")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Extreme desert dust storms and COPD morbidity on the island of Crete
Authors Lorentzou C, Kouvarakis G, Kozyrakis GV, Kampanis NA, Trahanatzi I, Fraidakis O, Tzanakis N, Kanakidou M , Agouridakis P, Notas G
Received 9 March 2019
Accepted for publication 22 June 2019
Published 6 August 2019 Volume 2019:14 Pages 1763—1768
DOI https://doi.org/10.2147/COPD.S208108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Christina Lorentzou,1 Giorgos Kouvarakis,2 Georgios V Kozyrakis,3 Nikolaos A Kampanis,3 Irene Trahanatzi,4 Othon Fraidakis,4 Nikolaos Tzanakis,5 Maria Kanakidou,2 Panagiotis Agouridakis,1 George Notas1,3
1University of Crete, School of Medicine, University Hospital, Department of Emergency Medicine, Heraklion, Greece; 2Department of Chemistry, Environmental Chemical Processes Laboratory, University of Crete, Heraklion, Greece; 3Foundation for Research and Technology - Hellas (FORTH), Institute of Applied and Computational Mathematics, Coastal and Marine Research Lab, Heraklion, Greece; 4Venizeleion Hospital of Heraklion, Department of Emergency Medicine, Heraklion, Greece; 5University of Crete, School of Medicine, University Hospital, Department of Pulmonary Medicine, Heraklion, Greece
Introduction and objectives: Short-term extreme increases in desert-derived particulate-matter with aerodynamic diameter below 10 μm (PM10) may affect emergency department (ED) visits due to COPD exacerbations.
Research question: Our aim was to identify the effect of extreme increases in desert-derived PM10 on ED visits for dyspnea and COPD exacerbations and on the related hospital admissions.
Methods: We performed a retrospective analysis of dyspnea-related ED visits and hospital admissions in Heraklion, Crete, during four consecutive storms of desert-derived PM10 that happened during March 2018. We collected data from over 17,000 ED visits and recorded patients with atopic symptoms, COPD exacerbations, and dyspnea, as well as admissions to the departments of pulmonary medicine, internal medicine, and cardiology. PM10 data were collected from a monitoring station in the same geographic area.
Results: Four desert dust storms were recorded during the study period with 238, 203, 1138, and 310 μg/m3 average-daily PM10 and 652, 308, 4262, and 778 μg/m3 hourly mean day-peak PM10, respectively. There was no clinically important increase in total ED visits, total admissions or admissions to the departments of cardiology, pulmonary medicine, or internal medicine, during PM10 peaks. However, during the desert dust storm with daily-average PM10 above 500 μg/m,3 there was a striking increase in dyspnea-related ED visits (including COPD exacerbations, 3.6-fold increase), while there was no clinically important increase in non-asthma allergy-related ED visits.
Conclusion: Extreme desert dust storm episodes may cause meaningful increases in ED visits for dyspnea and COPD exacerbations/admissions.
Keywords: desert dust storms, emergency department overcrowding, particulate-matter, COPD
Plain language summary
Increased urban particulate-matter with aerodynamic diameter below 10 μm (PM10) may compromise respiratory function in patients with preexisting respiratory diseases. Apart from urban PM10, Southern Europe experiences desert dust PM10 storms due to climatic change. Previous studies have failed to show a significant impact of desert dust storms on emergency department visits for respiratory complaints. We describe the effect of a unique and extreme desert dust PM10 storm with daily average PM10>1000 μg/m3 on emergency department overload, focusing on respiratory and especially COPD pathology, in the southernmost region of the European Union, the island of Crete. We conclude that while most desert dust storms do not affect COPD admissions, extreme desert dust storms with a threshold of PM10 above at least 500 μg/m3 may indeed increase ED visits for dyspnea and COPD exacerbations/admissions.
Introduction
Southern European areas frequently experience dust storms caused by certain, well characterized, meteorological conditions that promote transportation of particles from the adjacent Sahara desert. These desert particles consist of fine particulate-matter (PM) and are able to penetrate deep in the respiratory system. This is especially true regarding PM with an aerodynamic diameter of less than 10 μm, abbreviated as PM10. PM10 includes desert dust (crustal material), re-suspended dust (crustal and anthropogenic material), sea-salt, anthropogenic inorganic and organic components, and biogenic components.1–3 Although PM10 is expected to compromise respiratory function, especially in patients with preexisting respiratory diseases,4 several previous studies failed to show a statistically significant impact of desert dust storms on emergency department (ED) visits for respiratory complaints.5,6 However, these studies focused mostly on urban areas that are characterized by high levels of human activity derived PM10. Even when adjusting for non-desert PM10, these studies reported relatively small increases in desert-derived PM10 (<100 μg/m3 increases compared to non-desert storm days). Less is known about the short-term effect of the extreme desert dust storms lasting several hours with PM10 levels higher than 200 μg/m3.
The aim of our study was to report the short-term effect of consecutive extreme increases in desert-originating PM, on ED visits for respiratory symptoms and acute exacerbation of COPD (AECOPD) in the Southmost point of Europe; the island of Crete.
Materials and methods
Study design, setting, and statistical analysis
This is a retrospective analysis of ED visits at the two hospitals located in the city of Heraklion in Crete, the University Hospital of Heraklion (PAGNI, 739 beds) and Venizelion Hospital (440 beds), from March 1st to March 31st, 2018. Both Hospitals cover the Municipality of Heraklion (≥300,000 inhabitants), with a rotating on-call system (every day one of the hospitals is on-call and the other one is on alert). The two hospitals are about 15 km apart and both have fully developed pulmonary medicine departments.
Population
All data regarding the number of ED visits were available for both hospitals, while administrative data from the University Hospital of Heraklion ED were also fully available. The number of patients visiting the ED for allergies (hives, angioedema, or anaphylactic shock), COPD exacerbations, dyspnea unrelated to other well-documented causes (eg, pleural effusion, pneumonia, pulmonary embolism, heart disease, etc.) were recorded. Data regarding the number of admissions to the departments of internal medicine, pulmonary medicine, and cardiology, including admission diagnosis, from both hospitals, were also analyzed. The study design and execution were in compliance with the Declaration of Helsinki. Patient consent to review their medical records was not required by the University Hospital of Heraklion/Venizeleion Hospital Bioethics Committee since only administrative data were collected and patient data anonymity and confidentiality were guaranteed.
Statistical analysis
One-Way ANOVA and Pearson Correlation (PC) with Bonferroni correction for multiple comparisons were performed with ΙΒΜ SPSS Statistics 21.0 (IBM, Armonk NY, USA)
PM10 data collection
PM10 data were collected and measured by an FH 62 I-R particulate monitor (Thermo TSM Anderson) continuously operating in Heraklion city center. PM10 mass measurements are based on b-attenuation and are conducted in the range 0–10,000 μg/m3 with a resolution of 1 μg/m3. They are found in very good agreement with gravimetric measurements.1
Results
Long-term monitoring of aerosols on Crete is based on PM10 measurements (Figure 1). PM2.5 measurements are not available for the studied period. However, size-segregated PM observations performed over a period of 2 years have shown a good correlation between PM10 and PM2.5 measurements with PM2.5 accounting on average for 60% of the PM10 mass.7 Dust storms were defined by PM10 levels above 100 μg/m3, a limit that has been previously used for Asian dust storms.8,9 We, therefore, used 24 hrs PM10 average concentration above 100 μg/m3, to characterize four desert dust storm episodes during the study period. These were between March 3rd and 5th, on March 7th, on March 22nd, and during March 26th-27th with top daily-average (hourly mean day-peak) PM10 values of 238 (652), 203 (308), 1138 (4262), and 310 (778) μg/m3, respectively. The monthly and the non-peak days PM10 average were 112 and 24 μg/m3, respectively and were higher compared to previous years (Figure 2A).
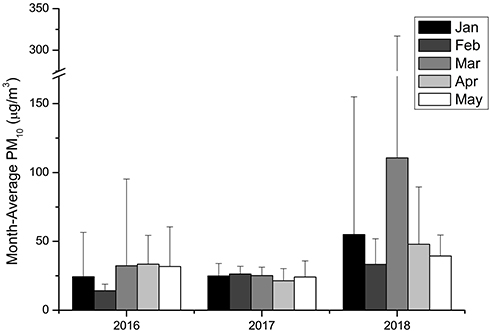 |
Figure 1 Monthly mean of PM10 aerosols in Heraklion, Crete from January to May for the years 2016–2018. Values represent the monthly mean (μg/m3) + standard deviation. |
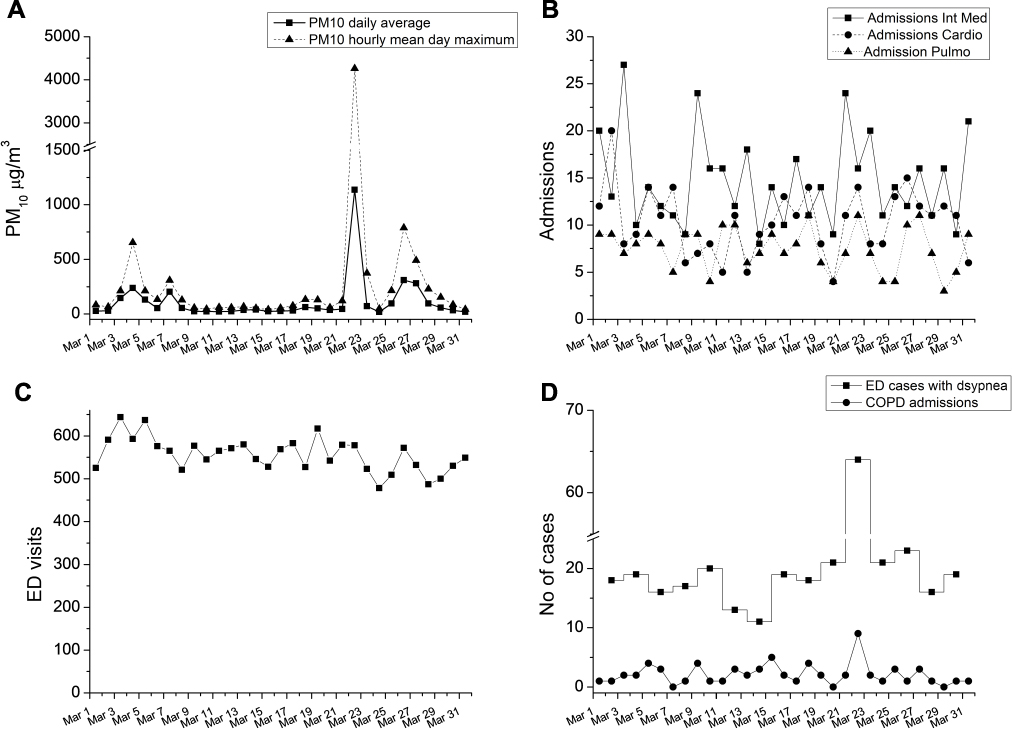 |
Figure 2 (A) Particulate matter with aerodynamic diameter below 10 μm (PM10) daily average and hourly mean day maximum during March 2018 in the geographic area of Heraklion. (B) Admissions to the departments of internal medicine (Int Med), cardiology (Cardio) and pulmonary (Pulmo) medicine during March 2018. (C) Total emergency department (ED) visits in Heraklion during the study period. (D) ED cases with dyspnea and COPD admissions at the University Hospital of Heraklion during the study period. We did not identify any increases in the studied parameters the days ensuing a desert dust storm. |
Overall, there were 17,239 ED visits in both hospitals. During PM10 peaks we did not identify clinically important increases in the number of total ED visits, the number of all hospital admissions or the number of admissions to the departments of cardiology, pulmonary medicine, or internal medicine (Figure 2B and C and Table 1).
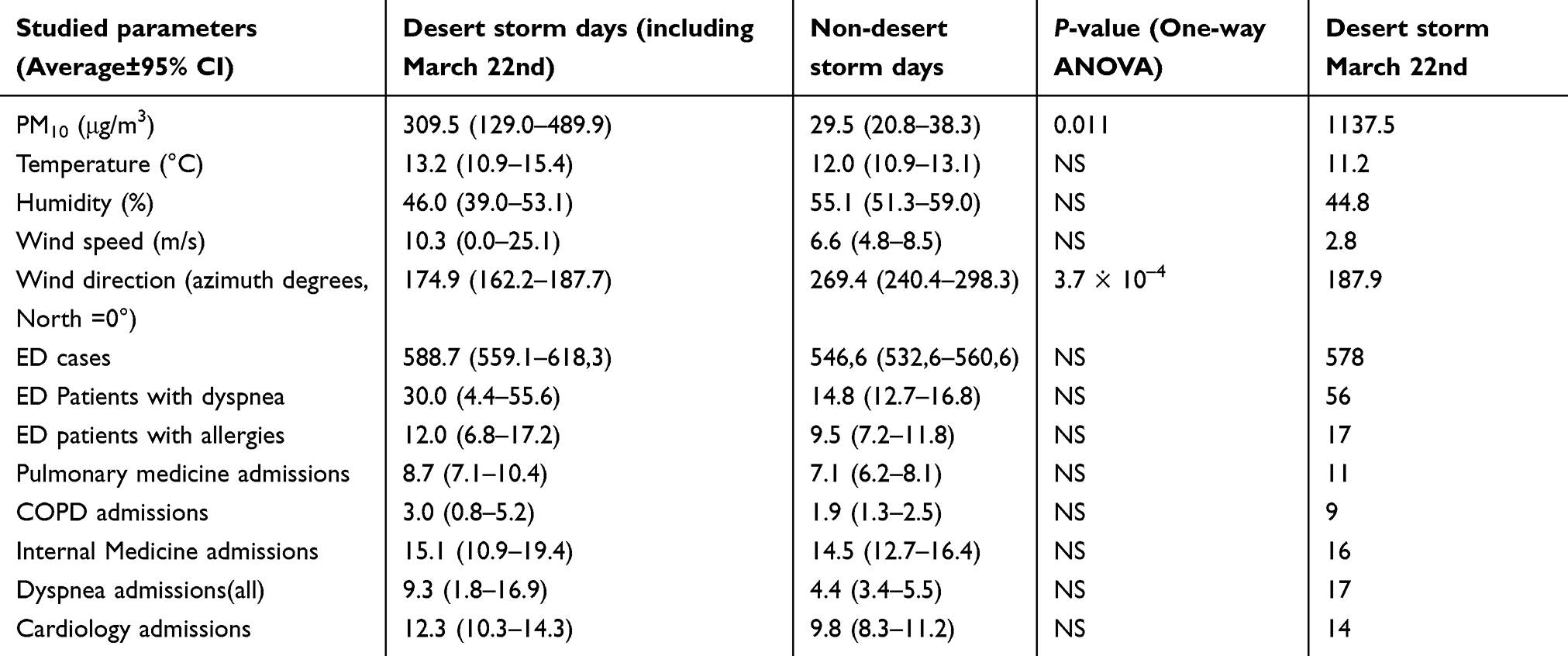 |
Table 1 Comparison of environmental and clinical information between days with and without desert dust storm. It is reasonable to have mostly southern winds during desert dust storms |
In the extreme desert dust storm (PM10>1000 μg/m3), there was a striking increase (a) in the number of patients presenting to the ED with dyspnea (including COPD exacerbations, 3.6 times vs other days), and (b) in admissions due to COPD exacerbation (4.2 times vs other days) (Figure 2D).
Using Pearson correlation coefficient with Bonferroni correction for multiple comparisons (Table 2) a significant correlation was observed between (a) PM10 concentrations and ED visits for dyspnea (Pearson Correlation 0.929, p<0.00001), and (b) PM10 concentrations and admissions for COPD exacerbations and dyspnea (PC 0.813, p<0.0001 and PC 0.718, p<0.001) respectively. There was no significant increase in the number of patients visiting the ED for allergies. Regarding the rest of the environmental factors, temperature, wind speed, and humidity did not correlate with ED visits or COPD admissions and were not further examined as confounding factors. Wind direction, as expected correlated with clinical events since South wind direction is a prerequisite for the transfer of Sahara dust to the island of Crete.
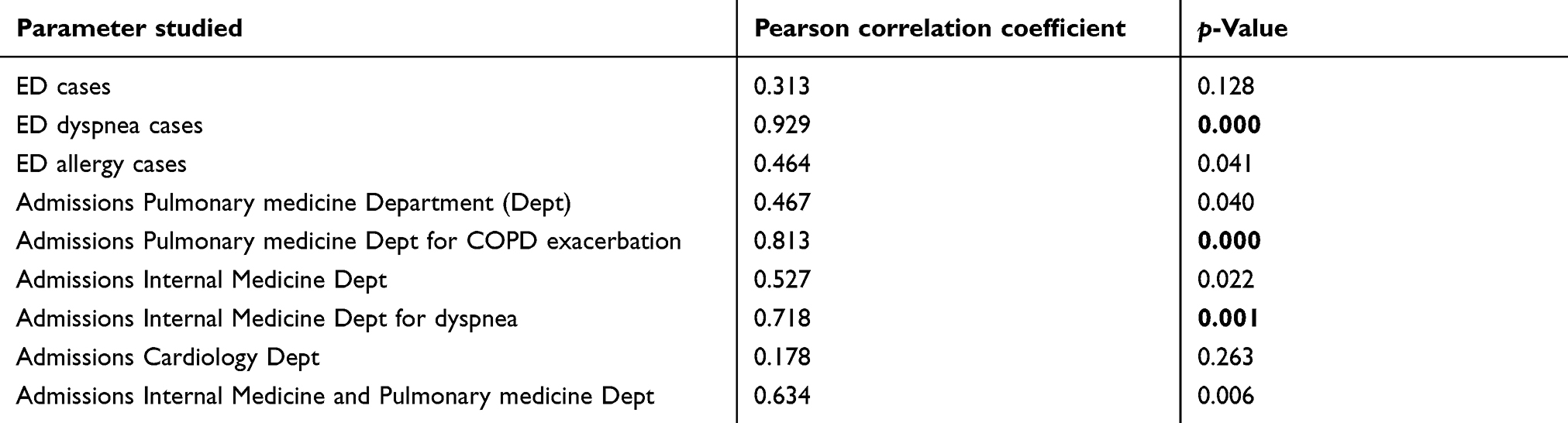 |
Table 2 Pearson correlation results for the parameters tested. Significant results after Bonferroni correction of p (≤0.05/9=0.0056) are presented in bold |
Discussion
The main finding of this study was that only extreme desert dust storms seem to be related to increased ED visits and hospital admissions for dyspnea and COPD. However, even at extreme levels, they do not acutely affect the number of allergic or cardiovascular disease-related events. Although such extreme conditions are rare and currently difficult to predict, emergency physicians and pulmonary medicine specialists in Southern Europe should be aware of the expected high incidence of patients with respiratory compromise, when they occur. Dust storms with lower levels of PM10 do not seem to affect the workload of emergency medicine and pulmonary medicine departments.
Previous studies and meta-analysis on PM effects on health have focused mostly on pollution-related increases of PM10.3 In studies that concentrated on desert dust storms, the reported outcomes are mostly mortality and hospitalizations,5 and the reported increases of PM10 were much less compared to the phenomena experienced in Crete on March 2018. A previous study in Athens reported a higher incidence of ED visits for asthma, COPD and respiratory infections by 38%, 57%, and 60%, respectively, for daily PM10 increases in the range of 36.5–78.5 μg/m3.6 However, in this study, the percentage of increases described are very small compared to the extreme event described in our report, while human-activity related PM10 levels could be a significant confounding factor. Vodonos et al, have also reported a significant correlation between desert dust storms and COPD exacerbations in Israel.4 In accordance with our study, a significant increase in ED respiratory disorders visits, and no effect on all causes hospital admissions, was reported in Sydney, Australia during September 2009 when peak dust storm PM10 levels reached 11,000 μg/m3.10 However, in contrast to our results, they reported increases in all-cause ED visits. This difference may be attributed to the higher PM10 levels in the Australian event.
Our research presents, to our best knowledge, the most extreme event of desert dust storm within Europe (for images visit https://www.youtube.com/watch?v=O5gUvUK8FDM). The comparison of the extreme dust storm of March 22nd with the other dust storms during that month, suggests for the first time, that there exists a threshold of daily-average PM10 around (or above) 500 μg/m3. Above this level, Emergency Services should expect a clinically important increase in the number of patients presenting with respiratory compromise. However, more research is necessary in order to confirm this threshold. A limitation of our study is its short duration. We also did not identify any lag effect between the change of PM10 and the measured effects. A more extended study covering more desert dust storms and a larger population would be more efficient in identifying such effects. However, the desert dust storms sequence during this small period provided us with a unique opportunity to study health effects without major influence from seasonal variations of ED visits and AECOPD due to infections, while the absence of a lag between the massive event on March 22nd and the measured clinical effects suggests that such high levels of desert dust derived PM10 can induce acute (within hours) effects in COPD patients. Another limitation of our study is the use of the administrative data to define admission diagnosis, instead of a per-patient clinical analysis. However, it is unlikely to introduce a significant bias as the same approach was also used for the reference day’s data.
Conclusion
Intense desert dust storms with a threshold of PM10 above at least 500 μg/m3 may cause clinically important increases in ED visits for COPD exacerbations as well as COPD-related admissions. Climatic change may lead to an increased incidence of extreme desert dust storms in Southern Europe. Early identification or prediction of extreme desert dust storms will allow the prompt issue of health warnings for patients with COPD and other preexisting pulmonary diseases to avoid exposure to such irritating conditions and will allow EDs to prepare for climaxes of dyspnea-related cases during these events.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gerasopoulos E, Kouvarakis G, Babasakalis P, Vrekoussis M, Putaud JP, Mihalopoulos N. Origin and variability of particulate matter (PM10) mass concentrations over the Eastern Mediterranean. Atmos Environ. 2006;40(25):4679–4690. doi:10.1016/j.atmosenv.2006.04.020. PubMed PMID: WOS:000239820600004. English.
2. Perrino C, Catrambone M, Esposito G, Lahav D, Mamane Y. Characterisation of gaseous and particulate atmospheric pollutants in the East Mediterranean by diffusion denuder sampling lines. Environ Monit Assess. 2009;152(1–4):231–244. doi:10.1007/s10661-008-0311-9. PubMed PMID: 18535917.
3. Pope CA
4. Vodonos A, Friger M, Katra I, et al. The impact of desert dust exposures on hospitalizations due to exacerbation of chronic obstructive pulmonary disease. Air Qual Atmos Health. 2014;7(4):433–439. doi:10.1007/s11869-014-0253-z. PubMed PMID: WOS:000345393400004. English.
5. Stafoggia M, Zauli-Sajani S, Pey J, et al. Desert dust outbreaks in Southern Europe: contribution to daily PM(1)(0) concentrations and short-term associations with mortality and hospital admissions. Environ Health Perspect. 2016;124(4):413–419. doi:10.1289/ehp.1409164. PubMed PMID: 26219103. Pubmed Central PMCID: 4829979.
6. Trianti SM, Samoli E, Rodopoulou S, Katsouyanni K, Papiris SA, Karakatsani A. Desert dust outbreaks and respiratory morbidity in Athens, Greece. Environ Health. 2017;16(1):72. doi:10.1186/s12940-017-0281-x. PubMed PMID: 28666479. Pubmed Central PMCID: 5493869.
7. Gerasopoulos E, Koulouri E, Kalivitis N, et al. Size-segregated mass distributions of aerosols over Eastern Mediterranean: seasonal variability and comparison with AERONET columnar size-distributions. Atmos Chem Phys. 2007;7(10):2551–2561. doi:10.5194/acp-7-2551-2007. PubMed PMID: WOS:000246903900007. English.
8. Lai LW, Cheng WL. The impact of air quality on respiratory admissions during Asian dust storm periods. Int J Environ Health Res. 2008;18(6):429–450. doi:10.1080/09603120802272227. PubMed PMID: 19031147.
9. Lin YK, Chen CF, Yeh HC, Wang YC. Emergency room visits associated with particulate concentration and Asian dust storms in metropolitan Taipei. J Expo Sci Environ Epidemiol. 2016;26(2):189–196. doi:10.1038/jes.2015.70. PubMed PMID: 26531803.
10. Merrifield A, Schindeler S, Jalaludin B, Smith W. Health effects of the September 2009 dust storm in Sydney, Australia: did emergency department visits and hospital admissions increase? Environ Health. 2013;12:32. doi:10.1186/1476-069X-12-32. PubMed PMID: 23587335. Pubmed Central PMCID: 3639126.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.