
8. Böer A, Herder N, Winter K, Falk T. Herpes folliculitis: clinical, histopathological, and molecular pathologic observations. Br J Dermatol. 2006;154(4):743–746. doi:10.1111/j.1365-2133.2005.07118.x
9. Jang KA, Kim SH, Choi JH, Sung KJ, Moon KC, Koh JK. Viral folliculitis on the face. Br J Dermatol. 2000;142(3):555–559. doi:10.1046/j.1365-2133.2000.03378.x
10. Bello CC, Burgos CS, Cárdenas DC, González BS. Foliculitis necrotizante herpética. Revista médica de Chile. [Necrotizing herpes folliculitis. Report of one case]. Rev Med Chil. 2012;140(12):1589–1592. Spanish. doi:10.4067/S0034-98872012001200011
11. Mir-Bonafé JM, Román-Curto C, Santos-Briz A, Palacios-álvarez I, Santos-Durán JC, Fernández-López E. Eczema herpeticum with herpetic folliculitis after bone marrow transplant under prophylactic Acyclovir: are patients with underlying dermatologic disorders at higher risk? Transpl Infect Dis. 2013;15(2):E75–E80. doi:10.1111/tid.12058
12. Brabek E, El Shabrawi-Caelen L, Woltsche-Kahr I, Soyer HP, Aberer W. Herpetic folliculitis and syringitis simulating acne excoriée. Arch Dermatol. 2001;137(1):97–98.
13. Campanelli A, Marazza G, Stucki L, et al. Fulminant herpetic sycosis: atypical presentation of primary herpetic infection. Dermatology. 2004;208(3):284–286. doi:10.1159/000077323
14. Thomas CA, Smith SE, Morgan TM, White WL, Feldman SR. Clinical application of polymerase chain reaction amplification to diagnosis of herpes virus infection. Am J Dermatopathol. 1994;16(3):268–274. doi:10.1097/00000372-199406000-00007
15. Wei EY, Coghlin DT. Beyond folliculitis: recognizing herpes gladiatorum in adolescent athletes. J Pediatr. 2017;190:283. doi:10.1016/j.jpeds.2017.06.062
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.